Reducing Sepsis Mortality Richard Crowell, MD Chief Quality Officer UNM Health System Professor,...
61
Reducing Sepsis Reducing Sepsis Mortality Mortality Richard Crowell, MD Richard Crowell, MD Chief Quality Officer Chief Quality Officer UNM Health System UNM Health System Professor, Dept of Internal Professor, Dept of Internal Medicine Medicine
-
Upload
patrick-cobb -
Category
Documents
-
view
223 -
download
0
Transcript of Reducing Sepsis Mortality Richard Crowell, MD Chief Quality Officer UNM Health System Professor,...

Reducing Sepsis MortalityReducing Sepsis Mortality
Richard Crowell, MDRichard Crowell, MDChief Quality OfficerChief Quality OfficerUNM Health SystemUNM Health System
Professor, Dept of Internal MedicineProfessor, Dept of Internal Medicine

ObjectivesObjectives
• History of Early Goal-Directed Therapy History of Early Goal-Directed Therapy at UNM Hospital: SMITeat UNM Hospital: SMITe
• Recent Sepsis informationRecent Sepsis information
• The future is nowThe future is now

Sepsis: A Complex DiseaseSepsis: A Complex Disease
Adapted from: Bone RC et al. Adapted from: Bone RC et al. Chest.Chest. 1992;101:1644- 1992;101:1644-5555..Used with permission, S.Simpson, MD, KU, 2008Used with permission, S.Simpson, MD, KU, 2008
SevereSevereSepsisSepsis
Trauma
Infection
SepsisOther
Pancreatitis
Burns
SIRS

Sepsis: A Deadly ContinuumSepsis: A Deadly Continuum
• A clinical response arising from a nonspecific insult, with 2 of the following:• T >38oC or <36oC• HR >90 beats/min• RR >20/min• WBC >12,000/mm3 or <4,000/mm3
or >10% bands
SIRS with a presumed
or confirmed infectious process
Chest 1992;101:1644.Chest 1992;101:1644.
SepsisSepsisSIRSSIRSSevere Severe
SepsisSepsisShockShock
SepticSeptic
Sepsis with organ
dysfunction
RefractoryHypotension
Related toSepsis

Clinical Alterations in Severe SepsisClinical Alterations in Severe Sepsis
• VasculopathyVasculopathy• Loss of regional autoregulationLoss of regional autoregulation• VasodilationVasodilation• Relative intravascular hypovolemiaRelative intravascular hypovolemia
• CardiopathyCardiopathy• ↓ ↓ contractility, ↑ compliancecontractility, ↑ compliance• ↑ ↑ CO, but ↓ EFCO, but ↓ EF
• Acute organ dysfunctionAcute organ dysfunction• Toxin and cytokine actions on Toxin and cytokine actions on
vascular / tissue barriersvascular / tissue barriers

Inflammatory MediatorsCardiovascular Insufficiency
Global Tissue HypoxiaGlobal Tissue Hypoxia
Increased MetabolicDemands
Hypovolemia VasodilationMyocardial Depression
Microvascular AlterationsOO22 Delivery DeliveryOO22 Demand Demand
After Fink. Crit Care Clin 2002.After Fink. Crit Care Clin 2002.Used with permission, S.Simpson, MD, KU, 2008Used with permission, S.Simpson, MD, KU, 2008

Acute Organ Dysfunction as the Hallmark of Acute Organ Dysfunction as the Hallmark of Severe SepsisSevere Sepsis
TachycardiaTachycardiaHypotensionHypotension
OliguriaOliguriaAnuriaAnuria
CreatinineCreatinine
PlateletsPlatelets PT/APTTPT/APTT Protein CProtein C D-dimerD-dimer
Altered Altered ConsciousnessConsciousness
ConfusionConfusionPsychosisPsychosis
TachypneaTachypneaPaOPaO22 <70 mm Hg <70 mm Hg
SaOSaO22 <90% <90%
PaOPaO22/FiO/FiO22 300 300
JaundiceJaundice EnzymesEnzymes AlbuminAlbumin
PTPT
Lactic acidosisLactic acidosis
Used with permission, S.Simpson, MD, KU, 2008Used with permission, S.Simpson, MD, KU, 2008

Treatment of SepsisTreatment of Sepsis
• Address cause: Treat infectionAddress cause: Treat infection
• Intravascular volume resuscitationIntravascular volume resuscitation
• Cardiovascular supportCardiovascular support
• Support of dysfunctional organ systemsSupport of dysfunctional organ systems
But prior to the new millenium, little improvement in But prior to the new millenium, little improvement in sepsis mortality…sepsis mortality…

• Patients enrolled on entry into EDPatients enrolled on entry into ED
• Evidence of Infection Evidence of Infection
• Met SIRS criteria Met SIRS criteria
• Hypotensive OR Lactic acidosis (>4 mmol/L)Hypotensive OR Lactic acidosis (>4 mmol/L)• 6 hour protocol6 hour protocol
• Cultures and antibioticsCultures and antibiotics
• Fluid resuscitation 20 ml/kgFluid resuscitation 20 ml/kg
• CV support with vasopressors, augmented O2 CV support with vasopressors, augmented O2 deliverydelivery

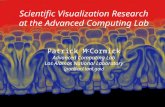
The Importance of Early Goal-DirectedThe Importance of Early Goal-DirectedTherapy for Sepsis Induced Hypoperfusion Therapy for Sepsis Induced Hypoperfusion
Adapted from Table 3, page 1374, from Rivers E, Nguyen B, Havstad S, et al. Early goal-directed Adapted from Table 3, page 1374, from Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. therapy in the treatment of severe sepsis and septic shock. N Engl J MedN Engl J Med 2001; 345:1368-1377 2001; 345:1368-1377
In-hospital In-hospital mortality mortality
(all (all patients)patients)
00
1010
2020
3030
4040
5050
6060 Standard therapyStandard therapy
EGDTEGDT
28-day 28-day mortalitymortality
60-day 60-day mortality mortality
NNT to prevent 1 event (death) = 6-8NNT to prevent 1 event (death) = 6-8
Mort
ality
(%
)M
ort
ality
(%
)

Early Goal-Direct Therapy (EGDT)Early Goal-Direct Therapy (EGDT)
EGDT is designed to: EGDT is designed to:
Recognize patients with severe sepsis as early as Recognize patients with severe sepsis as early as possible and begin treatment quicklypossible and begin treatment quickly
Assess laboratory and clinical variables for acute Assess laboratory and clinical variables for acute organ dysfunction, hemodynamic instabilityorgan dysfunction, hemodynamic instability
Delineate time targets for delivery of treatment of Delineate time targets for delivery of treatment of patients with sepsispatients with sepsis
Develop hospital-specific bundled protocolsDevelop hospital-specific bundled protocols
Earlier treatment leads to better outcomesEarlier treatment leads to better outcomes

Good Evidence-based Data for EGDTGood Evidence-based Data for EGDT
• Mortality improvement Mortality improvement
• Use of lactate as severity and prognostic indicatorUse of lactate as severity and prognostic indicator
• Bundled protocols improve outcomesBundled protocols improve outcomes• But not all individual bundle elements have been But not all individual bundle elements have been
shown to specifically improve mortalityshown to specifically improve mortality
• Early and appropriate antibioticsEarly and appropriate antibiotics
• Aggressive fluid resuscitation improve outcomesAggressive fluid resuscitation improve outcomes
• But how much fluid?But how much fluid?
• Enough to improve end organ dysfunctionEnough to improve end organ dysfunction
• But not too much…But not too much…

© 2012 by the Society of Critical Care Medicine and Lippincott Williams & Wilkins. Published by Lippincott Williams & Wilkins, Inc.
11
Figure 5Hospitalizations, costs, and outcomes of severe sepsis in the United States 2003 to 2007. Lagu, Tara, et.al. Critical Care Medicine. 40(3):754-761, 2012.DOI: 10.1097/CCM.0b013e318232db65
Figure 5 . Discharge disposition among patients with severe sepsis, 2003 to 2007.

Date of download: 7/16/2014Copyright © 2014 American Medical
Association. All rights reserved.
From: Mortality Related to Severe Sepsis and Septic Shock Among Critically Ill Patients in Australia and New Zealand, 2000-2012
JAMA. 2014;311(13):1308-1316. doi:10.1001/jama.2014.2637 Mean Annual Mortality in Patients With Severe SepsisError bars indicate 95% CI.

Good Evidence-based Data for EGDTGood Evidence-based Data for EGDT
• Mortality improvement Mortality improvement
• Use of lactate as severity and prognostic indicatorUse of lactate as severity and prognostic indicator
• Bundled protocols improve outcomesBundled protocols improve outcomes• But not all individual bundle elements have been But not all individual bundle elements have been
shown to specifically improve mortalityshown to specifically improve mortality
• Early and appropriate antibioticsEarly and appropriate antibiotics
• Aggressive fluid resuscitation improve outcomesAggressive fluid resuscitation improve outcomes
• But how much fluid?But how much fluid?
• Enough to improve end organ dysfunctionEnough to improve end organ dysfunction
• But not too much…But not too much…

Best current, generally available measure of Best current, generally available measure of Global Tissue Hypoxia is Global Tissue Hypoxia is LactateLactate
• What is role of lactate ?What is role of lactate ?
• Patient assessmentPatient assessment
• Assigning prognosisAssigning prognosis
• Guiding treatment decisionsGuiding treatment decisions

Serum Lactate as a predictor of mortality in Serum Lactate as a predictor of mortality in patients with infectionpatients with infection
Trzeciak S, et.al. Intensive Care Medicine 33:970-77, 2007
•Retrospective analysis of patients with dx of infection and lactate measured•Did not evaluate +/- shock

© 2009 Lippincott Williams & Wilkins, Inc. Published by Lippincott Williams & Wilkins, Inc. 4
Lactate is associated with mortality in Severe Sepsis Independent of organ failure and shock
Prospective cohort study
Critical Care Medicine. 37(5):1670-1677, May 2009.

© 2009 Lippincott Williams & Wilkins, Inc. Published by Lippincott Williams & Wilkins, Inc. 7
Figure 3.
Critical Care Medicine. 37(5):1670-1677, May 2009.
Lactate is associated with mortality in Severe Lactate is associated with mortality in Severe Sepsis Independent of organ failure and shockSepsis Independent of organ failure and shock

© 2009 Lippincott Williams & Wilkins, Inc. Published by Lippincott Williams & Wilkins, Inc. 6
Lactate is associated with mortality in Severe Sepsis Independent of organ failure and shock 2.
Critical Care Medicine. 37(5):1670-1677, May 2009.

Outcomes of patients undergoing early sepsis resuscitation for cyptic shock compared with overt shock. Puskarich MA, etal. Resuscitation 82:1289, 2011

Outcomes of patients undergoing early sepsis resuscitation for cyptic shock compared with overt shock. Puskarich MA, etal. Resuscitation 82:1289, 2011

Good Evidence-based Data for EGDTGood Evidence-based Data for EGDT
• Mortality improvement Mortality improvement
• Use of lactate as severity and prognostic indicatorUse of lactate as severity and prognostic indicator
• Bundled protocols improve outcomesBundled protocols improve outcomes• Even though not all individual bundle elements have Even though not all individual bundle elements have
been shown to specifically improve mortalitybeen shown to specifically improve mortality
• Early and appropriate antibioticsEarly and appropriate antibiotics
• Aggressive fluid resuscitation improve outcomesAggressive fluid resuscitation improve outcomes
• But how much fluid?But how much fluid?
• Enough to improve end organ dysfunctionEnough to improve end organ dysfunction
• But not too much…But not too much…

Good Evidence-based Data for EGDTGood Evidence-based Data for EGDT
• Mortality improvement Mortality improvement
• Use of lactate as severity and prognostic indicatorUse of lactate as severity and prognostic indicator
• Bundled protocols improve outcomesBundled protocols improve outcomes• Even though all individual bundle elements have not Even though all individual bundle elements have not
been shown to specifically improve mortalitybeen shown to specifically improve mortality
• Early and appropriate antibioticsEarly and appropriate antibiotics
• Aggressive fluid resuscitation improve outcomesAggressive fluid resuscitation improve outcomes
• But how much fluid?But how much fluid?
• Enough to improve end organ dysfunctionEnough to improve end organ dysfunction
• But not too much…But not too much…

EGDT: Bundled approaches to protocolsEGDT: Bundled approaches to protocols
• Use is evidence-based:Use is evidence-based:
• Combine multiple elementsCombine multiple elements
• Outcome is additive or synergisticOutcome is additive or synergistic
• Framework that leverages changeFramework that leverages change
• Avoids a piecemeal approachAvoids a piecemeal approach

Do Bundles Work?Do Bundles Work?
Gao, et al. Gao, et al. Critical CareCritical Care 2005, 2005, 9:9:R764-R770.R764-R770.With Permission from S. Simpson, MD,, Kansas University, 2008With Permission from S. Simpson, MD,, Kansas University, 2008

Multicenter implementation of a severe sepsisand septic shock treatment bundle. Miller RR, et.al. Am Journal Respir Crit Care Med, 2013; 188, 77-82
A. All subjects with Severe Sepsis/Septic Shock
B. Only subjects with Septic Shock

Good Evidence-based Data for EGDTGood Evidence-based Data for EGDT
• Mortality improvement Mortality improvement
• Use of lactate as severity and prognostic indicatorUse of lactate as severity and prognostic indicator
• Bundled protocols improve outcomesBundled protocols improve outcomes• But not all individual bundle elements have been But not all individual bundle elements have been
shown to specifically improve mortalityshown to specifically improve mortality
• Early and appropriate antibioticsEarly and appropriate antibiotics
• Aggressive fluid resuscitation improve outcomesAggressive fluid resuscitation improve outcomes
• But how much fluid?But how much fluid?
• Enough to improve end organ dysfunctionEnough to improve end organ dysfunction
• But not too much…But not too much…

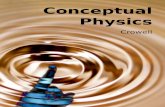
Timeliness of Antibiotics in Septic Shock
• Kumar, et.al. reviewed medical records of 2731 adults Kumar, et.al. reviewed medical records of 2731 adults with septic shock over 25 years in Manitoba, Canadawith septic shock over 25 years in Manitoba, Canada
• Focused on 2,154 patients who received Ab ONLY Focused on 2,154 patients who received Ab ONLY after onset of hypotensionafter onset of hypotension
• Clinical site infectionsClinical site infections
• 37.2% lung37.2% lung
• 29.3% intraabdominal29.3% intraabdominal
• 10.7% genitourinary10.7% genitourinary
• Documented infection (by cx) in 78% of casesDocumented infection (by cx) in 78% of cases
• Others by definitive xray, surgical, biopsy, or Others by definitive xray, surgical, biopsy, or autopsy evidenceautopsy evidence
• Microbiology: Gram (-) 47.9%, Gram (+) 38.3%Microbiology: Gram (-) 47.9%, Gram (+) 38.3%
Kumar A, et.al. Crit Care Med 34:1589, 2006

Septic Shock: Timing of AntibioticsSeptic Shock: Timing of AntibioticsKumar et al, CCM. 2006:34:1589-96
0.00.0
.20.20
.40.40
.60.60
.80.80
1.001.00
% Survival
% Total receiving antibiotics
0 - .5
.5 – 1.01 - 2 2 - 3 3-4 4 - 5 5 - 6 6 - 9 9 - 1
212 - 2
424 - 3
6> 36
Percent of Percent of total ptstotal pts
Time (hrs) from hypotension onset
14 ICUs; n = 2,731
Only 50% of patients in Septic Shock
received antibiotics w/in 6 hrs.

Timeliness of Antibiotics in Septic Shock
• Antibiotics w/in first hour: 79.9% survivalAntibiotics w/in first hour: 79.9% survival
• Every hour delay decreased survival by 7.6%Every hour delay decreased survival by 7.6%
• OR of in-hospital mortality increased by 12% for OR of in-hospital mortality increased by 12% for each hour delay in administrationeach hour delay in administration
• In Multivariate analysis:In Multivariate analysis:
• Time to antimicrobial therapy most strongly Time to antimicrobial therapy most strongly associated with survivalassociated with survival
• Others: APACHE score, volume of fluid in first Others: APACHE score, volume of fluid in first hour of resuscitationhour of resuscitation
•Kumar A, et.al. Crit Care Med 34:1589, 2006Kumar A, et.al. Crit Care Med 34:1589, 2006

Mor
tali
ty (
%)

Good Evidence-based Data for EGDTGood Evidence-based Data for EGDT
• Mortality improvement Mortality improvement
• Use of lactate as severity and prognostic indicatorUse of lactate as severity and prognostic indicator
• Bundled protocols improve outcomesBundled protocols improve outcomes• But not all individual bundle elements have been But not all individual bundle elements have been
shown to specifically improve mortalityshown to specifically improve mortality
• Early and appropriate antibioticsEarly and appropriate antibiotics
• Aggressive fluid resuscitation improves outcomesAggressive fluid resuscitation improves outcomes
• But how much fluid?But how much fluid?
• Enough to improve end organ dysfunctionEnough to improve end organ dysfunction
• But not too much…But not too much…

Cardiovascular Resuscitation-Based EGDTLin, et.al. 2006
• 241 consecutive patients enrolled, randomized to protocol vs no protocol
• Protocol focused on rapid fluids to:
• 1) attain CVP ≥ 8-12
then
2) MAP ≥ 65 (pressors, steroids as needed)
then
• 2) urine output ≥ 0.5 ml/kg/hr
• All patients got antibiotics per clinician; no differences in groups
Lin SM, et.al. Shock 6:551-7, 2006Lin SM, et.al. Shock 6:551-7, 2006

Cardiovascular Resuscitation-Based EGDT
Outcome Protocol (n=108)
No Protocol (n=116)
p
Hosp Mortality 53.7 % 71.6% 0.006
Shock reversal (hrs) 47 ± 22.8 65.4 ± 32.1 0.006
Resuscitation fluids 136.2 ± 119 88.6 ± 57.7 0.034
Time to pressors 78 22.2 104.4 29 0.001
Length of ICU stay 14.3 ± 11.7 20.3 ± 16.6 0.003
Renal failure 42 (38.9%) 64 (55.2%) 0.015
CNS failure 20 (18.5%) 42 (36.2%) 0.003
Lin SM, et.al. Shock 6:551-7, 2006Lin SM, et.al. Shock 6:551-7, 2006

Good Evidence-based Data for EGDTGood Evidence-based Data for EGDT
• Mortality improvement Mortality improvement
• Use of lactate as severity and prognostic indicatorUse of lactate as severity and prognostic indicator
• Bundled protocols improve outcomesBundled protocols improve outcomes• But not all individual bundle elements have been But not all individual bundle elements have been
shown to specifically improve mortalityshown to specifically improve mortality
• Early and appropriate antibioticsEarly and appropriate antibiotics
• Aggressive fluid resuscitation improve outcomesAggressive fluid resuscitation improve outcomes
• But how much fluid?But how much fluid?
• Enough to improve end organ dysfunctionEnough to improve end organ dysfunction
• But not too much…But not too much…

Successful fluid resuscitation in EGDTSuccessful fluid resuscitation in EGDT
• What are appropriate endpoints for “successful” What are appropriate endpoints for “successful” volume resuscitation?volume resuscitation?
• Depends on “volume responsiveness”Depends on “volume responsiveness”• where is the patient on the Starling curve?where is the patient on the Starling curve?
• CVP: may not be best measure for volume CVP: may not be best measure for volume responsivenessresponsiveness
• Pulse pressure variation, IVC diameter Pulse pressure variation, IVC diameter before/after fluid challengesbefore/after fluid challenges

Study Overview
• In septic shock, the first few hours of care are critical for survival.In septic shock, the first few hours of care are critical for survival.
• In this study, two protocols for the care of patients with septic shock In this study, two protocols for the care of patients with septic shock were compared with usual care with respect to 60-day mortality and were compared with usual care with respect to 60-day mortality and other outcomes.other outcomes.
• There were no significant differences in outcome.There were no significant differences in outcome.

Screening, Randomization, and Follow-up
The ProCESS Investigators. N Engl J Med 2014;370:1683-1693

Cumulative Mortality.
The ProCESS Investigators. N Engl J Med 2014;370:1683-1693

Notes from ProCess StudyNotes from ProCess Study• All patients received mean 2.2L volume resuscitation prior All patients received mean 2.2L volume resuscitation prior
to randomization (180 min)to randomization (180 min)
• Mean of 29 ml/kgMean of 29 ml/kg
• 75% in each group received antibiotics prior to 75% in each group received antibiotics prior to randomizationrandomization
• Unknown distribution of Ab within 1 vs. 2 vs. 3 hrs in Unknown distribution of Ab within 1 vs. 2 vs. 3 hrs in each groupeach group
• All patients in non-EGDT groups cared for by Critical All patients in non-EGDT groups cared for by Critical Care or ED-trained facultyCare or ED-trained faculty
• All institutions had long history of participation in SCC All institutions had long history of participation in SCC EGDT guidelinesEGDT guidelines
• Question of illness severity compared to other studiesQuestion of illness severity compared to other studies
• Did NOT evaluate value of ScVO2 as treatment guidelineDid NOT evaluate value of ScVO2 as treatment guideline

UNM ED -> MICUUNM ED -> MICU
• Plans to evaluate alternative approaches to Plans to evaluate alternative approaches to evaluation of adequacy of fluid resuscitationevaluation of adequacy of fluid resuscitation
• Passive Leg Raise, Pulse Pressure Variation Passive Leg Raise, Pulse Pressure Variation with FloTrackwith FloTrack
• IVC diameter responsiveness to fluidsIVC diameter responsiveness to fluids
• Minimal volume resuscitation of 2-3L within 3 Minimal volume resuscitation of 2-3L within 3 hourshours

Lee S, et.al. Increased fluid administration in the first 3 hours of sepsis resuscitation is associated with reduced mortality: a retrospective cohort study. Chest Online, 2014

Surviving Sepsis Campaign:Surviving Sepsis Campaign:Early Recognition is Crucial!!!Early Recognition is Crucial!!!
• Use of screening tools improves overall Use of screening tools improves overall awareness, educates, and increases awareness, educates, and increases recognitionrecognition
• UNM: UNM: • Wards/MICU: qshift screening by Wards/MICU: qshift screening by
nursing staffnursing staff• ED: Triage nurses, EMS do initial ED: Triage nurses, EMS do initial
evaluationevaluation

Surviving Sepsis Campaign:Surviving Sepsis Campaign:Early Recognition is Crucial!!!Early Recognition is Crucial!!!
• UNM ScreeningUNM Screening
• Temp >38.3C, <36CTemp >38.3C, <36C
• RR >20RR >20
• HR >90HR >90
• WBC >10, <4*WBC >10, <4*
• *ED triage: Mental Status Changes*ED triage: Mental Status Changes

Identification of sepsis severity !!
3 pathways
Green (sepsis)
Yellow (lactate 2-4)
Red (severe sepsis or septic shock)
• Protocol was based on literature and input from all areas involved
• Several revisions before consensus

SEPSIS
RRT
SEPSIS/Critical Care Team
Septic Shock(hypotension)
Occult Septic Shock(lactate > 4,
No hypotension)
Bedside LactateMeasured
SEPSIS(Lactate < 4
No organ dysfunctionNo hypotension)
Severe SEPSIS(organ dysfunction*
lactate < 4No hypotension)
Basic SMITE Bundle1. Lactate q 4 X 2⁰2. Blood culture3. Antibiotics within 1 hr4. Fluids
Re-evaluate as needed
Advanced SMITE BundleBasic Bundle Plus:4. Fluids bolus5. CVP6. Vasopressors
NOTIFY MD Ward Team/Covering Provider
“Intermediate Risk”
Bedside Lactate “High Risk” Bedside
Lactate
*Organ Dysfunction•AMS (Glasgow < 12)•Creat > 1.5•Total Bili > 2.0 •INR > 1.5•Platelets < 100K
• Confirm Sepsis Dx• Determine Sepsis Severity
If NOT Sepsis: Document alternative Dx
OrderSerumLactate
Contact RRT
YES
SIRS CriteriaAssess for 2 or more1.Temp > 38 C or ⁰ < 36 C⁰2.HR > 903.Resp rate > 20 or pa CO₂ < 324.WBC > 12K, < 4K, or > 10% bands
YES NO Evaluate as clinically indicated
Suspected site of
Infection
ICU Admission
NO
Re-asses Q shift

Table 2Table 2
TABLE 2. Severe SepsisTABLE 2. Severe Sepsis
Copyright © 2013 Critical Care Medicine. Published by Lippincott Williams & Wilkins. 48
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012
Dellinger, R. Phillip; Levy, Mitchell M.; Rhodes, Andrew; Annane, Djillali; Gerlach, Herwig; Opal, Steven M.; Sevransky, Jonathan E.; Sprung, Charles L.; Douglas, Ivor S.; Jaeschke, Dellinger, R. Phillip; Levy, Mitchell M.; Rhodes, Andrew; Annane, Djillali; Gerlach, Herwig; Opal, Steven M.; Sevransky, Jonathan E.; Sprung, Charles L.; Douglas, Ivor S.; Jaeschke, Roman; Osborn, Tiffany M.; Nunnally, Mark E.; Townsend, Sean R.; Reinhart, Konrad; Kleinpell, Ruth M.; Angus, Derek C.; Deutschman, Clifford S.; Machado, Flavia R.; Rubenfeld, Roman; Osborn, Tiffany M.; Nunnally, Mark E.; Townsend, Sean R.; Reinhart, Konrad; Kleinpell, Ruth M.; Angus, Derek C.; Deutschman, Clifford S.; Machado, Flavia R.; Rubenfeld, Gordon D.; Webb, Steven A.; Beale, Richard J.; Vincent, Jean-Louis; Moreno, Rui; and the Surviving Sepsis Campaign Guidelines Committee including the Pediatric SubgroupGordon D.; Webb, Steven A.; Beale, Richard J.; Vincent, Jean-Louis; Moreno, Rui; and the Surviving Sepsis Campaign Guidelines Committee including the Pediatric Subgroup
Critical Care Medicine. 41(2):580-637, February 2013.Critical Care Medicine. 41(2):580-637, February 2013.
doi: 10.1097/CCM.0b013e31827e83afdoi: 10.1097/CCM.0b013e31827e83af
•

IHI Severe Sepsis Collaborative IHI Severe Sepsis Collaborative Expanded SMITe to EDExpanded SMITe to ED
• Fall 2009 Fall 2009 Joined IHI collaborative Joined IHI collaborative• Aims:Aims:
• Improve ED recognition of Improve ED recognition of severe sepsissevere sepsis• Facilitate transfers to the Facilitate transfers to the MICUMICU• Improve communication between both unitsImprove communication between both units
• ED-specific screening tool for triageED-specific screening tool for triage• Concurrent patient trackingConcurrent patient tracking• Still have twice-monthly group meetingStill have twice-monthly group meeting• Patient criteriaPatient criteria
• Septic shockSeptic shock• Lactate >/= 4Lactate >/= 4

UNMH Mortality: Severe SepsisUNMH Mortality: Severe Sepsis2010 – May, 20142010 – May, 2014

Figure 1. Surviving Sepsis Campaign Care Figure 1. Surviving Sepsis Campaign Care Bundles.Bundles.
Copyright © 2013 Critical Care Medicine. Published by Lippincott Williams & Wilkins. 51
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012Dellinger, R. Phillip; Levy, Mitchell M.; Rhodes, Andrew; Annane, Djillali; Gerlach, Herwig; Opal, Steven M.; Sevransky, Jonathan E.; Sprung, Charles L.; Douglas, Ivor S.; Jaeschke, Roman; Osborn, Tiffany M.; Nunnally, Mark E.; Townsend, Sean R.; Reinhart, Konrad; Kleinpell, Ruth M.; Angus, Dellinger, R. Phillip; Levy, Mitchell M.; Rhodes, Andrew; Annane, Djillali; Gerlach, Herwig; Opal, Steven M.; Sevransky, Jonathan E.; Sprung, Charles L.; Douglas, Ivor S.; Jaeschke, Roman; Osborn, Tiffany M.; Nunnally, Mark E.; Townsend, Sean R.; Reinhart, Konrad; Kleinpell, Ruth M.; Angus, Derek C.; Deutschman, Clifford S.; Machado, Flavia R.; Rubenfeld, Gordon D.; Webb, Steven A.; Beale, Richard J.; Vincent, Jean-Louis; Moreno, Rui; and the Surviving Sepsis Campaign Guidelines Committee including the Pediatric SubgroupDerek C.; Deutschman, Clifford S.; Machado, Flavia R.; Rubenfeld, Gordon D.; Webb, Steven A.; Beale, Richard J.; Vincent, Jean-Louis; Moreno, Rui; and the Surviving Sepsis Campaign Guidelines Committee including the Pediatric SubgroupCritical Care Medicine. 41(2):580-637, February 2013.Critical Care Medicine. 41(2):580-637, February 2013.doi: 10.1097/CCM.0b013e31827e83afdoi: 10.1097/CCM.0b013e31827e83af
•

Is optimization of oxygen delivery/utilization Is optimization of oxygen delivery/utilization necessary for successful EGDT?necessary for successful EGDT?
• Is ScVOIs ScVO22 the appropriate surrogate measure for the appropriate surrogate measure for
optimizing oxygen delivery/utilization in septic optimizing oxygen delivery/utilization in septic shock? shock?
• Role of transfusion, inotropic supportRole of transfusion, inotropic support
• Can lactate clearance be used as a measure of Can lactate clearance be used as a measure of successful EGDT ?successful EGDT ?

Summary of recent data on EGDTSummary of recent data on EGDT
• EGDT bundle completion improves mortalityEGDT bundle completion improves mortality
• Antibiotics within 1 hour saves livesAntibiotics within 1 hour saves lives
• Hospital-derived Sepsis much higher mortality Hospital-derived Sepsis much higher mortality than if present on admissionthan if present on admission
• UH Sepsis mortality NOT POA 2x that if UH Sepsis mortality NOT POA 2x that if Present On Admission (PAO)Present On Admission (PAO)

Non-POA Severe SepsisNon-POA Severe SepsisUNMH: 2/2013 – 3/2014UNMH: 2/2013 – 3/2014
Total Obs Mortality
Medical Mortality Index
Surgical MortalityIndex
Sepsis 8.0 % 12.0 % 1.93 4.0% 0.42
Severe Sepsis
39.25% 50% 2.8 31.5% 2.19

Non-POA Severe Sepsis TeamNon-POA Severe Sepsis Team
• Member of national SCCM CollaborativeMember of national SCCM Collaborative• Focus is on:Focus is on:
• Early and accurate identificationEarly and accurate identification
• Physician responsiveness, assessment, Physician responsiveness, assessment, documentation of decisionsdocumentation of decisions
• Identification and transfer to higher level of Identification and transfer to higher level of care as neededcare as needed
• Adequate fluid resuscitationAdequate fluid resuscitation
• Antibiotics within 1 hourAntibiotics within 1 hour

Brought to you by Brought to you by SMITeSMITe
SSepsisepsis
MMortalityortality
IImprovement mprovement
TeTeamam
at UNMat UNM

Documentation of Disease Severity: Documentation of Disease Severity: Severe Sepsis/Septic ShockSevere Sepsis/Septic Shock
• Severe sepsis w/o MV 96+ hours Severe sepsis w/o MV 96+ hours
with MCCwith MCC• DRG 871 DRG 871 RW: 1.9090RW: 1.9090
Est. Payment: $17,654Est. Payment: $17,654
• Severe sepsis w/o MV 96+ hoursSevere sepsis w/o MV 96+ hours
without MCCwithout MCC• DRG 872 DRG 872 RW 1.1339 RW 1.1339
Est. Payment: $10,486Est. Payment: $10,48657

Severity of Illness and Risk of MortalitySeverity of Illness and Risk of Mortality
Comorbidity and/or Complication (CC)Comorbidity and/or Complication (CC)•Comorbitidy: Comorbitidy: A pre-existing condition/illness A pre-existing condition/illness that will cause an increase in length of stay because that will cause an increase in length of stay because of its presence with the condition that caused the of its presence with the condition that caused the admission.admission.
•ComplicationComplication: A condition that arises during the : A condition that arises during the hospital stay that may prolong the length of stay. hospital stay that may prolong the length of stay.
•Major comordibity/complication (MCC)Major comordibity/complication (MCC)
58

MCCs for Sepsis MCCs for Sepsis
Example of MCCs for SepsisExample of MCCs for Sepsis
•Respiratory Failure due to SepsisRespiratory Failure due to Sepsis• Acute Respiratory FailureAcute Respiratory Failure
• Lung AbcessLung Abcess
• EmpyemaEmpyema
• Ventilator Dependent (can’t use unable to wean)Ventilator Dependent (can’t use unable to wean)
59

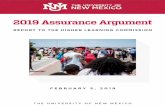
Figure 1. Mean hospital mortality (solid line) and 95% confidence interval (dotted lines) based on the magnitude of lactate change within 12 hours compared with index values. Patients with decreased lactate (across percentage strata) are represented toward the right of the figure, whereas those with increased lactate are toward the left. The vertical line demarcates increased and decreased repeat lactate values.
Annals ATS, 2013http://www.atsjournals.org/doi/abs/10.1513/AnnalsATS.201304-099OC
Published in: Vincent Liu; John W. Morehouse; Jay Soule; Alan Whippy; Gabriel J. Escobar; Annals ATS 10, 466-473.DOI: 10.1513/AnnalsATS.201304-099OCCopyright © 2013 by the American Thoracic Society
One PowerPoint slide of each figure may be downloaded and used for educational not promotional purposes by an author for slide presentations only. The ATS citation line must appear in at least 10-point type on all figures in all presentations. Pharmaceutical and Medical Education companies must request permission to download and use slides, and authors and/or publishing companies using the slides for new article creations for books or journals must apply for permission. For permission requests, please contact the Publisher at [email protected] or 212-315-6441.