Renal Excretion of Urobilinogen in the Dog
8
Renal Excretion of Urobilinogen in the Dog MORTIMER LEVY, RoGER LESTER, and Noimu N G. LEVINSKY From the Fifth and Sixth (Boston University) Medical Services, Boston City Hospital, and the Department of Medicine, Boston University School of Medicine, Boston University Medical Center, Boston, Massachusetts 02118 A B S T R A C T The renal excretion of urobilinogen was studied in dogs by standard clearance tech- niques. The use of radiochemically pure tritiated mesobilirubinogen as a representative urobilinogen afforded much greater analytical precision than can be obtained with the usual colorimetric and fluorimetric techniques which are only semiquanti- tative. With constant plasma levels of urobilino- gen, raising urinary pH from 5 to 8 increased urobilinogen excretion from about 30% to up to 2007%o of the filtered load. When urinary pH was kept constant, changes in blood pH had no effect on urobilinogen excretion. Increases in urinary flow had no effect on urobilinogen excretion when the urine was alkaline but increased excretion markedly during aciduria. Probenecid did not influence urobilinogen excretion by the kidney. It is concluded that urobilinogen is excreted by a three-component system of glomerular filtration, active secretion, and pH-dependent nonionic diffu- sion in the distal nephron. Urobilinogen is a weak acid, and this mode of excretion is similar to that of other weak, organic acids, such as salicylates. These results indicate that urinary pH and flow must be considered in the clinical interpretation of measurements of urinary urobilinogen. This work was presented in part before the American Federation for Clinical Research, National Meeting, At- lantic City, N. J., April, 1967. Dr. Levinsky is an Established Investigator of the American Heart Association. Address reprint requests to Dr. Norman G. Levinsky, Boston University Medical Center, 15 Stoughton Street, Boston, Mass. 02118. Received for publication 25 March 1968 and in revised form 27 May 1968. INTRODUCTION Considering how frequently urobilinogen is esti- mated clinically, surprisingly little is known about the mechanism of urobilinogen excretion. Three studies of urobilinogen excretion in man have come to three different conclusions: that excretion is by glomerular filtration alone (1), that both filtration and tubular secretion occur (2), and that excretion is a complex process involving filtration, secretion, and reabsorption by pH-dependent non- ionic diffusion (3). The only previous study in the dog suggested that glomerular filtration alone is involved (2). All these results, however, depend on spectrophotometric or fluorescent analytical techniques which probably are not completely re- liable (3). In order to obtain greater analytical accuracy, we have, therefore, restudied this prob- lem in dogs, taking advantage of the availability of techniques for the preparation of radiolabeled uro- bilinogen (4). Our data extend the observations of Bourke, Milne, and Stokes (3) and support their conclusions as to the mechanism of urobilinogen excretion. METHODS Experiments were performed on 28 female mongrel dogs, anaesthetized with sodium pentobarbital. Food and water were removed 15-18 hr before an experiment. Preparation and administration of tritiated mesobili- rubinogen (urobilinogen-3H). Mesobilirubinogen-'H, a representative urobilinogen, was prepared by catalytic re- duction of bilirubin in the presence of tritiated water, according to the method of Lester and Klein (4). This compound has been shown to be radiochemically pure (4), and it has been established that it behaves in vivo identically to C14-labeled mesobilirubinogen (5). Urobilinogen-'H prepared as a lyophilized powder was stored in sealed vials at -20'C. Just before an experi- The Journal of Clinical Investigation Volume 47 1968 2117
Transcript of Renal Excretion of Urobilinogen in the Dog

Renal Excretion of Urobilinogen in the Dog
MORTIMER LEVY, RoGER LESTER, and Noimu N G. LEVINSKY
From the Fifth and Sixth (Boston University) Medical Services, Boston CityHospital, and the Department of Medicine, Boston University School ofMedicine, Boston University Medical Center, Boston, Massachusetts 02118
A B S T R A C T The renal excretion of urobilinogenwas studied in dogs by standard clearance tech-niques. The use of radiochemically pure tritiatedmesobilirubinogen as a representative urobilinogenafforded much greater analytical precision thancan be obtained with the usual colorimetric andfluorimetric techniques which are only semiquanti-tative. With constant plasma levels of urobilino-gen, raising urinary pH from 5 to 8 increasedurobilinogen excretion from about 30% to up to2007%o of the filtered load. When urinary pH waskept constant, changes in blood pH had no effecton urobilinogen excretion. Increases in urinaryflow had no effect on urobilinogen excretion whenthe urine was alkaline but increased excretionmarkedly during aciduria. Probenecid did notinfluence urobilinogen excretion by the kidney. Itis concluded that urobilinogen is excreted by athree-component system of glomerular filtration,active secretion, and pH-dependent nonionic diffu-sion in the distal nephron. Urobilinogen is a weakacid, and this mode of excretion is similar to thatof other weak, organic acids, such as salicylates.These results indicate that urinary pH and flowmust be considered in the clinical interpretation ofmeasurements of urinary urobilinogen.
This work was presented in part before the AmericanFederation for Clinical Research, National Meeting, At-lantic City, N. J., April, 1967.
Dr. Levinsky is an Established Investigator of theAmerican Heart Association.
Address reprint requests to Dr. Norman G. Levinsky,Boston University Medical Center, 15 Stoughton Street,Boston, Mass. 02118.Received for publication 25 March 1968 and in revised
form 27 May 1968.
INTRODUCTION
Considering how frequently urobilinogen is esti-mated clinically, surprisingly little is known aboutthe mechanism of urobilinogen excretion. Threestudies of urobilinogen excretion in man havecome to three different conclusions: that excretionis by glomerular filtration alone (1), that bothfiltration and tubular secretion occur (2), and thatexcretion is a complex process involving filtration,secretion, and reabsorption by pH-dependent non-ionic diffusion (3). The only previous study inthe dog suggested that glomerular filtration aloneis involved (2). All these results, however, dependon spectrophotometric or fluorescent analyticaltechniques which probably are not completely re-liable (3). In order to obtain greater analyticalaccuracy, we have, therefore, restudied this prob-lem in dogs, taking advantage of the availability oftechniques for the preparation of radiolabeled uro-bilinogen (4). Our data extend the observations ofBourke, Milne, and Stokes (3) and support theirconclusions as to the mechanism of urobilinogenexcretion.
METHODSExperiments were performed on 28 female mongrel dogs,anaesthetized with sodium pentobarbital. Food and waterwere removed 15-18 hr before an experiment.
Preparation and administration of tritiated mesobili-rubinogen (urobilinogen-3H). Mesobilirubinogen-'H, arepresentative urobilinogen, was prepared by catalytic re-duction of bilirubin in the presence of tritiated water,according to the method of Lester and Klein (4). Thiscompound has been shown to be radiochemically pure(4), and it has been established that it behaves in vivoidentically to C14-labeled mesobilirubinogen (5).
Urobilinogen-'H prepared as a lyophilized powder wasstored in sealed vials at -20'C. Just before an experi-
The Journal of Clinical Investigation Volume 47 1968 2117

ment, vials were opened and the contents dissolved in0.7-1.0 ml of methanol or ethanol. This was furtherdiluted 2.5 times in distilled water and the entire volumeadded to 10-20 ml of autologous fresh heparinizedplasma. An aliquot of this solution was set aside in orderto determine the total amount of urobilinogen adminis-tered to the dog (approximately 0.5-1.0 mg). The re-mainder was then administered to the dog by constantintravenous infusion at a rate of 0.04 ml/min (approxi-mately 2-3 gg/min) after an initial prime of 1.5-2.0 mlhad been given. At least 30 min was allowed for equili-bration before the start of an experiment. During theexperiment the urobilinogen was kept covered to avoidexposure to light; marked color change, indicating sig-nificant urobilin formation, was never noted.
Clearance experiments. The renal excretion of uro-bilinogen-3H was studied by conventional clearance tech-niques. The clearance of exogenous creatinine was usedto measure glomerular filtration rate (GFR). Urine wascollected from a retention catheter in the bladder, andblood samples were taken from an indwelling arterialneedle. All infusions were administered intravenously byconstant infusion pumps.To induce urinary acidification, dogs were given 10.0
g of ammonium chloride daily for 2 days before anexperiment, and 0.015 N HCl in 0.9% saline was infusedintravenously during appropriate periods of the experi-ment. Alkaline urines were produced by changing thisinfusion to 0.15 M or 0.30 M NaHCO3. When urine pHwas to be determined, small aliquots of urine were col-lected under oil at the mid-point of each clearance period.
Analytical techniques. Samples of plasma and urinecontaining urobilinogen-8H were counted in a PackardTri-carb liquid scintillation counter as previously de-scribed (4). Internal standard was added to each vialto correct for quenching. Counting efficiency was gener-ally 8-15%o. Thin-layer chromatography of urobilino-gen-3H was carried out as previously described (4).Blood pH was measured with the capillary electrode
of a Radiometer pH meter (Radiometer Co., Copen-hagen). Urinary pH was determined immediately aftercollection of a sample, using a Corning pH meter. Read-ings were made at .room temperature and corrected to370C. Serum proteins were measured by refractometry.Creatinine was determined on an Auto-Analyzer.
Protein binding of urobilinogen was measured severaltimes during each experiment. All analyses were per-formed in duplicate. 3.5 ml of plasma was centrifugedunder oil for 16 hr at approximately 125,000 gma1, usinga No. 40 rotor, in a Beckman Model L ultracentrifuge.At the end of this, time, the serum proteins had been con-centrated into a reddish-orange pellet at the bottom ofthe tube, and 0.5 ml of clear supernatant was aspiratedfor counting. This supernatant was essentially protein-free when checked by refractometry or with biuret re-agent. It was counted in the same way as plasma andurine samples (4).
Calculations. Urobilinogen excretion was evaluatedfrom the clearance of free, or unbound, urobilinogen. Theclearance of free urobilinogen was calculated as equal
to urobilinogen excretion/plasma free urobilinogen. Uro-bilinogen excretion, dpm/min = urinary urobilinogen,dpm/ml, X urine flow, ml/min.. Plasma free urobilino-gen = total plasma urobilinogen, dpm/ml, X fraction ofunbound plasma urobilinogen, as estimated by ultracentri-fugation several times in each experiment. Binding wasdetermined directly on about one-half of the plasmasamples in each experiment and was interpolated for theother values.
RESULTS
Protein binding. During the infusion of uro-bilinogen into dogs, the steady-state plasma con-centrations of the infused material were of theorder of 2-3 ug/100 ml (range, 0.6-5 usg/100 ml).There was great variation among dogs in the frac-tion of urobilinogen bound to plasma proteins.The mean of 42 observations was 46.1 ± 10.1%(SD) bound, with a range from 28 to 67%.However, values for a given dog remained quiteconstant throughout the course of an experiment.Protein binding seemed to be unaffected by theuse of heparinized plasma as opposed to serumand by blood pH changes in the range 7.1-7.55.In a few dogs, dilution of plasma proteins de-creased binding slightly. When large amounts ofcarrier urobilinogen were infused, plasma con-centrations of 50-2500 ,ug/100 ml were obtained.Under these conditions, protein binding was de-creased slightly (38.6 ± 9.3%o, n = 14) as com-pared to the experiments in which only traceramounts were infused, but the difference was notstatistically significant. Because Bourke et al. (3)reported little scatter for the protein binding ofurobilinogen in human sera (77-85o ), we studiedthe binding of urobilinogen-3H in human serum byultracentrifugation, as described in Methods, andby ultrafiltration. By ultracentrifugation, values of70.7-72.9%o (n = 9) were obtained in humansera, and by ultrafiltration, values were 68.8-76.0% (n 6). These results provide evidencethat the ultracentrifugation method used in ourpresent dog studies is a valid technique for deter-mining protein binding. They also suggest that thelarge scatter observed in dogs in contrast to theuniformity of protein binding in man is probablydue to species difference.
Validity of urobilinogen-3H clearance measure-ments. The validity of clearances with meso-bilirubinogen-3H depends on the assumptions thatthis substance is excreted unaltered and with the
2118 M. Levy, R. Lester, and N. G. Levinsky

isotopic label intact. That this was indeed so in ourexperiments was determined in two different ways.First, it was demonstrated by thin-layer chroma-tography that the Rf value for urobilinogen-3Hextracted from dog urine was identical to that ofthe infusate. Moreover, all the radioactivity on thechromatograph corresponded to the urobilinogenband. Secondly, large amounts of carrier uro-bilinogen-3H were infused into two dogs and serialurine collections made. The specific activity of theurinary urobilinogen was 95 and 105%o that ofthe infusate. These data indicate that urobilino-gen-3H is excreted in the urine without significantalteration, and that urinary radioactivity is anaccurate index of urobilinogen excretion.
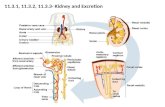
Influence of urinary pH on urobilinogen-'Hexcretion. In clearance experiments in whichplasma levels of urobilinogen-3H and urine flowwere held relatively constant, progressive increasesin urinary pH produced marked changes in uro-bilinogen excretion. Data from eight dogs areplotted in Fig. 1, and a detailed experimental pro-tocol is given in Table I. As urinary pH wasprogressively elevated, urobilinogen excretion in-creased from as little as 30%o of the filtered load in
2.01. _
i1.6
z 1.2hi
; 0.8
;
0w0
00
00
i_
00
*. *.
* : : -!
0 * 0. ** @00
* S0
00 * 0
I0
5 6 7 8URINE pH
FIGURE 1 Effect of urinary pH on urobilinogen-H ex-cretion. Data are from eight dogs; each point representsone clearance period. Urine flow (V) /glomerular filtra-tion rate (GFR) was relatively constant in these ex-periments.
TABLE I
Effect of Urine pH on Urobilinogen Excretion
C1/Urine V/ GFR
Time pH GFR V GFR Cu x100
min ml/ ml/ % ml/min min mmn
-175 1 g of creatinine prime; infusion started at 10.5 mg/minin water
-151 0.015 N HCO in 0.9% saline infused at 4.4 ml/min-35 Urobilinogen-&H, 1.5 ml prime; infusion started at 0.034
ml/min0-6 5.9 41 2.3 5.7 28 68
6-12 5.9 37 2.3 6.4 24 6412-18 5.9 40 2.3 5.8 27 6618-25 5.8 42 2.7 6.4 30 71
34 Start 0.15 M NaHCOs at 8.5 ml/min, discontinue HCOinfusion
40-52 6.0 41 2.1 5.1 31 7652-58 6.2 42 2.2 5.3 47 11258-66 6.35 42 2.1 4.9 47 112
70 Increase NaHCOa infusion to 16.4 ml/min70-81 6.55 46 2.5 4.7 41 9081-89 6.55 36 1.7 4.3 43 11989-99 6.8 47 2.0 4.3 59 125
99-111 6.8 43 1.9 5.0 62 144111-117 6.9 46 2.3 5.6 86 186
119 Increase NaHCOs infusion to 32 ml/min119-125 7.3 57 3.2 5.4 119 210125-132 7.3 44 3.2 7.3 81 182132-138 7.45 36 4.1 11.6 76 214138-945 7.45 39 5.0 12.0 75 193
GFR, glomerular filtration rate; V, urine flow; Cu, clearance of un-bound urobilinogen-3H.
the acid urines to as much as twice the filteredload in urines of maximal alkalinity. Thus, whilenet reabsorption of urobilinogen was occurringduring aciduria, net secretion was usually ob-served when the urine was alkaline. Since thefree urobilinogen clearance-to-creatinine clearanceratio (Cu/Ccr) reached 2 in some cases, the rateof secretion can at least equal the rate at whichurobilinogen is being filtered.
In four experiments, an alkaline urine wasachieved by inducing respiratory alkalosis. Thedogs were hyperventilated by means of a mechani-cal respirator for an hour or more until the urinebecame alkaline. At a urine pH of 6.5, Cu/Ccr was0.77 during hyperventilation; at pH 7.1, 1.31; atpH 7.3, 1.55; at pH 7.4, 1.49. (Each value is themean of two to five clearance collections in oneexperiment.) C./Cr at any urinary pH was ap-proximately equivalent when urine alkalinity wasproduced by this technique or by bicarbonate infu-sion, as may be seen by comparing these valueswith Fig. 1. These experiments indicate that the
Renal Excretion of Urobilinogen 2119

TABLE I IFailure of Changes in Blood pH to
Alter Urobilinogen Excretion
Urine Blood C./GFRTime pH pH GFR X100
min ml/min
-93 Creatinine prime and infusion at 0.5 ml/min-34 Urobilinogen prime and infusion at 0.4
ml/min
0-20 6.2 7.26 33 5020-38 6.2 7.27 32 6038-54 6.2 7.27 29 40
Start mechanical respirator57-67 6.2 7.50 33 4067-77 6.2 7.54 38 50
Abbreviations as in Table I.
volume loading which occurred during the induc-tion of alkalosis with bicarbonate infusions wasnot a factor in the increased urobilinogen excretionwhich occurred.The production of alkaline urines by infusion of
NaHCO8 and by prolonged hyperventilation ofnecessity led to mild systemic alkalosis. To deter-mine whether net secretion of urobilinogen was infact being caused by changes in plasma, ratherthan urinary pH, clearance periods were collectedin two dogs before and within the first 20-30 minafter hyperventilation by means of a mechanicalrespirator was begun. This maneuver producedmarked systemic alkalosis without initially influ-encing urinary pH. The results of one such ex-periment are shown in Table II. Systemic alka-losis per se had no effect on the excretion ofurobilinogen-8H.
Effect of urine flow on urobilinogen-3H excre-tion. The effect of varying urine flow whenurinary pH is held constant was studied in 6 dogsunder conditions of aciduria, and in three dogspassing alkaline urines (produced by either pro-longed hyperventilation or prefeeding NaHCO3).Increasing urinary flow rates were produced byinfusing increasing amounts of 3% urea in salineas an osmotic diuretic. When the urine was acidinitially, urinary pH fell 0.5 U below control val-ues in one experiment as the osmotic diuresisprogressed, increased up to 0.8 U in three experi-ments, and remained virtually constant in twoexperiments. When the dogs initially were passing
alkaline urines, the pH tended to fall slightly (upto 0.5 U) as the duiresis increased. The resultsobtained in all experiments of each type weresimilar. One representative experiment of eachtype is shown in Fig. 2. Under conditions ofaciduria, Cu/Ccr ratio increases markedly as urineflow increases up to 3-5%o of GFR, but tends tolevel off at flows beyond this rate. When the urineis alkaline variation in flow rate has no appreciableeffect on the Cu/Ccr ratio.
Effect of probenecid on urobilinogen-3H excre-tion. We attempted to demonstrate a transportmaximum (Tm) for urobilinogen by infusinglarge amounts of urobilinogen-3H under conditionsof alkaline diuresis, but we failed due to technicaldifficulties in preparing, handling, and infusinglarge amounts of carrier urobilinogen. It seemedof interest, therefore, to test the effect of pro-benecid,1 a potent inhibitor of the organic acid
1 Kindly supplied by Merck, Sharpe & Dohme, WestPoint, Pa.
2.4
1.60.8
.t
0.6
00.5
0.4
0.3
0.1
Alkaline Urine I
t t WkeFs F."~s pHI. aJ a
.I
iFI Acid Urine I
-.
tt f fU£44A4 54 Urine pH
0 I 2 3 4 5 10 15 2o0 25V/GfR MS
FIGURE 2 Effect of osmotic diuresis on urobilinogen-'Hexcretion. Each point represents a single clearanceperiod. The upper half of the figure shows an experimenttesting response to 3%o urea in saline when the urine wasalkaline. The lower part of the figure shows the responseto increasing urine flow during aciduria. The numberedarrows refer to urinary pH during each experiment.Lines through the points were drawn by inspection.
2120 M. Levy, R. Lester, and N. G. Levinsky
0
A 0
4f
r.4

TABLE II IFailure of Proximal Tubular Transport Inhibitors to Alter
Urobilinogen Excretion
Cu/Cer
Experiment Control Experimental
Probenecid (400-600 mg prime intravenously,then constant infusion of 12-18 mg/min)
1 0.89 0.792 0.74 0.783 0.90 0.934 0.85 1.005 0.81 0.936 0.86 0.74
Acetazolamide (500 mg intravenously)7 0.78 0.718 1.10 1.309 1.73 1.47
PAH (p-aminohippurate, 3 g prime intra-venously, then constant infusion of 30mg/min)
10 1.07 1.04
Cer, creatinine clearance. All other abbreviations as inTable I. Each value is the mean of 2-4 clearance periods.Periods were 6-10 min in length. Collections were begun7-20 min after drug was started. All periods were col-lected during alkaline diuresis induced by NaHCO3 in-fusion; the infusion was adjusted to maintain urinary pHconstant within ±0.2 U during the course of an experiment.
transport system of the proximal tubule. This wasdone in a total of six dogs during alkaline diuresisand with plasma levels of urobilinogen-8H whichvaried from 50 to 1200 ,ug/100 ml. There was nodemonstrable effect of probenecid in any experi-ment. Negative results were obtained in a few ex-periments under similar conditions with p-amino-hippurate and acetazolamide, also known to inhibitthe organic acid transport system. These experi-ments are summarized in Table III.
DISCUSSION
Previous studies have led to conflicting opinionsas to the renal mechanisms for the excretion ofurobilinogen. Using infusions of urobilin, Royerand Solari (2) concluded that urobilin and uro-bilinogen are excreted only by glomerular filtra-tion in the dog, and by filtration and tubularsecretion in man. Fassati, Fassati, and Andel (1)have recently claimed that glomerular filtrationalone accounts for urinary urobilinogen in man.
Our data in the dog support the studies of Bourkeet al. (3) in man concerning the mechanism ofurobilinogen excretion. They concluded that uro-bilinogen is handled by the kidney in a fashionanalogous to other weak organic acids, i.e., by acomplex process of filtration, tubular secretion(probably in the proximal tubule), and reabsorp-tion in the distal nephron by pH-dependent non-ionic back diffusion. Our studies show that whenthe urine is acid, urobilinogen excretion may beequivalent to as little as 30% of the filtered load.Under these conditions, increasing urine flow willincrease urobilinogen excretion two- to threefold.Increasing urine pH to alkaline values will convertnet reabsorption of urobilinogen into net secretion;in urines of maximal alkalinity, at least as muchurobilinogen may be secreted as is filtered. Underthese circumstances changes in urine flow do notaffect urobilinogen excretion.
This pattern of pH and flow dependence is bestexplained by the laws governing nonionic diffusion(6). Urobilinogen is a weak acid (Fig. 3) whosePK, has been estimated by Bourke et al. (3) tobe about 5.4. In acid urines, much of the urobilino-gen will exist in the nonionic form. According tothe principles of nonionic diffusion, the tubularepithelium is permeable to the nonionic form oforganic acids. Hence, tubular reabsorption of uro-bilinogen will occur along the concentration gra-dient established by water reabsorption. Whenurine flow is increased by an osmotic diuretic,tubular reabsorption is limited because both theintratubular concentration of urobilinogen and thetime available for back diffusion are decreased.In alkaline urines, most of the urobilinogen willexist in the ionic form. According to the principlesof nonionic diffusion, tubular epithelium is con-sidered to be impermeable to this molecularspecies. Hence, back diffusion of filtered andsecreted urobilinogen will be minimal, and theurobilinogen clearance will be greater than thatobserved when the urine is acid. Since the concen-tration of the diffusible nonionic species is in anycase minimal in alkaline urine, variations in urineflow can have little or no effect on back diffusionand clearance.
Nonionic diffusion by itself, however, cannotaccount for the net secretion of urobilinogen ob-served when the urine is alkaline. Many other
Renal Excretion of Urobilinogen 2121

0~~~~
0
I b
3r- 4)
0 ~ .=
0
0~~~~~~~~~~05-.4)'gSSZED ~~~~~Z5.
:; W I o-
zx O
i' 0 o.0
.0 4)
o 7 * .
a~~~~~
CC)I XbO.v0 ~~00
o.&.%i _U
S..4)
Sogzn[I
0~i~iI~zx 0c
.2E.o~~~~~~~~~hC4~ ~ ~ )C
C)~~~~~~~~~4~~~04 0
0~~~
2122 M. Levy, R. Lester, and N. G. Levinsky

weak organic acids have been shown to be activelysecreted, and studies suggest that a common secre-tory pathway may be present in the proximaltubule (7, 8). It would seem reasonable that thisproximal organic anion secretory mechanism mightbe the site at which urobilinogen is secreted.Hence, it was rather surprising that probenecid,acetazoleamide, and p-aminohippurate, known in-hibitors of this mechanism, had no influence onurobilinogen excretion in our studies. The dose ofprobenecid we used will depress salicylate excre-tion markedly (8). Bourke et al. (3) state that inman probenecid did inhibit urobilinogen secretion.However, these authors noted only a small re-sponse in one of three subjects studied, and theirresults seem inconclusive.The failure of probenecid to alter urobilinogen
excretion could be due to several causes. First, itcould be that urobilinogen is tightly and preferen-tially bound to the transport carrier and cannotbe dislodged by competitive inhibitors. Secondly,urobilinogen, an endogenous weak acid, might behandled by a separate transport system not inhib-ited by probenecid rather than by the probenecid-sensitive mechanism for exogenous organic acids.This is a distinct possibility, since recent unpub-lished studies by one of us (R.L.) have shownthat probenecid also fails to inhibit urobilinogenexcretion by the rat liver. Since Despopoulos andSonnenberg (9) have provided evidence that kid-ney and liver organic acid secretory pathwayscorrespond both as to the compounds transportedand in susceptibility to probenecid inhibition, itseems quite possible that urobilinogen is indeedsecreted by a different mechanism from that whichsecretes substances such as salicylates.
Finally, it is theoretically possible that weakacids might be secreted into the urine within therenal medulla by passive diffusion, if the concen-tration of nonionic urobilinogen in vasa rectaplasma were increased by concentration and in-creased acidity of the plasma. However, net secre-tion in some of our studies was equal to filteredload, i.e., equivalent to the total urobilinogen inabout 15%o of renal plasma flow.2 Since totalmedullary plasma flow is probably less than this
2 In the anesthetized dog, glomerular filtration is about30% of renal plasma flow, and approximately half ofthe plasma urobilinogen is not bound and hence filtrable.
(10), secretion in the medulla cannot account forthe maximum rates of secretion in our experi-ments.
Given the instability of the urobilinogen mole-cule it is conceivable that errors in the measure-ment of protein binding could spuriously accountfor net secretion. However, it would require enor-mous errors in the measurement of protein bindingto account for the observed ratios of Cu/Ccr ashigh as 2. This is most unlikely since two separatemethods, ultracentrifugation and ultrafiltration,gave very similar results for human serum in ourstudies. Moreover, the values we obtained werevery similar to those reported by Bourke et al.(3), who employed still a third method, equi-librium dialysis.We have made the not unreasonable assumption
in these experiments that the isotope used, meso-bilirubinogen-3H, is indeed a representative uro-bilinogen. Moreover, we measured only the ex-ogenous urobilinogen with our techniques. In thetracer experiments, total urobilinogen concentra-tion was roughly twice the probable physiologicallevels (3). Within these limitations, our resultshave an important clinical bearing. They demon-strate quite clearly that the urinary concentrationof urobilinogen may reflect not only plasma levels,but also renal function, rates of urine flow, andurinary pH. Varying amounts of urinary uro-bilinogen may be excreted in the face of constantplasma levels, if flow and pH are altered. In ourstudies, during steady states, the fraction of in-fused urobilinogen excreted in the urine increasedfrom 2-3% in acid urines to 12-14% when theurine was made alkaline. Similar changes in theproportion of endogenous urobilinogen excreted inthe urine may be anticipated. Therefore, clinicalmeasurements of urinary urobilinogen can be in-terpreted as an index of plasma urobilinogen onlyif urinary pH and flow are considered.
ACKNOWLEDGMENTS
We wish to acknowledge the technical assistance of Miss,Joanna Little and Mr. David Levinson, and the secre-tarial assistance of Mrs. Phyllis Tuttle.These studies were supported in part by U. S. Public
Health Service Grant Nos. AM09881, AM11793, andHE06795. Dr. Levy is supported by U. S. Public HealthService Traineeship No. AM05209. Dr. Lester is therecipient of U. S. Public Health Service Career Develop-ment Award 12,127.
Renal Excretion of Urobilinogen 2123

REFERENCES
1. Fassati, M., P. Fassati, and J. Andel. 1966. Vyluco-vanf urobilinogenu ledvinami (Renal excretion of uro-bilinogen). Casopis Lekaru. Ceskych. 105: 640.
2. Royer, M., and A. V. Solari. 1941. Depuracionplasmatica de la urobilina. Rev. Soc. Arg. Biol. 17:329.
3. Bourke, E., M. D. Milne, and G. S. Stokes. 1965.Mechanism of renal excretion of urobilinogen. Brit.Med. J. 2: 1510.
4. Lester, R., and P. D. Klein. 1966. Bile pigment excre-tion: a comparison of the biliary excretion of bili-rubin and bilirubin derivatives. J. Clin. Invest. 45:1839.
5. Klein, P. D., and R Lester. 1966. The introductionof tritium into bile pigments. The Second Eur-
atom Conference on Preparation and Storage ofLabelled Molecules, Brussels. In press.
6. Milne, M. D., B. H. Scribner, and M. A. Crawford.1958. Non-ionic diffusion and the excretion of weakacids and bases. Am. J. Med. 24: 709.
7. Weiner, I. M., and G. H. Mudge. 1964. Renaltubular mechanisms for excretion of organic acidsand bases. Am. J. Med. 36: 743.
8. Weiner, I. M., J. A. Washington, and G. H. Mudge.1959. Studies on the renal excretion of salicylate inthe dog. Bull. Johns Hopkins Hosp. 105: 284.
9. Despopoulos, A., and H. Sonnenberg. 1967. Con-gruence of excretory functions of liver and kidney:sulfonamides. Am. J. Physiol. 212: 1117.
10. Thurau, K 1964. Renal haemodynamics. Am. J.Med. 36: 698.
2124 M. Levy, R. Lester, and N. G. Levinsky














![URINARY EXCRETION OF ALBUMIN - nephro-necker.org · urinary excretion of albumin ... tojo and endou [12], ... 105, 1353-1361 2000. renal albumin handling in megalin knock out mice](https://static.fdocuments.net/doc/165x107/5c4a0c7693f3c317653c31ff/urinary-excretion-of-albumin-nephro-urinary-excretion-of-albumin-tojo.jpg)


