
Increase healthcare social media engagement with content strategy (Geisinger Case Study)
Upload
oscar-hancockCategory
view
215download
0
Reforming the HealthCare Delivery System

Learning Objectives
1. Recognize the drivers that lead Geisinger to initiate reform of their healthcare delivery system
2. Identify best practices from Geisinger's program success to replicate in other organizations
3. Outline the Health Information Technology Geisinger utilizes to manage their population health
4. Summarize initial results achieved such as up to 25% reduction in admissions for patients with multiple chronic disease conditions such as Congestive Heart
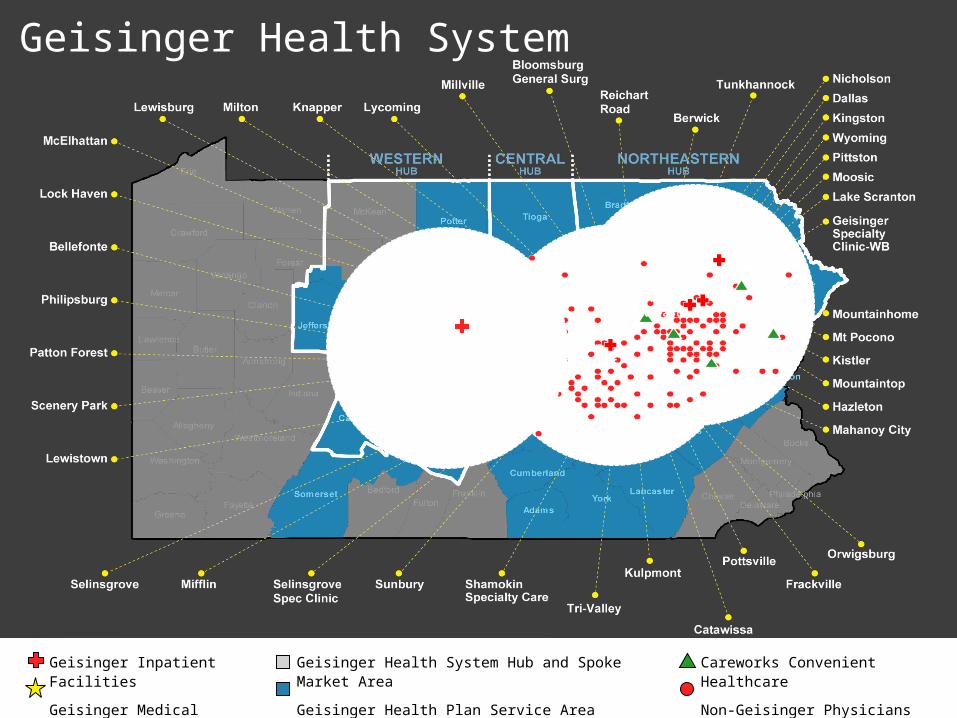
Geisinger Health System
Geisinger Inpatient Facilities
Geisinger Medical Groups
Geisinger Health System Hub and Spoke Market Area
Geisinger Health Plan Service Area
Careworks Convenient Healthcare
Non-Geisinger Physicians With EHR
Gray’s Woods

Geisinger Health System
• 2.6 million in service area • ~ 1000 physicians • 42 community practice sites• 2 hospitals • 300,000 health plan members• Healthcare IT and Informatics
– EPIC Ambulatory since 1998– Inpatient since 2007– OpTime, ED and other modules
• Data warehouse since 2009– Care Gap identification and closure


Digital Translation of Quality
Establish the Digital
Gold Standard
Adopt the Digital Gold
Standard
Maintain and
Optimize
Close Gaps in
Care

Care Plans
Populations
Leveraging Care Gaps
Action Arms
Lab and Imaging “Gap”
Management
Referral “Gap” Management
Care Gaps
Goals –Endpoints
Mammo every year
Prevention
Chronic Diseases
A1c 7- 8
Unclosed Loops
Abnormal Pap Follow up
Medication Safety
Methotrexate monitoring
Regular care “failures”
HF exacerbation
Office-Based Decision Support

Improving Care for 23,555 Diabetics

Improving CAD Care for 14,804 Patients

Improving Preventive Care for 210,681 Pats

Care Gaps Program
Population Health—Closing Care Gaps: – Close preventive, chronic and restorative care gaps for targeted patient
populations by age/gender, disease, or condition
Engaging Patients:– Patient & family-centric care coordination– Proactive– Technically elegant– Patient experience is personalized and warm
Transform Geisinger Culture by Leveraging Technology:– Data mining using evidence-based protocols & registries– Decision support (patient, clerical, nursing, provider-level)– Seamless connections (patient, PCP, specialty, ancillary, payor)– Strong relationships
“Geisinger knows and cares about me and my family”

Care Gaps Mission
Achieve ‘Best Outcomes in the Nation’
Patient Level Population Level Professional Level
– Lift clinician load by facilitating work outside of exam room
– Clinicians cheering for Care Gaps closed
Financial Level
Flawless Coordination, Execution, Partnerships
• Patients • Clinical Service Lines • Scheduling Services• Geisinger Health Plan• Marketing• IT• Research• Finance

Population Health: Auto Orders
Where we were: routine orders are placed by staff and providers in office visit [MANUAL PROCESS]
Where we’re now: auto-generate routine orders outside of the office visit [AUTOMATED PROCESS]– Standardized lab/imaging testing– Take work off of providers and nurses– Display open orders to clinic/scheduling staff to increase
opportunities to close care gaps

Contact Strategies
Method
Option 1: Single Contact Method
Option 2: Multiple Contact Methods
• Letters/Auto Letters
• Pt Portal Broadcast
• Personal Phone Calls
• Telephony Recorded Msg
• Telephony Warm Transfer
• Office Visit
Data Warehouse
Validate Data
Care Gaps Identified
Appoint Patient
Obtain Order/Referral (Auto Orders)

Benefits of Auto Orders
• Pts receive labs and imaging studies when due (monthly mining process)
• Ordering “work” is lifted from the office visit• Provides an opportunity to stage pt visits to the
lab or radiology through Care Gaps Outreach

Care Gaps Closed 19,257
Care Gaps YTD
$662,689
$2,262,264
$4,001,340
$2,481,788
$0
$500,000
$1,000,000
$1,500,000
$2,000,000
$2,500,000
$3,000,000
$3,500,000
$4,000,000
$4,500,000
Jul-10 Aug-10 Sep-10 Oct-10
0
5000
10000
15000
20000
25000
Net Revenue
Care Gaps Closed

Geisinger’s Medical Home Model enabled thru the Keystone Health Information Exchange

OUR BEACON COMMUNITY:IMPROVING HEALTHCARE COORDINATION

Profile of the Keystone Beacon Community• Serving 256,000 citizens in 5 counties of
Pennsylvania’s mostly rural Susquehanna Valley• 4 hospitals• More than 100 primary care physicians• More than 10 specialists• More than 100 physician offices• 2 long term care facilities• Long term acute care hospital• Home health care

Keystone Beacon Community Objectives• To reduce hospital readmissions in patients with
CHF and COPD• Provide immediate, secure access to patient
information • Reduce admissions and E.D. visits for patients
with conditions that could have been treated in an outpatient setting
• Link participants to the Keystone Health Information Exchange

Keystone Beacon Community Objectives
• To provide E. D. physicians and hospitals rapid access to patients who are new to your hospital
• To develop a robust database with critical information (including medication lists) on thousands of participating residents in Columbia, Montour, Northumberland, Snyder and Union counties

Electronic Health Record+ Health Information Exchange+ Care Coordination – Case Management
Process + Healthcare Providers + Patients + Care Coordinators – Case Managers ______________________________
Care Coordination Components

Electronic Health Record (EHR)
• Computerized version of patient’s clinical, demographic and administrative information
– Laboratory results– Immunizations– Diagnoses– Medications– Images– Allergies
• Stored in a secure electronic format• Requires healthcare providers to have a reason to
view it– s
– s
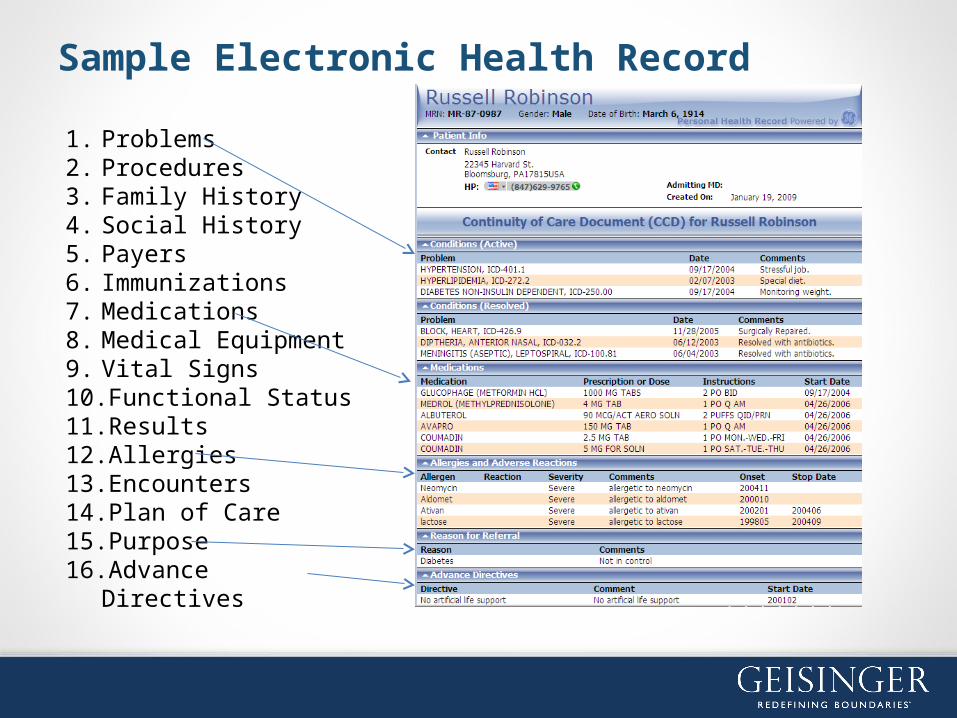
1. Problems2. Procedures3. Family History4. Social History5. Payers6. Immunizations7. Medications8. Medical Equipment9. Vital Signs10.Functional Status11.Results12.Allergies13.Encounters14.Plan of Care15.Purpose16.Advance Directives
Sample Electronic Health Record

Electronic channel between healthcare provider and patients that allows sharing of the electronic health record:
• Requires patient permission• Access limited to participating healthcare providers and
patient and patient designees (such as spouse, daughter, son)
– S
Health Information Exchange

What a shared EHR means to a patient in the emergency room…
It means that a patient who had surgery at Geisinger, post-surgical care at Riverwoods (L.T.C.) and is treated for chest pain at Evangelical Community Hospital has all his information in one place … in real time!
– S

What a shared EHR means to a patient taking multiple medications…
It means a healthcare provider can quickly see all the medications prescribed for a patient and reduces the likelihood of an additional medication being added that could cause an interaction.
– S

What a shared EHR means to someonewho is out of town…
It means a healthcare provider at a healthcare facility outside of the area can access a patient’s health information and avoid duplicative testing and unnecessary procedures.
– S
What a shared EHR means to a mother who needs to quickly access her child’s immunization records…
It means that the mother can access and print the information from the electronic health record whenever or wherever the information is needed.
– S

Keystone Beacon Community Security
• Provides critical patient information when and where
• it is needed• Only accessible by participating provider • Able to track who accesses patient information• Able to track when it is accessed• Backed up to redundant off-site servers via
“Cloud”
– S

Coordinated Care = Best Treatment Possible
Results of a recent study of the Greater Susquehanna Valley shows that coordinated care is capable of simultaneously improving quality and reducing costs, while enhancing physician and patient satisfaction.
American Journal of Managed Care, August 2010
– S

Care coordination results*
• 40% reduction in unnecessary hospital readmissions
• 20% reduction in unnecessary hospital admissions
• 7% reduction in cost of care
*Statistics reflect three year observational study of 15,000 Geisinger Health Plan Medicare Advantage members at 11 of Geisinger’s community practice sites.
– S

Thank You!
John M. KravitzGeisinger Health System
570.214.8833


















