
Reducing Readmission Following Ambulatory Surgery -- Ripe ...

Reducing Readmission Case StoriesDiscussion of SuccessesUniversity of California, San FranciscoMaureen Carroll RN, CHFNTransitional Care ManagerHeart Failure Program Coordinator
UnityPoint Cedar Rapids Iowa Peg Bradke RN, MA
Vice President, Post Acute Care
UnityPoint Health St. Luke’s

University of California, San Francisco
Mission: The reason that we exist is Caring, Healing, Teaching, and Discovery
Top 10 Hospitals (US World and News past 13 yrs)
722 licensed beds; 28,000 admissions,
New UCSF Mission Bay Hospitals
– Benioff Children’s Hospital
– Betty Irene Moore Woman’s Hospital
– Bakar Cancer Hospital
– Ron Conway Family Gateway Medical Building
2

The Cross Continuum Team
Multidisciplinary cross continuum team – it takes a village;
Family caregivers, nurses, physicians, senior leadership, case managers, social workers, dieticians, pharmacists, nurse practitioners, home care team, palliative care, Care Support team, chaplains, managers, community partners, SNF liaisons, outpatient clinic liaisons, community clinics liaisons, and more
3

The Cross Continuum Team
Excellence in Transitions of Care – ETOC
Workgroups – Hospital wide readmission projects
Data review and management
Highlights on progress on projects/programs
Inpatient and outpatient programs
Senior leadership participation
Office of Population Health
4

Cross Continuum Teams
UCSF Care Support
UCSF Bridges
UCSF Housecalls
UCSF Center for
Geriatrics Care
UCSF-Hastings
Medical Legal
Partnership for
Seniors

St. Luke’s Hospital - UnityPoint Health
System
Private hospital – Cedar Rapids, Iowa
Affiliate in the UnityPoint Health System
Licensed for 500 Beds with more than 17,000 admissions
Truven Top 100 Hospital – 5 years; Heart Hospital - 3 years
Iowa Recognition for Performance Excellence Gold Award - 2010
Joint Commission Disease-Specific Recertifications in Stroke (2006-14), Heart Failure (2008-14), Total Joint (2008-14) and Palliative Care (2010-14).
Society of Chest Pain Center – Chest Pain Certification (2010, 2013)
Magnet Re-designation – 2014
Mayo Clinic Care Network – 2014

CCT – Transition to Home
Our mission: “To give the healthcare we’d like our loved ones to receive”
Meets monthly
Reviews readmissions for each month related to core diagnosis to assess causes and opportunities for improvement
Reviews process and outcome measures
Continually testing and improving, aggregating the experiences of patients, families and caregivers
Each site/level of care reports on testing occurring in their area

Transition to Home Team Members
Inpatient Nursing Units
– Manager
– Care Managers
Palliative Care
Home Care
Respiratory Care
Emergency Dept.
Case Management
CardioPulm. Rehab.
Pharmacy
Nurse Practitioners
UnityPoint Clinics Reps
Critical Access Hospital
Community SNF’s
Hospitalist Rounding Nurses
Outpatient Social Services
Inpatient Social Services
Performance Improvement

Several Subgroups Report into the
Larger Transition to Home Team
Data Management
Patient Education Processes
Home Care
SNF/Nursing Facilities Work Processes
Physician Clinic Processes
Case Management/Social Work/Care Coordination
Several members of the Transition to Home team are members of the hospital ACO and Population Health Management work. Information is bidirectional between these teams.

Program Overview
10

Overview of the Process
Standardized evidence-based care through order sets.
Patient Education/Teaching:
– Utilizing Universal Health Literacy Concepts
– Enhanced teaching materials
– Teach back
Utilization of whiteboard to individualize patient’s plan of care and communicate to team.
Bedside Report
Transition to Home Huddles

Continuum of Care (Cont’d)
Touch points post discharge:Home Care - care coordination visit 24 to 48 hours post discharge on high-risk patientsPhysician Clinic follow-up appointment made prior to discharge for 3-7 days afterWork closely with PCP offices on Transitional Code (TCM) and Patient Centered Medical Home Standardized tool for transfer of information to nursing facilities for next level of care.Telehealth monitor available through Home CareEmergency Department Consistent Care Program Advanced Medical Team Outpatient Social WorkerPalliative Care Program

The Foundation
Monthly Heart Failure Grant Meetings with Multidisciplinary Team
Comprehensive Patient Education
Care coordination
Implemented IHI Evidence Based Interventions
Development of Data Collection System
Patient Advisory Group, Heart Healthy classes on unit
Palliative Care Collaboration
Staff trained on Teach Back & HF Education
Patient stories shared to drive change
Focus on Continuum of Care - Communication and Collaboration

Patient Interventions
Patient Identification- Daily Chart Reviews
Extensive Patient and Family education
Referrals: Inpatient and Outpatient
Follow-up Appointments– Within 7 days for primary HF, COPD, PNA,AMI
– Heart Failure Clinic NPs visits for high risk patients
– Outpatient programs for high risk patients
Follow-up calls – Increased with automation to 5/month
Medication Reconciliation- Pharmacist consult
Discharge Summaries- within 48 hours
Hand off Communication to Outpatient providers
Care at Home Programs – High Risk patients

Outpatient Focus
Collaboration with Outpatient Providers
– Skilled Nursing Facilities, Home Care Agencies, Primary Care Physicians, and Cardiologists
“Virtual Team” Email to connect providers (in/outpatient)
Geriatric Transitions, Consultation, and Comprehensive Care (GeriTraCCC) started UC–Care Support at Home
MD House Calls for High Risk HF Patients (Aug 2010)
Advanced Heart Failure Clinic; High Risk pts- NP follow up
In-services for staff, home care, skilled nursing staff
Hospital wide projects to standardize and improve discharge process and readmission projects

Assessment
16

UCSF MDR Improvements
Quieter space
New team monthly- welcome and orientation
Clear expectations for all members
Readmission discussions
What can we do differently?
Address level of support needed
Risk discussed
17

Readmission Interviews
Gain perspective of patient and family caregivers
Reach out to inpatient and outpatient providers
Notification of # of admissions in past year, 30 and 90 day readmits, and possible factors
Low health literacy
Lack of support
Medication challenges
Transportation challenges
Assessments: Cognitive, depression, functional, motivation
18

The Patient Story …
to share and learn from
19

Enhanced Assessment
During Admission Assessment, the patient and family are asked, “Who would you like to have present when we provide your discharge information?”
Medication reconciliation: Dedicated Admission Center RN’s complete home medication list and prepare an appropriate list for physician to address.
Readmission Interviews

Whiteboard

Multidisplinary Rounds
Bedside shift report
– To involve patient and family caregivers as partners in care
Daily discharge huddles
– Identification of patient/family needs/concerns
– Daily goals are reviewed
– Available support for patient: need for Palliative Care Referral
– Educational needs
– Identification of home care needs/other levels of care
– Nurse sensitive indicators: fall risk, skin issues

Patient Education/Teach Back
23

Enhanced Teaching and Learning
Same materials are used across the continuum: in the hospital, with home care, long-term care settings and the clinics.
Short, succinct patient/family education packet
Teach Back questions part of packet
Patient teaching flowsheets “close the loop” to help staff nurses address Teach Back and assure the documentation and use of Teach back.


Example: MI 2nd page with TB questions

27

Example from EPIC
Patient Teaching Flowsheet

Teach Back Utilized with Discharge
Instructions
Can you show me on these instructions:
– How you find your doctors’ office appointment?
– What other tests you have scheduled and when?
Is there anything on these instructions that could be difficult for you to do?
Have we missed anything?
Who will you call if you have questions?

Discharge SmartPhrase


Patient Education
Teach Back Technique- WORKS
Health Literacy principles
Multiple languages- use of interpreters
Input from patients and family caregivers
Same materials and technique across the Continuum of Care
Educate patient regarding diagnosis, self –care management, and importance of follow up
Lesson Learned: Listen before we teach. Ask open-ended questions
Goal for Patient: Take action when you notice a change in your health

Real-Time Handover
33

Real-Time Handover Communications
“Warm Hand-overs” to Skilled Nursing Facilities, Home care agencies, outpatient clinics, and providers
Email-notifications to inpatient team, case manager, consultants, HF clinic, home care RNs, SNF and PCP on admission
Creates a “Virtual Care Team”
Time consuming but valuable
Unites the entire team working on transition of care
Importance of Home Care referrals
– Medication reconciliation
– Focus on self management skills

Email to Team on Admission:Dear Medical Team,We wanted to let you know that we are following Mr. XXXXXXXXXXX in the Heart Failure / Transitional Care Program . We are very familiar with this high risk patient from previous admissions (5th in past 4 months). We have provided education, initiated palliative care consults, and coordinated services in the past . We would like to provide as much support as possible for the patient and family.
Recommendations:1.Bridges Program- MD home visits 2.UC RN home care 3.Pharmacist consult for discharge medications4.Follow up appointment within 7 days5.Goals of care discussion/Palliative care consult
The goal of this program is to provide our Medicare patients and families with as much information and support as possible to enable them to safely manage their care during this vulnerable post hospitalization period, and to prevent avoidable 30 day readmissions. We will be following patients with primary heart failure, COPD, PNA, and AMI. We will be sharing information through tracking of the readmissions to identify trends and to learn from. The focus of the program is as follows;
In-house consults when indicated – dietary, pharmacist, palliative careGoals of care conversations initiated ( by the team or PCS) for all patients admitted 3 times within a yearRN/PT home care visits whenever deemed appropriateFollow up appointments scheduled within 7 days for primary heart failure patients and 14 days for all others at time of dischargeFollow up calls through the UCSF discharge phone call program and by the transitional care program for patients identified as high risk for readmissions
Please let us know if there is anything that we might do to assist and thank you for the great care that you provide our patients!

Real-Time Handover Communications
Interagency standardized transfer form
Warm handover Communication
Work with Clinic and the TCM code
ARNP’s assigned to Post Acute Facilities to oversee care management
Transition Feedback opportunities

Support Programs
37
Support Programs
Consistent Care Program (EDCCP) Patients who had Emergency Room visits >12 times in previous 12 months.
Care Plan is developed by a team coordinated by an assigned Social Worker.
Communication tool provides data specific to patient’s medical Hx. and current medical needs, and Goals of Care for when patients presents again.
Advance Medical Team
High Risk patients assigned a Care Navigator to work with them across the continuum.
Team includes resource for Outpatient Social Work and Pharmacy consult for medication management.

Support Programs39
Heart Failure Clinics
MD/NP home visits programs
Outpatient Palliative Care program
Health Care Navigators
ACO case managers
Discharge phone calls program

UCSF Automated Calls Program
Goal: All patients receive a discharge phone call- 80%
Currently: ED, Neuro, Medicine, Ortho, Cardiac
Disease Management
Heart Failure, COPD, AMI
– Specific calls –promotes accountability
– 4-6 additional calls over 30 days
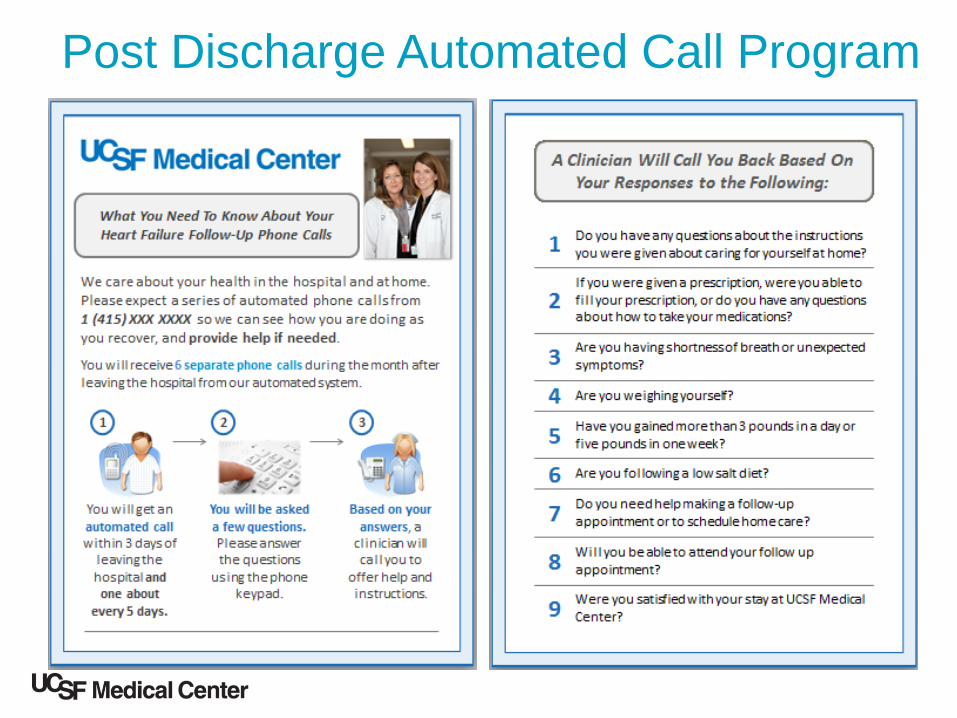
Post Discharge Automated Call Program

HealtheHeart Study
Nurse Avatar “Molly”
Heart Failure management
Calls recorded by Heart Failure Coordinators
Weights, B/P, Heart Rate
Promotes self care management
Inpatient Survey- patients 65+ positive feedback

UCSF Palliative Care Program43

Palliative Care
Palliative care proven to improve symptoms, quality of life,
satisfaction, and patient and family outcomes
25% of our Heart Failure patients die within one year
Up to one- half of deaths with Heart Failure are due to Sudden Death
Palliative care prompts patients to think about all their options in the
future and to start the important discussions for making plans
Standard- consult on 3rd Readmission /Year
New this year, PC MD on Heart Failure Service
Increased palliative care options in outpatient setting- expansion
Pantilat and Steimle JAMA 2004;291:2476-82Wright et al. JAMA 2008;300:1665-73Morrison J Palliat Med 2005;8:S79-87

The Goals of Care Conversation:
When you think about the future what do you hope for?
When you think about what lies ahead, what worries you most?
How do you approach these decisions in “your” family?
Sit and listen
Wait full 2 minutes without a wordSteve Pantilat, MD
Director of the UCSF Palliative Care Program

Results
46

47

Medicare FFS 30 day Readmissions48
FY 2012 FY 2013 FY 2014FY 2015
YTDAMI 12.3% 15.8% 13.6% 20%CHF 22.3% 17.0% 18.4% 16.6%
COPD 17.5% 13.5% 16.2% 23.9%PNA 18.1% 13.3% 14.6% 6.9%
Index 67 readmit 16
Index 40 readmit 8
HF – 75%
of patients in
Transitions
Program

UCSF Readmission Dashboard

Results


HCAHPS RESULTSDISCHARGE INFORMATION (% Yes)
The following questions make up this composite measure:
#19 – During hospital stay, did doctors, nurses or other hospital staff talk about whether you would have the help
you needed when you left the hospital?
#20 - During hospital stay, did you get the information in writing about what symptoms
or health problems to look out for after you left the hospital?

Lessons Learned
53

Lessons Learned
Importance of engaged executive leaders and physicians.
Patients and families help transform care in profound ways.
The patient and family home environment must be understood.
Involving frontline staff in the changes helps them understand why they are important and grows ownership by engaging them in redesign.

Lessons Learned (cont)
The role of Information Technology in the process should be addressed simultaneously with the work.
Ongoing monitoring of Process and Outcome Measures is important to hardwiring best practices.
Using patient stories unleashes energy and participation that becomes evident in process and outcome results.
The power of relationship building and collaboration of the cross-continuum team builds new ideas to work and removes many of the “silos’ in the care.

Lessons Learned…
Collaboration with IHI – extremely valuable
Dedicated Heart Failure/Disease Management
Program Coordinators - accountable, reliable
processes
Willingness to test, trial, and change interventions
Make efforts to move outside of silos
Senior Leadership and Champions necessary
Cohesive, committed multidisciplinary cross
continuum teams

Lessons Learned…
Palliative Care Team Collaboration
Home Care collaboration and referrals
Outpatient program & Community Partners essential
Results are not immediate – takes time to show
improvement
Teach Back works – focus on Health Literacy
Technology – great potential – Here to stay
Power of the patient story to learn from and drive change


















