RENAL DISEASES IN PREGNANCY Professor Hassan Nasrat Faculty of Medicine King Abdul-Aziz University.
30
RENAL DISEASES IN PREGNANCY Professor Hassan Nasrat Faculty of Medicine King Abdul-Aziz University
Transcript of RENAL DISEASES IN PREGNANCY Professor Hassan Nasrat Faculty of Medicine King Abdul-Aziz University.
RENAL DISEASES IN PREGNANCY
Professor Hassan Nasrat
Faculty of Medicine
King Abdul-Aziz University
Physiological changes in renal system and its clinical implications.
Common urinary tract diseases in pregnancy.
Pregnancy in women with chronic kidney disease.
Acute renal injury (failure) in pregnancy.
Anatomic Changes
Functional Changes:
oImaging studies Increases in size and weight due to increased renal vasculature. Also physiological hydro-ureter and hydronephorosis.
oStasis and vesico-eretric reflux increase risk of urinary tract infection in pregnancy.
The Effective Renal plasma flow (ERPF):
The Glomerular filtration rate (GFR):
The filtration fraction:
The kidneys:
The ureters:
The Bladder:
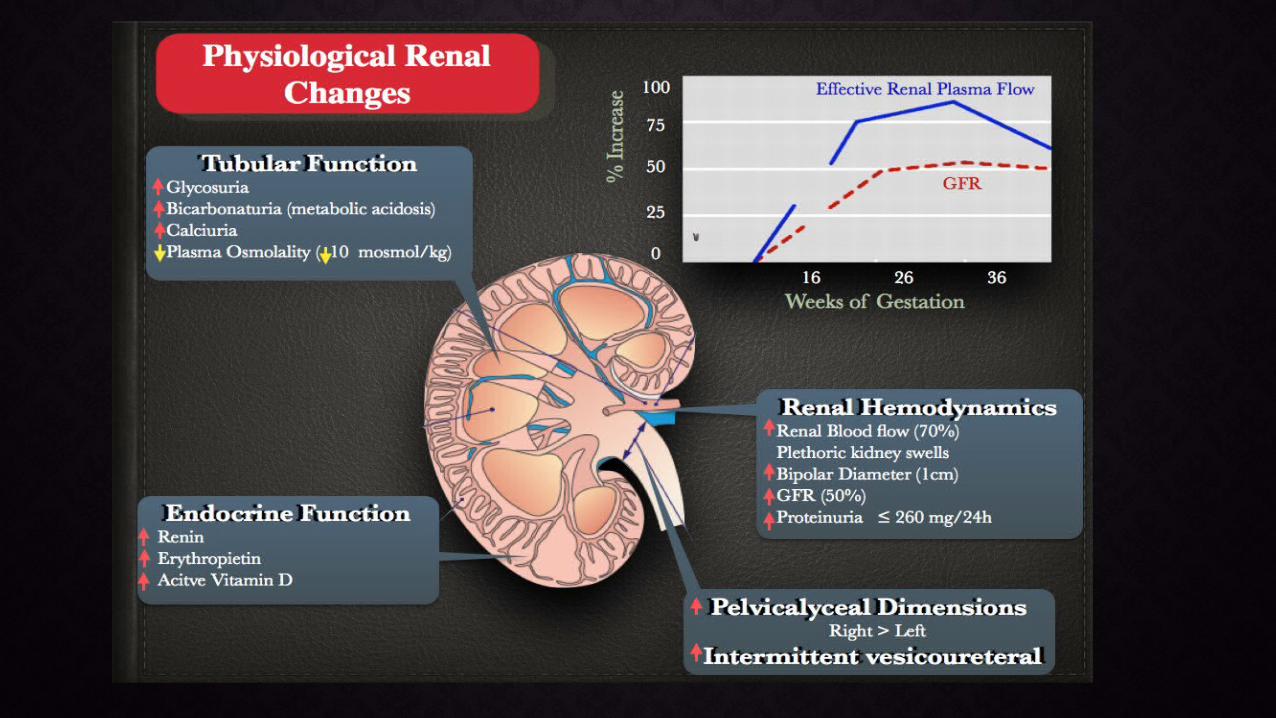
Glucose: In pregnancy glucosuria does not necessary indicate hyperglycemia i.e. it is not correlated with the blood glucose level.
Proteinuria: Increased protein loss. Loss of more that 300 mg of protein/24hours is abnormal
Reduction in maternal plasma levels of creatinine, blood urea nitrogen (BUN) and uric acid.
Serum Creatinie: falls by an average of 0.4 mg/dL (35 micromol/L) to a normal range of 0.4 to 0.8 mg/dL (35 to 70 micromol/L)
Blood urea nitrogen (BUN) levels fall to approximately 8 to 10 mg/dL (2.9 to 3.9 mmol/L)
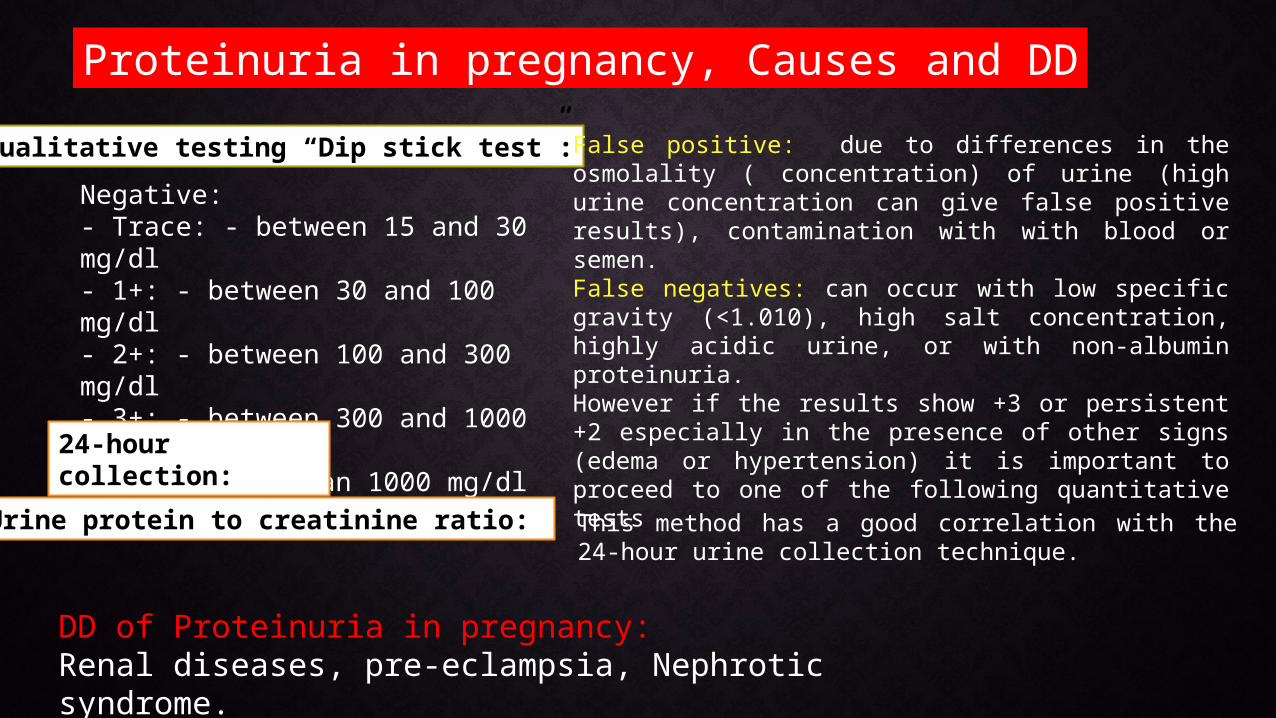
Proteinuria in pregnancy, Causes and DD
Qualitative testing “Dip stick test”:
Negative:- Trace: - between 15 and 30 mg/dl- 1+: - between 30 and 100 mg/dl- 2+: - between 100 and 300 mg/dl- 3+: - between 300 and 1000 mg/dl- 4+: - more than 1000 mg/dl
False positive: due to differences in the osmolality ( concentration) of urine (high urine concentration can give false positive results), contamination with with blood or semen. False negatives: can occur with low specific gravity (<1.010), high salt concentration, highly acidic urine, or with non-albumin proteinuria.However if the results show +3 or persistent +2 especially in the presence of other signs (edema or hypertension) it is important to proceed to one of the following quantitative tests24-hour
collection:
This method has a good correlation with the 24-hour urine collection technique.
Urine protein to creatinine ratio:
DD of Proteinuria in pregnancy:Renal diseases, pre-eclampsia, Nephrotic syndrome.
Asymptomatic Bacteriuria.
Cystitis.
Pyelonephritis.
Urinary Tract Infection in pregnancy
Factors that increase women susceptibility to UTI inpregnancy:
1. Impaired complete emptying of
2. the bladder (Increased residual volume).
3. Increase vesicoureteric reflux.
4. The physiological glucosuria.
5. Urine alkalinity.
Definition: A significant bacterial colonization of the urinary tract without symptoms.
Incidence: 4-7% same among pregnant and non-pregnant women. But in pregnancy the complications rate is more, it include:
oPyelonephritis In About 30 % Of Cases.oRisk Of Preterm Labor, Premature Rupture Of Membrane.oLow Birth Weight Infants.
Screening for ASB is part of effective intervention for all women in their first antenatal visit by culture of a midstream sample of urine (MSU).
Treatment: according to the culture and sensitivities results increase the fluid intake. Follow up culture after 2 weeks.
significant bacterial colonization : > 100,000 colonies/ml of a single bacterial organism in culture from a clean catch voided sample of urine.
Asymptomatic Bacteriuria
Definition: Acute bacterial cystitis presents with clinical signs and symptoms of urgency, frequency, dysuria, pyuria, and hematuria without evidence of systemic illness. It affect
Frequency:1% to 4% of all pregnancies.
The treatment: regiment is the same as in ASB.
Follow-up surveillance, including monthly urine cultures for the duration of the pregnancy, is recommended.
Uretheral Syndrome often due to Chlamydia infection is suspected in women symptoms consistent with cystitis but with a negative urine culture.
Cystitis
Incidence: 1-2 %. Rt > Lt.
The risk factors: ASB, previous history of pyelonephritis, urinary tracts malformations and calculi.
Complications:
Maternal: bacterial endotoxemia, can lead to endotoxic shock, adult Respiratory Distress Syndrome (ARDS), hemolytic anemia and permanent damage to of renal tissues.
Fetal: preterm labor, premature rupture of membranes (PROM) and fetal growth restriction (IUGR).
Acute Pyelonephritis
The diagnosis• Systemic signs and symptoms: fever; dysuria, costovertebral angle tenderness (CVAT); shaking chills; nausea and vomiting.• midstream urine (MSU) culture: Positive culture, in addition to of pyuria or leukocyte casts.The treatment: • Hospitalization.• Parenteral antimicrobial therapy (to be changed to oral route
once the patient is a-febrile).• Adequate intravenous hydration and close monitoring of urine
output.• Antipyretics and analgesics.
Investigations: Sonosgraphy: If there is no clinical improvement by 48 to 72 hrs. blood and urine samples: for culture and sensitivity. Complete blood count and serum chemistry.
Acute Pyelonephritis
Definition: Acute Renal Failure (ARF) is a sudden decrease in renal function
Diagnosis:
Rapid increase in serum creatinine levels (of at least 0.5 mg/dL/day (44 μmol/L/day).
And oliguria with urine output of less than 400 mL in 24 hours (20% of the patients maintain normal urine volumes).
Incidence: Rare he incidence of ARF that require dialysis is less than 1 in 10,000 - 15,000 pregnancies.
Acute Renal Failure (ARF) in pregnancy
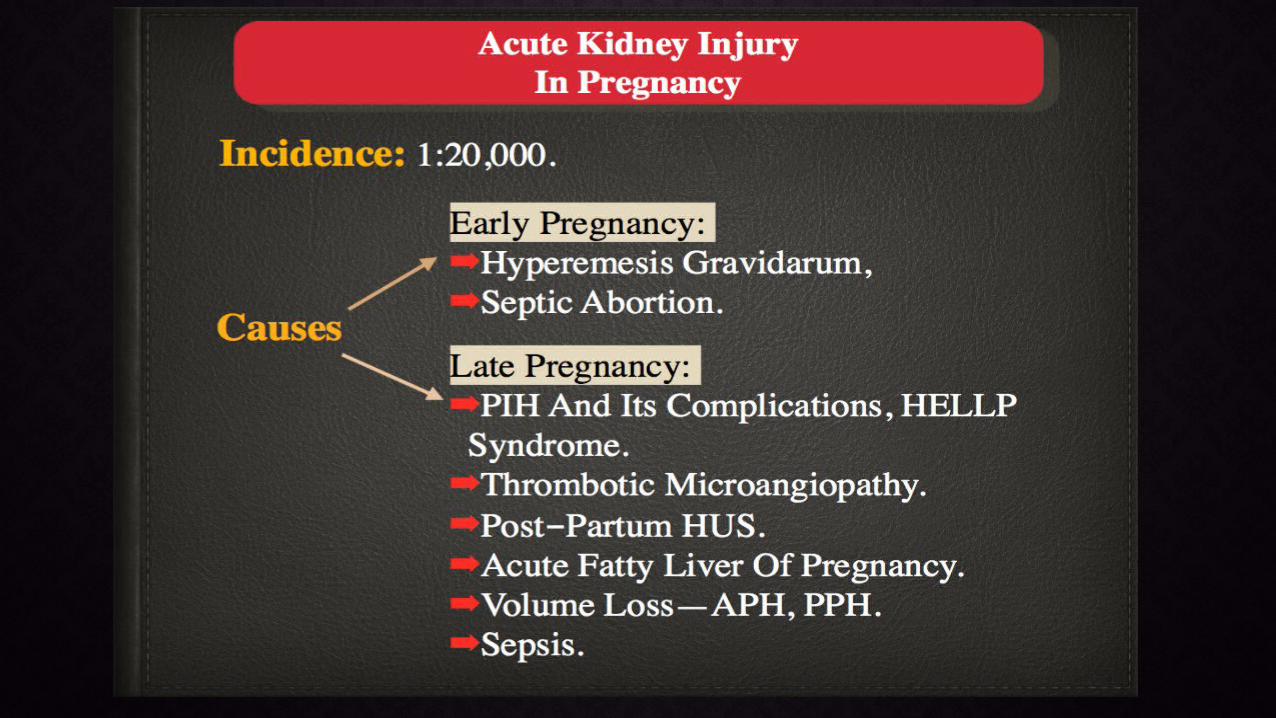
Preeclampsia and Eclampsia: Although rare event, but contributes significantly to obstetric causes of ARF. The picture is similar to acute tubular necrosis and recovery of renal function is the rule.
Severe Hemorrhage:
Abruptio placenta, amniotic fluid embolism, and retained dead fetus:
Hemolytic-Uremic Syndrome (HUS): This unusual cause of ARF can develop following several precipitating events including infections, pregnancy, and certain drugs.
It occurs 7-10 days after a seemingly normal pregnancy. There is microangiopathic hemolytic anaemia, thrombocytopenia, with variable degree of neurologic symptoms.
The prognosis of this disease is generally poor (61% mortality rate for cases reported prior to 1979). Recently it has markedly been improved with plasma exchange using plasmapheresis.
Acute Fatty liver of Pregnancy:
High mortality rate: that ranges from 20% to 60%, mostly from the underlying cause e.g. sepsis and hemorrhage.Development of chronic renal failure: bilateral renal cortical necrosis (BRCN). This complication is particularly common with abruptio placenta. Some patients might have slow recovery of the renal function for up to 3 years after the onset and can achieve a satisfactory lifestyle without dialysis.
Complications of ARF
• The effect of the pregnancy on the kidneys function:
• The effect of the kidney disease on the pregnancy:
This depends on:
1. The cause of renal disease (e.g. diabetes, SLE ...etc.)
2. The renal function at the time of conception.
Pregnancy with chronic Renal Disease (Failure)
1. Does pregnancy jeopardize the graft?
2. What are the criteria that must be fulfilled before a transplanted patient is allowed to get pregnant?
3. What is the effect of medication i.e. immunosuppressive therapy on the fetus?
Pregnancy after Renal Transplant
The general advice are:
pregnancy should be deferred for 1 - 2 years after transplantation with General good health.
No proteinuria.
No significant hypertension.
No evidence of graft rejection.
Serum creatinine < 2 mg/dl.
Drug therapy <= 10 mg prednisone and <= 3 mg /kg azathioprine.
Pregnancy after Renal Transplant
Studies have shown that pregnancy does not seem to increase the rate of graft rejection in patients who fulfill the required criteria for pregnancy after transplant. However the management of such patients requires a highly specialized multidisciplinary team.
In pregnancy the potential risks are:•Increased risk of developing pre-eclampsia.•Increased risk of contracting infections (being on immunosuppressant drugs).
Labor:Delivery is normal (the transplanted kidney rarely obstructs normal labor and delivery). Cesarean section should only be undertaken for obstetric reasons.
Pregnancy after Renal Transplant
Incidence “ urinary calculi” varies between 0.03 and 0.35 %.
The condition is considered a serious pathology that can lead to permanent parenchymatous damage if not properly treated, in addition to the risk of serious systemic infection.
The diagnosis can be difficult and a high index of suspicion is needed. Ultrasound scan is not very helpful in the late pregnancy.
In the mean time there is usually hesitancy in using radiological examination. However if used judiciously it is not contraindicated.
The management depends on several factors such as the degree of obstruction, the presence or absence of infection, the general condition of the patient and the stage of pregnancy.
Although medical intervention is often tried first, surgical intervention is not contraindicated.
Urinary Calculi (Urolithiasis)
Thanks