
Ending the Employment Relationship: Government Response - Gov.uk

1
Relationship between complete pathologic response to neoadjuvant chemotherapy and
survival in triple negative breast cancer
Christos Hatzisa, W. Fraser Symmansb, Ya Zhangb, Rebekah E. Gouldb, Stacy L. Moulderc, Kelly
K. Huntd, Maysa Abu-Khalafa, Erin W. Hofstattera, Donald Lannine, Anees B. Chagpare, Lajos
Pusztaia
aDepartment of Internal Medicine, Yale School of Medicine, Yale Cancer Center, New Haven,
CT
bDepartment of Pathology, University of Texas MD Anderson Cancer Center, Houston, TX
cDepartment of Breast Medical Oncology, University of Texas MD Anderson Cancer Center,
Houston, TX
dDepartment of Surgical Oncology, University of Texas MD Anderson Cancer Center, Houston,
TX
eDepartment of Surgery, Yale School of Medicine, Yale Cancer Center, New Haven, CT
Running Title: Pathologic complete response and survival benefit in cancer
Keywords: Breast cancer, neoadjuvant studies, trial design, pathologic complete response,
survival
Financial Support
This work was supported in part by grants from The Breast Cancer Research Foundation (WFS, LP) and Susan G. Komen for The Cure (KG081680 to WFS).
Research. on June 7, 2020. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 18, 2015; DOI: 10.1158/1078-0432.CCR-14-3304

2
Corresponding Authors
Christos Hatzis ([email protected]) or Lajos Pusztai ([email protected] )
Breast Medical Oncology
Yale School of Medicine
333 Cedar Street
PO Box 208032
New Haven, CT 06520-8032
Tel: 203-737-8309
Fax: 203-785-5792
Conflicts of Interest
The authors declare that they have no competing interests to disclose.
Word Count
Abstract: 247 words
Body: 2830 words
Research. on June 7, 2020. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 18, 2015; DOI: 10.1158/1078-0432.CCR-14-3304

3
Translational Relevance
Pathologic complete response (pCR) to neoadjuvant chemotherapy is indicative of the cytotoxic
efficacy of a drug, but patient survival is influenced by several other factors. The answer to the
often-quoted question, “Is pCR a surrogate for long term survival?” is yes at the individual
patient level. For the subtly different question “If increased pCR rate is a surrogate for improved
survival in a trial arm”, the answer depends on the absolute improvement in pCR rate, baseline
prognosis of the trial population, interaction of pCR with prognostic variables and efficacy of
post-neoadjuvant treatment modalities . Our framework helps estimating the impact of increased
pCR rate on survival and could help designing and powering the next generation of neoadjuvant
trials, particularly if the goal is to demonstrate improved survival from a regimen that results in
higher pCR rate.
Research. on June 7, 2020. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 18, 2015; DOI: 10.1158/1078-0432.CCR-14-3304

4
Abstract Background: Pathologic complete response (pCR) to neoadjuvant chemotherapy reflects the
cytotoxic efficacy of a drug, but patient survival is influenced by many other factors. The
purpose of this study was to assess the relationship between increased pCR rate and trial-level
survival benefit in triple negative breast cancer (TNBC).
Methods: We used bootstrap resampling from a neoadjuvant trial to simulate trials with different
pCR rates. We used estimates from AdjuvantOnline to simulate trial populations with different
baseline prognosis and estimated survival improvements associated with changes in pCR rate.
Results: Assuming that survival is similar for patients with pCR regardless of treatment arm, a
linear relationship exists between increasing pCR rate and increasing RFS. The slope is equal to
the difference in survival between those with pCR and RD which in turn is influenced by (i) the
baseline prognosis of the trial population, (ii) interactions between prognostic variables and pCR,
and (iii) the efficacy of the post-neoadjuvant therapies. For example, if the pCR rates are 30%
and 60% (OR=3.5) and the 10-year RFS of the control arm is 0.74, the trial would require 3550
patients per arm, whereas if the RFS is 0.54 the trial would only require 425 patients per arm to
detect significant survival benefit.
Conclusions: We provide a framework for understanding the relationship between pCR and
overall survival benefit that can help inform the design of neoadjuvant trials aiming to
demonstrate improved survival from a regimen that results in higher pCR rate.
Research. on June 7, 2020. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 18, 2015; DOI: 10.1158/1078-0432.CCR-14-3304

5
Introduction
Breast cancer patients who achieve pathologic complete response (pCR) defined as complete
eradication of invasive cancer from the breast and lymph nodes have excellent survival
regardless of hormone receptor status or molecular subtype while those with residual invasive
disease (RD) have variable prognosis depending on disease subtype and clinical stage.(1-4)
Triple negative breast cancer (TNBC) patients with RD have a poor prognosis that is
proportionate to the extent of residual disease, but some patients with estrogen receptor (ER)
positive cancer have excellent survival even with RD after neoadjuvant chemotherapy.(3, 5, 6)
One could expect that more effective cytotoxic therapies that produce higher pCR rates will lead
to improved survival compared to less effective cytotoxic therapies, as they push more patients
into the favorable survival group. Indeed, inclusion of taxanes in neoadjuvant chemotherapy
increased pCR rates and also increased survival in much larger adjuvant trials.(7, 8) The
inclusion of trastuzumb with a broad range of chemotherapy drugs doubled the pCR rates
compared to chemotherapy alone, and also increased survival.(9, 10) The NOAH study for
locally advanced breast cancer, directly demonstrated improvement in pCR rate (38% vs 19%)
followed by an improvement in disease free survival (DFS; 71% vs 56%) in the same trial.(11)
Based on these and other supportive data, the US Food and Drug Administration (FDA) is
currently considering pCR as an endpoint to support accelerated drug approval for early stage
breast cancer.(12, 13)
However, the relationship between improvement in pCR rate and trial-arm level survival
benefit is less than straightforward. Even studies that directly or indirectly support a positive
association show substantially greater absolute improvements in pCR rate than in survival.
Furthermore, the largest randomized neoadjuvant trial, the NSABP B-27 (n=2411), failed to
Research. on June 7, 2020. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 18, 2015; DOI: 10.1158/1078-0432.CCR-14-3304

6
demonstrate a significant improvement in 5-year DFS (71% v 68%) or overall survival (OS),
despite a significant improvement in pCR rate (26% vs 13%) with the inclusion of docetaxel
with anthracycline/cyclophosphamide neoadjuvant therapy.(2) Several other randomized
neoadjuvant trials with sample sizes between 200 to 2000, and including both estrogen receptor
(ER) positive and negative cases, also failed to demonstrate improvements in survival despite
increased pCR rates in the experimental arms.(14, 15) The FDA-led meta-analysis of 12
neoadjuvant clinical trials (CTNeoBC) confirmed the patient-level prognostic value of pCR but it
could not demonstrate a significant correlation between pCR odds ratio and event-free survival
hazard ratio at the trial-level across the studies.(16) More recently, the ALTTO adjuvant trial
(n=6281) that compared one year of anti-HER2 therapy with lapatinib alone, trastuzumab alone
or the combination of the two drugs concomitant with or after chemotherapy in HER2-positive
early breast cancer also failed to show statistically significant improvement in survival,(17)
despite a significant improvement in pCR rate (51% vs 29% and 24%) with the dual HER2
blockade in the neoadjuvant NeoALTTO trial.(18) Clearly, substantial and statistically
significant improvements in pCR rate can translate in minor, non-significant improvements in
patient survival in large trials.
At least five factors could contribute to why a regimen with increased cytotoxic activity
would fail to improve survival. First, the baseline prognosis of the patient cohort has a major
impact on the absolute survival benefit; patients with good initial prognosis (e.g. earlier clinical
stage) can only have small gains in survival. Second, the frequency of pCR may be higher in
patients with good initial prognosis, meaning that increased pCR rate may have a diminished
impact on overall survival at the trial level. Third, effective post-neoadjuvant therapy, such as
adjuvant endocrine therapy for ER positive cancers, will improve the outcome in the RD group.
Research. on June 7, 2020. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 18, 2015; DOI: 10.1158/1078-0432.CCR-14-3304

7
Fourth, patients with minimal residual cancer burden after neoadjuvant chemotherapy often have
the same excellent prognosis as patients who achieve pCR;(6) if a regimen increases the pCR
rate primarily by moving patients who would have with minimal residual cancer burden after
standard therapy to the pCR group in the experimental arm, the net survival benefit from the
increase in pCR rate would be minimal. Fifth, 5-6% of patients who achieve pCR will experience
distant recurrence, which further limits its early surrogate function. All the above factors co-exist
and influence survival in a clinical trial and most are poorly understood and difficult to model.
The lack of independence between many prognostic and predictive markers further complicates
building theoretical models, which has motivated us to use real patient data to assess the
relationship between pCR and survival. In real patient data, the hidden biomarker associations
and above confounders are already accounted for. We also assessed our model on simulated
survival data generated by Adjuvant!Online predictions to examine the impact of anatomical
prognostic risk variables on the relationship between pCR and survival.
The purpose of this study was to evaluate the relationship between increased pCR rate
and trial-level survival using bootstrap resampling from real and simulated neoadjuvant trial
patient outcome data. We varied the pCR frequency through biased resampling to simulate trials
with different pCR rates. We also varied the survival of the RD cohort to simulate TNBC trial
populations with different baseline prognoses.
Materials and Methods
Patient data
Research. on June 7, 2020. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 18, 2015; DOI: 10.1158/1078-0432.CCR-14-3304

8
We used survival data from 127 clinical stage I-III TNBC cases from our previously published
cohort from M.D. Anderson Cancer Center (6) with recently updated survival outcomes.(19)
TNBC status was defined as ER and PR < 1% positivity by routine immunohistochemistry (IHC)
and lack of HER2 amplification by FISH (HER2:CEP17 copy number ratio < 2.0) or HER2 IHC
score of 0. All patients received preoperative chemotherapy with weekly paclitaxel and
fluorouracil, doxorubicin (or epirubicin), and cyclophosphamide, as previously reported.
Pathologic complete response was defined as no residual invasive cancer in the breast or lymph
nodes; the pCR rate for TNBC patients was 35%. The median follow up for event-free survivors
was 9.3 years (range 0.5 to 13.4 years). The 5-year distant recurrence-free survival (DRFS) for
the pCR and RD groups was 0.93 (95%CI: 0.86-1.00) and 0.58 (95%CI: 0.49-0.69), respectively.
Patient characteristics are presented in Supplementary Table 1.
We also generated simulated survival data sets for TNBC using Adjuvant!Online (AO)
predictions (20) to vary the baseline prognosis of the trial population. In these data sets all
patients were designated as 60 years of age with average comorbidities, grade 3, ER negative
cancers and treated with 3rd generation adjuvant chemotherapy (i.e. control arm). Clinical tumor
size and clinical nodal status were considered in brackets of increasing disease burden T1bN0,
T1cN0, T2N0, or T2N1. Adjuvant!Online only provides recurrence free survival (RFS) estimates
and not DRFS, therefore in these data sets we report RFS as outcome. The overall 10-year RFS
associated with the 4 distinct prognostic groups were 0.782, 0.741, 0.657, and 0.548, respectively
(Table 1).
Statistical analysis
Research. on June 7, 2020. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 18, 2015; DOI: 10.1158/1078-0432.CCR-14-3304

9
We used biased bootstrap resampling to simulate 1:1, two-arm randomized clinical trial
scenarios with N=127 patients per arm. For each scenario, 1000 bootstrap replicates were drawn
from the reference cohort with replacement, stratified by response group to keep the pCR rate at
35% in the control arm. To simulate the experimental arm, 1000 different datasets were
generated from the same TNBC reference cohort using biased resampling of the pCR and RD
groups from the TNBC reference cohort to achieve various pre-specified pCR rates. This
simulation strategy requires two assumptions: (i) the survival of cases with pCR is similar
regardless of which treatment arm they are, and (ii) the survival of patients with residual disease
is also similar in both arms. These assumptions are supported by observations from several
randomized neoadjuvant clinical trials. (2,17) We used the Kaplan-Meier estimator and
univariate Cox regression to estimate the 5-year DRFS for the control and experimental arms and
the treatment-related DRFS hazard ratio, respectively. Means and 95% confidence intervals were
estimated from the 1000 bootstrapped datasets for each scenario. The power to detect a
significant DRFS hazard ratio was estimated by the proportion of datasets for which the Wald
statistic for the hazard ratio was significant (p<0.05). The bootstrap procedure is equivalent to
generating event and censoring times from the Kaplan-Meier estimator of the survival and
censoring distributions.(21, 22)
To evaluate the effect of baseline prognosis on survival, we generated cohorts for the
control arm that matched the 10-year RFS predicted by Adjuvant!Online for the specified patient
characteristics. We further assumed independent exponential relapse times for the pCR and RD
patient groups in either arm.(23) We assumed that the pCR rate for the control arm (TNBC
treated with 3rd generation chemotherapy) is 30% and that the 10-year RFS of patients who
achieved pCR is 82% for both arms corresponding to an exponential hazard rate of 0.0198
Research. on June 7, 2020. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 18, 2015; DOI: 10.1158/1078-0432.CCR-14-3304

10
(events/year).(19) Under these assumptions, the survival function of the entire cohort for each
arm will be the mixture of the survival functions of the pCR and RD groups. Based on this we
then calculated the 10-year RFS of patients with RD as
(10| ) = 11 − (10) − 1 − (10| )
where (10) is the 10-year RFS for the overall cohort as predicted by Adjuvant! Online, (10| ) and (10| ) are the 10-year RFS for the pCR and RD subgroups and is the
pCR rate. The exponential hazard rate for the RD group is then estimated as = − ( | ). The values used in the simulated scenarios are summarized in Table 1. We modeled censoring
times for both pCR and RD cohorts as being distributed according to an exponential distribution
with rate = 0.5 , which corresponded to the censoring pattern observed in our reference
cohort. The R (v.3.2.0) statistical software was used for all computations.(24)
Results
The relationship between trial-level pCR rate and survival benefit
We consider a two-arm randomized neoadjuvant trial where the experimental treatment has
greater cytotoxic efficacy compared to the control treatment, as reflected by an increase in pCR
rate of ∆ (Figure 1). If the survival functions for the control and experimental arms are ( )
and ( ), then ( ) = ( | ) + (1 − ) ( | ) and ( ) = ( + Δ ) ( | ) + (1 − − Δ ) ( | )
Assuming that the survival outcome of patients with pCR is the same in both treatment arms, the
survival benefit at the study level is
Research. on June 7, 2020. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 18, 2015; DOI: 10.1158/1078-0432.CCR-14-3304

11
Δ ( ) = ( ) − ( ) = Δ ( | ) − ( | ) + (1 − ) ( | ) − ( | ) ,
indicating a linear association between trial-level survival benefit (Δ ) and improvement in
pCR rate (∆ ), conditional on all other prognostic factors between the two arms being held equal.
The magnitude of the trial-level survival benefit derived from an improvement in pCR is driven
by the patient-level survival benefit between the pCR and RD groups in the experimental arm. If
the baseline prognosis of the overall patient cohort is good, the difference in outcome between
pCR and RD groups can only be small and therefore even a large ∆ translates into a minimal
trial-level survival benefit. A more effective cytotoxic therapy, in addition to pushing more
patients into the pCR response category, may also reduce the extent of residual disease in those
patients who did not achieve pCR. The second term in the expression is the secondary
contribution of this residual disease down staging on the trial-level survival benefit.
Association between odds for pCR and DRFS benefit in TNBC
Figures 2A and 2B illustrate a scenario where doubling of the pCR rate (from 35% to 70%) is
accompanied by a sizable patient level survival benefit (Figure 2A) yet it translates into only a
small improvement in trial-arm level survival (Figure 2B).
The impact of pCR odds ratio (OR) on the DRFS hazard ratio (HR) and DRFS difference
at 5 years was determined through simulations of a large number of trial scenarios. Higher OR
results in smaller DRFS hazard ratios (Figure 2C) or greater DRFS difference at 5 years (Figure
2D). Power analysis suggests that an experimental treatment that increases the pCR rate from
35% to 65% (pCR OR of 3.45) would have a 50%, 76%, and 90% power to detect a significant
survival benefit at the 95% confidence level in 1:1 randomized trials with 127, 250 or 350
patients per arm, respectively (Figure 2E). These results suggest that the power to detect
Research. on June 7, 2020. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 18, 2015; DOI: 10.1158/1078-0432.CCR-14-3304

12
significant survival HR effect is quite low (<50%) for studies with less than 350 patients per arm
unless the pCR OR is high (OR > 2).
Power to detect significant survival benefit does not only depend on pCR odds ratio but also on
the baseline prognosis of patients
To evaluate how baseline prognostic risk impacts the trial-level survival benefit, we simulated a
series of scenarios where the baseline prognosis of patients differed by adjusting anatomical risk
variables (T size and N stage). We assumed a pCR rate of 30% in the control arm for all baseline
risk groups, as the effect of tumor size and nodal status on pCR rate is modest.(16) The study-
level survival benefit, measured by the difference in 10-year RFS, increased with increasing pCR
rate effect but was considerably larger in patients with the worst prognosis (T3N2 – Figure 3A).
A 100 patient per arm randomized trial that includes only T1cN0 patients, or any patient
population with similar good baseline prognosis, would fail to show significant survival benefit
unless the absolute pCR rate increase is > 60% (corresponding to an OR > 20; Figure 3A). Even
studies with 1000 patients per arm would require an absolute pCR increase > 40% (OR > 5.4) to
demonstrate a significant survival benefit in a good risk patient population (Figure 3A). Figure
3B provides a more systematic exploration of the effect of baseline prognostic characteristics on
the power to detect significant survival benefit. It shows that if a trial targets high-risk patients
only, clinically T3N2 or similar high risk population, then 300 patients per arm could yield 80%
power to detect significant survival benefit for an absolute pCR rate increase of > 20%
corresponding to an OR of 2.3.
Table 2 provides sample size estimates for 1:1 randomized trials to detect a significant
improvement at 5% significance level in trial-level RFS with 80% or 90% power as a function of
Research. on June 7, 2020. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 18, 2015; DOI: 10.1158/1078-0432.CCR-14-3304

13
(i) the improvement in pCR in the experimental arm and (ii) the overall baseline risk of the trial
population. Power estimates for the extreme hypothetical scenario of 100% pCR in the
experimental group versus 0% pCR in the control group are provided in Supplemental Table 2
for comparison. Even in this unrealistic scenario, a study involving only low risk T1cN0 patients
will require 333 patients to show significant survival benefit with 80% power. It is apparent that
the size of a phase III trial powered to demonstrate significant survival benefit depends not only
on the expected pCR rate improvement but also to a large degree on the baseline risk of the
treated cohort.
Discussion
There is confusion and contradictory data in the literature about how increase in pCR rate may
impact survival difference between arms in a randomized trial. We show that trial-level survival
benefit is a complex function of many factors beyond the difference in pCR rate. We used
survival data from real patients participating in neoadjuvant studies and simulated patient
outcome derived from AdjuvantOnline estimates to assess the relationship between pCR rate and
survival for TNBC. Assuming that the survival outcome is similar for those who achieve pCR
regardless of which treatment arm they are in a linear relationship exists between trial-level pCR
rate effect and RFS benefit. The slope is equal to the difference in survival between those with
pCR and RD, or the patient-level survival benefit, in the experimental arm, which in turn is
influenced by the baseline prognosis of the trial population and the effectiveness of post-
neoadjuvant therapies. Patients with favorable TNM stage derive little benefit from even highly
efficacious neoadjuvant therapies. Similarly, patients with highly endocrine sensitive cancers
Research. on June 7, 2020. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 18, 2015; DOI: 10.1158/1078-0432.CCR-14-3304

14
will derive a large survival benefit from adjuvant endocrine therapy and therefore their initial
response to neoadjuvant cytotoxic therapy is less important.
There are molecular variables that could simultaneously influence both the probability of
achieving pCR and the prognostic risk of a patient (i.e. risk of recurrence in the absence of any
systemic therapy). For example, high tumor proliferation rate is associated with higher
probability of pCR but also with worse prognosis, (25) while high tumor infiltrating lymphocyte
count is associated higher pCR rate and also better prognosis.(26, 27) Many similar, yet to be
identified, interactions between prognostic markers and pCR may exist. Some could be breast
cancer subtype specific and may also differ by treatment and hard to model. (28) We focused our
analysis on TNBC because the pCR and survival relationship is the clearest in this disease subset
due to the lack of effective post-neoadjuvant systemic therapies. We also assumed that the
experimental therapy behaves like a third generation chemotherapy in terms of its hidden
interaction with prognostic and predictive markers but it is more effective. This implies that the
power and sample size relationship that we report here could be different for neoadjuvant
therapies that have substantially different mechanism of action because different interactions
could exist between the experimental therapy and prognostic and predictive markers. Our model
relies on a commonly used constant hazard function to generate exponential survival estimates,
although we recognize that the hazard of distant recurrence for TNBC peaks initially and then
diminishes over time.
We recognize that clinical trials accrue patients with different baseline prognoses, and we
selected a set of specific T/N stage groups to illustrate the dependence on baseline prognosis of
the trial population and to provide some general guidelines. Power calculations for actual trials
will have to consider the specific TNM stage distribution of the intended patient population.
Research. on June 7, 2020. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 18, 2015; DOI: 10.1158/1078-0432.CCR-14-3304

15
We did not elaborate in our analysis on the effects of down staging of residual cancer on
the association between pCR and survival benefit. An effective treatment could improve survival
in the RD group by reducing the amount of residual disease without affecting the overall pCR
rate resulting in a smaller trial-level survival benefit. Alternatively, a treatment could increase
the pCR rate by shifting patients with minimal residual cancer into the pCR category which
would impact the net survival benefit only marginally as patients with minimal residual cancer
burden have the same excellent prognosis as patients who achieve pCR.(6) The net effect of
residual cancer down staging on the association between pCR rate and trial-level survival will
need to be evaluated in neoadjuvant studies that also monitor levels of residual disease.
In summary, our results indicate that modest improvements in pCR rate translate into
very small improvements in survival in low and moderate risk trial populations, consistent with
the existing literature. Almost all trials included in the CTNeoBC pooled analysis had pCR OR <
1.5 and included many ER positive patients. These results do not undermine the value of pCR as
an efficacy measure to identify more effective cytotoxic therapies in early stage breast cancer but
highlight the importance of selectively administering more effective novel treatments to those
who remain high risk for recurrence despite current best therapies.
Research. on June 7, 2020. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 18, 2015; DOI: 10.1158/1078-0432.CCR-14-3304

16
References
1. Kuerer HM, Newman LA, Smith TL, Ames FC, Hunt KK, Dhingra K, et al. Clinical
course of breast cancer patients with complete pathologic primary tumor and axillary lymph
node response to doxorubicin-based neoadjuvant chemotherapy. Journal of clinical oncology :
official journal of the American Society of Clinical Oncology. 1999;17:460-9.
2. Rastogi P, Anderson SJ, Bear HD, Geyer CE, Kahlenberg MS, Robidoux A, et al.
Preoperative chemotherapy: updates of National Surgical Adjuvant Breast and Bowel Project
Protocols B-18 and B-27. Journal of clinical oncology : official journal of the American Society
of Clinical Oncology. 2008;26:778-85.
3. von Minckwitz G, Untch M, Blohmer JU, Costa SD, Eidtmann H, Fasching PA, et al.
Definition and impact of pathologic complete response on prognosis after neoadjuvant
chemotherapy in various intrinsic breast cancer subtypes. Journal of clinical oncology : official
journal of the American Society of Clinical Oncology. 2012;30:1796-804.
4. Wolmark N, Wang J, Mamounas E, Bryant J, Fisher B. Preoperative chemotherapy in
patients with operable breast cancer: nine-year results from National Surgical Adjuvant Breast
and Bowel Project B-18. Journal of the National Cancer Institute Monographs. 2001;30:96-102.
5. Mazouni C, Kau SW, Frye D, Andre F, Kuerer HM, Buchholz TA, et al. Inclusion of
taxanes, particularly weekly paclitaxel, in preoperative chemotherapy improves pathologic
complete response rate in estrogen receptor-positive breast cancers. Annals of oncology : official
journal of the European Society for Medical Oncology / ESMO. 2007;18:874-80.
6. Symmans WF, Peintinger F, Hatzis C, Rajan R, Kuerer H, Valero V, et al. Measurement
of residual breast cancer burden to predict survival after neoadjuvant chemotherapy. Journal of
Research. on June 7, 2020. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 18, 2015; DOI: 10.1158/1078-0432.CCR-14-3304

17
clinical oncology : official journal of the American Society of Clinical Oncology. 2007;25:4414-
22.
7. Green MC, Buzdar AU, Smith T, Ibrahim NK, Valero V, Rosales MF, et al. Weekly
paclitaxel improves pathologic complete remission in operable breast cancer when compared
with paclitaxel once every 3 weeks. Journal of clinical oncology : official journal of the
American Society of Clinical Oncology. 2005;23:5983-92.
8. Sparano JA, Wang M, Martino S, Jones V, Perez EA, Saphner T, et al. Weekly paclitaxel
in the adjuvant treatment of breast cancer. The New England journal of medicine.
2008;358:1663-71.
9. Buzdar AU, Ibrahim NK, Francis D, Booser DJ, Thomas ES, Theriault RL, et al.
Significantly higher pathologic complete remission rate after neoadjuvant therapy with
trastuzumab, paclitaxel, and epirubicin chemotherapy: results of a randomized trial in human
epidermal growth factor receptor 2-positive operable breast cancer. Journal of clinical oncology :
official journal of the American Society of Clinical Oncology. 2005;23:3676-85.
10. Slamon D, Eiermann W, Robert N, Pienkowski T, Martin M, Press M, et al. Adjuvant
trastuzumab in HER2-positive breast cancer. The New England journal of medicine.
2011;365:1273-83.
11. Gianni L, Eiermann W, Semiglazov V, Manikhas A, Lluch A, Tjulandin S, et al.
Neoadjuvant chemotherapy with trastuzumab followed by adjuvant trastuzumab versus
neoadjuvant chemotherapy alone, in patients with HER2-positive locally advanced breast cancer
(the NOAH trial): a randomised controlled superiority trial with a parallel HER2-negative cohort.
Lancet. 2010;375:377-84.
Research. on June 7, 2020. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 18, 2015; DOI: 10.1158/1078-0432.CCR-14-3304

18
12. ASCO. FDA Approves Pertuzumab for Neoadjuvant Breast Cancer. 2013 October 1,
2013 [cited; Available from: http://www.asco.org/advocacy/fda-approves-pertuzumab-
neoadjuvant-breast-cancer
13. Prowell TM, Pazdur R. Pathological complete response and accelerated drug approval in
early breast cancer. The New England journal of medicine. 2012;366:2438-41.
14. Earl HM, Vallier AL, Hiller L, Fenwick N, Young J, Iddawela M, et al. Effects of the
addition of gemcitabine, and paclitaxel-first sequencing, in neoadjuvant sequential epirubicin,
cyclophosphamide, and paclitaxel for women with high-risk early breast cancer (Neo-tAnGo): an
open-label, 2x2 factorial randomised phase 3 trial. The lancet oncology. 2014;15:201-12.
15. von Minckwitz G, Schneeweiss A, Loibl S, Salat C, Denkert C, Rezai M, et al.
Neoadjuvant carboplatin in patients with triple-negative and HER2-positive early breast cancer
(GeparSixto; GBG 66): a randomised phase 2 trial. The lancet oncology. 2014;15:747-56.
16. Cortazar P, Zhang L, Untch M, Mehta K, Costantino JP, Wolmark N, et al. Pathological
complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis.
Lancet. 2014;384:164-72.
17. Piccart-Gebhart M, Holmes AP, Baselga J, De Azambuja E, Dueck AC, Viale G, et al.
First results from the phase III ALTTO trial (BIG 2-06; NCCTG [Alliance] N063D) comparing
one year of anti-HER2 therapy with lapatinib alone (L), trastuzumab alone (T), their sequence (T
→L), or their combination (T+L) in the adjuvant treatment of HER2-positive early breast cancer
(EBC). Journal of clinical oncology : official journal of the American Society of Clinical
Oncology. 2014;32:suppl; abstr LBA4.
Research. on June 7, 2020. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 18, 2015; DOI: 10.1158/1078-0432.CCR-14-3304

19
18. Baselga J, Bradbury I, Eidtmann H, Di Cosimo S, de Azambuja E, Aura C, et al.
Lapatinib with trastuzumab for HER2-positive early breast cancer (NeoALTTO): a randomised,
open-label, multicentre, phase 3 trial. Lancet. 2012;379:633-40.
19. Symmans WF, Wei C, Gould R, Zhang Y, Hunt KK, Buchholz TA, et al. Long-term
prognostic value of residual cancer burden (RCB) classification following neoadjuvant
chemotherapy. Cancer Res. 2013;73:S6-02.
20. Ravdin PM, Siminoff LA, Davis GJ, Mercer MB, Hewlett J, Gerson N, et al. Computer
program to assist in making decisions about adjuvant therapy for women with early breast cancer.
Journal of clinical oncology : official journal of the American Society of Clinical Oncology.
2001;19:980-91.
21. Efron B. Censored data and the bootstrap. J Am Stat Assoc. 1981;76:312-9.
22. Akritas MG. Bootstrapping the Kaplan-Meier estimator. J Am Stat Assoc. 1986;81:1032-
8.
23. Bender R, Augustin T, Blettner M. Generating survival times to simulate Cox
proportional hazards models. Statistics in medicine. 2005;24:1713-23.
24. R Core Team. R: A language and environment for statistical computing. Vienna, Austria:
R Foundation for Statistical Computing; 2015.
25. Iwamoto T, Lee JS, Bianchini G, Hubbard RE, Young E, Matsuoka J, et al. First
generation prognostic gene signatures for breast cancer predict both survival and chemotherapy
sensitivity and identify overlapping patient populations. Breast cancer research and treatment.
2011;130:155-64.
26. Denkert C, Loibl S, Noske A, Roller M, Muller BM, Komor M, et al. Tumor-associated
lymphocytes as an independent predictor of response to neoadjuvant chemotherapy in breast
Research. on June 7, 2020. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 18, 2015; DOI: 10.1158/1078-0432.CCR-14-3304

20
cancer. Journal of clinical oncology : official journal of the American Society of Clinical
Oncology. 2010;28:105-13.
27. Loi S, Sirtaine N, Piette F, Salgado R, Viale G, Van Eenoo F, et al. Prognostic and
predictive value of tumor-infiltrating lymphocytes in a phase III randomized adjuvant breast
cancer trial in node-positive breast cancer comparing the addition of docetaxel to doxorubicin
with doxorubicin-based chemotherapy: BIG 02-98. Journal of clinical oncology : official journal
of the American Society of Clinical Oncology. 2013;31:860-7.
28. Andre F, Hatzis C, Anderson K, Sotiriou C, Mazouni C, Mejia J, et al. Microtubule-
associated protein-tau is a bifunctional predictor of endocrine sensitivity and chemotherapy
resistance in estrogen receptor-positive breast cancer. Clin Cancer Res 2007; 13:2061-2067.
Research. on June 7, 2020. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 18, 2015; DOI: 10.1158/1078-0432.CCR-14-3304

21
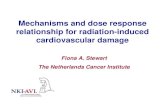
Figure Legends Figure 1. Patient-level (first plot) versus trial-level (second plot) survival analysis for a 1:1 two
arm randomized clinical study. Patient-level analysis shows a survival benefit associated with
patients who achieve pathologic complete response (pCR) compared to patients who have
residual disease (RD). The trial-level survival benefit in the experimental treatment arm depends
on the increase in pCR rate and also on the patient-level survival benefit, which varies depending
on baseline prognostic risk of the trial population. In both clinical trial scenarios shown, the pCR
rate increase in the experimental arm is 20% (pCR odds ratio = 2.33), but scenario A is assumed
to involve a low prognostic risk population (T1c, N0), whereas scenario B a high risk population
(T3, N2). The prognostic risk characteristics of these populations are shown in Table 1. The
survival functions of the pCR and RD groups are assumed to be exponentials.
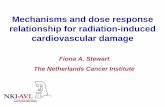
Figure 2. The Kaplan-Meier plots in panel A illustrate patient-level survival by responder group
in each arm (pCR subgroups shown in solid lines and RD subgroups in dashed lines), and panel
B shows the trial-level survival of the two arms for one typical bootstrap sample in the MDACC
TNBC cohort. The control arms (n=127) were generated through unbiased stratified bootstrap to
have 35% pCR rate, and the experimental arms were generated by biased bootstrap resampling to
yield a pCR rate of 70%. The association between pCR odds ratio and trial-level survival benefit
in terms of the DRFS hazard ratio or the difference in 5-yr DRFS between the study arms is
shown in panels C and D, respectively. The points represent the means and the vertical lines the
95% confidence intervals of the survival outcome estimates obtained by 1000 bootstrap
replicates. Panel E shows the power to detect significance in DRFS hazard ratio at 95%
Research. on June 7, 2020. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 18, 2015; DOI: 10.1158/1078-0432.CCR-14-3304

22
confidence level as a function of pCR odds ratio for studies of different sample sizes (number of
patients per arm: circles: N=127, triangles: N=250, squares: N=350).
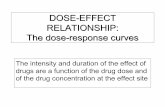
Figure 3. Power to detect significant survival benefit from scenarios for 1:1 randomized trials
involving TNBC patient cohorts with different baseline risk. Simulated scenarios included 30 to
3200 patients per arm. The pCR rate of the control arm was set at 30% and the 10-year RFS of
patients with pCR to 82%. Ten-year RFS estimates of four different prognostic risk populations
T1cN0 (circles), T2N1 (triangles), T3N1 (squares), and T3N2 (crosses) were obtained from
Adjuvant! Online and listed in Table 1. Panels show the estimated power to detect by Cox
proportional hazards based on the Wald test a significant RFS hazard ratio between the
experimental and control arms of the trial as a function of the between-arm difference in pCR
rate, the baseline prognosis of the trial population, and the number of patients per study arm (N).
Research. on June 7, 2020. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 18, 2015; DOI: 10.1158/1078-0432.CCR-14-3304

Figure 1
A
B
Research. on June 7, 2020. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 18, 2015; DOI: 10.1158/1078-0432.CCR-14-3304

Figure 2
Research. on June 7, 2020. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 18, 2015; DOI: 10.1158/1078-0432.CCR-14-3304

N = 30 N = 60 N = 100
N = 180 N = 320 N = 560
N = 1000 N = 1800 N = 3200
0.00
0.25
0.50
0.75
1.00
0.00
0.25
0.50
0.75
1.00
0.00
0.25
0.50
0.75
1.00
0.2 0.4 0.6 0.2 0.4 0.6 0.2 0.4 0.6
Difference in pCR Rate (Experimental - Baseline)
Po
we
r
Baseline Group
T1c,N0
T2,N1
T3,N1
T3,N2
Figure 3
N = 100
N = 320
N = 1000
0.0
0.2
0.4
0.0
0.2
0.4
0.0
0.2
0.4
0.2 0.4 0.6
Difference in pCR Rate
RF
S D
iffe
ren
ce
at
10
ye
ars
A B
Research. on June 7, 2020. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 18, 2015; DOI: 10.1158/1078-0432.CCR-14-3304

Table 1. Patient parameters used in simulated scenarios (all scenarios assumed 60-year
old patients with average comorbidities and grade 3 ER-negative tumors treated with 3rd
generation chemotherapy with a pCR rate of 30%).
Clinical T-stage
Clinical N-stage
10-year RFS Hazard Rate (1/year)
Overall (Adjuvant!
online)
pCR cohort
RD cohort
pCR cohort RD cohort
T1c N0 0.741 0.82 0.707 0.0198 0.0347
T2 N1 0.545 0.82 0.427 0.0198 0.0851
T3 N1 0.456 0.82 0.300 0.0198 0.1204
T3 N2 0.350 0.82 0.149 0.0198 0.1908
Research. on June 7, 2020. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 18, 2015; DOI: 10.1158/1078-0432.CCR-14-3304

Table 2. Sample size per arm required for 1:1 randomized trials to detect improvement
in trial-level RFS at an one-sided 5% significance level as a function of the overall
baseline risk of the trial population and the improvement in pCR rate in the experimental
arm (the pCR rate of control arm is assumed to be 30% and the 10-year RFS of the pCR
subgroup to be 82%). The power to detect significant survival benefit between treatment
arms using unadjusted Cox proportional hazards regression analysis based on the Wald
test (hazard ratio for RFS between arms < 1) was estimated by 1000 simulations of each
baseline and pCR improvement scenarios with study sizes ranging from 30 to 3200
patients per arm. Natural spline interpolation was then used to obtain the sample sizes for
80% and 90% power. No adjustments were made for patient accrual time.
Baseline Risk Group
Power Improvement in pCR Rate in Experimental Arm
0.1 0.2 0.3 0.4 0.5 0.6
T1cN0 0.8 >4,000 >4,000 2680 1551 929 673
0.9 >4,000 >4,000 3554 2056 1258 903
T2N1 0.8 3078 717 315 168 105 71
0.9 >4,000 942 425 223 137 94
T3N1 0.8 1788 460 186 103 66 46
0.9 2320 598 247 136 88 58
T3N2 0.8 1122 284 124 75 45 31
0.9 1488 364 159 95 56 42
Research. on June 7, 2020. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 18, 2015; DOI: 10.1158/1078-0432.CCR-14-3304

Published OnlineFirst August 18, 2015.Clin Cancer Res Christos Hatzis, W. Fraser Symmans, Ya Zhang, et al. cancer
breastneoadjuvant chemotherapy and survival in triple negative Relationship between complete pathologic response to
Updated version
10.1158/1078-0432.CCR-14-3304doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2016/01/05/1078-0432.CCR-14-3304.DC1
Access the most recent supplemental material at:
Manuscript
Authoredited. Author manuscripts have been peer reviewed and accepted for publication but have not yet been
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/early/2015/08/18/1078-0432.CCR-14-3304To request permission to re-use all or part of this article, use this link
Research. on June 7, 2020. © 2015 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on August 18, 2015; DOI: 10.1158/1078-0432.CCR-14-3304









![pine Dose Response Relationship in.4[1]](https://static.fdocuments.net/doc/165x107/577d26eb1a28ab4e1ea28d3e/pine-dose-response-relationship-in41.jpg)





