REDUCING HOSPITAL READMISSIONS BY TRANSFORMING CHRONIC · PDF fileREDUCING HOSPITAL...
71
REDUCING HOSPITAL READMISSIONS BY TRANSFORMING CHRONIC CARE Harold D. Miller Executive Director, Center for Healthcare Quality and Payment Reform and Strategic Initiatives Consultant, Pittsburgh Regional Health Initiative
Transcript of REDUCING HOSPITAL READMISSIONS BY TRANSFORMING CHRONIC · PDF fileREDUCING HOSPITAL...

REDUCING HOSPITAL READMISSIONS
BY TRANSFORMING CHRONIC CARE
Harold D. MillerExecutive Director,
Center for Healthcare Quality and Payment Reformand
Strategic Initiatives Consultant, Pittsburgh Regional Health Initiative

2© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Some Background
• About the Center for Healthcare Quality and Payment Reform– Founded in 2008 to encourage comprehensive, outcome-driven,
regionally-grounded approaches to achieving higher-value healthcare
– Works at the national level and with regions around the country to develop and implement payment reforms and delivery system reforms
• About the Pittsburgh Regional Health Initiative– A non-profit Regional Health Improvement Collaborative founded in
1997 to improve the safety and quality of health care in the Pittsburgh Region and nationally
– Board members include CEOs and senior staff from regional hospitals, physician groups, health insurers, employers, and consumers
– Funded by local corporations, foundations, health plans, and government contracts and grants
– Organizes and supports demonstration projects in hospital infection reduction, chronic care improvement, etc.
– Trains health care staff in Perfecting Patient CareSM
, a quality improvement method based on the Toyota Production System

3© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
It Started in 2007 With Data:
PA’s All-Payer Readmission Data

4© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Readmissions in Western PA, 2005-06
0
500
1,000
1,500
2,000
2,500
3,000
3,500
4,000
CHF Pneumonia Depression COPD Kidney
Failure
Abnormal
Heartbeat
Diabetes Asthma
Diagnosis at Initial Admission
# R
ea
dm
itte
d
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
% R
ea
dm
itte
d
# Readmits
Readmit Rate
Chronic Diseases Are Largest
Categories of Readmissions

5© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Readmissions in Western PA, 2005-06
0
500
1,000
1,500
2,000
2,500
3,000
3,500
4,000
CHF Pneumonia Depression COPD Kidney
Failure
Abnormal
Heartbeat
Diabetes Asthma
Diagnosis at Initial Admission
# R
ea
dm
itte
d
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
% R
ea
dm
itte
d
# Readmits
Readmit Rate
Initial Focus: COPD is 4th Highest
Volume & 25% Readmission Rate

6© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Diagnosis Chains:
Pneumonia as Initial Admit
1st Adm PDx 2nd Adm PDx 3rd Adm PDx 4th Adm PDx
Pneumonia COPD COPD
435 51 48
12% Pneumonia
0
Pneumonia COPD
71 1
16%
All Diagnoses COPD
23
All Diagnoses COPD
19
Pneumonia
as PDx on
first
admission,
COPD on
PDx or SDx
on some
admission

7© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Readmissions in Western PA, 2005-06
0
500
1,000
1,500
2,000
2,500
3,000
3,500
4,000
CHF Pneumonia Depression COPD Kidney
Failure
Abnormal
Heartbeat
Diabetes Asthma
Diagnosis at Initial Admission
# R
ea
dm
itte
d
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
% R
ea
dm
itte
d
# Readmits
Readmit Rate
40% of Pneumonia Readmits
Are COPD Patients
C
O
P
D

8© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Readmissions in Western PA, 2005-06 (Adjusted)
0
500
1,000
1,500
2,000
2,500
3,000
3,500
4,000
CHF Pneumonia
w/o COPD
Depression COPD
+Pneum.
Kidney
Failure
Abnormal
Heartbeat
Diabetes Asthma
Diagnosis at Initial Admission
# R
ea
dm
itte
d
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
% R
ea
dm
itte
d
# Readmits
Readmit Rate
So COPD Patients are 2nd
Highest Volume of Readmits

9© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
33% of Admissions Under Age 65,
With Similar Readmission RatesCOPD Admissions/Readmissions by Age
0
500
1,000
1,500
2,000
2,500
20-49 50-59 60-69 70-79 80+
Age Group
# R
ea
dm
itte
d
0%
5%
10%
15%
20%
25%
30%
% R
ea
dm
itte
d
# Admits
% Readmit
Readmission Rate
Similar for All Ages

10© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
60% of COPD Readmissions
Are for COPD or Lung Problems
COPD (37%)
Other Lung Condition
(21%)
Non-Pulmonary Diagnosis
(42%)
0%
5%
10%
15%
20%
25%
30%
30
Day
Re
adm
issi
on
Rat
e
Reasons for Readmission of COPD Patient Discharges

11© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
*Long-Term Treatment for
Stable COPD
Avoidance of Risk Factors;
Influenza Vaccination
Add Rapid-Acting
Bronchodilator when indicated
Add Short or Long-acting
Bronchodilators and
Pulmonary Rehabilitation
Add medium to high-dose
inhaled or oral
glucocorticosteroids or
antibiotics when indicated
Add long-term oxygen;
consider surgical referral
At RiskNormal lung function
with or without
Chronic symptoms
Moderate COPDChronic symptoms
Shortness of breath
on exertion
Severe COPDShortness of breath
worsens
Exacerbations common
Mild COPDAbnormal lung function
with or without
Chronic symptoms
Very Severe COPDQuality of life impaired
Exacerbations may be
Life threatening
*Adapted from
Global Initiative for COPD
www.goldcopd.org
Clinical Practice Guidelines Exist

12© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
*Long-Term Treatment for
Stable COPD
Avoidance of Risk Factors;
Influenza Vaccination
Add Rapid-Acting
Bronchodilator when indicated
Add Short or Long-acting
Bronchodilators and
Pulmonary Rehabilitation
Add medium to high-dose
inhaled or oral
glucocorticosteroids or
antibiotics when indicated
Add long-term oxygen;
consider surgical referral
At RiskNormal lung function
with or without
Chronic symptoms
Moderate COPDChronic symptoms
Shortness of breath
on exertion
Severe COPDShortness of breath
worsens
Exacerbations common
Mild COPDAbnormal lung function
with or without
Chronic symptoms
Very Severe COPDQuality of life impaired
Exacerbations may be
Life threatening
*Adapted from
Global Initiative for COPD
www.goldcopd.org
Treatment Primarily Relies on
Use of One or More Inhalers

13© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Medication Access & Education
is Critical for Chronic Diseases
FOR COPD PATIENTS:
•79% do not know how to use their inhalers properly
• Some have 3 different inhalers, all of which work differently
Inhale slowly Inhale quickly Inhale quickly
14© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
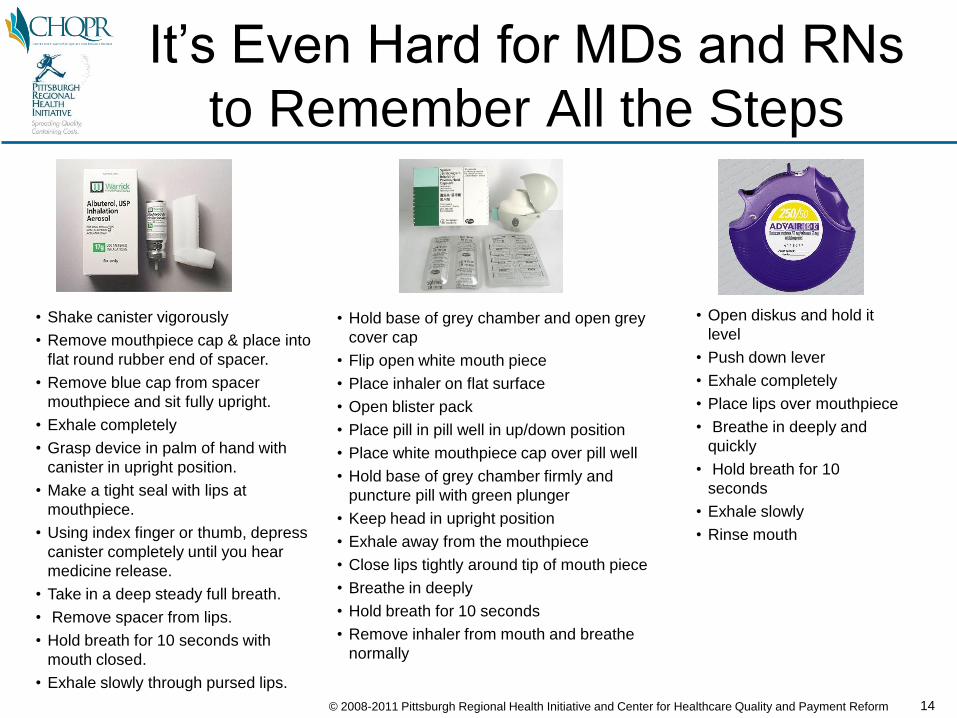
It’s Even Hard for MDs and RNs
to Remember All the Steps
• Open diskus and hold it
level
• Push down lever
• Exhale completely
• Place lips over mouthpiece
• Breathe in deeply and
quickly
• Hold breath for 10
seconds
• Exhale slowly
• Rinse mouth
• Hold base of grey chamber and open grey
cover cap
• Flip open white mouth piece
• Place inhaler on flat surface
• Open blister pack
• Place pill in pill well in up/down position
• Place white mouthpiece cap over pill well
• Hold base of grey chamber firmly and
puncture pill with green plunger
• Keep head in upright position
• Exhale away from the mouthpiece
• Close lips tightly around tip of mouth piece
• Breathe in deeply
• Hold breath for 10 seconds
• Remove inhaler from mouth and breathe
normally
• Shake canister vigorously
• Remove mouthpiece cap & place into
flat round rubber end of spacer.
• Remove blue cap from spacer
mouthpiece and sit fully upright.
• Exhale completely
• Grasp device in palm of hand with
canister in upright position.
• Make a tight seal with lips at
mouthpiece.
• Using index finger or thumb, depress
canister completely until you hear
medicine release.
• Take in a deep steady full breath.
• Remove spacer from lips.
• Hold breath for 10 seconds with
mouth closed.
• Exhale slowly through pursed lips.

15© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Results of Interviews with
Readmitted Patients
0%
10%
20%
30%
40%
50%
Yes, All Yes, Some No, None
Has Anyone Shown You How to Use Inhalers/Nebulizers?
0%
20%
40%
60%
80%
Yes No
Has Anyone Watched You Use Inhalers/Nebulizers?

16© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
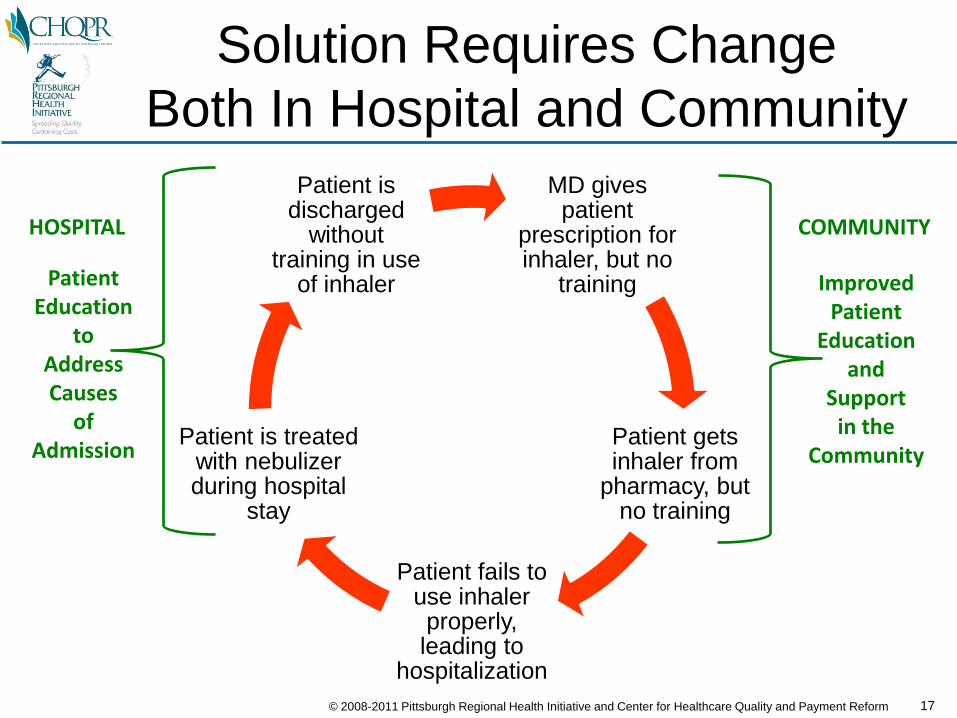
The Vicious Cycle of Chronic
Disease Admission/Readmissions
MD gives patient
prescription for inhaler, but no
training
Patient gets inhaler from
pharmacy, but no training
Patient fails to use inhaler properly, leading to
hospitalization
Patient is treated with nebulizer during hospital
stay
Patient is discharged
without training in use of inhaler
17© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Solution Requires Change
Both In Hospital and Community
MD gives patient
prescription for inhaler, but no
training
Patient gets inhaler from
pharmacy, but no training
Patient fails to use inhaler properly, leading to
hospitalization
Patient is treated with nebulizer during hospital
stay
Patient is discharged
without training in use
of inhaler ImprovedPatient
Educationand
Supportin the
Community
PatientEducation
toAddressCauses
ofAdmission
COMMUNITYHOSPITAL

18© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
How is a Patient’s Chronic
Disease Managed Today?
Treat Exacerbation
HOSPITAL
COMMUNITY CARE
Readm
issio
n
Admission
Discharge
MD Treatment
When/If
Office Visit Occurs
Limited
Patient
Education
ER Used As
Solution to
Problems

19© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Most Readmission Initiatives
Focus on the Transition Process
Treat Exacerbation
HOSPITAL
COMMUNITY CARE
Readm
issio
n
Admission
Discharge
MD Treatment
When/If
Office Visit Occurs
Limited
Patient
Education
ER Used As
Solution to
Problems
Improving Transition

20© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Not Just a Discharge Issue: 60%
of Readmits Occur After 30 Days
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0-7 Days 8-30 Days 31-90 Days 91-180 Days 181-365 Days
Days to Readmission
30-Day Readmits

21© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
What We Tried to Fix:
Better Discharge Planning, PLUS...
Treat Exacerbation
HOSPITAL
COMMUNITY CARE
Readm
issio
n
Admission
Discharge
MD Treatment
When/If
Office Visit Occurs
Improved
Patient
Education
ER Used As
Solution to
Problems

22© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
What We Tried to Fix:
Improved Care in Hospital
Treat Exacerbation
Address Root Causes:
-medication skills
-smoking cessation
-other
CARE PROTOCOL
Improved
Patient
Education
HOSPITAL
COMMUNITY CARE
Readm
issio
n
Admission
Discharge
MD Treatment
When/If
Office Visit Occurs
Identify
as
COPD
Patient
ER Used As
Solution to
Problems

23© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
What We Tried to Fix:
Expanded PCP/Care Mgr Support
Identify
as
COPD
Patient
Treat Exacerbation
Address Root Causes:
-medication skills
-smoking cessation
-other
CARE PROTOCOL
Improved
Patient
Education
HOSPITAL
COMMUNITY CARE
Readm
issio
n
Admission
Discharge
MD Treatment
RN Care Manager
Medication Access
CARE PROTOCOL
Prompt
Follow-up :
- Home Visit
- PCP Visit
ER Used As
Solution to
Problems

24© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
What We Tried to Fix:
Non-Hospital Solution to Problems
Identify
as
COPD
Patient
Treat Exacerbation
Address Root Causes:
-medication skills
-smoking cessation
-other
CARE PROTOCOL
Improved
Patient
Education
HOSPITAL
COMMUNITY CARE
Readm
issio
n
Admission
Discharge
MD Treatment
RN Care Manager
Medication Access
Prompt Response
to Exacerbations:- Action Plan
- 24/7 Phone Support
CARE PROTOCOL
Prompt
Follow-up :
- Home Visit
- PCP Visit
25© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
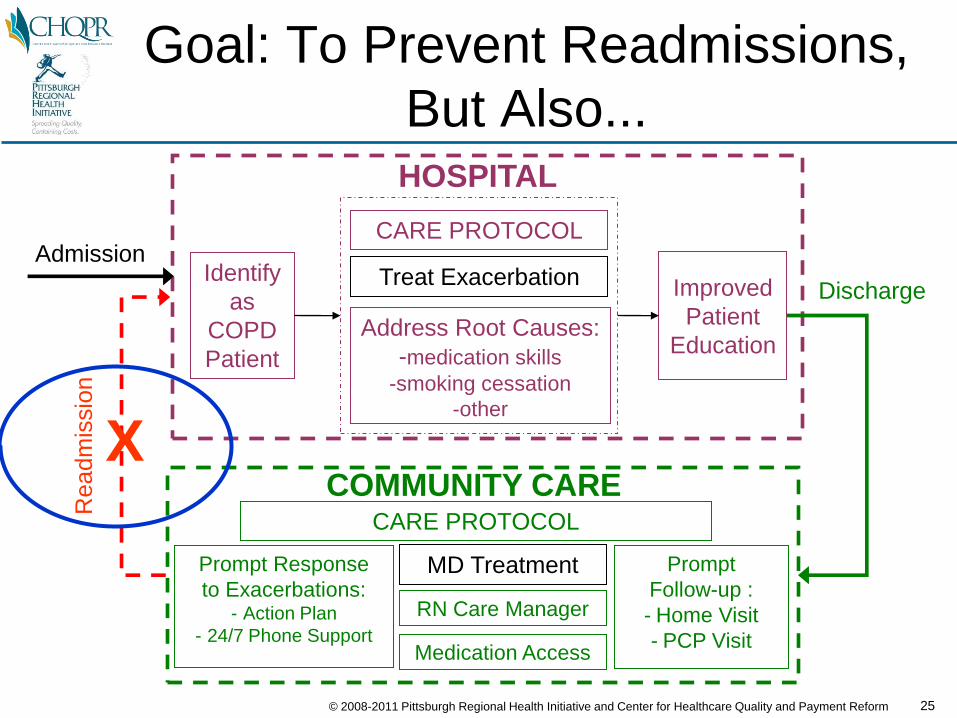
Goal: To Prevent Readmissions,
But Also...
Identify
as
COPD
Patient
Treat Exacerbation
Address Root Causes:
-medication skills
-smoking cessation
-other
CARE PROTOCOL
Improved
Patient
Education
HOSPITAL
COMMUNITY CARE
Readm
issio
n
X
Admission
Discharge
MD Treatment
RN Care Manager
Medication Access
Prompt Response
to Exacerbations:- Action Plan
- 24/7 Phone Support
CARE PROTOCOL
Prompt
Follow-up :
- Home Visit
- PCP Visit

26© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
... Ultimately to Prevent
Initial Admissions
Treat Exacerbation
Address Root Causes:
-medication skills
-smoking cessation
-other
CARE PROTOCOL
Improved
Patient
Education
HOSPITAL
Adm
issio
n/R
eadm
issio
n
X
Patientwith
ChronicDisease
COMMUNITY CARE
MD Treatment
RN Care Manager
Medication Access
Prompt Response
to Exacerbations:- Action Plan
- 24/7 Phone Support
CARE PROTOCOL
Dis
charg
e

27© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Barrier: One Hospital,
But Many MD Practices
MD Office
MD Office
MD Office
MD Office
MD Office
MD Office
MD Office
HOSPITAL
28© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
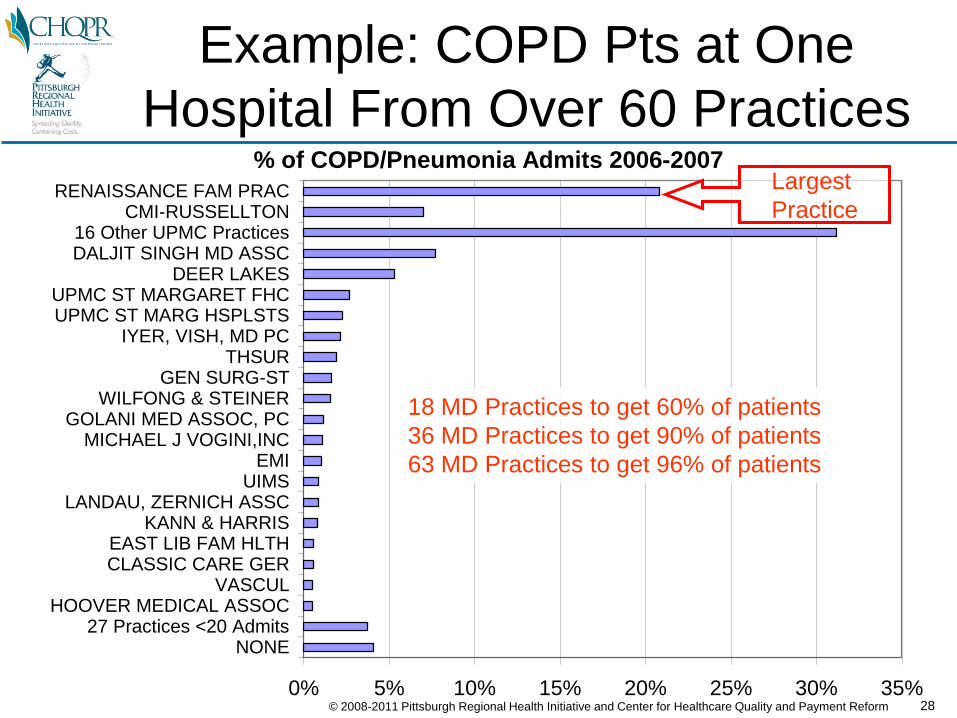
Example: COPD Pts at One
Hospital From Over 60 Practices% of COPD/Pneumonia Admits 2006-2007
0% 5% 10% 15% 20% 25% 30% 35%
NONE27 Practices <20 Admits
HOOVER MEDICAL ASSOCVASCUL
CLASSIC CARE GEREAST LIB FAM HLTH
KANN & HARRISLANDAU, ZERNICH ASSC
UIMSEMI
MICHAEL J VOGINI,INCGOLANI MED ASSOC, PC
WILFONG & STEINERGEN SURG-ST
THSURIYER, VISH, MD PC
UPMC ST MARG HSPLSTSUPMC ST MARGARET FHC
DEER LAKESDALJIT SINGH MD ASSC16 Other UPMC Practices
CMI-RUSSELLTONRENAISSANCE FAM PRAC Largest
Practice
18 MD Practices to get 60% of patients
36 MD Practices to get 90% of patients
63 MD Practices to get 96% of patients

29© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Solution: Start with Larger MD
Practices and Expand to Others
MD Office
MD Office
MD Office
MD Office
MD Office
MD Office
MD Office
HOSPITAL

30© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Initial Demonstration Sites
UPMC
St. Margaret
Hospital
Renaissance Family Practice
Other MD Practices
DEMONSTRATION SITE 1
Forbes
Regional
Hospital
Premier Medical Associates
DEMONSTRATION SITE 2
Other MD Practices

31© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
0%
5%
10%
15%
20%
25%
30%
35%
40%
Mey
ersd
ale
Com
mun
ity
Cla
rion
G
rove
Cit
y C
har
les
Co
le M
emo
rial
A
liqui
ppa
Com
mun
ity
Was
hing
ton
Ma
ge
e-W
om
en
s El
k R
egio
nal
Wes
tmor
elan
d R
egio
nal
Ellw
ood
Cit
y M
onon
gahe
la V
alle
y Sh
aro
n R
eg
ion
al
Can
onsb
urg
Gen
eral
A
lleg
hen
y G
ener
al
Tyro
ne
UPM
C S
t M
arga
ret
UPM
C N
orth
wes
t M
ercy
Pit
tsbu
rgh
UPM
C S
outh
Sid
e C
orr
y M
emo
rial
Je
ffe
rso
n R
eg
ion
al
UP
MC
Pre
sby
Shad
ysid
e La
tro
be
Are
a
Fric
k TO
TAL:
Sta
tew
ide
Wes
tern
PA
Ho
sp/F
orbe
s H
ighl
ands
Ka
ne C
omm
unit
y W
este
rn P
enn
sylv
ania
A
CM
H H
osp
ita
l C
lear
fiel
d D
uB
ois
Re
gio
na
l A
ltoo
na R
egio
nal
But
ler
Mem
oria
l T
itu
svill
e A
rea
A
lle-K
iski
C
on
em
au
gh
Va
lley
Me
mo
ria
l U
PMC
McK
eesp
ort
UPM
C P
assa
vant
Pu
nxsu
taw
ney
Are
a M
edic
al C
ente
r B
eave
r Se
wic
kley
Val
ley
Ha
mot
In
dia
na
Re
gio
na
l Ja
mes
on
Mem
ori
al
Min
ers
St C
lair
Mem
oria
l U
PMC
Bra
ddoc
k U
nio
nto
wn
M
illcr
ee
k C
om
mu
nit
y M
eadv
ille
War
ren
Gen
eral
U
PMC
Ho
rizo
n Sa
int V
ince
nt H
ealt
h So
mer
set
Cen
ter
He
alth
U
PM
C B
edfo
rd
Bro
okv
ille
N
ason
W
este
rn P
enn
sylv
ania
B
rad
ford
Re
gio
na
l M
ercy
Jea
nn
ette
So
uth
we
st R
eg
ion
al M
C
Win
dber
O
hio
Va
lle
y G
en
era
l
COPD Readmission Rate, Western PA Hospitals, 2005-06
Above-Average But Typical COPD
Readmit Rate at Both Hospitals
UPMC St. Margaret
Forbes Reg.Hospital

32© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Part 1: Redesigning Inpatient
Care to Reduce Readmissions
Identify
as
COPD
Patient
Treat Exacerbation
Address Root Causes:
-medication skills
-smoking cessation
-other
CARE PROTOCOL
Improved
Patient
Education
HOSPITAL
COMMUNITY CARE
Readm
issio
n
X
Admission
Discharge
MD Treatment
RN Care Manager
Medication Access
Prompt Response
to Exacerbations:- Action Plan
- 24/7 Phone Support
CARE PROTOCOL
Prompt
Follow-up :
- Home Visit
- PCP Visit

33© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
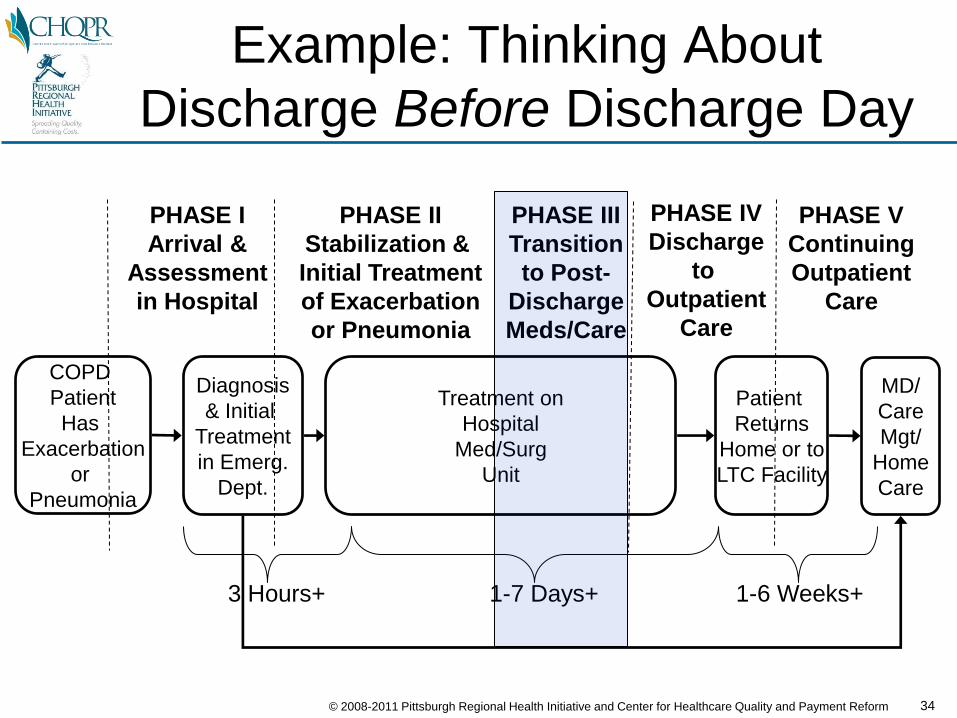
Phases of Care for a Hospitalized
COPD Patient
COPD
Patient
Has
Exacerbation
or
Pneumonia
Diagnosis
& Initial
Treatment
in Emerg.
Dept.
Treatment on
Hospital
Med/Surg
Unit
Patient
Returns
Home or to
LTC Facility
PHASE I
Arrival &
Assessment
in Hospital
PHASE II
Stabilization &
Initial Treatment
of Exacerbation
or Pneumonia
PHASE III
Transition
to Post-
Discharge
Meds/Care
PHASE IV
Discharge
to
Outpatient
Care
PHASE V
Continuing
Outpatient
Care
MD/
Care
Mgt/
Home
Care
3 Hours+ 1-7 Days+ 1-6 Weeks+
34© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Example: Thinking About
Discharge Before Discharge Day
COPD
Patient
Has
Exacerbation
or
Pneumonia
Diagnosis
& Initial
Treatment
in Emerg.
Dept.
Treatment on
Hospital
Med/Surg
Unit
Patient
Returns
Home or to
LTC Facility
PHASE I
Arrival &
Assessment
in Hospital
PHASE II
Stabilization &
Initial Treatment
of Exacerbation
or Pneumonia
PHASE III
Transition
to Post-
Discharge
Meds/Care
PHASE IV
Discharge
to
Outpatient
Care
PHASE V
Continuing
Outpatient
Care
MD/
Care
Mgt/
Home
Care
3 Hours+ 1-7 Days+ 1-6 Weeks+

PHASE III
Transition to Post-Discharge Meds/Care
Treatment on Hospital Med/Surg Unit
MD
Orders
Respiratory Therapy Administers Nebulizer
RN Administers MDI Inhalers
No Transition to
Inhaler Before
Discharge
CU
RR
EN
T S
TA
TE
RN Administers All Other MedicationsLittle or No
Patient Training
on Inhaler

PHASE III
Transition to Post-Discharge Meds/Care
Treatment on Hospital Med/Surg Unit
MD
Orders
Respiratory Therapy Administers Nebulizer
RN Administers MDI Inhalers
No Transition to
Inhaler Before
Discharge
MD
Orders
CU
RR
EN
T S
TA
TE
RE
CO
MM
EN
DA
TIO
N
RN Administers All Other Medications
Respiratory Therapy
Administers Nebulizer
Resp. Therapy Trains Patient on
Placebo MDI As Early As Possible
Resp. Therapy Administers
MDI Inhaler until Discharge
Little or No
Patient Training
on Inhaler
RN Administers All Other Medications
Resp. Therapy Recommends
When Transition to Inhaler Occurs
37© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
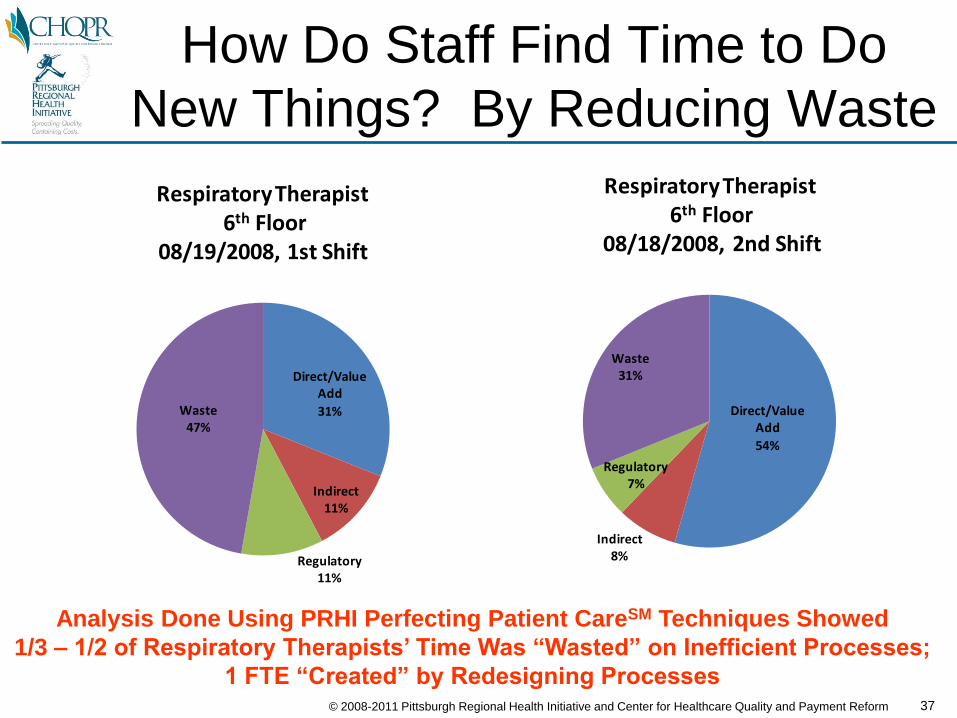
How Do Staff Find Time to Do
New Things? By Reducing Waste
Direct/Value Add
54%
Indirect8%
Regulatory7%
Waste31%
Respiratory Therapist6th Floor
08/18/2008, 2nd Shift
Direct/Value Add
31%
Indirect11%
Regulatory11%
Waste47%
Respiratory Therapist6th Floor
08/19/2008, 1st Shift
Analysis Done Using PRHI Perfecting Patient CareSM Techniques Showed
1/3 – 1/2 of Respiratory Therapists’ Time Was “Wasted” on Inefficient Processes;
1 FTE “Created” by Redesigning Processes
38© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Other Inpatient Changes Made
• Process Improvements– EHR Order Set for COPD Patients
– Improved Patient Education Materials; Same Materials Now Used by All Department (RT, PT, OT, RNs)
– Better Smoking Cessation Process
– Comprehensive Discharge Preparation Checklist (Paper, But Still Not in EHR…)
• Monitoring/Analyzing Performance– Monthly Reports on Readmission Rates
– Questionnaire Administered to Readmitted Patients
– Chart Reviews to Ensure Processes Are Being Followed
– Monthly Meetings to Review Performance

39© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Part 2: Creating a
Community Care (RN) Manager
Identify
as
COPD
Patient
Treat Exacerbation
Address Root Causes:
-medication skills
-smoking cessation
-other
COPD PROTOCOL
Improved
Discharge
Planning
HOSPITAL
COMMUNITY CARE
Readm
issio
n
X
Admission
Discharge
MD Treatment
RN Care Manager
Medication Access
Prompt Response
to Exacerbations:- Action Plan
- 24/7 Phone Support
CARE PROTOCOL
Prompt
Follow-up :
- Home Visit
- PCP Visit

40© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Research: Dramatic Impact From
Community Care Managers
• 40% reduction in hospital admissions, 41% reduction in ER
visits for exacerbations of COPD using in-home & phone
patient education by nurses or respiratory therapists (2003)J. Bourbeau, M. Julien, et al, “Reduction of Hospital Utilization in Patients with Chronic
Obstructive Pulmonary Disease: A Disease-Specific Self-Management Intervention,”
Archives of Internal Medicine 163(5), 2003
• 27% reduction in hospital admissions, 21% reduction in ER
visits for COPD patients through self-management education
(2005)M.A. Gadoury, K. Schwartzman, et al, “Self-Management Reduces Both Short- and Long-
Term Hospitalisation in COPD,” European Respiratory Journal 26(5), 2005

41© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Challenge: Payers Don’t
Reimburse for Care Managers• Medicare, Medicaid, and commercial health plans do not
reimburse primary care practices for calls/visits by nurses
• Major health plans already employ their own care managers,
at considerable expense– not integrated with physician practices
– little or no face-to-face contact w/patients
(primary mode of contact is by telephone)
– paying for care managers in MD practices seems like (and is)
duplication
• Different solutions from different health plans
means providers can’t treat all patients alike– e.g., “practice-based care manager” employed by a particular health
plan could span multiple small providers, but would only improve care
for the patients of that particular health plan

42© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Our (Short-Run) Solution
• Grant from a large private foundation in the
community to pay for the costs of the care
managers (as well as coaching and other support to
hospitals and physician practices)
• Solution would end when the grant runs out unless
payment reforms are implemented
43© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Goal: Establishing the Business
Case for Nurse Care Managers
Reduction in Hospital Payments
from Reduced Readmissions
Costs of Interventions
(Community Care Mgrs, etc.)-
>>$0

44© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Readmissions Are Costly for
Medicare & Other Payers
CURRENT
# Admissions/Year:
Cost of Readmissions:
500
25%
$5,400
$675,000
$/Admission
(Medicare/No Complic.):
% Readmitted:
(<30 Days)

45© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Goal: Reduce Readmissions By
More Than Cost of Care Mgt
CURRENT
# Admissions/Year:
% Readmitted:
(<30 Days)
$/Admission
(Medicare/No Complic.):
Cost of Readmissions:
Net Savings to Payer:
20% REDUCTION
500
25%
$5,400
500
20%
$5,400
$675,000 $540,000
$55,000
Cost of Care Mgr: $80,000

46© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Hiring the
Community Care Manager• Goals:
– Integral member of primary care team
– Focus on patients with COPD (initially) with ability to expand to other
patients with high rates of readmission in the future
– Sufficient number of cases at risk of hospitalization to justify expense
of a new position
– Willingness/ability to make home visits (not just phone calls)

47© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Challenge: Where Does the
Community Care Manager Work?• Goals:
– Integral member of primary care team
– Focus on patients with COPD (initially) with ability to expand to other
patients with high rates of readmission in the future
– Sufficient number of cases at risk of hospitalization to justify expense
of a new position
– Willingness/ability to make home visits (not just phone calls)
• Options:– Employee in physician practice
• works only for large practices

48© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
2/3 of MDs in
Practices of 5 or Smaller
0%
5%
10%
15%
20%
25%
1 2 3 4 5 6 7 8 9 101112131516181921222528
Size of Physician Practice
% of Regional Physicians by Practice Size

49© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Solution: Sharing the
Community Care Manager• Goals:
– Integral member of primary care team
– Focus on patients with COPD (initially) with ability to expand to other
patients with high rates of readmission in the future
– Sufficient number of cases at risk of hospitalization to justify expense
of a new position
– Willingness/ability to make home visits (not just phone calls)
• Options:– Employee in physician practice
• works only for large practices
– Shared employee among physician practices
– Hospital-based employee (covering multiple small practices)
– Contract for services with home health agency

50© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Part 3: Ensuring Prompt
Response to Exacerbations
Identify
as
COPD
Patient
Treat Exacerbation
Address Root Causes:
-medication skills
-smoking cessation
-other
COPD PROTOCOL
Improved
Discharge
Planning
HOSPITAL
COMMUNITY CARE
Readm
issio
n
X
Admission
Discharge
MD Treatment
RN Care Manager
Medication Access
Prompt Response
to Exacerbations:- Action Plan
- 24/7 Phone Support
CARE PROTOCOL
Prompt
Follow-up :
- Home Visit
- PCP Visit
51© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
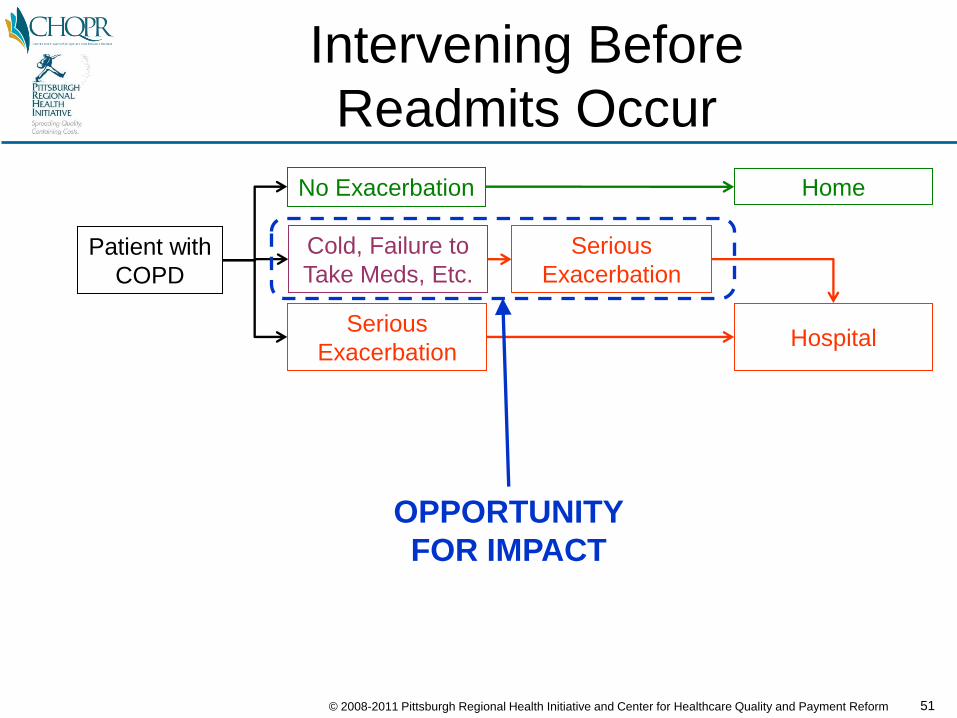
Intervening Before
Readmits Occur
Patient with
COPD
No Exacerbation
Cold, Failure to
Take Meds, Etc.
Serious
Exacerbation
Serious
ExacerbationHospital
Home
OPPORTUNITY
FOR IMPACT

52© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Creating a COPD Action Plan
Patient with
COPD
No Exacerbation
Cold, Failure to
Take Meds, Etc.
Serious
Exacerbation
Patient with
COPD
Serious
ExacerbationHospital
Home
No Exacerbation
Cold, Failure to
Take Meds, Etc.
ACTION PLAN:
Call MD/RN,
Add Meds, Etc.
Serious
ExacerbationHospital
Home
BEFORE
AFTER

53© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Making an Action Plan Work
Primary
Care
Practice
Patient
Must Be Willing to
Call Right Away
For Help Resolving
an Exacerbation
Must Be Able to
Respond Right Away
When a Patient Calls
(And Not By Sending
Them to the ER)

54© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
How We Hope A Primary Care
Practice Answers Patient Calls
Patient with
Action PlanHas
Problem
CallsPCP Office
During
Office
Hours:
After
Office
Hours:
Speaks toScheduler
Patient treated
andremainsout of
hospital
Seen byPCP
CallsAnsw. Svc.
Speaks toPCP

55© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
What Actually Happens,
All Too Often
Patient with
Action PlanHas
Problem
CallsPCP Office
During
Office
Hours:
After
Office
Hours:
Goes toER
Can’t GetThrough
Speaks toScheduler
Patient admitted
to Hospital
No ApptsAvailable
Patient treated
andremainsout of
hospital
Seen byPCP
CallsAnsw. Svc.
Goes toER
Patient admitted
to Hospital
Speaks toPCP
Speaks toOn-Call MD

56© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Results of Interviews with
Readmitted Patients
0%10%20%30%40%50%60%
Called Early/Several
Times
Only Called When Really Sick
Just Went to ER
Did Patient Call Doctor's Office?
0%10%20%30%40%50%
M-F Day M-F After 5pm Sat-Sun
Time Came to ER or Hospital

57© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Redesigning How a Primary Care
Practice Answers Patient Calls
Call fromPatient with
COPD Action Plan
Receptionist
AnsweringService
ScheduleVisit TodayIf Possible
PatientCan’t Come
Today
Assessed asOK to Come Tomorrow
Needs Home Visit
or Call Now
PhysicianSees
Patient
Treatment ChangedIf Needed
MD Calls& Assesses
ER VisitNeeded
Patient Stable, Can
Wait
Care MgrNotified
RequiresAdmission
Patient CanReturn Home
Communication Between
Office & Care Manager
Protocol for On-Call
Physicians to Use
Protocol for ER/Admits
Process for Office Phone Screening, Assessment, and Scheduling
NurseNotifies
Care Mgr
Home Visits for At-Risk Patients
During
Office
Hours:
After
Office
Hours:
COPD?
No
Nurse PhoneAssessment
Send toER If
Necessary
ContactRN/MD w/
FindingsNeeds Home
Visitor Call Now
Call CareMgr or
Home Care
Home Visitto Patient
Short-TermTreatment
in ER
RequiresHome Visit
to Not Admit

58© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Chain of Factors Affects
Successful Medication Usage
Diagnosis
of Disease
Stable Disease
Management
Hospitalization
Education
?
Affordability
?
Adherence
?Yes Yes Yes
No No No
Barriers to Successful Use of Chronic Disease Medication

59© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Challenge: Copays & Doughnut
Hole Deter Use of Medications
Diagnosis
of Disease
Stable Disease
Management
Hospitalization
Education
?
Affordability
?
Adherence
?Yes Yes Yes
No No No
Barriers to Successful Use of Chronic Disease Medication
Requires
Change in
Benefit Design

60© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Solutions to Medication
Access and Affordability
• Aggressive efforts to help patients obtain financial
assistance from pharmaceutical companies
• Allowing patients to take unused medications home
from the hospital
• Purchasing medication to serve as free “samples” in
practices prohibited from using drug co. samples
61© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Creating a Continuous
Improvement Process• Outcome Measurement:
– Monthly reports generated by the hospital on readmission rates
• PHC4 data indicate that for these hospitals, 80-90% of
readmissions return to the same hospital
– Tracking of individual patients in registry by Care Manager
• Causal Analysis:– Special questionnaire in hospital to all readmitted patients
– Care manager recorded reasons for hospitalization and identified any weaknesses in community support
• Prioritization of Patient Support:– Help for care managers to identify the subset of patients
where more time/help would likely have the biggest impact
62© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
0%
1%
2%
3%
4%
5%
6%
7%
8%
9%
10%
11%
12%
13%
14%
15%
Jan-Dec 2008 Jan-Dec 2009
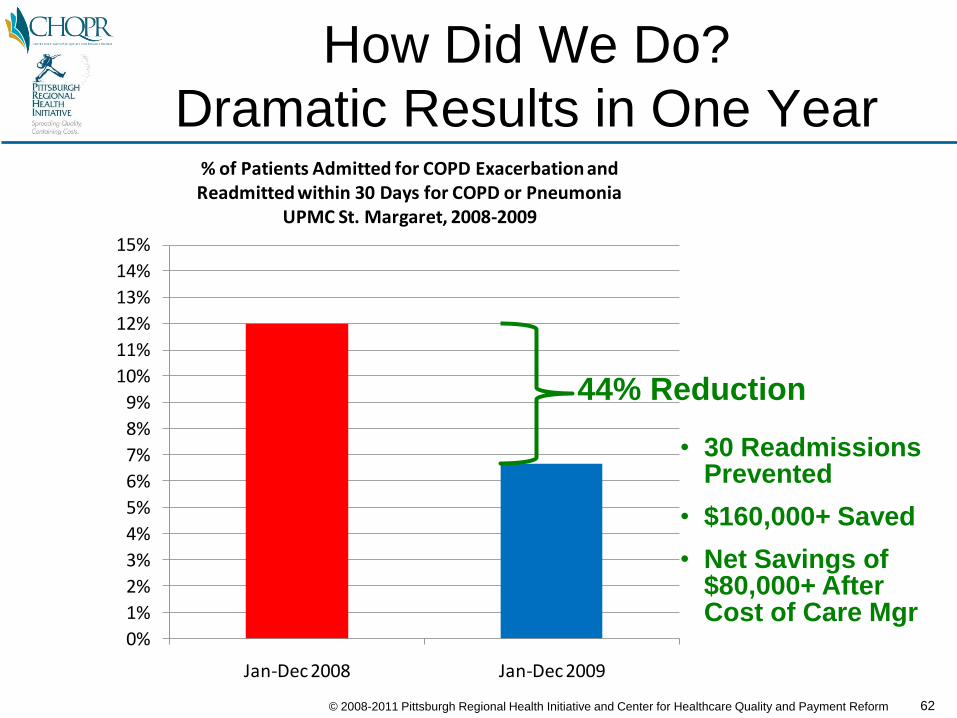
% of Patients Admitted for COPD Exacerbation andReadmitted within 30 Days for COPD or Pneumonia
UPMC St. Margaret, 2008-2009
How Did We Do?
Dramatic Results in One Year
44% Reduction
• 30 ReadmissionsPrevented
• $160,000+ Saved
• Net Savings of$80,000+ AfterCost of Care Mgr

63© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
COPD Readmissions Is Just
A Starting Point
COPD
Readmission
Reduction

64© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Similar Approach Applicable to
Initial Admissions
COPD
Readmission
Reduction
COPD
Admission
Reduction

65© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Similar Approach Likely Applicable
to Asthma
COPD
Readmission
Reduction
COPD
Admission
Reduction
Asthma
Admission
Reduction

66© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Similar Approach Likely Applicable
to Other Chronic Diseases
COPD
Readmission
Reduction
COPD
Admission
Reduction
Other
Chronic Disease
Readmission/
Admission
Reduction
Asthma
Admission
Reduction

67© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Some Lessons Learned
• Focusing on outcomes is more motivating for MDs, RNs, etc. than simply focusing on processes; evidence-based guidelines can unintentionally deter outcome-driven experimentation
• Getting accurate data rapidly enough to allow continuous improvement is difficult; just identifying COPD patients is hard
• EHRs don’t help much – they aren’t flexible enough to adapt to new care processes, and it’s hard to use them to measure progress
• Healthcare providers need conveners/facilitators/coaches to help them develop innovative, comprehensive, coordinated solutions to problems, particularly across department/organizational boundaries
• Patients need personalized education and encouragement to use treatment properly and act on symptoms early
• Home visits are an essential piece of the solution, but finding nurses willing to make home visits is difficult
• Pharmaceutical benefit design needs to be more closely linked to patient care management
• Payment reform is critical: everybody loses under today’s payment– Primary care practices lose money if they hire nurses– Hospitals lose money if readmissions are reduced

68© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Implementing
Medical Home/
Chronic
Care Model
Reducing
Hospital
Readmissions
Penalize Hospitals for
Readmissions Even
If the Cause is Poor
Primary Care
Too Many Payment Reforms
Are Proceeding in Silos
Pay More to Physicians
For Being Certified
As a “Medical Home”
And Hope That Outcomes
Improve
SILO #1 SILO #2

69© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
Implementing
Medical Home/
Chronic
Care Model
Reducing
Hospital
Readmissions
Reforming
Payment for
Primary/
Chronic
Care
Chronic
Care
Requires
Higher/Different
Payment
Reducing
Hospital
Readmissions
Requires
Improved
Community Care
Lower
Hospital
Readmissions
Provides ROI
for Chronic
Care Investment
Marrying the Medical Home
and Hospital Readmissions
70© 2008-2011 Pittsburgh Regional Health Initiative and Center for Healthcare Quality and Payment Reform
How to Analyze/Redesign Delivery
Systems to Reduce Readmissions
http://www.prhi.org/documents/ReadmissionReductionGuide-Final1-12-11.pdfhttp://www.prhi.org/documents/PRHIReadmissionBriefOverviewREVISED06-08-10.pdf

For More Information:
Harold D. MillerExecutive Director
Center for Healthcare Quality and Payment Reform
www.CHQPR.org
(412) 803-3650
Pittsburgh Regional Health Initiative
www.PRHI.org
Karen Wolk Feinstein, CEO
Keith Kanel, CMO
(412) 586-6700