Rehabilitation in surgery - upjs.sk
68
Rehabilitation in surgery
Transcript of Rehabilitation in surgery - upjs.sk

Rehabilitation in
surgery





















Rehabilitation after surgery
Enhanced Recovery After Surgery

What is ERAS?
• Or Fast-track
• Developed by Kehlet in Denmark in colonic
surgery
• Gradually has gained world-wide acceptance
• Originally described in Open Surgery but same
advantages seem to apply for Laparoscopy

Enhance (vb) (tr) to intensify or increase in quality, value,
power, etc.; improve; augment
In practice, usually equated and quantified in terms of
time/speed: Length of Stay
Hot topic for NHS managers Can be applied to colorectal, urology, gynae and musculosketal surgery

What is Enhanced
Recovery?• Minimise stress
responses during & after
surgery
• Optimise pre-op condition
• Optimise peri-operative
care
• Optimise post-op
rehabilitation
Time
Function
Traditional care
Enhanced Recovery

• Pre-operatively: Other health
problems are identified & managed to
enable the patient to be in the best
possible condition for surgery
• Intra-operatively: Best possible
evidence based management is given
to the patient during and after surgery
• Post-operatively: Patients are
encouraged with early mobilisation
and timely discharge for the best
rehabilitation with support
Goals of FAST TRACK SURGERY
• Lower risk, better outcome
• Accelerate recovery
• Reduce morbidity, complications
(pulmonary, cardiac, thromboembolic,
infectious)
• Shorten convalescence
• Less expensive healthcare

Factors influencing
patient recoveryPre-op informationOptimised organ functionNo nutritional defectsNo alcohol pre-opStop smoking pre-opNeuraxial blockadeMinimally invasive surgeryNormothermiaNausea preventionIleus preventionEarly feedingGood oxygenationGood sleepOpioid sparingEvidence-based post-op care
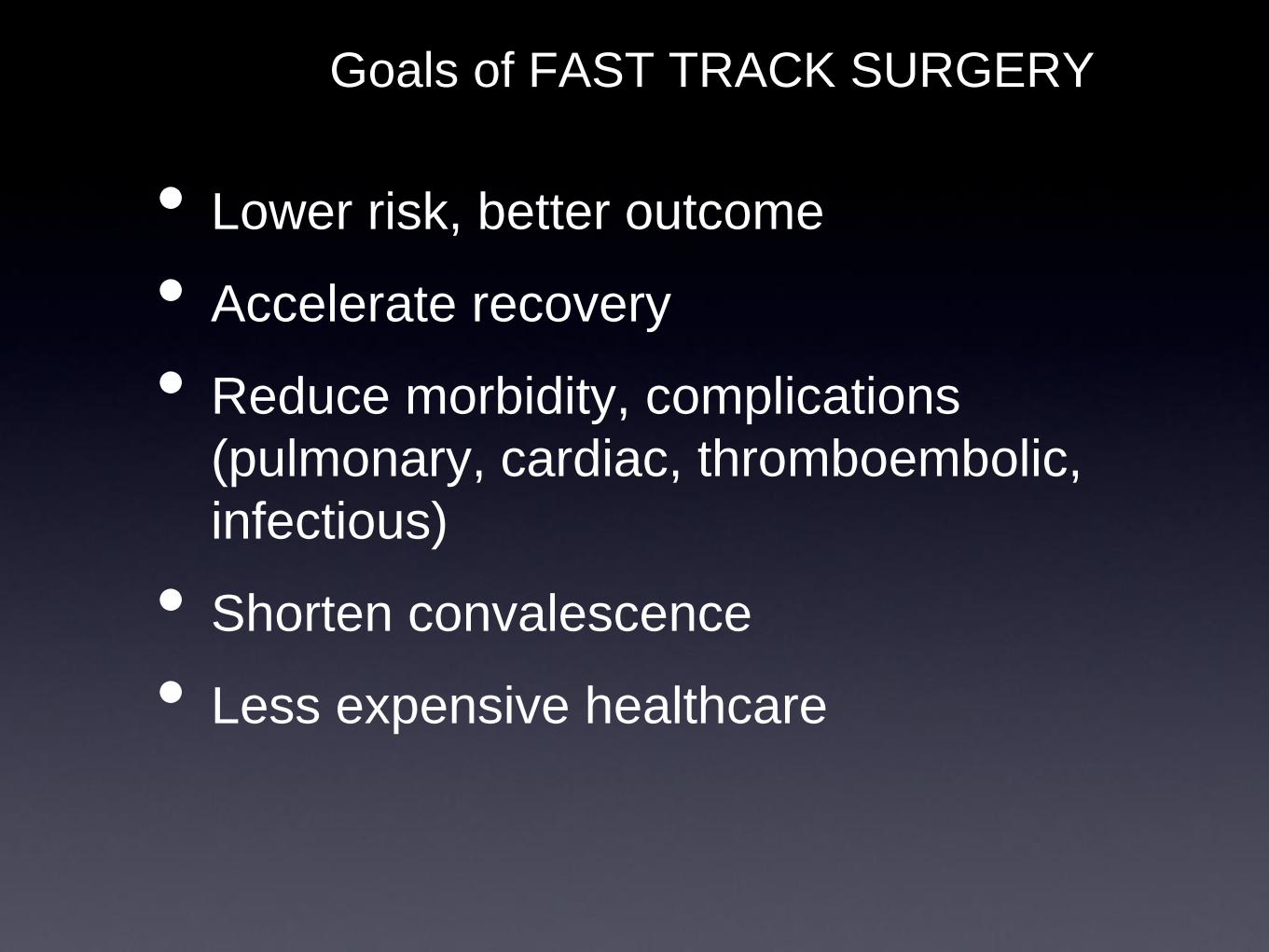
Referral from
Primary Care
Pre-
Operative
Admission
Operative
Post-
Operative
Follow-up
•Optimising pre-operative
haemoglobin levels
•Managing pre-existing co-
morbidities eg Diabetes
•Discharge on
planned day
•Therapy input
(stoma / physio /
dietician)
•Audit & outcome
measures
•Planned mobilisation
•Rapid hydration & nourishment
•Appropriate iv therapy
•No wound drains
•No NGT (bowel surgery)
•Catheters removed early
•Regular oral analgesia
•Avoid opiates
•Day of surgery
admission
•Reduced starvation
/ CHO load
•Optimise fluid
hydration
•No pre-med/bowel
prep
•Minimally invasive surgery
•Transverse incisions
•Avoid nasogastric tubes
•Use of LA/ Regional
analgesia with sedation
•Epidural (thoracic)
•Optimised fluid therapy
•Optimised health /
medical conditions
•Informed decision-
making
•Pre-operative health
& risk assessment
•Patient well-informed
/ expectations
managed
•Stoma training
•Discharge planning
(EDD)

What is ERAS?

Patient Information
• At the clinic
Carbohydrate drinks
• 4 night before surgery if having bowel prep
• 2 morning of the surgery
No mechanical bowel preparation
Patients admitted on the morning of surgery
Pre-op

Thoracic Epidural Analgesia
Incision choice
• Transverse for R) sided
• Mid-line or Laparoscopic for L) sided
Avoidance of Drains and NGT post-operatively
Limited Intra-Operative fluid therapy
• Aiming to max of 1.5-2 L
Surgery

IVF
• unless clinically indicated
• Pressors for epidural hypotension
Regular pre-emptive antiemetics
• ondansetron as first line
On arrival to the departement
Patient sits up
• Starts drinking protein drinks (Resource/Fortisip etc)
After surgery

• Solids until 6 hours before surgery
• Clear fluids until 2 hours before surgery
• Safe
• Beneficial
• Carbohydrate-loaded liquid pre-op
• post-op catabolism
• insulin resistance, hyperglycemia
• muscle loss

Early Feeding
• Start clear fluids 2h post-op
• Aim > 800mL fluids on day of surgery
• Routine nutritional supplements
• IV appropriately, avoid fluid overload,
• Length of time a patient can remain NPO
after surgery without complications is
uknown, however depends on:
• Severity of operative stress
• Patient’s preexisting nutritional status
• Nature and severity of illness
• Two types of nutritional support
• Enteral
• Parenteral

Day 1
• Urine catheter removed in the morning
• 8 hrs of enforced mobilisation
• Resumes normal diet
• Pre-emptive oral analgesia is started
• Paracetamol and NSAIDs
• Avoid Opioids
Day 2
• Epidural infusion is stopped in the morning
• Epidural Catheter is removed if pain controlled, and
timed with Clexane dose

Day 3/4 - discharge criteria:
• Return of GI function
• Able to eat and drink without discomfort
• Passing flatus
• Pain controlled with oral analgesia
• Adequate home support
Discharge date is an important target for
patients and staff but flexibility is vital

What is Cardiac
Rehabilitation? • It is defined as, “all measures used to help
cardiac patients return to an active and
satisfying life and to prevent re-ocurrence
of cardiac events”.
• Cardiac Rehabilitation includes exercise,
education, and social and emotional
support.
• Rehabilitation can be hospital or home
based.

Rehabilitation Outcome and Quality of
Life• The benefits include psychological well being, reduction in mortality, improvement in quality of life, and lowering of hospital re-admission rates, with the prevention of reoccurrence of future cardiac events
• Cardiac rehabilitation lowers the risk of death in survivors by 20-25%
• Cardiac rehab also decreases the need for medication
• Improves exercise tolerance, coronary risk factors, physiological well being and health related quality of life, as well as reducing long term mortality

Complication due to Non-
Rehabilitation• Reoccurrence of cardiac events
• Re-hospitalization due to re-occurrence of
cardiac event with high cost of treatment
• Decreased quality of life
• Increased need for medication
• Increased risk of death
• Increased risk for co-morbidity
• Predisposition to blood clotting from stasis

Standard Interventions
• Cardiac rehab staff nurse will meet patient prior to discharge from hospital and address the rehabilitation program protocol.
• rehabilitation consists of forty exercise sessions; 24 sessions (3/per week) endurance training on a cycle ergometer ( with 5 minute warm up) 20 min training with constant workload, 5 minute cool down, and 5 min post exercise monitoring. In addition 16, (2/per week) 1 hour sessions of stretching and flexibility exercises.

Goals for Rehabilitation Focus on 4 aspects of activities of daily
living:
i) Somatic goals – Teaching individuals
to
learn one’s optimal exercise limits
ii) Social goals – helping individuals to
reintegrate into family life with
optimal
reintegration regarding working,
household, hobbies and leisure
activities.

Goals for Rehabilitation (Con’t)
iii). Psychosocial goals – empowering
individuals by evaluating anxiety levels
and concerns towards cardiac exertion
during exercise, that may lead to negative
emotions.
iv). Secondary prevention goals – helping
individuals to modify risk behavior &
reinforce compliance to therapy
regimen

Give “advanced anticipatory guidelines”
towards expectations including advantages,
outcomes, side effects, possible
complications, how to monitor their own
pulse rates and maximum heart rates, and
how to recognize symptoms of over-exertion
(ex: muscle cramps, short of breath).
Assess patient’s stress level, emotional status,
and functional status every time the nurse
calls

Outcome measuring tools• Establish a baseline evaluation for cardiac rehabilitation.
• vital signs, pulse ox
• EKG
• BMI
• pulse ox with activities to monitor the need for oxygen.
• Re-hospitalization do to reoccurrence of a cardiac event.
• Establish daily patient journal to monitor patient
impression of daily improvement and level of
performance of ADL.
• Pre, intra, post –echocardiogram to evaluate ejection
fraction.

ERAS Results
Type of Operation Duration of stay
Carotid endarterectomy 1-2 days
Lung lobectomy 1-2 days
Prostatectomy 1-2 days
Colectomy 1-3 days
Aortic Aneurysm 3-4 days
Fast-track surgeryPersonal experience
• Day surgery/One day surgery
- hernia
- laparoscopy (diam< 3 cm)
- hemorrhoids
- thoracocenthesis

Fast-track surgery
Cholecystectomy

Fast-track surgeryPersonal experience
• Cholecystectomy
- medical history!
- admittance day of operation
- early mobilization: I°day
- drain: II°day
- discharge: II°-III° day

Pre-operative examinations
• Hemocromo – PT- PTT
• ECG > 40 years
• X ray chest > 60 years
• Electrolyte-urea -creatinina > 60 years
• Glycemia > 60 years
• Urine: only specific indication

Fast-track surgery
Thyroidectomy

Fast-track surgeryThyroidectomy
'Same-day' thyroid surgery. Results
after 805 thyroidectomies in a fast-
track program

Fast-track surgeryThyiroidectomy
…conclusions:
• Specialized centre
• Lobectomy or sub-total
• No total thyroidectomy
• No ASA 3

Fast-track surgeryPersonal experience• Thyiroydectomy
- Admittance day of operation
- Free nutritional intake until midnight
- Free oral fluid intake
- Drains: I°-II°day
- Discharge: II°-III° day

Fast-track surgery
Breast surgery

William Stewart Halsted1852 - 1922
Surgeon-in-chief Johns Hopkins Hospital
1890-1922



Fast-track surgeryPersonal experience.
• Brest surgery:
- Free oral intake
- Admittance day of operation
- Mobilization: I° day
- Drains: I°-V° day
- Discharge: I°-V° day

Fast-track surgery
Colon surgery
Fast-track surgeryColon
The “Coast trial” is an important multicentric randomized and controlled trial that shows an
hospital stay significantly decreased after laparoscopic surgery (5 days) respect to open
surgery (6 days)

Basse L et al. – Dis Colon Rectum 2004; 47: 271“Colonic surgery with accelerated rehabilitation or conventional care”
•Post-op. stay: II°-III° day
•Readmission: 20%

Morbility
Traditional Care 20-35%
Fast-track Rehabilitation < 10%
Wolfgang Schwenk – TATM 2007; 9: 43-44
“Editorial: principles of fast-track rehabilitation in
elective colonic surgery”

Fast-track surgery
Gastric surgery

Gastic surgery
• Free nutritional oral intake until midnight
• Naso-gastric tube: II°-III° day
• Urinary catheter: I° day
• Oral nutritional intake: IV°-VI° day
• Mobilization: I° day
• Discharge: VI°-VIII° day

Fast-track surgeryPersonal experience
• Lung surgery:
pneumothorax: II°-III° day
- VATS
wedge-resection: II°-III° day
- TAC-guidate needle biopsy: ambulat.
- Lobectomy: VII° day
- Pneumonectomy: IX°-X° day

La Fast-track surgery demands a motivated team:
- Anaesthesist- Surgeon- Dietician
- Physiologist- Nursing staff
- Home/Ambulatory care