Reducing Avoidable Emergency Department Utilization€¦ · Raven, et al. (2013). Annals of...
59
Reducing Avoidable Emergency Department Utilization Reforming States Group – October 15, 2015
Transcript of Reducing Avoidable Emergency Department Utilization€¦ · Raven, et al. (2013). Annals of...

Reducing Avoidable Emergency Department Utilization
Reforming States Group – October 15, 2015

First things first… • Conflicts or disclosures: None • Thanks and acknowledgements • A brief follow-up from RSG 2014
Presenter
Presentation Notes
No relevant financial disclosures Thanks to Chris and Trina for the invitation. Acknowledge Bob Lowe. Acknowledge Mark and Martha So you solved HCV treatment, right? -Major driver of the VA budget shortfall this year -Evidence in real world populations has not been as robust -This has been the tip of the iceberg for other high cost drugs – oncology drugs, MS drugs, biologics, etc… -One of the major drivers of a return to more historic levels of annual growth in healthcare costs

Case 1 – Medication mix-up

Case 2 – Swedish light bulbs

The scope of the problem
Is avoidable ED use a major problem?

Background • About 10-15% of all ED visits are for non-urgent or
primary care treatable issues • Medicaid beneficiaries are more likely to use the ED

Increasing ED Use • EDs are now the main source of hospital admissions
– About 70% of non-elective admissions are through the ED
• Non-elective admissions from clinics dropped by 25% between 2003 and 2009

A snapshot of ED use in the VA Usage category (visits/year)
# of patients (%) # of visits (%)
1 493,391 (53) 493,391 (24.5)
2-4 356,258 (38.3) 910,195 (45.3)
5-10 70,741 (7.6) 447,875 (22.3)
11-25 9,705 (1.0) 137,152 (6.8)
>25 617 (0.07) 21,669 (1.1)
Raven, et al. (2013). Annals of Emergency Medicine. 62(2):151-159

Measuring avoidable ED use • Identifying avoidable ED visits is challenging
– ED discharge diagnoses that are “non-emergent” or “primary care treatable”
– Various algorithms are promoted – Poor correlation between the patient’s complaint and the
seriousness of the issue or ultimate need for admission • A patient with chest pain could have acid reflux or could be
having a heart attack
Raven, et al. (2013). JAMA. 309(11):1145-1153.

Area of interest and innovation • CMS Diversion Grant Program, 2008-2012
– $50 million to support 29 projects in 20 states • Increased primary care capacity • ED to primary care linkages • Programs targeting superutilizers
– 12 states (16 programs) submitted brief results – Effect and sustainability of the programs was mixed

Causes of avoidable ED utilization
Why do people go to the ED anyway?

Access
Gindi, et al. (2014). NCHS Data Brief. No. 160

Access
Gindi, et al. (2014). NCHS Data Brief. No. 160

Patient factors Characteristics Odds ratio for 11-25 visits Odds ratio for >25 visits
Homelessness 4.43 6.60
Schizophrenia 3.72 6.86
Opioid prescription 5.06 5.08
Substance abuse 2.85 2.97
Raven, et al. (2013). Annals of Emergency Medicine. 62(2):151-159

Patient factors Patient Subgroup Number % of all superutilizers
Terminal cancer patients
11 0.7%
Emergency dialysis patients
30 1.8%
Orthopedic surgery patients
60 3.6%
Trauma patients 195 11.6%
Patients with serious mental health diagnosis
685 40.7%
Patients with multiple chronic conditions
701 41.6%
Johnson, et al. (2015). Health Affairs. 34(8):1312-1319.

Practice culture and patterns • Changing relationships between PCPs, EDs, and
hospitalists • Productivity demands for PCPs make it hard to
accommodate acutely ill patients – These patients are often referred to the ED – Fewer direct admissions from outpatient clinics – Ease of complex diagnostic work-ups
Morganti, et al. (2013). RAND Research Report.

Impacts of avoidable ED utilization
Does overuse of the ED matter?

Overcrowding • ED use grew at twice the rate of population growth from
2001 to 2008 • 198,000 fewer hospital beds during the same period • This has led to overcrowding and boarding
– Associated with poorer patient outcomes

Lost opportunity for care coordination • Poor coordination with PCPs and erratic follow-up • Preventive care falls through the cracks • Medication errors

Perspectives on ED “cost”
Diagnosis Mean total ED bill Mean total PC office bill
Otitis media $410 $157
Acute pharyngitis $562 $152
Urinary tract infection $776 $189
Mehrotra, et al. (2009). Annals of Internal Medicine. 151(5): 321-328.

Perspectives on ED “cost”
Caldwell, et al. (2013). PloS One. 8(2): e55491.

Perspectives on ED “cost”
Inpatient 29%
Office-based provider
24%
Prescriptions 20%
Hospital outpatient
10%
Dental 7%
Home health 4%
ED 4%
Other 2%
Medical Expenditure Panel Survey, 2009

Perspectives on ED “cost”
Alhassani, et al. (2012). New England Journal of Medicine. 366(4): 289-291.

Perspectives on ED “cost” “Put simply, when an ED is fully staffed to manage 2 major traumas, a myocardial infarction and a septic neonate at the same time, it does not take many additional resources to evaluate a sprained ankle or a headache.”
Lowe, et al. (2012). Annals of Emergency Medicine. 58(3):235-238.

Proposed solutions What is being tried to reduce avoidable ED use?

CMS Guidance • Center for Medicaid and CHIP Services (CMCS) Bulletin on
reducing non-urgent use (July 2014) – Three proposed strategies:
• Expanded primary care access • Programs targeting super-utilizers • Programs addressing co-morbid mental health and substance
abuse issues – Differential payments and cost-sharing
Presenter
Presentation Notes
This CMCS on reducing non-urgent, released in January 2014, offers three strategies to reduce avoidable ED utilization before providing guidance on regulatory issues relevant to cost-sharing programs for non-urgent ED use. The first proposed strategy is to broaden access to more appropriate care settings through establishment of medical and health homes or through alternative primary care sites including urgent care and retail clinics. CMCS highlights the Community Care of North Carolina program that focused on primary care medical homes for patients with asthma and was able to show a 16% reduction in ED visits. The second proposed strategy is to focus on ED super-utilizers and refers to the separate CMCS bulletin on super-utilizer programs that we will discuss next. The third proposed strategy involves targeting people with comorbid mental health and substance abuse disorders. CMCS highlights programs in Indiana and Michigan that provide integrated medical homes for people with substance abuse, as well as housing and case management programs in Illinois, Pennsylvania, and Maryland that have shown reductions in ED use of 20% to 59%. States are also empowered to implement differential payments or cost-sharing arrangements for non-emergency use of the ED. CMCS acknowledges the difficulty in identifying non-urgent ED utilization and notes that various algorithms for making these determinations rarely agree. Despite this, the bulletin emphasizes that in order to institute differential payments or cost-sharing schemes, states “must establish a reasonable clinically-based method to distinguish emergency from non-emergency visits.” States must also show that there is sufficient access to services outside the ED before these programs can be implemented.

CMS Guidance • CMCS Bulletin on super-utilizer programs
– Offers support by way of: • Enhanced federal match for MMIS redesign or health
information exchanges • Assistance with utilization review and data analysis • Temporary enhanced match for Medicaid health homes • Shared savings methodologies for integrated care and case
management – Super-utilizer program case studies
• OR, NC, MN, ME, MI, VT

Studied interventions • Patient education programs • Increased primary care capacity • Pre-hospital diversion • Managed care: Capitation and gatekeeping • Patient financial incentives

Studied Interventions • Intensive case management programs
– Care coordination by social workers – Crisis intervention – Supportive therapy – Assistance with benefits applications – Substance abuse treatment – Supportive housing – “Assertive community outreach”


Discussion
1. Is this issue serious enough to warrant attention from policymakers?
2. What kind of evidence would you want that these programs work before moving forward?

Systematic reviews of the evidence
What does the evidence say about these programs?

Systematic Review – Morgan 2012 • Non-ED interventions to reduce ED visits • 5 RCTs, 34 observational studies • Mostly very low quality because of design • Mix of public and private insurance • Some studies outside the U.S.
Presenter
Presentation Notes
Now we’ll turn our attention to the results programs to reduce avoidable ED use that have been summarized in the academic literature. We will quickly cover 3 systematic reviews. The first, Morgan 2012, is a systematic review of non-ED interventions to reduce ED utilization. The authors identified five randomized controlled trials (RCTs) and 34 observational studies that met inclusion criteria. The studies were grouped and analyzed by the type of intervention: patient education, expanded non-ED capacity, pre-hospital diversion, managed care, and financial incentives. The majority of the studies (including all 34 observational studies) were judged to be very low quality, and the remaining randomized trials were low to moderate quality. General limitations include observational studies occurring during periods of substantial system-wide changes, absence of risk adjustment in most studies, and indirectness due to settings outside the United States and non-Medicaid populations. Overall, the results were mixed, but we will examine these by the type of intervention used.

Systematic Review – Morgan 2012 • How many studies? • What outcomes were measured/reported? • Did the studies reach similar conclusions? • Was the estimate of the effect narrow or wide? • What’s your overall assessment of the evidence?

Systematic Review – Patient Education • Patient education interventions (5 studies)
– 2 studies showed 20-80% decrease in ED use – 3 studies with non-significant decreases
Presenter
Presentation Notes
Five studies examined patient education programs involving informational handouts or face-to-face education and included both adults and children. Two of the programs reported significant reductions in ED use ranging from 21% to 80%. The remaining three programs reported non-significant reductions in ED use. Notably, one of the studies also found a slight decrease in non-ED use. None of the studies reporting on health outcomes found significant adverse events.

Systematic Review – Expanded access • Expanded non-ED capacity interventions (10 studies)
– Mix of new community clinics and increased access at existing clinics
– 4 studies showed decreased ED use (9% to 54%) – 5 studies found no difference – 1 study found a 21% increase in ED use – Most found significant increase in non-ED care – 2 reported on total cost with mixed results (-16% to +20%)
Presenter
Presentation Notes
Ten studies examined the effects of expanded capacity in non-ED settings. Three involved new community clinics, and seven involved increased access through existing primary care practices. Four studies showed significant decreases in ED-use ranging from 9% to 54%, five studies found no significant effects, and one found an increase in ED use of 21%. As expected, most of these studies found substantial increases in the use of non-ED care. The effect of these interventions on total cost were reported in two studies with conflicting results ranging from increased costs of up to 20% to decreased costs of up to 16%.

Systematic Review – Pre-hospital diversion
• Pre-hospital diversion interventions (2 studies) – 1 study (U.S.-based) offered ~1,000 low acuity
patients care at home or in the PC office – 7% decrease in ED use compared with matched
historical controls
Presenter
Presentation Notes
Two studies examined pre-hospital diversion by emergency medical services (EMS), but only one of these studies was done in the United States. In the U.S. study, 1,016 low acuity patients were offered care in their homes or at a primary care clinic in place of transport to the ED. This cohort was then compared to matched historical control group. Overall, there was a 7% reduction in ED use with the intervention and there was a corresponding increase in care provided in clinic or at home.

Systematic Review – Managed care • Managed care interventions (12 studies)
– 6 studies on effects of capitation, 5 studies on PC gatekeeping, 1 hybrid study
– 9 studies found decreases in ED use of 1% to 46% – 3 studies found no difference in ED use – 2 reported total cost decreases with capitation – Better designed trials showed more modest effects
Presenter
Presentation Notes
Twelve studies examined the effects of managed care interventions on ED utilization. Of these, six examined the effects of capitated payment models, while five studied primary care gatekeeping. The final study employed a hybrid approach. The majority of studies (9 of 12), including several that included Medicaid recipients, found that capitation and gatekeeping reduced ED utilization by 1% to 46%. The remaining three studies showed either no difference or mixed results. Two of the studies on capitation reported cost outcomes with both demonstrating a reduction in total cost. It should be noted that the more rigorous study designs showed more modest reductions or no difference in ED utilization.

Systematic Review – Financial incentives
• Financial incentive interventions (10 studies) – Mix of co-payments, co-insurance, or high-
deductibles – 9 studies found decreases in ED use of 3% to 50% – 1 study found increased ED use of 34% – 3 reported mixed cost outcomes
Presenter
Presentation Notes
Ten studies examined the effects of patient financial incentives on ED utilization. All of these studies were done in the United States, and half of them involved Medicaid patients. The interventions were either institution of copayments or coinsurance or the implementation of high-deductibles. Nine of the 10 studies found reductions in ED use ranging from 3% to 50%, while the remaining study actually found an increase in ED use of 34%. The effects on total cost were mixed in the three studies that reported that outcome.

Systematic Review – Althaus 2011 • Programs targeting super-utilizers • 3 RCTs, 8 before-and-after studies • Low-to-moderate quality evidence • About half conducted in the U.S. • Mostly case management of varying intensity • Relatively short follow-up periods (5 to 24 months)
Presenter
Presentation Notes
The second SR by Althaus and colleagues in 2011 looked at programs specifically targeted at ED superutilizers. The authors identified three RCTs and eight before-and-after studies. Meta-analysis was not done because of differences in the study populations and interventions. Five of the studies were done in the United States. The overall quality of the included studies was judged to be low to moderate. Most of the studies examined case management interventions of varying intensity. The most comprehensive case management approaches included assignment to a case manager, care coordination with outpatient providers, crisis intervention, supportive therapy, assistance obtaining housing, referral to substance abuse treatment, and “assertive community outreach.”

Systematic Review – Althaus 2011 • 7 programs showed decreases in ED use • 3 programs showed no difference • 1 program showed an increase in ED use • Effect on total cost (from perspective of the hospital) was mixed in 3
studies – 1 RCT reporting on cost found better social and clinical
outcomes at the same cost as “usual care” • Other benefits: decreased substance abuse and homelessness,
increased primary care engagement
Presenter
Presentation Notes
Overall, seven of the studies found decreases in ED utilization, three found no difference, and one found an increase in ED use. The effects on total costs (from the perspective of the hospital) were also mixed, although the one RCT that reported on cost concluded that, because the case management intervention resulted in better social and clinical outcomes at the same cost, these interventions are more cost-effective than usual care. Reductions in substance abuse and homelessness were noted in several of the studies. Outpatient visits and engagement with primary care increased in the intervention groups in the studies that reported these outcomes.

Discussion
1. Is this evidence adequate to support wider adoption of these programs?
2. What concerns do you have about the evidence, and what other outcomes would be of interest?

Risk of bias in study design • Higher quality studies less likely to show effects • Outcomes are often preliminary (6 or 12 month effects) • Publication bias

Risk of before-and-after studies • Observed differences in a group after the intervention
could be due to: – Other changes occurring simultaneously – Natural history of the problem
Johnson, et al. (2015). Health Affairs. 34(8):1312-1319.

Risk of before-and-after studies • The natural history of ED use may also vary by
enrollment time

Indirectness • Caution with multicomponent interventions • Broader use of highly targeted interventions • Lack of head-to-head comparisons (choosing among
multiple policy options)

Imprecision • Wide estimates of the effects in the studies • “Discounting” for effects in the real world

Unintended outcomes • Co-pays in Oregon Medicaid (OHP vs OHP Plus)
Service type Probability of service use
Expenditure per user
Expenditure per person
ED -8% +8% -2%
Inpatient +27% -6% +20
Overall +2%
Wallace, et al. (2008). Health Services Research. 43(2):1312-1319.

Dealing with insufficient evidence
The evidence isn’t clear – how do we move forward?

An opportunity • When the evidence is lacking, policy innovation can be
even more important – Must be done with careful plans for evaluation – Focus on outcomes that matter to you as
policymakers – Academic and agency collaborations

Washington ER is for Emergencies • Collaboration with hospitals and providers • Seven best practices:
– Health information exchange – Patient education – Identification of frequent users – Care plans and primary care follow-up – Strict narcotic guidelines – Participation in prescription drug monitoring – Feedback to hospitals on performance

Washington ER is for Emergencies • 10% reduction in ED use with a 23% reduction for the
most frequent users • Overall cost savings of $10 million in fee-for-service and
$23 million in managed care

Hennepin County Ambulatory ICU • Coordinated care model for ~300 highest-utilizers
– Primary care, nurses, pharmacists, social worker, community health workers, behaviorists, substance use treatment
– Major focus on establishing stable housing

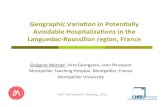
Hennepin County Ambulatory ICU

Hennepin County Ambulatory ICU
-50%
0%
50%
100%
150%
200%
Outpatientservices
EMS services ED services Inpatientadmissions
Totoal cost ofcare

Emerging data and ideas
What’s on the horizon?

Effect of primary care medical homes • Medicare beneficiaries in PCMHs had lower rates of ED
use than those in non-PCMHs • A pilot PCMH and shared saving program in PA reduced
ED (and inpatient) utilization and improved quality • A multipayer PCMH pilot in CO reduced ED use by 8-
10%
Pines, et al. (2015). Annals of Emergency Medicine. 65(6):652-660 Friedberg, et al. (2015). JAMA Internal Medicine. 175(8):1362-1368 Rosenthal, et al. (2015). Journal of General Internal Medicine. Pre-pub [Oct 8, 2015]

Cold-spotting? • Seeks to understand and address community factors
that lead to avoidable healthcare use
Westfall, J.M. (2013). Journal of the American Board of Family Medicine. 26(3):228-230

Questions and Discussion Contact: [email protected]