Renal Denervation Therapy: Anxiolytic for nervous … Graham - Renal Denervation- SMH Day... ·...
36
Renal Denervation Therapy: Anxiolytic for nervous kidneys John J. Graham MBChB MRCP(UK) Interventional Cardiologist, St. Michael’s Hospital Assistant Professor, University of Toronto
-
Upload
phungkhanh -
Category
Documents
-
view
219 -
download
0
Transcript of Renal Denervation Therapy: Anxiolytic for nervous … Graham - Renal Denervation- SMH Day... ·...

Renal Denervation Therapy: Anxiolytic for nervous kidneys
John J. Graham MBChB MRCP(UK)
Interventional Cardiologist, St. Michael’s HospitalAssistant Professor, University of Toronto

OBJECTIVES•Outline problem of hypertension and treatment resistance•Introduce renal denervation therapy (RDN) and evidence for its use•Potential future indications for RDN (other disorders with ‘nervous’ kidneys•Intersperse with clinical scenarios

• 73 y.o. male
• Referred for HTN management
• Multiple CV risk factors
• Type II DM
• Dyslipidemia
• Sedentary
• 20+ year history of HTN
• CKD - creatinine 160 - 200umol/L
Patient

• Adherent with 8 medications: Acebutolol 400mg bid, Doxazosin 16mg qhs, Verapamil MR 240mg od, Clonidine 0.2mg tid, Enalapril 20mg bid, HCTZ 25mg od, Losartan 100mg od, Aliskiren 300mg od.
• BP 180/110 - repeated testing
• Rest of examination normal
Initial Assessment

What would you do?
A. Refer for further investigation to R/O secondary causes
B. Refer for RDN
C. Add spironolactone
D. All of the above

Hypertension
• Major healthcare burden
• Causative risk factor:
• stroke, ischemic heart disease, CHF, CKD
• Increased mortality rates
• Cardiovascular and all cause
• Affects 25% of global population
• Responsible for 7,000,000 p.a. (13% of global mortality)
WHO. Global health risks: Mortality and burden of disease attributable to selected major risks. 2009:1-‐ 62
Fagard RH. Resistant hypertension. Heart. 2012;98:254-‐261

Hypertension
• Increasingly recognised problem
• Recent Canadian study
• 26 million Canadians over nine-‐year period
• ↑ prevalence from 12.5% to 19.6%
• Higher all-‐cause mortality in patients with HTN (HR 1.9-‐4.2)
Robitaille C, et al. Diagnosed hypertension in canada: Incidence, prevalence and associated mortality. CMAJ : 2012;184:E49-‐56

Resistant Hypertension
• Recognised for some time
• Gifford & Tarazi (1978): “the failure to control blood pressure adequately (arbitrarily <150/100 mmHg) with a good regimen, provided that medications are taken as prescribed”
• Recent tightening of definition
• Above-target BP despite compliance with three different anti-hypertensive agents - at adequate dosage and including a diuretic

Resistant Hypertension• Increasingly recognised as a problem
• Incidence 1.9% in newly diagnosed hypertensives after 1.5 years treatment
• Prevalence up to 15% hypertensive patients
• Poor prognosticator
• After 3.8 years, presence of RH associated with increased risk of adverse events (HR1.47, 95% CI, 1.33-1.62,
Daugherty SL, et al. Incidence and prognosis of resistant hypertension in hypertensive patients. Circulation. 2012;125:1635-‐1642

Secondary HypertensionCauses to be excluded
• Renovascular disease
• Hyperaldosteronism
• Glucocorticoid excess
• Phaeochromocytoma
• Hyperthyroid/parathyroid
• Obstructive sleep apnea
• Medications (illicit/precsribed
• Aortic coarctation
• Renal parenchymal diseaseCalhoun et al. Hypertension. 2008;51:1403-1419

Renovascular Disease• 43y.o. male
• Dyslipidemic, smoker, +ve FHx CAD
• Approx 3 year history ↑BP
• Persisting despite increasing numbers/doses anti-hypertensives
• 3x admissions with hypertensive crises and symptoms CHF
• Duplex USS of renal arteries
• Inconclusive due to body habitus
• Referred for consideration of RDN

Anatomic suitability

Further Evaluation
Captopril MAG3 ScanRight Kidney - 82% uptake
Left - 18% uptake

Hyperaldosteronism
•5-12% of patients with presumed essential hypertension, 23-26% of patients with resistant hypertension
•Patients tend to be normokalemic
•Spironolactone is useful adjunct in patients with resistant hypertension

Sympathetic Activity in HTN
Esler et al, Clin Exp Hypertens 1989

Renal Sympathetic Innervation
• Ipsilateral paravertebral sympathetic ganglia T11 - L3
• Enter the kidneys with the renal arteries and spread through the parenchyma following the blood vessels

Renal Sympathetic Innervation
Cutting of the greater splanchnic nerve resulted in the ureter becoming distended with urine....Stimulation of the ends of the greater splanchnic nerve and urine flow ceases”
Claude Bernard 1859

Renal Sympathetic Innervation

6757
[FEB. 28, 1953ORIGINAL ARTICLES
SYMPATHECTOMY IN THE TREATMENTOF HYPERTENSION
REVIEW OF 122 CASES
D. M. MORRISSEYM.Ch. N.V.I., F.R.C.S.
LECTURER IN SURGERY, UNIVERSITY OF BIRMINGHAM ;ASSISTANT SURGEON, QUEEN ELIZABETH HOSPITAL, BIRMINGHAM
VICTOR S. BROOKESM.B. Birm., F.R.C.S.
SENIOR REGISTRAR, QUEEN ELIZABETH HOSPITAL
W. T. COOKEM.D. Camb., F.R.C.P.
READER IN MEDICINE, UNIVERSITY OF BIRMINGHAM
Tms paper reviews the results of thoracolumbarsympathectomy in 122 patients with hypertension treatedat the Queen Elizabeth Hospital, Birmingham, between1943 and 1951. All except 2, who were untraced aftera year, have been seen and examined regularly. Up to1947 a limited sympathectomy was performed, usingtechniques similar to those described by Peet et al.(1940) and Smithwick (1940) ; but from then onwardsthe more extensive resection associated with Grimson(1941) was done. The two series are not strictly com-parable ; but, when some additional information isthereby gained, separate analyses have been made.
TABLE I-GROUP, SEX, AND TYPE OF OPERATION IN 113PATIENTS SURVIVING OPERATION
In classifying the patients the system described byHammarstrom and Bechgaard (1950) has been adoptedas being more convenient than the more complicatedone of Smithwick (1951) or the method of Keith et al.(1939), which is based mainly on an accurate but personalassessment of retinal changes.
Investigation and Classification of CasesRoutine investigations included intravenous pyelo-
graphy, estimation of the blood-urea, analysis and con-centration tests of urine, electrocardiography, radio-graphy of the chest, and ophthalmoscopy. In somecases early in the series inulin and diodone clearanceswere estimated. Much interest centred at one stage onthe demonstration of the hypotensive effects of amylo-barbitone, tetraethylammonium bromide, sympatheticblockade by local anaesthetics, and vasodilation byvarious pyrogens. These tests were gradually abandonedwhen it was found that they added little to the informa-tion gained by recording the blood-pressure hourly fortwenty-four hours and had no prognostic value.
TABLE II——AGE-DISTRIBUTION Iw’ 113 PATIENTS SURVIVING
OPERATION
According to the results of these investigations thepatients were divided into four groups (Hammaratromand Bechgaard 1950) as follows :Group l.-Hypertension, with no secondary vascular
complications, and either no subjective symptoms or onlyslight symptoms.Group 2.-Hypertension. Marked subjective symptoms.
No signs of myocardial damage or vascular change. Leftaxis-deviation on electrocardiography and/or a relativeenlargement of the left ventricle, and heart volume radio-graphically within normal limits. Retinal changes grade I
or II (Keith et al. 1939).Group 3.-Hypertension, with subjective symptoms and/or
signs of secondary vascular complications-i.e., retinalgrade-in changes (Keith et al. 1939), including retinalhaemorrhages with or without thrombosis of the retinalvessels, or retinae grade I or II with one or more of the
TABLE III-DISTRIBUTION OF SECONDARY VASCULAR MANI-
FESTATIONS IN 64 GRoup-3 CASES
following : negative T wave in the electrocardiogram ; heartvolume above predicted normal (transverse diameter greaterthan half the thoracic diameter) ; residual damage to centralnervous system after cerebral accident ; or albuminuria.
Grmtp 4.-Hypertension, with retinal exudates and
papillcedema grade IV (Keith et al. 1939).The composition of each group is further analysed by
sex and age in tables i and 11.Essentially, group 3 contains all the patients with
evidence of secondary vascular damage of the retinal,cerebral, cardiac, or renal vessels. Many had involve-ment of more than one system, and it will be noted(table 111) that coronary and renal damage was associatedwith the highest mortality since operation.TABLE IV-PREOPERATIVE BLOOD-PRESSURES IN 113 PATIENTS
SURVIVING OPERATION
ESTIMATIONS OF BLOOD-PRESSURE
A very large series of preoperative blood-pressurereadings was collected for each patient, and the selectionof a figure which could be called " the blood-pressure "for each case was a most difficult task. We took the viewthat the occasional very high or very low figure in therecords of most patients had little value for comparisonwith " casual " follow-up figures, since our patientswere not readmitted for serial postoperative blood-
pressure readings. We have therefore chosen as the
preoperative level in each case the resting recumbentpressure taken on the second or third day in hospital.Table iv gives the preoperative diastolic and systoliclevels in the 113 cases available for observation.
I
6757
[FEB. 28, 1953ORIGINAL ARTICLES
SYMPATHECTOMY IN THE TREATMENTOF HYPERTENSION
REVIEW OF 122 CASES
D. M. MORRISSEYM.Ch. N.V.I., F.R.C.S.
LECTURER IN SURGERY, UNIVERSITY OF BIRMINGHAM ;ASSISTANT SURGEON, QUEEN ELIZABETH HOSPITAL, BIRMINGHAM
VICTOR S. BROOKESM.B. Birm., F.R.C.S.
SENIOR REGISTRAR, QUEEN ELIZABETH HOSPITAL
W. T. COOKEM.D. Camb., F.R.C.P.
READER IN MEDICINE, UNIVERSITY OF BIRMINGHAM
Tms paper reviews the results of thoracolumbarsympathectomy in 122 patients with hypertension treatedat the Queen Elizabeth Hospital, Birmingham, between1943 and 1951. All except 2, who were untraced aftera year, have been seen and examined regularly. Up to1947 a limited sympathectomy was performed, usingtechniques similar to those described by Peet et al.(1940) and Smithwick (1940) ; but from then onwardsthe more extensive resection associated with Grimson(1941) was done. The two series are not strictly com-parable ; but, when some additional information isthereby gained, separate analyses have been made.
TABLE I-GROUP, SEX, AND TYPE OF OPERATION IN 113PATIENTS SURVIVING OPERATION
In classifying the patients the system described byHammarstrom and Bechgaard (1950) has been adoptedas being more convenient than the more complicatedone of Smithwick (1951) or the method of Keith et al.(1939), which is based mainly on an accurate but personalassessment of retinal changes.
Investigation and Classification of CasesRoutine investigations included intravenous pyelo-
graphy, estimation of the blood-urea, analysis and con-centration tests of urine, electrocardiography, radio-graphy of the chest, and ophthalmoscopy. In somecases early in the series inulin and diodone clearanceswere estimated. Much interest centred at one stage onthe demonstration of the hypotensive effects of amylo-barbitone, tetraethylammonium bromide, sympatheticblockade by local anaesthetics, and vasodilation byvarious pyrogens. These tests were gradually abandonedwhen it was found that they added little to the informa-tion gained by recording the blood-pressure hourly fortwenty-four hours and had no prognostic value.
TABLE II——AGE-DISTRIBUTION Iw’ 113 PATIENTS SURVIVING
OPERATION
According to the results of these investigations thepatients were divided into four groups (Hammaratromand Bechgaard 1950) as follows :Group l.-Hypertension, with no secondary vascular
complications, and either no subjective symptoms or onlyslight symptoms.Group 2.-Hypertension. Marked subjective symptoms.
No signs of myocardial damage or vascular change. Leftaxis-deviation on electrocardiography and/or a relativeenlargement of the left ventricle, and heart volume radio-graphically within normal limits. Retinal changes grade I
or II (Keith et al. 1939).Group 3.-Hypertension, with subjective symptoms and/or
signs of secondary vascular complications-i.e., retinalgrade-in changes (Keith et al. 1939), including retinalhaemorrhages with or without thrombosis of the retinalvessels, or retinae grade I or II with one or more of the
TABLE III-DISTRIBUTION OF SECONDARY VASCULAR MANI-
FESTATIONS IN 64 GRoup-3 CASES
following : negative T wave in the electrocardiogram ; heartvolume above predicted normal (transverse diameter greaterthan half the thoracic diameter) ; residual damage to centralnervous system after cerebral accident ; or albuminuria.
Grmtp 4.-Hypertension, with retinal exudates and
papillcedema grade IV (Keith et al. 1939).The composition of each group is further analysed by
sex and age in tables i and 11.Essentially, group 3 contains all the patients with
evidence of secondary vascular damage of the retinal,cerebral, cardiac, or renal vessels. Many had involve-ment of more than one system, and it will be noted(table 111) that coronary and renal damage was associatedwith the highest mortality since operation.TABLE IV-PREOPERATIVE BLOOD-PRESSURES IN 113 PATIENTS
SURVIVING OPERATION
ESTIMATIONS OF BLOOD-PRESSURE
A very large series of preoperative blood-pressurereadings was collected for each patient, and the selectionof a figure which could be called " the blood-pressure "for each case was a most difficult task. We took the viewthat the occasional very high or very low figure in therecords of most patients had little value for comparisonwith " casual " follow-up figures, since our patientswere not readmitted for serial postoperative blood-
pressure readings. We have therefore chosen as the
preoperative level in each case the resting recumbentpressure taken on the second or third day in hospital.Table iv gives the preoperative diastolic and systoliclevels in the 113 cases available for observation.
I

Renal Arteries as Therapeutic Target

Symplicity HTN-1
Initial Cohort – Reported in the Lancet, 2009:-First-in-man, non-randomized-Cohort of 45 patients with resistant HTN (SBP ≥160 mmHg on ≥3 anti-HTN drugs, including a diuretic; eGFR ≥ 45 mL/min) - 12-month data
Expanded Cohort* – This Report (Symplicity HTN-1):-Expanded cohort of patients (n=153)-36-month follow-up

Demographics Age (years) 57 ± 11
Gender (% female) 39%
Race (% non-Caucasian) 5%
Co-morbidities Diabetes Mellitus II (%) 31%
CAD (%) 22%
Hyperlipidemia (%) 68%
eGFR (mL/min/1.73m2) 83 ± 20
Blood Pressure Baseline BP (mmHg) 176/98 ± 17/15
Number of anti-HTN meds (mean) 5.1 ± 1.4
Diuretic (%) 95%
Aldosterone blocker(%) 22%
ACE/ARB (%) 91%
Direct Renin Inhibitor 14%
Beta-blocker (%) 82%
Calcium channel blocker (%) 75%
Centrally acting sympatholytic (%) 33%
Vasodilator (%) 19%
Alpha-1 blocker 19%
Baseline Characteristics
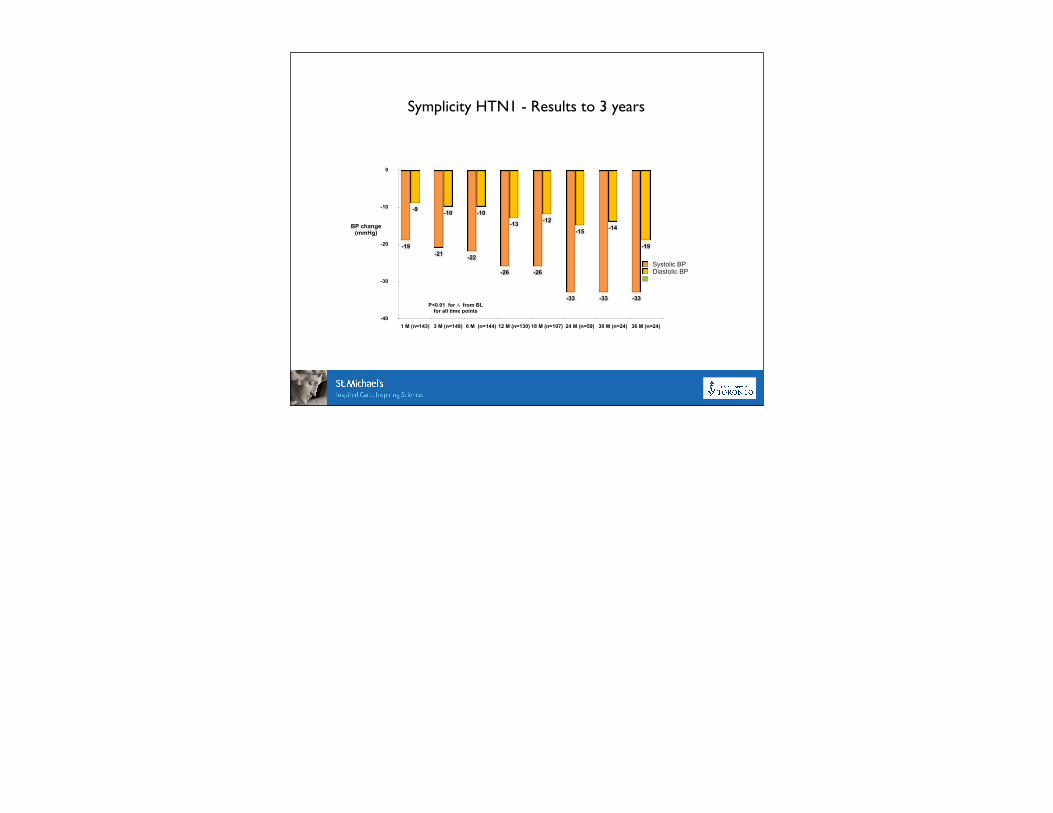
Symplicity HTN1 - Results to 3 years
-40
-30
-20
-10
0
1 M (n=143) 3 M (n=148) 6 M (n=144) 12 M (n=130) 18 M (n=107) 24 M (n=59) 30 M (n=24) 36 M (n=24)
-19
-14-15
-12-13
-10-10-9
-33-33-33
-26-26
-22-21-19
Systolic BPDiastolic BP
BP change(mmHg)
P<0.01 for ∆ from BLfor all time points

Increased Responders with Time
0%
25%
50%
75%
100%
1 Mo 3 Mo 6 Mo 12 Mo 18 Mo 24 Mo 30 Mo 36 Mo
100%
92%90%
81%79%
71%74%69%
Responder was defined as an office SBP reduction ≥ 10 mmHg
(n=143) (n=148) (n=144) (n=130) (n=107) (n=59) (n=24) (n=24)

Symplicity HTN-2
Lancet. 2010;376:1903-1909.

Symplicity HTN-2Inclusion Criteria:
– Office SBP ≥ 160 mmHg (≥ 150 mmHg with type II diabetes mellitus)
– Stable drug regimen of 3+ more anti-HTN medications
– Age 18-85 years
Exclusion Criteria:– Hemodynamically or anatomically significant renal
artery abnormalities or prior renal artery intervention – eGFR < 45 mL/min/1.73m2 (MDRD formula)– Type 1 diabetes mellitus– Contraindication to MRI– Stenotic valvular heart disease for which reduction of
BP would be hazardous– MI, unstable angina, or CVA in the prior 6 months
• Treatment-resistant HTN population
• BL OBP 178/97 mmHg• 49 RDN, 51 Control
• Age 58 years• BMI 31 kg/m²
• 40% with Diabetes• eGFR 77*
• Avg # meds 5.2• RDN and Control groups
generally well-matched

Baseline Medications RDN
(n=52)Control(n=54) p-value
Number Anti-HTN medications 5.2 ± 1.5 5.3 ± 1.8 0.75
% patients on HTN meds >5 years 71% 78% 0.51
% percent patients on ≥5 medications 67% 57% 0.32
% patients on drug class:
ACEi/ARB 96% 94% >0.99
Direct renin inhibitor 15% 19% 0.80
Beta-adrenergic blocker 83% 69% 0.12
Calcium channel blocker 79% 83% 0.62
Diuretic 89% 91% 0.76
Aldosterone antagonist 17% 17% >0.99
Vasodilator 15% 17% >0.99
Alpha-1 adrenergic blocker 33% 19% 0.12
Centrally acting sympatholytic 52% 52% >0.99

Symplicity HTN2 - extended follow up
-40
-30
-20
-10
0
10
RDN (n = 49) Control (n = 51)
0
-12
1
-32
∆ from Baseline to
6 Months (mmHg)
Primary Endpoint:•84% of RDN patients had ≥10 mmHg reduction in SBP•10% of RDN patients had no reduction in SBP
Systolic
Diastolic
Systolic Diastolic
RDN (n= 47)
∆ from Baseline to
12 Months (mmHg)
Systolic
Diastolic
Primary Endpoint (6M post Randomisation)
Latest Follow-up(12M post Randomisation)
Latest Follow-up:•Control crossover (n = 35): -24/-8 mmHg (Analysis on patients with SBP ≥ 160 mmHg at 6 M)
p <0.01 for Δ from baseline
p <0.01 for difference between RDN and Control

RDNBaseline
RDN6 Months
ControlBaseline
Control6 Months
45%35%
0%
6%
39%
31%61%
0%
12%
51%
18%
4%0%
43%
10%
< 140 mmHg140-159 mmHg160-179 mmHg≥ 180 mmHg

‘Nervous’ Kidney Disorders
• Hyperglycemia
• Obstructive sleep apnea
• Congestive heart failure
• CKD - hemodialysis

Sympathetic Activity in Human Heart Failure
Hasking et al, Circulation 1985

St. Michael’s Experience
• Resistant hypertension clinic established
• Input from cardiology/nephrology
• Patients undergo thorough evaluation
• 24hr ABPM
• Imaging - renal/cardiac MRI
• Approximately 20-25% of those referred go forward to RDN

St. Michael’s Experience
• Province-wide study
• Efficacy, economic evaluation
• Early versus delayed RDN
• Co-ordinated through Applied Health Research Centre
• Imminently enrolling patients

• Recent assessment
• Now on 5 medications - stopped aliskiren, doxazosin, enalapril
• Recent office BP - 134/80 (lowest recorded BP in >10 years)
Patient

Summary
• Hypertension is becoming commoner and is a major healthcare burden
• Resistant hypertension is increasingly recognised and is associated with worse outcomes
• Renal sympathetic overactivity is implicated in HTN (and other common conditions)
• Percutaneous attenuation of renal sympathetic activity is possible and offers an effective treatment option for patients with resistant hypertension

Thank you
• Resistant hypertension referrals:
• Tel: 416-864-5846/5399
• Fax: 416-864-5914