Reducing chronic undernutrition in Ethiopia
27
Reducing chronic undernutrition in Ethiopia: Retrospect and prospects John Hoddinott Cornell University * Drawing on work undertaken with Guush Berhane,Yaeeun Han, Derek Headey, Kalle Hirvonen, Neha Kumar, Bart Minten, Seollee Park, and David Stifel
-
Upload
transform-nutrition -
Category
Education
-
view
119 -
download
0
Transcript of Reducing chronic undernutrition in Ethiopia
Reducing chronic undernutrition in Ethiopia:
Retrospect and prospects
John Hoddinott
Cornell University
* Drawing on work undertaken with Guush
Berhane, Yaeeun Han, Derek Headey, Kalle
Hirvonen, Neha Kumar, Bart Minten, Seollee
Park, and David Stifel

Chronic undernutrition
Given age and sex:
(HAZ) Height for age Z score = (measured height – median height for reference child) / SD
• Low HAZ reflects limited skeletal (linear) growth – it captures the cumulative effects of poor nutrition (food intake, illness or both). Low HAZ reflects chronic undernutrition
• A child is considered:– Moderately stunted if she has a HAZ ≤ -2
– Severely stunted if she has a HAZ ≤ -3
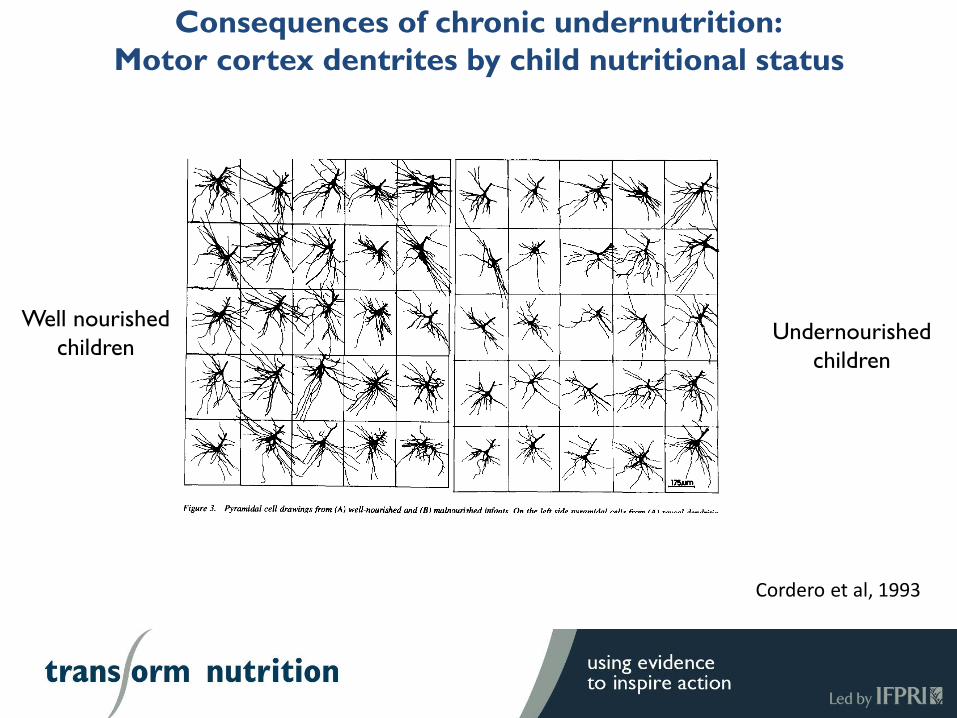
Consequences of chronic undernutrition:
Motor cortex dentrites by child nutritional status
Well nourished
childrenUndernourished
children
Cordero et al, 1993
Neurological consequences of chronic undernutrition in
the first two years of life
• In the brain, development of axonal and dentritic systems is complete by 24 months.
In children who are chronically undernourished:
• Dentrites in the motor cortex and the occipital lobe (responsible for the processing of visual information) are shorter, having fewer spines and greater numbers of abnormalities; consequently, chronic malnutrition leads to delays in the evolution of locomotor skills
• There is reduced dentrite density in the hippocampus. This adversely affects spatial navigation and memory formation
• There is reduced production of glia cells (cells in the brain responsible for producing myelin); reduced myelination of axon fibers slows the speed at which signals are transmitted across neurons
• There is a decrease in the number of neurons in the locus coeruleus which plays a role in signalling the need to inhibit the production of cortisol. Thus early-life chronic undernutrition diminishes the ability to exhibit down regulation and handle stressful situations.

Further consequences of chronic undernutrition
• Considerable evidence now exists showing that chronically undernourished children attain fewer grades of school, drop out earlier and score poorly on tests of cognitive ability– None of this is surprising given the adverse neurological consequences of chronic
undernutrition
• Reduced schooling leads to lower economic productivity, lower incomes and higher rates of poverty
• A study that traced individuals over a 35 year period found that a 1SD ↑ in HAZ at age 24m was causally linked to a 21% ↑ in per capita consumption in adulthood and a 10 percentage point reduction in the likelihood of living in poverty (Hoddinott et al, 2013)

Trends in chronic undernutrition in Ethiopia(Source: DHS)
55.4
51.3
44.4
38.4
0
10
20
30
40
50
60
2000 2005 2011 2016
17 p.p reduction
1.06% py
Among top five developing
countries
Drivers of change in stunting: 2000 – 2011(Source: Headey, Hoddinott and Park, 2016)
• Regression decomposition analysis using DHS data from 2000 and 2011 shows that rise in assets (proxy for income) accounts for about 20 percent of the reduction in stunting
• Improvements in health care (% mothers receiving 4+ ANC visits; child being born in a health center) also contribute
• Improvements in maternal schooling and reductions in open defecation play a role but the magnitudes of these effects are small
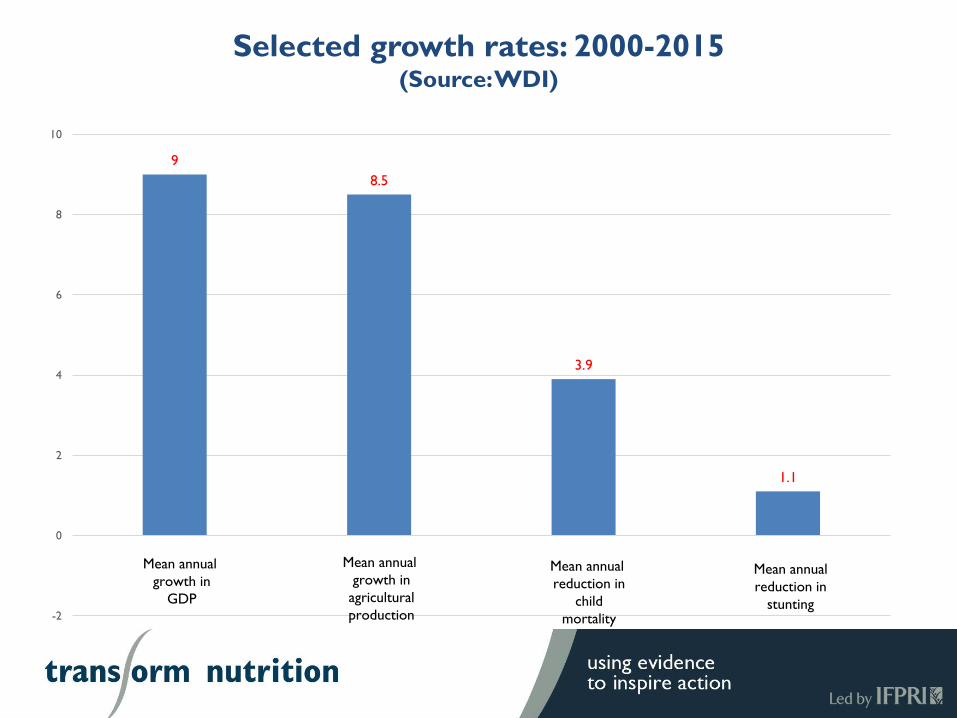
Selected growth rates: 2000-2015(Source: WDI)
9
8.5
3.9
1.1
-2
0
2
4
6
8
10
Mean annual
growth in
GDP
Mean annual
reduction in
child
mortality
Mean annual
growth in
agricultural
production
Mean annual
reduction in
stunting
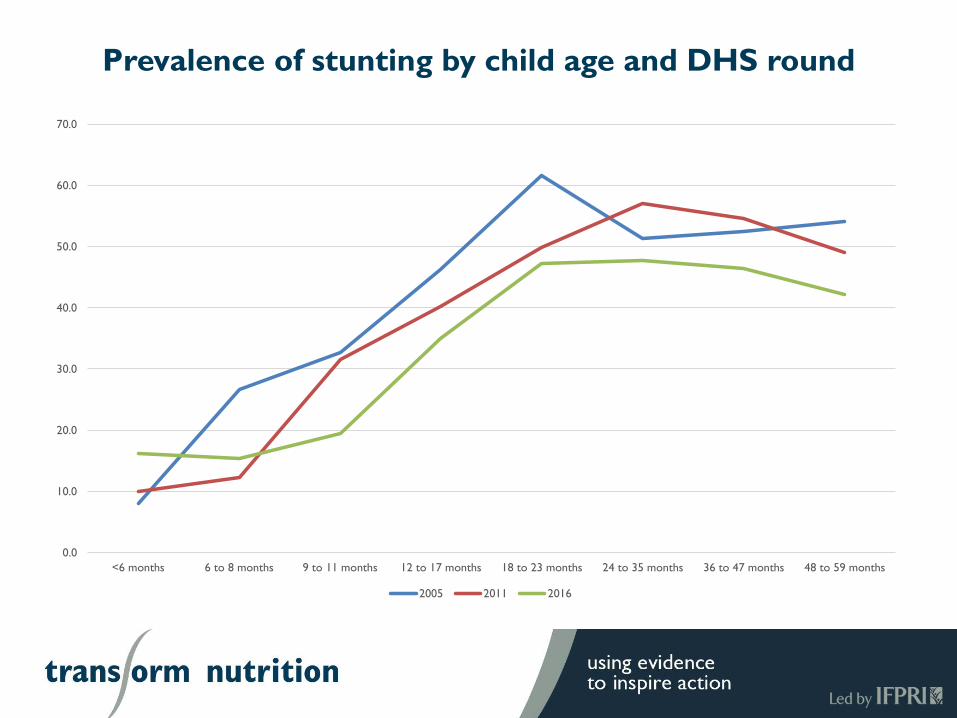
Prevalence of stunting by child age and DHS round
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
<6 months 6 to 8 months 9 to 11 months 12 to 17 months 18 to 23 months 24 to 35 months 36 to 47 months 48 to 59 months
2005 2011 2016

Change in prevalence of stunting across age groups and
DHS round
% stunted 2005
6-8m 26.6
18 – 23m 61.7
Increase 35.1
% stunted 2011
6-8m 12.2
18 – 23m 49.9
Increase 37.7
% stunted 2016
6-8m 15.3
18 – 23m 47.2
Increase 31.9

From retrospect to prospect:Addressing chronic undernutrition in children 6-23m
• So why does stunting continue to rise so dramatically between ages 6 and 23 months in a country where agricultural production has risen by 8.5 percent per year for the last 10 years?
• Some of this is related to delays in the introduction of complementary foods, some is related to the lack of caloric density in foods given to infants and some may be related to insufficient meal frequency
• Further, children in this age group consume a remarkably monotonous diet

Addressing chronic undernutrition in children 6-23m:Diet quality
• Why might this lack of diversity matter?– Children consuming more diverse diets consume more calories
And/or
– There is something specifically important about the foods found in a diverse diet
• For example, cow’s milk (in addition to being an important source of animal-source protein, amino acids, calcium, iron, and vitamin B-12) stimulates the secretion of insulin-like growth factor I (IGF-I), the hormone that stimulates bone and tissue growth

Addressing chronic undernutrition in children 6-23m:Diet quality
• Rapid advances are occurring in metabolomics – the study of small molecule chemicals that are the consequence of metabolic processes.
• For example, recent work has shown that when essential amino acids are absent from diets:– The body represses protein and lipid synthesis and cellular growth
– Bone growth is restricted
• Essential amino acids cannot be synthesized from scratch within the human body; these must be obtained via diet. The best sources are animal sourced foods (meat, poultry, fish, eggs). Plant sources also contain these, but typically in much lower concentrations.
• Biochemical analysis by Semba et al (2016a) of serum blood samples in Malawi showed that stunted children lacked all essential amino acids.
Addressing chronic undernutrition in children 6-23m:Diet quality
• Metabolomic work has also focused attention on choline, an essential nutrient
• Choline is needed for the synthesis of phosphatidycholines; this synthesis is needed for bone formation and cell membrane formation.
• Choline also appears to play a role in neurotransmitter synthesis which plays a role in the transmission of chemicals across synapses in the brain
• Eggs are an excellent source of choline. Flesh foods (beef, chicken) are another source as are groundnuts, though the latter contain much less choline than eggs
• Semba (2016b) find that in Malawi, children with low serum choline concentrations are more likely to have experienced linear growth failure

Addressing chronic undernutrition in children 6-23m:Diet quality
• What do diets of Ethiopian children look like?
• Most recent example comes from 2016 survey of Highland households where the PSNP operates. In this sample, 47 percent of children age 6-23m are stunted. Looking at their diets:– 19.5% consume dairy products
– 1.3% consume flesh foods (meat, poultry, fish)
– 3.5% consume eggs
– (Earlier DHS data show similar results)
• With the important caveat that I am describing associations in these data:– Recent advances in nutritional sciences tell us that animal source foods (dairy, meat,
chicken, fish, eggs) contain nutrients critical for child growth
– The vast majority of Ethiopian children aged 6-23m do not consume these foods
– And we continue to observe high prevalences of stunting in this age group
Improving diet quality in children 6-23m (1)The role of knowledge and beliefs
• One reason why diet quality is poor is that mothers may be unaware of the nutritional benefits of these foods or may even perceive them to be harmful– For example (Han, 2016 unpublished) finds in focus group discussions that mothers do
not feed children 6-12m eggs or meat because they are perceived to cause digestive problems
• So is poor dietary quality a consequence of poor nutrition knowledge?
• Hirvonen et al (2016) show that a 1SD ↑ in mother’s nutrition knowledge increases the number of food groups children <60m consume by 0.85 even after controlling for household wealth and the endogeneity of nutrition knowledge.
• But the Hirvonen et al results disappear for households most remote from food markets
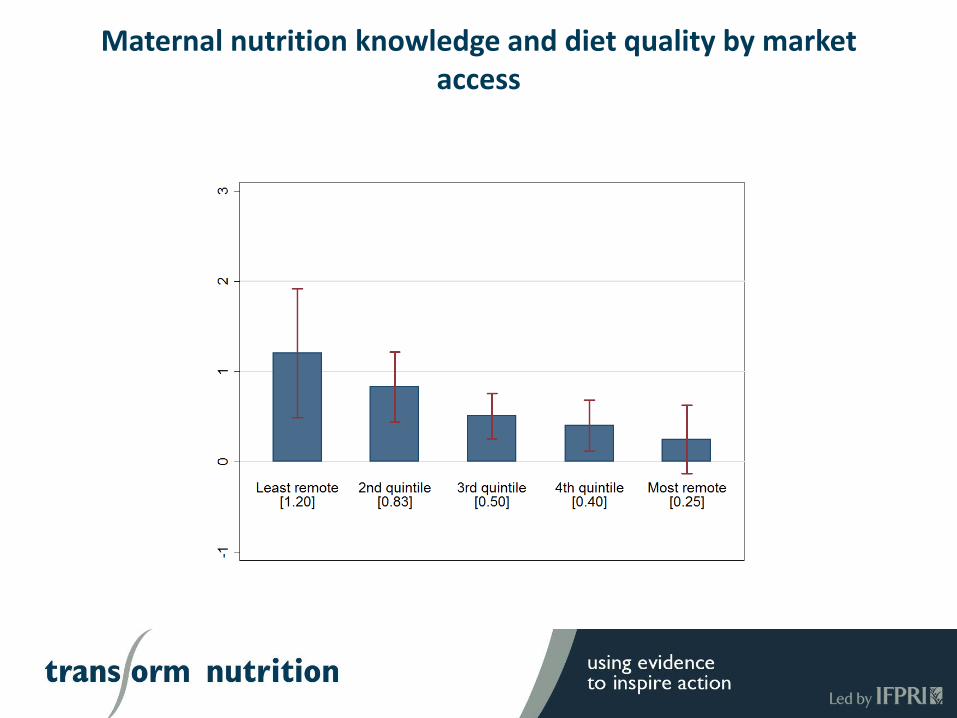
Maternal nutrition knowledge and diet quality by market access
Improving diet quality in children 6-23m (2)The role of income
• A second reason why diet quality is poor is that many households may be too poor to afford the foods needed for a high quality diet
• Analysis of DHS data from Ethiopia shows that growth in asset ownership is associated with reductions in stunting
• But … first results from the 2016 Ethiopian DHS show that:– 27% of children in the highest wealth quintile are stunted
• Analysis of earlier phase of PSNP (Hoddinott, Berhane and Kumar, 2016) showed that PSNP participation had:– No impact on stunting
– No impact on diet quality
Improving diet quality in children 6-23m (3)The role of home production
• Using FtF data, Hirvonen and Hoddinott (forthcoming) show that a one food group ↑ in household food production leads to a 0.6 ↑ in the number of food groups consumed by children 6-59m
• Using AGP baseline data, Hoddinott, Headey and Dereje (2015) find that after controlling for household wealth and income, ownership of dairy cows reduces the prevalence of stunting in children 12-24m by 9.1 percentage points
• Hirvonen and Headey (2016) find that ownership of poultry is associated with an increase in HAZ of children 0-59m by 0.29
• So does the solution to diet quality lie in home production?
Improving diet quality in children 6-23m (3)The role of home production
• The Hoddinott et al “milk” results disappears for children residing in households where there is a local food market
• The Hirvonen and Hoddinott results disappear for households living less than 3km from a food market
• Hirvonen and Headey’s beneficial association of poultry and HAZ is completely offset when poultry are kept in the house
• Unpublished preliminary work by Han, Kim and Park replicating the “milk” results in Bangladesh find that ownership of livestock (primarily dairy cattle) increases HAZ but nearly all of this beneficial effect is offset when cattle are allowed to roam within the homestead
Chronic undernutrition and exposure to animal fecal matter
• The Hirvonen and Headey and the Han et al results are consistent with recent work on environmental enteropathy, also known as tropical enteropathy or Environmental Enteric Dysfunction (EED), a subclinical disorder believed to result from frequent intestinal infections.
• The basic idea is that in resource-poor settings, very young children are continually exposed to bacterial infections, particularly through contact (or consumption) with animal (or human) fecal material in places where they eat or play. Often, the acute symptoms are minimal.
• However, this means that on an ongoing basis, the child’s body is diverting energy to fit off infection.
• The longer term consequence of this are a series of changes in the child’s intestinal system. These changes result in poor absorption of energy and micronutrients. Reduced energy absorption reduces growth.
21
Reducing chronic undernutrition in Ethiopia:
Summary and Prospects
• Some caveats before we begin
• I have not talked about– Other dimensions of undernutrition such as wasting and micro-nutrient deficiencies
– Other important nutrition behaviors including the importance of maternal nutrition and breastfeeding
– Programmatic interventions including those undertaken by the Government of Ethiopia (for example, the role of Health Extension Workers) and its development partners (for example: Alive and Thrive; and ENGINE)
• These are all clearly important; there simply is not enough time today to discuss them all
• In some aspects of the material discussed today, I have talked about causal relations but in others, the relationships described are associational
Reducing chronic undernutrition in Ethiopia:
Summary and Prospects
• Reducing chronic undernutrition has both intrinsic and instrumental value. In the long run, given the links from:– Chronic undernutrition to neurological development
– Neurological development to schooling
– Schooling to income
• Reducing chronic undernutrition is a prerequisite for sustainable poverty reduction
• Ethiopia has made impressive progress in reducing chronic undernutrition; this progress is amongst the fastest in the developing world
Reducing chronic undernutrition in Ethiopia:
Summary and Prospects
• That said, the rate of change in chronic undernutrition is slow when compared to country income growth, agricultural production and reductions in child mortality
• The rate of increase in chronic undernutrition from ages 6-8m (when complementary foods are introduced) to 18-23m (when neurological development is largely complete) has barely changed since 2005
• Growing body of work in nutritional sciences suggests that animal source foods (dairy; flesh foods; eggs) are necessary for linear growth
• But in Ethiopia, children 6-23m almost never consume flesh foods or eggs and even milk consumption is low

Reducing chronic undernutrition in Ethiopia:
Summary and Prospects
• It is tempting to believe that “single solutions” can reduce chronic undernutrition, especially in children 6-23m. But this would seem to be wishful thinking
• Improving knowledge of good nutritional practices will improve diet quality:– But not if food markets are inaccessible
• Increasing incomes will solve the problem of undernutrition– But not always
• Let’s give everyone a cow! Or some chickens!– But if these animals roam free, these possible benefits will not materialize
– And market access may act as a substitute for these
Reducing chronic undernutrition in Ethiopia:
Summary and Prospects
• Instead, prospects for reducing chronic undernutrition may well hinge on the interplay between:
– Improving nutrition knowledge
– Having the resources income to acquire diverse foods, especially animal source foods
– Enhancing access to diverse foods through markets or, where it makes economic and agro-ecological sense, through own production
– Increased attention to both human and animal hygiene

ReferencesCordero, M., et al, 1993. “Dentric development in neocortex of infants with early postnatal life undernutrition”, Pediatric Neurology 9(6): 457-464.
Headey, D., J. Hoddinott and S. Park, 2016. “Accounting for nutritional changes in six success stories: A regression-decomposition approach”, mimeo.
Headey, D. and K. Hirvonen, 2016. “Is exposure to poultry harmful to child nutrition? An observational analysis for Ethiopia”, PLoSOne 11(8) e0160590
Hoddinott, J., G. Berhane and N. Kumar, 2016. “The impact of Ethiopia’s Productive Safety Net Programmme on the Nutritional Status of Children: 2008 – 2012”, mimeo.
Hoddinott, J., D. Headey, and M. Dereje, 2015. “Cows, missing milk markets and nutrition in rural Ethiopia,” Journal of Development Studies, 51(8): 958-975.
Hoddinott, J., J. Maluccio, J. Behrman, R. Martorell, Paul Melgar, Agnes R. Quisumbing, Manuel Ramirez-Zea, Aryeh D. Stein, and Kathryn M. Yount, 2013. “Adult consequences of growth failure in early childhood,” American Journal of Clinical Nutrition, 98: 1170-1178.
Hirvonen, K. and J. Hoddinott, forthcoming “Agricultural production and children’s diets: Evidence from rural Ethiopia”, Agricultural Economics.
Hirvonen, K., J. Hoddinott, B. Minten and D. Stifel, 2016. “Children’s diets, nutrition knowledge, and access to markets", mimeo.
Semba, R., et al, 2016a. “Child stunting is associated with low circulating amino acids”, EBioMedicine 6: 246-252.
Semba. R., et al, 2016b. “The association of serum choline with linear growth failure in young children from rural Malawi”, American Journal of Clinical Nutrition 104: 191-7.