1 Renal Physiology PART ONE Renal Physiology overview PART TWO Renal Physiology details.

of 35
Upload
riccardo-mason-troiaCategory
view
224download
0description
Renal PhysiologyD. C. MikuleckyFaculty Mentoring ProgramVirginia Commonwealth Univ.
FUNCTIONS OF THE KIDNEYWater balanceElectrolyte balancePlasma volumeAcid-base balanceOsmolarity balanceExcretionHormone secretion
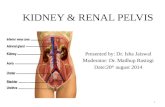
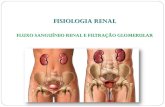
THE URINARY SYSTEMKidneysBlood supply: Renal arteries and veinsUreterUrinary bladderUrethra
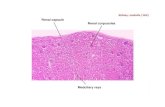
THE NEPHRON IS THE FUNCTIONAL UNIT OF THE KIDNEYBowmansCapsuleGlomerulusProximal ConvolutedTubuleDistal ConvolutedTubule
Loop of Henle CortexMedullaArteryVeinPeritubular CapillariesCollectingDuct
THREE BASIC RENAL PROCESSESGlomerular Filtration: Filtering of blood into tubule forming the primitive urineTubular Reabsorption: Absorption of substances needed by body from tubule to bloodTubular Secretion: Secretion of substances to be eliminated from the body into the tubule from the blood
BASIC RENAL PROCESSES
GFTRTAUrine ExcretedEfferent ArterioleAfferentArterioleGlomerulusKidneyTubulePeritubular Capillary
Glomerular FiltrationFirst step in urine formation180 liters/day filteredEntire plasma volume filtered 65 times/dayProteins not filtered
Forces Involved inGlomerular Filtration
Glomerular CapillaryBlood Pressure+55Plasma Colloid Osmotic Pressure-301510Bowmans CapsuleHydrostatic Pressure -Net Filtration Pressure+
Tubular ReabsorptionWater: 99% reabsorbed
Sodium: 99.5% reabsorbed
Urea: 50% reabsobed
Phenol: 0% reabsorbed
Tubular ReabsorptionBy passive diffusion
By primary active transport: Sodium
By secondary active transport: Sugars and Amino Acids
Tubular Reabsorption is a Function of the Epithelial Cells Making up the TubuleLumenPlasmaCells
Sodium ReabsorptionLumenPlasmaCellsPUMP: Na/K ATPaseSodiumPotassiumChlorideWater
Rennin-Angiotensin-Aldosterone SystemStimulates Sodium Reabsorption in distal and collecting tubulesNaturetic peptide inhibitsIn absence of Aldosterone, 20mg of sodium/day may be excretedAldosterone can cause 99.5% retention
Rennin-Angiotensin-Aldosterone SystemFall in NaCl, extracellular fluid volume, arterial blood pressureJuxtaglomerularApparatusReninLiverAngiotensin+AngiotensinAngiotensinAldosteroneLungsConvertingEnzymeAdrenalCortexIncreasedSodiumReabsorptionHelpsCorrect
DIURETICSACE Inhibitors (Angiotensin Converting Enzyme): Cause loss of salt---> water followsAtrial Naturetic Peptide (ANP) also inhibits sodium reabsorptionOsmotic diuretics: Are not reabsorbed
Glucose and Amino Acids are reabsorbed by secondary active transportThey are actively transported across the apical cell membranes of the epithelial cellsTheir active transport depends on the sodium gradient across this membraneAll other steps are passive
GLUCOSE REABSORPTION HAS A TUBULAR MAXIMUMRenal threshold (300mg/100 ml)Plasma Concentration of GlucoseGlucoseReabsorbedmg/minFiltered ExcretedReabsorbed
Tubular SecretionProtons (acid/base balance)
Potassium
Organic ions
Potassium SecretionLumenPlasmaCellsPUMP: Na/K ATPaseSodiumPotassiumChlorideWater
DUAL CONTROL OF ALDOSTERONE SECRETIONFall in sodiumECF VolumeBlood PressureIncreased PlasmaPotassiumIncreased Aldosterone secretionIncreased TubularPotassium SecretionIncreased UrinaryPotassium SecretionIncreased TubularSodium ReabsorptionFall in UrinarySodium Excretion
Reabsorption in Proximal Tubule (Summary) Glucose and Amino Acids67% of Filtered SodiumOther Electrolytes65% of Filtered Water50% of Filtered UreaAll Filtered Potassium
Secretion in Proximal Tubule (Summary)Variable Proton secretion for acid/base regulation
Organic Ion secretion
Reabsorption in Distal Tubule (Summary)Variable Sodium controlled by Aldosterone
Chloride follows passively
Variable water controlled by vasopressin
Secretion in Distal Tubule (Summary)Variable Proton for acid/base regulation
Variable Potassium controlled by aldosterone
Collecting Duct (Summary)Variable water reabsorption controlled by vasopressin
Variable Proton secretion for acid/base balance
REGULATION OF URINE CONCENTRATIONMedullary countercurrent system
Vasopressin
Medullary countercurrent systemOsmotic gradient established by long loops of Henle
Descending limb
Ascending limb
Descending limbHighly permeable to water
No active sodium transport
Ascending limbActively pumps sodium out of tubule to surrounding interstitial fluid
Impermeable to water
COUNTERCURRENT MAKESTHE OSMOTIC GRADIENT30045060075090010501200 1200From ProximalTubuleTo DistalTubuleCortexMedulla
300450600750900105012001200
10025040055070085010001000ActiveSodiumTransportPassiveWaterTransportLong Loopof Henle
THE OSMOTIC GRADIENT CONCENTRATES THE URINE WHEN VASOPRESSIN (ANTI DIURETIC HORMONE [ADH]) IS PRESENTFrom DistalTubuleCortexMedulla
300450600750900105012001200
300400550700850100011001200Interstitial FluidCollectingDuctPoresOpenPassive Water Flow
WHEN VASOPRESSIN (ANTI DIURETIC HORMONE [ADH]) IS ABSENT A DILUTE URINE IS PRODUCEFrom DistalTubuleCortexMedulla
300450600750900105012001200
100100100100100100100100Interstitial FluidCollectingDuctPoresClosedNo Water FlowOut of Duct
Renal FailureAcute: Sudden onset, rapid reduction in urine output - usually reversible
Chronic: Progressive, not reversible
Up to 75% function can be lost before it is noticeable
THE URINARY BLADDER STORES THE URINEGravity and peristaltic contractions propel the urine along the ureterParasympathetic stimulation contracts the bladder and micturition results if the sphincters (internal and external urethral sphincters) relaxThe external sphincter is under voluntary control
Reflex and Voluntary Control of MicturitionBladder filling reflexively contracts the bladderInternal Sphincter mechanically opensStretch receptors in bladder send inhibitory impulses to external sphincterVoluntary signals from cortex can override the reflex or allow it to take place