Relationship of 3D meniscal morphology and position with knee pain in subjects with knee...
10
MAGNETIC RESONANCE Relationship of 3D meniscal morphology and position with knee pain in subjects with knee osteoarthritis: a pilot study Andrea Wenger & Martin Englund & Wolfgang Wirth & Martin Hudelmaier & Kent Kwoh & Felix Eckstein & for the OAI Investigators Received: 13 May 2011 /Revised: 6 July 2011 /Accepted: 1 August 2011 /Published online: 14 August 2011 # European Society of Radiology 2011 Abstract Objectives To explore whether quantitative, three-dimensional measurements of meniscal position and size are associated with knee pain using a within-person, between-knee study design. Methods We studied 53 subjects (19 men, 34 women) from the Osteoarthritis Initiative, with identical radiographic OA grades in both knees, but frequent pain in one and no pain in the other knee. The tibial plateau and menisci were analyzed using coronally reconstructed double echo steady- state sequence with water excitation (DESSwe) MRI. Results The medial meniscus covered a smaller proportion of the tibial plateau (−5%) and displayed greater extrusion of the body (+15%) in painful than in painless knees (paired t-test; p < 0.05). The external margin of the lateral meniscus showed greater extrusion of the body in painful knees (+22%; p =0.03), but no significant difference in the position of its internal margin or tibial coverage. Medial or lateral extrusion ≥3 mm was more frequent in painful (n =23) than in painless knees (n =12; McNemar’ s test; p =0.02). No significant association was observed between meniscal size and knee pain. Conclusions These data suggest a relationship between extrusion of the meniscal body, as measured with quanti- tative MRI, and knee pain in subjects with knee OA. Further studies need to confirm these findings and their clinical relevance. Key Points & Meniscal segmentation provides quantitative measures of meniscal size/position & Between-knee, within-person approaches can explore potential sources of knee pain & Meniscal extrusion may be a potential source of knee pain Keywords Meniscus . Extrusion . Pain . Knee osteoarthritis . Magnetic resonance imaging Introduction The menisci are known to distribute loads, reduce friction, and protect the articular cartilage during joint loading [1]. Knee osteoarthritis (OA) is a whole-joint disorder involving multiple articular tissues such as cartilage, subchondral bone, ligaments, muscle and the menisci [2]. Meniscal lesions are highly prevalent in the general (healthy) population [3]. Meniscal tears and meniscectomy A. Wenger (*) : W. Wirth : M. Hudelmaier : F. Eckstein Institute of Anatomy & Musculoskeletal Research, Paracelsus Medical University (PMU), Strubergasse 21, A5020 Salzburg, Austria e-mail: [email protected] M. Englund Department of Orthopedics, Lund University, Lund, Sweden M. Englund Clinical Epidemiology Research & Training Unit, Boston University School of Medicine, Boston, MA, USA W. Wirth : M. Hudelmaier : F. Eckstein Chondrometrics GmbH, Ainring, Germany K. Kwoh Division of Rheumatology and Clinical Immunology, University of Pittsburgh and VA Pittsburgh Healthcare System, Pittsburgh, PA, USA Eur Radiol (2012) 22:211–220 DOI 10.1007/s00330-011-2234-z
-
Upload
andrea-wenger -
Category
Documents
-
view
218 -
download
0
Transcript of Relationship of 3D meniscal morphology and position with knee pain in subjects with knee...

MAGNETIC RESONANCE
Relationship of 3D meniscal morphology and positionwith knee pain in subjects with knee osteoarthritis: a pilotstudy
Andrea Wenger & Martin Englund & Wolfgang Wirth &
Martin Hudelmaier & Kent Kwoh & Felix Eckstein &
for the OAI Investigators
Received: 13 May 2011 /Revised: 6 July 2011 /Accepted: 1 August 2011 /Published online: 14 August 2011# European Society of Radiology 2011
AbstractObjectives To explore whether quantitative, three-dimensionalmeasurements of meniscal position and size are associatedwith knee pain using a within-person, between-knee studydesign.Methods We studied 53 subjects (19 men, 34 women) fromthe Osteoarthritis Initiative, with identical radiographic OAgrades in both knees, but frequent pain in one and no painin the other knee. The tibial plateau and menisci wereanalyzed using coronally reconstructed double echo steady-state sequence with water excitation (DESSwe) MRI.Results The medial meniscus covered a smaller proportion ofthe tibial plateau (−5%) and displayed greater extrusion of the
body (+15%) in painful than in painless knees (paired t-test; p<0.05). The external margin of the lateral meniscus showedgreater extrusion of the body in painful knees (+22%; p=0.03),but no significant difference in the position of its internalmargin or tibial coverage. Medial or lateral extrusion ≥3 mmwas more frequent in painful (n=23) than in painless knees(n=12; McNemar’s test; p=0.02). No significant associationwas observed between meniscal size and knee pain.Conclusions These data suggest a relationship betweenextrusion of the meniscal body, as measured with quanti-tative MRI, and knee pain in subjects with knee OA.Further studies need to confirm these findings and theirclinical relevance.Key Points& Meniscal segmentation provides quantitative measures
of meniscal size/position& Between-knee, within-person approaches can explore
potential sources of knee pain& Meniscal extrusion may be a potential source of knee
pain
Keywords Meniscus . Extrusion . Pain . Kneeosteoarthritis . Magnetic resonance imaging
Introduction
The menisci are known to distribute loads, reduce friction,and protect the articular cartilage during joint loading [1].Knee osteoarthritis (OA) is a whole-joint disorder involvingmultiple articular tissues such as cartilage, subchondralbone, ligaments, muscle and the menisci [2].
Meniscal lesions are highly prevalent in the general(healthy) population [3]. Meniscal tears and meniscectomy
A. Wenger (*) :W. Wirth :M. Hudelmaier : F. EcksteinInstitute of Anatomy & Musculoskeletal Research,Paracelsus Medical University (PMU),Strubergasse 21,A5020 Salzburg, Austriae-mail: [email protected]
M. EnglundDepartment of Orthopedics, Lund University,Lund, Sweden
M. EnglundClinical Epidemiology Research & Training Unit,Boston University School of Medicine,Boston, MA, USA
W. Wirth :M. Hudelmaier : F. EcksteinChondrometrics GmbH,Ainring, Germany
K. KwohDivision of Rheumatology and Clinical Immunology,University of Pittsburgh and VA Pittsburgh Healthcare System,Pittsburgh, PA, USA
Eur Radiol (2012) 22:211–220DOI 10.1007/s00330-011-2234-z

both predispose to the onset of knee OA, probably becauseof the loss of biomechanical functions [4–7]. Conversely,knee OA may lead to degenerative meniscal damage thatmay accelerate the disease process [8]. Meniscal tears areknown to be associated with structural progression (increasedcartilage loss) of kneeOA [9–11] and with meniscal extrusion[12–14], defined as a difference ≥3 mm between the externalmeniscal margin and that of the tibial plateau. Meniscalextrusion also is also common in knees without OA [15].
Although traumatic meniscal tears are often painful,degenerative lesions appear not directly associated withsymptoms [3, 16, 17]. Some studies reported a significantassociation between MRI-graded meniscal tears and pain[18], but others did not [19, 20]. To date, no study hasconfirmed a relationship between meniscal extrusion andpain [18, 20], although extrusion may mechanically stressthe pain-sensitive joint capsules [21, 22] and pain-sensitiveexternal portions of the meniscus [23].
As pain perception is subjective and varies widely acrosssubjects, relationships between structural alterations andpain are difficult to establish [24]. A between-knee, within-person study design has been advocated to circumvent thischallenge and provides additional benefits of eliminatingconfounding by other person-related factors such as age,sex, body mass index (BMI), genetics, etc. [24, 25]. Asmeniscal extrusion and size are difficult to evaluateobjectively by scoring, interest has emerged in developingquantitative measurement technology using MRI [26–29].
To explore the relationship between pain and quantitativemeasures of the meniscus [29] in knees with the same gradeof radiographic OA (rOA), we thus applied a within-person,between-knee study design, using clinical and imaging datafrom the Osteoarthritis Initiative (OAI). Specifically, weexplored whether knees with frequent pain display greatermeniscal extrusion (primary hypothesis), and whether kneeswith frequent pain display differences in meniscal sizecompared with contra-lateral knees with no pain (secondaryhypothesis). With the awareness that OA pain is multifac-torial and that no single (imaging) feature can explain thepresence and absence of pain, the current study is meant toprovide a contribution to understanding whether or notmeniscal extrusion is one of many factors that is related toosteoarthritic knee pain.
Materials and methods
Study design and sample selection
The selection of OAI study subjects that matched thecriteria of the current study design was performed usingbaseline and 12 months follow-up clinical and radiographicdata (public-use data set 0.2.2 and 1.2.1). The study
rationale and general inclusion criteria for the OAI (e.g.age 45–79, presence of symptoms and/or knee rOA or riskfactors for developing knee OA) are publicly available(http://oai.epi-ucsf.org/datarelease/) [25].
The radiographic grading used for participant selectionrelied on the fixed-flexion radiographs obtained at baseline.Calculated Kellgren–Lawrence grades (cKLG) were de-rived by centrally certified readers [30, 31]. Knees withdefinite osteophytes and grade 0 OARSI-JSN were classi-fied as cKLG2; knees with definite osteophytes andOARSI-JSN grade 1 and 2 were classified as cKLG3 [32].
Subjects were selected as follows:
& Presence of definite rOA and identical cKLG (cKLG2or cKLG3) in both knees at baseline.
& Frequent pain (grade 2 = pain on most days of a monthin the past 12 months) in one knee, and no pain (grade 0 =no pain in the past 12 months [any pain, aching orstiffness]) in the other knee at baseline. Knees withfrequent pain are termed “painful” and knees with nopain “painless” throughout the study.
& Maximal change of symptom status at 12 months’follow-up in either knee to infrequent pain (grade 1 =pain in past 12 months, but not on most days of themonths), to avoid subjects having more frequent pain inthe formerly painless knee than in the frequently painfulknee.
Of 4796 OAI participants, 56 fulfilled the above criteria.In two cases, MR images were not available; one case wasexcluded because of complete destruction/maceration of themedial meniscus.
MR image data
The image analysis relied on the public-use MR image dataset 0.E.1. acquired at 3T (Magnetom Trio, SiemensHealthcare Erlangen, Germany) using a quadraturetransmit-receive knee coil (USA Instruments, Aurora, OH,USA) [33, 34]. The quantitative meniscal analysis wasperformed using the double oblique coronal multi-planarreconstructions of the sagittal double echo steady-statesequence with water excitation (Fig. 1, corMPR DESSwe,reconstructed slice thickness = 1.5 mm, in-plane resolution0.37 mm×0.7 mm interpolated to 0.37 mm×0.37 mm) [35,36]. Two-dimensional coronal intermediate-weighted turbospin-echo (IW.TSE) images (slice thickness = 3 mminterpolated to 1.5 mm, in-plane resolution 0.37 mm×0.46 mm) were used to assist in the delineation of thesurfaces in the corMPR DESSwe sequence [33]. The IW.TSE was also used to determine lesion scores of themenisci [37] by two experienced musculoskeletal radiol-ogists in consensus (see acknowledgement) blinded toclinical status of the knees [37].
212 Eur Radiol (2012) 22:211–220

Quantitative meniscal analysis
All segmentations were performed by one reader (A.W.)previously trained using image data from the healthy OAIreference cohort and published series of anatomical kneejoint sections and corresponding MR images [38, 39].Manual segmentation was performed using specialised
software (Chondrometrics GmbH, Ainring, Germany)[29]. The reader was blinded both to pain and cKLG statusof the knees during the segmentation of the below tissueboundaries (Fig. 2):
& the articulating surface area of the tibial condyles: Inregions of cartilage coverage, the cartilage surface was
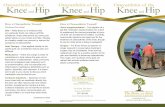
Fig. 1 Central images ofcontra-lateral knees of a studyparticipant. The right medialmeniscus (a, painful knee)shows greater extrusion than theleft (b, painless knee), with themedial joint capsule beingstretched (arrows). The medialmeniscus in the right knee alsoshows a complex tear
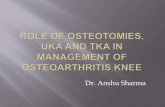
Fig. 2 3D reconstruction of themedial and lateral meniscus –measures are indicated schemat-ically. Femoral (FA), tibial (TA)and external (EA) area of themedial and lateral meniscus,respectively are shown in theupmost picture. Extrusion (mEx.Max) is defined as a ≥3 mmoverlap of the meniscus over thetibial plateau (ACdAB) andreflecting the area of themeniscus that is not adjacent tothe tibial plateau (TA.Uncov).The distance from the externalmargin of the tibial plateau tothe inner margin of the meniscus(OvD = overlap distance)reflects the computed area of thetibial plateau covered bymeniscus (ACdAB.Cov)
Eur Radiol (2012) 22:211–220 213

segmented, and in regions of cartilage denudation, thedenuded subchondral bone (dAB). This segmentedsurface was termed ACdAB, as suggested in a previousreport [29, 40]. Osteophyte surfaces were not includedin ACdAB.
& the tibial area of the medial meniscus and lateralmeniscus, i.e. the area of the meniscus facing the tibialplateau
& the femoral area of the medial and lateral meniscus,facing the femoral articulating surface
& the external area of the medial and lateral meniscus,representing the meniscal boundary facing the joint capsule
To avoid inconsistencies in the segmentation, images ofthe contra-lateral knee were horizontally flipped and theknee segmented first was uploaded as a reference. Seg-mentation started anteriorly and ended posteriorly using thefirst/last image in which both the tibial cartilage and themenisci could be reliably identified. Quantification ofanterior or posterior extrusion of the meniscus is notpossible using coronal images, but requires a sagittalimaging protocol [9].
Internally towards the intercondylar region, the bordersof the menisci were defined by the margin of the tibialcartilage surfaces, because of the missing intrinsic anatom-ical demarcation between the menisci and the transverseand meniscofemoral ligaments. Segmentations were qualitycontrolled by a second reader (F.E.), with adjustments beingmade by consensus.
Computation of three-dimensional morphometric outcomes
Three-dimensional reconstructions of the segmented surfaceswere performed for each compartment [29]. Coverage ofthe tibial plateau by the meniscus (ACdAB.Cov) wasdetermined in absolute (mm2) and relative units (%).Meniscal size was determined by computing the meniscalsurfaces, volume, mean (Th.Me) and maximum thickness(Th.Max, = height), and the mean (Wid.Me) and maxi-mum width (Wid.Max) of both menisci (Fig. 2) [9].Meniscal bulging (Bul.Me) was defined as the averagedistance between the external area and the surfaceconnecting the intersection of tibial and external andfemoral and external area, (Fig. 2).
Meniscal position relative to the tibial plateau wasdetermined as the absolute and relative area of the tibialarea not covering the tibial plateau (TA.Uncov/p). Themean (mEx.Me) and maximum extrusion (mEx.Max) weredetermined as the average and maximal distance betweenthe external area of the meniscus and the external margin ofthe ACdAB (Fig. 2). Positive values indicate an “external”position of the external margin of the meniscus (i.e. towardsthe capsule) compared with the external margin of the
ACdAB, whereas negative values indicate an “internal”position. The distance between the internal margin of themeniscus (i.e. intersection of the tibial and femoral area)and the external border of the tibial plateau was determinedas the mean (OvD.Me) and maximum overlap distance(OvD.Max; Fig. 2). The extrusion and overlap distancewere also computed for the central five images and for themost central image.
Statistical analyses
Primary analyses focused on measures of meniscal position-ing. Differences for continuous outcomes were evaluatedusing a paired two-tailed t-test. McNemar’s test was used tocompare the proportion of knees with extrusion ≥3 mm inpainful vs. painless knees. A two-tailed p-value <0.05 wasconsidered to be statistically significant. Differences betweencKLG2 and cKLG3 strata were evaluated in sensitivityanalyses. Because sets of correlated quantitative outcomeswere interpreted in conjunction rather than in isolation in thispilot study, no adjustment for multiple comparisons wasperformed.
To estimate intra-reader reliability, image data of fourparticipants were analysed again several weeks later. Theroot mean square (RMS) standard deviation across theparticipants was computed as described previously [41].Test-retest data of the quantitative measures of the medialmeniscus are given in Table 1, and those for the lateralmeniscus in Table 2.
Results
Demographic, clinical and semi-quantitative meniscal data
Of 53 participants in this sample, 19 were men and 34women. The mean±SD age was 62.7±9.4 years, bodyheight 1.67±0.10 m, body weight 83.8±15.7 kg, and BMI29.9±4.9. Twenty-two participants displayed cKLG2 inboth knees and 31 cKLG3 bilaterally. At 1-year follow-up,12 participants still displayed grade 2 vs. grade 0 pain incontra-lateral knees, 12 participants grade 2 vs. grade 1, 14grade 1 vs. grade 0, and 15 grade 1 vs. grade 1. At baseline,the painful knees displayed greater pain intensity (numer-ical rating scale = 3.7±2.6) than contra-lateral painlessknees (0.8±2.3), with 10 corresponding to the worst painthe subject can imagine. The total WOMAC score wasgreater in the frequently painful (15.9±13.3) than in thepainless knees (6.3±10.7).
Twenty-six (49%) of the painful and 28 (53%) of thepainless knees had a grade 3 lesion of the medial meniscus,with average±SD scores of 1.4±0.9 and 1.3±0.8, respec-tively. Nine (17%) of the painful and 6 (11%) of the
214 Eur Radiol (2012) 22:211–220

painless knees had a grade 3 meniscal lesion of the lateralmeniscus, with the average score of 0.8±1.0 in painful and0.5±0.8 in painless knees.
Quantitative results in the medial femorotibial compartment
The area of the tibia covered by the medial meniscuswas significantly smaller in painful than in painlessrOA knees (41±10% vs. 44±7%; p=0.04; Table 1), butno significant difference in the size of the medialmeniscus was observed between contralateral knees(Table 1). The relative area of the meniscus not coveringthe tibial plateau was significantly (p=0.03) greater inpainful (19±12%) than in painless knees (16±9%).Analysis of the central slice (p=0.04) and the central five
slices (p=0.02) showed significantly larger extrusionvalues for painful versus painless knees. The distancebetween the internal margin of the medial meniscus andthe external margin of the tibial plateau tended to besmaller in painful than in painless knees (−5 to −12%),but differences were only borderline significant (p=0.05 to0.10). Whereas 19 out of 53 knees with frequent pain (36%)showed a mean extrusion ≥3 mm in the central five slices ofthe medial meniscus, this was the case for only 12 out of 53knees without pain (23%) (p=0.02).
Quantitative results in the lateral femorotibial compartment
The size of the tibia and the proportion covered by thelateral meniscus was similar in painful versus painless
Table 1 Morphometric measures for the medial meniscus in the painful versus contra-lateral painless knees with the same radiographic knee OAstatus (calculated Kellgren-Lawrence grade 2 or 3) as well as test-retest results (n=53)
Medial Meniscus Mean±SD painful knees Mean±SD painless knees Mean Diff% pain vs. no pain t-test (paired) RMS SD
Tibial plateau coverage
ACdAB [mm²] 1108±205 1112±209 −0.5 0.622 15.0
ACdAB.Cov [mm²] 451±121 480±107 −6.3 0.044 22.0
ACdAB.Covp [%] 41.2±9.73 43.5±7.13 −5.4 0.042 1.72
Meniscal size and signal
Tibial area [mm²] 538±116 557±113 −3.8 0.139 16.3
Femoral area [mm²] 618±130 640±139 −3.8 0.162 12.1
External area [mm²] 385±100 387±99.5 −1.2 0.779 8.16
Th.Me [mm] 2.57±0.460 2.56±0.416 0.4 0.732 0.037
Th.Max [mm] 6.70±1.31 6.88±1.47 −2.7 0.276 0.472
Volume [mm³] 2085±690 2133±675 −2.9 0.477 37.9
Wid.Me [mm] 8.45±1.28 8.66±1.16 −2.5 0.186 0.236
Wid.Max [mm] 15.2±2.54 15.6±2.26 −1.8 0.235 0.750
Bul.Me [mm] 0.535±0.153 0.527±0.146 −0.9 0.781 0.114
Meniscal position
TA.Uncov [mm²] 99.2±66.6 89.9±61.0 10.1 0.183 4.41
TA.Uncovp [%] 18.8±12.0 15.9±9.18 18.3 0.029 1.81
mEx.Me [mm] 2.65±1.71 2.50±1.30 5.3 0.441 0.409
mEx.Max [mm] 6.85±1.55 6.66±1.64 3.6 0.422 1.17
mEx.Cent [mm] 2.56±1.45 2.21±1.09 15.5 0.038 0.415
mEx.Cent5 [mm] 2.64±1.46 2.28±1.05 15.7 0.024 0.443
OvD.Me [mm] −9.57±2.32 −10.1±1.81 −5.0 0.068 0.450
OvD.Max [mm] −3.03±1.95 −3.47±1.49 −11.7 0.062 0.639
OvD.Cent [mm] −4.48±2.57 −4.95±1.95 −9.3 0.104 0.696
OvD.Cent5 [mm] −4.67±2.53 −5.22±1.94 −10.4 0.046 0.802
SD: standard deviation; Diff(%): difference in percent; RMS SD: root mean square standard deviation; ACdAB: area of cartilage surface includingdenuded areas of subchondral bone; ACdAB.Cov: area of cartilage surface covered with meniscus; ACdAB.Covp: area of cartilage surfacecovered with meniscus in percent; Th.Me: mean thickness of the meniscus; Th.Max: maximal thickness of the meniscus; Wid.Me: mean width ofthe meniscus; Wid.Max: maximal width of the meniscus; Bul.Me: mean bulging of the meniscus; TA.Uncov: tibial area of the meniscus notcovering the tibial plateau; TA.Uncovp: tibial area of the meniscus not covering the tibial plateau in percent; mEx.Me: mean external extrusion;mEx.Max: maximal external extrusion; mEx.Cent: extrusion in the most central slice; mEx.Cent5: extrusion in the central five slices reflecting themeniscal body; OvD.Me: mean overlap distance; OvD.Max: maximal overlap distance; OvD.Cent: overlap distance in the most central slice;OvD.Cent5: overlap distance in the central five slices reflecting the meniscal body
Eur Radiol (2012) 22:211–220 215

rOA knees (Table 2). There was a trend towards a greatermeniscal size in painful than in painless knees (+1 to +4%),but this was only significant for the maximum width(p=0.03; Table 2). The relative area of the meniscus notcovering the tibial plateau was significantly (p<0.001)greater in painful (8±9%) than in painless knees (4±5%),and so was the mean extrusion distance for the entirelateral meniscus (p<0.001), the central slice (p=0.02),and the central five slices (p=0.03; Table 2). The distancebetween the internal margin of the lateral meniscus andthe external margin of the tibial plateau was similar inpainful versus painless knees. Whereas 4 out of a total of53 knees with frequent pain (8%) showed a meanextrusion ≥3 mm in the central five slices of the lateralmeniscus, none of the knees without pain displayed anextrusion ≥3 mm (p=0.13).
Quantitative results across the medial and lateral meniscus,and per cKLG strata
A significantly greater proportion of the painful (n=23;43%) than of the painless knees (n=12; 23%) had ≥3 mmextrusion (p=0.02) in the five central slices. Sensitivityanalyses revealed that smaller quantitative differencesbetween painful and painless knees were seen in KLG2than in KLG3 knees (data not shown). Within the cKLG3strata, 17 of the painful knees (55%) showed a meanextrusion ≥3 mm (central 5 slices) of either the medial orlateral meniscus, and only 2 (7%) of the painless knees (p=0.001). Within the cKLG2 strata, 6 (27%) of the painfulknees showed a mean extrusion ≥3 mm in the medial orlateral compartment compared with 2 (9%) of the painlessknees (p=0.29).
Table 2 Morphometric measures for the lateral meniscus in the painful versus contralateral painless knees with the same radiographic knee OAstatus (calculated Kellgren-Lawrence grade 2 or 3) as well as test-retest results (n=53)
Lateral Meniscus Mean±SD painful knees Mean±SD painless knees Mean Diff% pain vs. no pain t-test (paired) RMS SD
Tibial plateau coverage
ACdAB [mm²] 943±199 952±202 −0.8 0.423 35.6
ACdAB.Cov [mm²] 527±124 533±111 −1.4 0.631 27.6
ACdAB.Covp [%] 56.3±8.07 56.3±5.50 −0.6 0.987 1.56
Meniscal size and signal
Tibial area [mm²] 552±113 544±111 1.0 0.401 18.8
Femoral area [mm²] 631±134 617±128 1.7 0.207 17.8
External area [mm²] 379±100 368±82.5 2.8 0.151 10.2
Th.Me [mm] 2.64±0.401 2.59±0.349 1.5 0.225 0.077
Th.Max [mm] 6.88±1.39 6.77±0.940 1.4 1.400 0.132
Volume [mm³] 2157±672 2073±601 3.6 0.123 55.9
Wid.Me [mm] 9.14±1.29 9.03±1.25 1.0 0.466 0.229
Wid.Max [mm] 13.3±1.98 12.8±1.84 3.4 0.026 0.560
Bul.Me [mm] 0.520±0.222 0.506±0.121 3.6 0.642 0.137
Meniscal position
TA.Uncov [mm²] 44.7±54.0 21.5±26.6 101 0.002 19.0
TA.Uncovp [%] 8.00±9.38 3.92±4.63 97.7 0.003 4.07
mEx.Me [mm] −0.843±2.48 −1.84±1.74 −48.1 0.001 1.11
mEx.Max [mm] 8.02±1.87 7.95±1.95 1.5 0.778 0.644
mEx.Cent [mm] 1.48±1.12 1.15±0.485 25.0 0.020 0.506
mEx.Cent5 [mm] 1.46±1.10 1.15±0.442 22.3 0.026 0.424
OvD.Me [mm] −14.7±2.81 −14.9±2.59 −1.2 0.392 1.37
OvD.Max [mm] −8.01±2.70 −8.25±2.55 −2.2 0.491 0.750
OvD.Cent [mm] −9.10±3.45 −9.05±2.83 1.6 0.913 0.805
OvD.Cent5 [mm] −9.40±3.13 −9.43±2.63 0.2 0.935 0.798
Abbreviations are the same as in Table 1
Please note that a “negative” value for extrusion corresponds to an internal position of the external border of the meniscus compared with theexternal border of the tibial plateau (i.e. intrusion). The less negative values in the painful knees reflect a more external position of the meniscusthan in painless knees. Note that whereas the entire lateral meniscus shows an intrusion, on average, the meniscal body (i.e. the central five slices;mEx.Cent5) shows extrusion compared with the tibia
216 Eur Radiol (2012) 22:211–220

Discussion
In this study, we found a smaller proportion of the medialtibial plateau to be covered by the medial meniscus inpainful than in painless OA knees. Also the medialmeniscus displayed more extrusion in painful knees,reflected in a greater uncovered meniscal surface, and agreater extrusion distance. Meniscal lesion scores, on theother hand, were similar in painful and painless knees.Laterally, the external border of the meniscus was also in amore “extruded” position in painful knees but no significantdifferences were noted in the position of its internal border(but a trend towards a somewhat larger size and width).
Limitations of this study are the modest sample size (n=53), and that a large number of participants was required (i.e.4796) for case selection, as the approach chosen required aspecific combination of features. Because correlated meas-ures of extrusion and size were not corrected for multipletesting, the results need to be interpreted with caution. Aparticularity of the study, however, is the use of a within-person, between-knee study design that eliminates person-specific confounders and other differences in pain perceptionbetween individuals [24, 25]. This approach has been shownto be more effective in revealing a relationship between painand structural alterations (in radiographs) than across-subjectanalysis approaches [24]. Because this design does notcontrol for knee-specific differences, we additionally limitedthe analysis to subjects who displayed the same radiographicstage of knee OA in both knees. However, potential forconfounding by other structural features (e.g. bone marrowlesions) remains.
Quantitative measurements generally rely on a highspatial resolution. This was provided by the DESSwe whichalso has been previously validated for quantitative cartilagemeasurement [35, 36, 42, 43]. As IW- or T2-weighted TSEsequences are commonly used for evaluating meniscallesions, we additionally used IW.TSE images to assist thereadings of the DESSwe [44, 45] and to facilitate thesegmentation process, particularly in situations of unclearcontrast. A limitation is that only a coronal MPRorientation of the DESSwe was used, whereas sagittalimages are required [9] to establish whether anterior andposterior extrusion is correlated with pain frequency.Further, MRIs were acquired without weight-bearing,whereas the meniscus has its primary biomechanicalfunction during load bearing. However, a recent studyshowed that there were only minimal differences in themorphology and position of the meniscus between non-weight-bearing and weight-bearing [46], for MR imagesacquired with and without use of a loading device [47].Finally, this study is limited by its observational nature andthe lack of inclusion of extended semi-quantitative scores[48, 49] for the menisci, subchondral bone, cartilage,
ligaments and the synovium. Yet, to our knowledge, thisis the first study to explore whether novel quantitative,three-dimensional measures of meniscal extrusion andmeniscal size differ between painful and painless kneeswith rOA. These measures may potentially provide a moreobjective and sensitive evaluation of complex geometricfeatures that are challenging to evaluate based on subjectivegrading, as minute structural changes may extend overseveral image slices. Further studies, involving a face-to-face comparison, will have to confirm whether quantitativemeasures of extrusion provide additional (or more sensi-tive) information in relation to commonly employed scoringmethods [48]. The quantitative outcomes computed fromthe tibial surface and meniscal segmentation are notintended to replace semi-quantitative scoring of the menis-cus. Instead, they should be considered as a complimentaryassessment of tibial coverage, meniscal size and meniscalposition, which provide challenges in the subjective scoringof 2D images. Also, given its cost and complexity, themethod is targeted at research studies exploring the patho-physiology of knee OA, but not at clinical diagnostics. Toour knowledge, this is the first study to show a significantrelationship between pain frequency and meniscal position,whereas previous studies relying on semi-quantitativescores were unable to detect this association [18–20].
In our study, the number of meniscal tears was similar inpainful versus painless knees, so that side differences inpain frequency are probably not explained by lesions. Thisis in agreement with previous observations that degenera-tive meniscal tears are not directly associated withsymptoms [3, 16, 17]. A recent paper, however, describeda relationship between meniscal extrusion and bone marrowlesions (BMLs), potentially due to less mechanical protec-tion by the meniscus [50]. BMLs have been associated withpain status and have been discussed as a potential source ofpain [49, 51, 52]. Also, meniscal extrusion may causebulging and mechanical stretching of the joint capsule,which is richly innervated with pain fibres [21, 22] and/ormechanical stress on the external aspect of the meniscus,which is also richly innervated [23]. Interestingly, therelationship between pain and extrusion was more obviousin cKLG3 than in cKLG2 knees, with extrusion ≥3 mmbeing rare in cKLG2 knees. Boxheimer et al. [53] foundthat meniscal displacement of ≥3 mm (between differentknee positions) was strongly associated with complexmeniscal tears and collateral ligament lesions, and studyparticipants with displaceable meniscal tears had signifi-cantly more pain than did patients with non-displaceablemeniscal tears, independent of the concomitant kneeabnormalities. However, given the cross-sectional natureand the explorative character of our study, we can onlyspeculate about the relationship of meniscal extrusion andknee pain. If the current findings can be replicated, further
Eur Radiol (2012) 22:211–220 217

studies will have to explore whether meniscal extrusion iscausing pain, whether it is involved in mediating pain, orwhether it is simply an “innocent bystander” in thisrelationship.
In conclusion, this is to our knowledge the first study todescribe a relationship between meniscal extrusion (mea-sured quantitatively and in 3D) and the frequency of kneepain. Extrusion of ≥3 mm (in the central five slices) wasmore frequent in painful than in contra-lateral painlessknees, and more frequent in cKLG3 than in cKLG2 knees.Further studies will have to confirm these findings and willhave to explore whether and to what extent meniscalextrusion is involved in the causation or mediation of kneepain in OA.
Acknowledgements We thank Iris Nöbauer and Siegfried Trattnigfrom the Magnetic Resonance Centre of Excellence at the MedicalUniversity Vienna, Austria for providing the semi-quantitativemeniscal readings (Crues and Lotysch lesion scores). Katja Bloecker,Richard Frobell and Martina Sattler (Institute of Anatomy &Musculoskeletal Research, Paracelsus Medical University Salzburg,Austria) are thanked for their help with establishing the reading rulesfor meniscal segmentation and with selecting the participants from theOAI data base. Also, we thank the OAI participants, OAI investigatorsand OAI Clinical Center’s staff for generating the publicly availableimage data set.
The study and image acquisition was supported by the OAI(contract nos. N01-AR-2-2258; N01-AR-2-2259; N01-AR-2-2260;N01-AR-2-2261; N01-AR-2-2262) funded by the National Institutesof Health and conducted by the OAI Study Investigators. Privatefunding partners include Pfizer, Inc.; Novartis PharmaceuticalsCorporation; Merck Research Laboratories; and GlaxoSmithKline.Private sector funding for the OAI is managed by the Foundation forthe National Institutes of Health. This manuscript has received theapproval of the OAI Publications Committee based on a review of itsscientific content and data interpretation.
The image analysis was supported by funds from ParacelsusMedical University (PMU Forschungsfond). Dr. Englund is supportedby the Swedish Research Council, the Faculty of Medicine, LundUniversity, and the Royal Physiographic Society in Lund and Dr.Kwoh by grant AR054731. Felix Eckstein is CEO and co-owner ofChondrometrics GmbH; he also provides consulting services toMerckSerono, Novartis and Sanofi Aventis. Wolfgang Wirth is co-ownerof Chondrometrics GmbH.
References
1. Englund M, Guermazi A, Lohmander SL (2009) The role of themeniscus in knee osteoarthritis: a cause or consequence? RadiolClin North Am 47(4):703–712
2. Rannou F, Sellam J, Berenbaum F (2010) Pathophysiology ofosteoarthritis: updated concepts. Presse Med 39(11):1159–1163
3. Englund M, Guermazi A, Gale D, Hunter DJ, Aliabadi P, ClancyM, Felson DT (2008) Incidental meniscal findings on knee MRIin middle-aged and elderly persons. N Engl J Med 359(11):1108–1115
4. McNicholas MJ, Rowley DI, McGurty D, Adalberth T, Abdon P,Lindstrand A, Lohmander LS (2000) Total meniscectomy inadolescence. A thirty-year follow-up. J Bone Joint Surg Br 82(2):217–221
5. Englund M, Guermazi A, Roemer FW, Aliabadi P, Yang M, LewisCE, Torner J, Nevitt MC, Sack B, Felson DT (2009) Meniscal tearin knees without surgery and the development of radiographicosteoarthritis among middle-aged and elderly persons: TheMulticenter Osteoarthritis Study. Arthritis Rheum 60(3):831–839
6. Englund M, Lohmander LS (2004) Risk factors for symptomaticknee osteoarthritis fifteen to twenty-two years after meniscectomy.Arthritis Rheum 50(9):2811–2819
7. Fairbank TJ (1948) Knee joint changes after meniscectomy. JBone Joint Surg Br 30B(4):664–670
8. Roos H, Adalberth T, Dahlberg L, Lohmander LS (1995)Osteoarthritis of the knee after injury to the anterior cruciateligament or meniscus: the influence of time and age. OsteoarthrCartil 3(4):261–267
9. Hunter DJ, Zhang YQ, Niu JB, Tu X, Amin S, Clancy M,Guermazi A, Grigorian M, Gale D, Felson DT (2006) Theassociation of meniscal pathologic changes with cartilage loss insymptomatic knee osteoarthritis. Arthritis Rheum 54(3):795–801
10. Sharma L, Eckstein F, Song J, Guermazi A, Prasad P, Kapoor D,Cahue S, Marshall M, Hudelmaier M, Dunlop D (2008)Relationship of meniscal damage, meniscal extrusion, malalignment,and joint laxity to subsequent cartilage loss in osteoarthritic knees.Arthritis Rheum 58(6):1716–1726
11. Chang A, Moisio K, Chmiel JS, Eckstein F, Guermazi A, AlmagorO, Cahue S, Wirth W, Prasad P, Sharma L (2011) Subregionaleffects of meniscal tears on cartilage loss over 2 years in kneeosteoarthritis. Ann Rheum Dis 70(1):74–79
12. Rennie WJ, Finlay DB (2006) Meniscal extrusion in youngathletes: associated knee joint abnormalities. AJR Am J Roent-genol 186(3):791–794
13. Choi CJ, Choi YJ, Lee JJ, Choi CH (2010) Magnetic resonanceimaging evidence of meniscal extrusion in medial meniscusposterior root tear. Arthroscopy 26(12):1602–1606
14. Lee DH, Lee BS, Kim JM, Yang KS, Cha EJ, Park JH, Bin SI(2011) Predictors of degenerative medial meniscus extrusion:radial component and knee osteoarthritis. Knee Surg SportsTraumatol Arthrosc 19(2):222–229
15. Puig L, Monllau JC, Corrales M, Pelfort X, Melendo E, Caceres E(2006) Factors affecting meniscal extrusion: correlation with MRI,clinical, and arthroscopic findings. Knee Surg Sports TraumatolArthrosc 14(4):394–398
16. Englund M, Niu J, Guermazi A, Roemer FW, Hunter DJ, LynchJA, Lewis CE, Torner J, Nevitt MC, Zhang YQ, Felson DT(2007) Effect of meniscal damage on the development offrequent knee pain, aching, or stiffness. Arthritis Rheum 56(12):4048–4054
17. Bhattacharyya T, Gale D, Dewire P, Totterman S, Gale ME,McLaughlin S, Einhorn TA, Felson DT (2003) The clinicalimportance of meniscal tears demonstrated by magnetic resonanceimaging in osteoarthritis of the knee. J Bone Joint Surg Am 85-A(1):4–9
18. Torres L, Dunlop DD, Peterfy C, Guermazi A, Prasad P, HayesKW, Song J, Cahue S, Chang A, Marshall M, Sharma L (2006)The relationship between specific tissue lesions and pain severityin persons with knee osteoarthritis. Osteoarthr Cartil 14(10):1033–1040
19. Conaghan PG, Felson DT (2004) Structural associations ofosteoarthritis pain: lessons from magnetic resonance imaging.Novartis Found Symp 260:191–201
20. Kornaat PR, Bloem JL, Ceulemans RY, Riyazi N, Rosendaal FR,Nelissen RG, Carter WO, Hellio Le Graverand MP, KloppenburgM (2006) Osteoarthritis of the knee: association between clinicalfeatures and MR imaging findings. Radiology 239(3):811–817
21. Heppelmann B (1997) Anatomy and histology of joint innerva-tion. J Peripher Nerv Syst 2(1):5–16
218 Eur Radiol (2012) 22:211–220

22. Dye SF, Vaupel GL, Dye CC (1998) Conscious neurosensorymapping of the internal structures of the human knee withoutintraarticular anesthesia. Am J Sports Med 26(6):773–777
23. Mine T, Kimura M, Sakka A, Kawai S (2000) Innervation ofnociceptors in the menisci of the knee joint: an immunohis-tochemical study. Arch Orthop Trauma Surg 120(3–4):201–204
24. Neogi T, Felson D, Niu J, Nevitt M, Lewis CE, Aliabadi P,Sack B, Torner J, Bradley L, Zhang Y (2009) Associationbetween radiographic features of knee osteoarthritis and pain:results from two cohort studies. BMJ 339:b2844. doi:10.1136/bmj.b2844.:b2844
25. Eckstein F, Benichou O, Wirth W, Nelson DR, Maschek S,Hudelmaier M, Kwoh K, Guermazi A, Hunter D, for the OAIinvestigators (2009) Direct comparison of cartilage loss in painfulcontra-lateral knees with and without joint space narrowing - datafrom the Osteoarthritis Initiative (OAI). Arthritis Care Res 61(9):1218–1225
26. Swanson MS, Prescott JW, Best TM, Powell K, Jackson RD, HaqF, Gurcan MN (2010) Semi-automated segmentation to assess thelateral meniscus in normal and osteoarthritic knees. OsteoarthrCartil 18(3):344–353
27. Bowers ME, Tung GA, Fleming BC, Crisco JJ, Rey J (2007)Quantification of meniscal volume by segmentation of 3Tmagnetic resonance images. J Biomech 40(12):2811–2815
28. Elsner JJ, Portnoy S, Guilak F, Shterling A, Linder-Ganz E (2010)MRI-based characterization of bone anatomy in the human kneefor size matching of a medial meniscal implant. J Biomech Eng132(10):101008
29. Wirth W, Frobell RB, Souza RB, Li X, Wyman BT, Le GraverandMP, Link TM, Majumdar S, Eckstein F (2010) A three-dimensional quantitative method to measure meniscus shape,position, and signal intensity using MR images: a pilot study andpreliminary results in knee osteoarthritis. Magn Reson Med 63(5):1162–1171
30. Nevitt MC, Peterfy C, Guermazi A, Felson DT, Duryea J,Woodworth T, Chen H, Kwoh K, Harris TB (2007) Longitudinalperformance evaluation and validation of fixed-flexion radiogra-phy of the knee for detection of joint space loss. Arthritis Rheum56(5):1512–1520
31. Altman RD, Gold GE (2007) Atlas of individual radiographicfeatures in osteoarthritis, revised. Osteoarthr Cartil 15(SupplA):1–56
32. Spector TD, Hart DJ, Byrne J, Harris PA, Dacre JE, Doyle DV(1993) Definition of osteoarthritis of the knee for epidemiologicalstudies. Ann Rheum Dis 52(11):790–794
33. Peterfy CG, Schneider E, Nevitt M (2008) The osteoarthritisinitiative: report on the design rationale for the magneticresonance imaging protocol for the knee. Osteoarthr Cartil 16(12):1433–1441
34. Schneider E, NessAiver M, White D, Purdy D, Martin L, FanellaL, Davis D, Vignone M, Wu G, Gullapalli R (2008) Theosteoarthritis initiative (OAI) magnetic resonance imagingquality assurance methods and results. Osteoarthr Cartil 16(9):994–1004
35. Eckstein F, Hudelmaier M, Wirth W, Kiefer B, Jackson R, Yu J,Eaton CB, Schneider E (2006) Double echo steady state magneticresonance imaging of knee articular cartilage at 3 Tesla: a pilotstudy for the Osteoarthritis Initiative. Ann Rheum Dis 65(4):433–441
36. Wirth W, Nevitt M, Hellio Le Graverand MP, Benichou O, DreherD, Davies RY, Lee J, Picha K, Gimona A, Maschek S, HudelmaierM, Eckstein F (2010) Sensitivity to change of cartilage mor-phometry using coronal FLASH, sagittal DESS, and coronal MPRDESS protocols–comparative data from the Osteoarthritis Initia-tive (OAI). Osteoarthr Cartil 18(4):547–554
37. Crues JV III, Mink J, Levy TL, Lotysch M, Stoller DW (1987)Meniscal tears of the knee: accuracy of MR imaging. Radiology164(2):445–448
38. Burgkart R, Eckstein F, Sittek H, Schittich I, Träger J, Hipp E(1995) Schnittanatomie des Kniegelenks - Korrelation vonanatomischen Präparat, Computertomograhie und Magnetreso-nanztomographie, Schwerpunkt:hinteres Kreuzband und medialesKompartiment. Sportorthopädie - Sporttraumatologie 11(4):262–267
39. Burgkart R, Schelter R, Eckstein F, Rechl H, Träger J (1995)Schnittanatomie des Kniegelenks - Korrelation von anatomischenPräparat, Computertomograhie und Magnetresonanztomographie,Schwerpunkt:posterolaterale Knieregion. Sportorthopädie - Sport-traumatologie 11(2):112–117
40. Eckstein F, Ateshian G, Burgkart R, Burstein D, Cicuttini F,Dardzinski B, Gray M, Link TM, Majumdar S, Mosher T, PeterfyC, Totterman S, Waterton J, Winalski CS, Felson D (2006)Proposal for a nomenclature for magnetic resonance imagingbased measures of articular cartilage in osteoarthritis. OsteoarthrCartil 14(10):974–983
41. Glüer CC, Blake G, Lu Y, Blunt BA, Jergas M, Genant HK (1995)Accurate assessment of precision errors: how to measure thereproducibility of bone densitometry techniques. Osteoporos Int 5(4):262–270
42. Burgkart R, Glaser C, Hyhlik-Durr A, Englmeier KH, Reiser M,Eckstein F (2001) Magnetic resonance imaging-based assessmentof cartilage loss in severe osteoarthritis: accuracy, precision, anddiagnostic value. Arthritis Rheum 44(9):2072–2077
43. Graichen H, Eisenhart-Rothe R, Vogl T, Englmeier KH, Eckstein F(2004) Quantitative assessment of cartilage status in osteoarthritisby quantitative magnetic resonance imaging: technical validationfor use in analysis of cartilage volume and further morphologicparameters. Arthritis Rheum 50(3):811–816
44. Roemer FW, Zhang Y, Niu J, Lynch JA, Crema MD, Marra MD,Nevitt MC, Felson DT, Hughes LB, El-Khoury GY, Englund M,Guermazi A (2009) Tibiofemoral joint osteoarthritis: risk factorsfor MR-depicted fast cartilage loss over a 30-month period in themulticenter osteoarthritis study. Radiology 252(3):772–780
45. Guermazi A, Burstein D, Conaghan P, Eckstein F, Hellio LeGraverand-Gastineau MP, Keen H, Roemer FW (2008) Imaging inosteoarthritis. Rheum Dis Clin North Am 34(3):645–687
46. Frobell RB, Souza RB, Wyman BT, Wirth W., Hellio-LeGraverand MP, Hudelmaier M., Li X, Link T, Eckstein F,Majumdar S (2009) Mensicus shape, position, and signalunder simulated weightbearing and non-weightbearing con-ditions in vivo. Osteorthritis and Cartilage, OARSI 17 Supple 1,Abstract:S236
47. Cotofana S, Eckstein F, Wirth W, Souza RB, Li X, Wyman B,Hellio-Le Graverand MP, Link T, Majumdar S (2011) In vivomeasures of cartilage deformation: patterns in healthy andosteoarthritic female knees using 3T MR imaging. Eur Radiol21(6):1127–1135
48. Peterfy CG, Guermazi A, Zaim S, Tirman PF, Miaux Y, White D,Kothari M, Lu Y, Fye K, Zhao S, Genant HK (2004) Whole-OrganMagnetic Resonance Imaging Score (WORMS) of the knee inosteoarthritis. Osteoarthr Cartil 12(3):177–190
49. Hunter DJ, Lo GH, Gale D, Grainger AJ, Guermazi A, ConaghanPG (2008) The reliability of a new scoring system for kneeosteoarthritis MRI and the validity of bone marrow lesionassessment: BLOKS (Boston Leeds Osteoarthritis Knee Score).Ann Rheum Dis 67(2):206–211
50. Englund M, Guermazi A, Roemer FW, Yang M, Zhang Y, NevittMC, Lynch JA, Lewis CE, Torner J, Felson DT (2010) Meniscalpathology on MRI increases the risk for both incident andenlarging subchondral bone marrow lesions of the knee: theMOST Study. Ann Rheum Dis 69(10):1796–1802
Eur Radiol (2012) 22:211–220 219

51. Felson DT, Chaisson CE, Hill CL, Totterman SM, Gale ME, SkinnerKM, Kazis L, Gale DR (2001) The association of bone marrow lesionswith pain in knee osteoarthritis. Ann Intern Med 134(7):541–549
52. Felson DT, Niu J, Guermazi A, Roemer F, Aliabadi P, Clancy M,Torner J, Lewis CE, Nevitt MC (2007) Correlation of thedevelopment of knee pain with enlarging bone marrow lesions
on magnetic resonance imaging. Arthritis Rheum 56(9):2986–2992
53. Boxheimer L, Lutz AM, Zanetti M, Treiber K, Labler L, MarincekB, Weishaupt D (2006) Characteristics of displaceable andnondisplaceable meniscal tears at kinematic MR imaging of theknee. Radiology 238(1):221–231
220 Eur Radiol (2012) 22:211–220