
Redesigning studies and endpoints with...
41
Redesigning studies and endpoints with immuno-oncology Changes and challenges in early phase trial endpoints Ruth Plummer Professor of Experimental Cancer Medicine 1
Transcript of Redesigning studies and endpoints with...

Redesigning studies and endpoints with immuno-oncology
Changes and challenges in early phase
trial endpointsRuth Plummer
Professor of Experimental Cancer Medicine
1

Disclosures
• In the last 2 years I have received Honoria for attending advisory boards from Pierre Faber, Genmab, Bayer, Octimet, Clovis Oncology, Novartis, KarusTherapeutics, Biosceptre, BMS, Cybrexa, Ellipses, CV6 therapeutics and Sanofi Aventis.
• I have been paid for delivery of educational talks or chairing educational meetings by AstraZeneca, Novartis, Bayer, Tesaro and BMS.
• I have received funds to support attendance at conferences from BMS and MSD.• I have received a discretionary payment from my employing institution in
recognition of the royalties relating to rucaparib
• My Institution has received research costs to support a PhD studentship from AstraZeneca and costs for multiple clinical trials
2
Overview
• Immunotherapy in oncology– How it works
– Agents in development
• Challenges for trial endpoints– Allying the standard model does not work
– Time to response
– Emergence of toxicity
– Combination therapy
3
IMMUNOTHERAPY IN ONCOLOGY
4

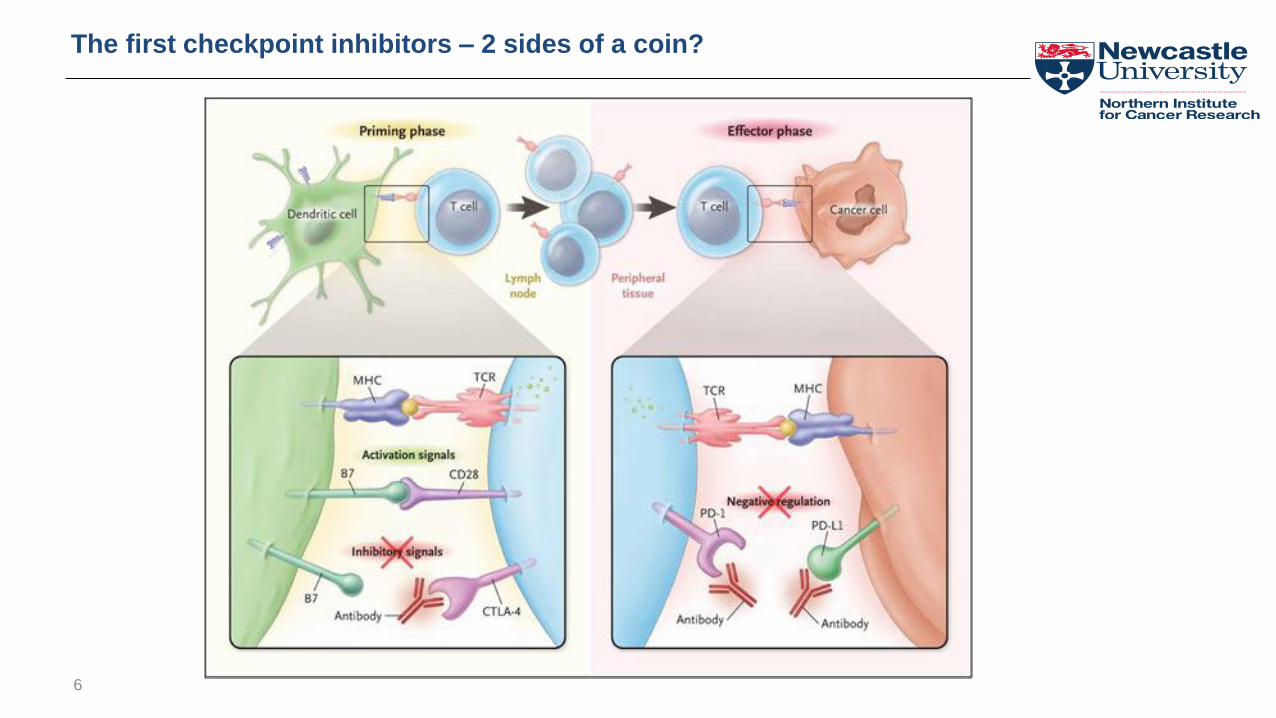
The first checkpoint inhibitors – 2 sides of a coin?
6

7


A REVOLUTION IS UNDERWAY: 2,004 IO AGENTS IN DEVELOPMENT
940 AGENTS ARE IN CLINICAL STAGES, AND 1,064 IN PRECLINICAL
Annals of Oncology, Dec 2017Tang, Shalabi, Hubbard-Lucey

This is a revolution in cancer treatment
Melanoma – the problem when I started as a consultant
10
0
1
2
3
4
197
1
197
4
197
7
198
0
198
3
198
6
198
9
199
2
199
5
199
8
200
1
200
4
200
7
Ra
te p
er
10
0,0
00
po
pu
lati
on
Year of death
males females persons
Age-standardised (European) mortality rates, malignant melanoma,

Changing face of melanoma treatment
11
Targeted therapies
Immunotherapy
Response rates!
Duration of response –“it’s all about the tail on the curve” – James Larkin
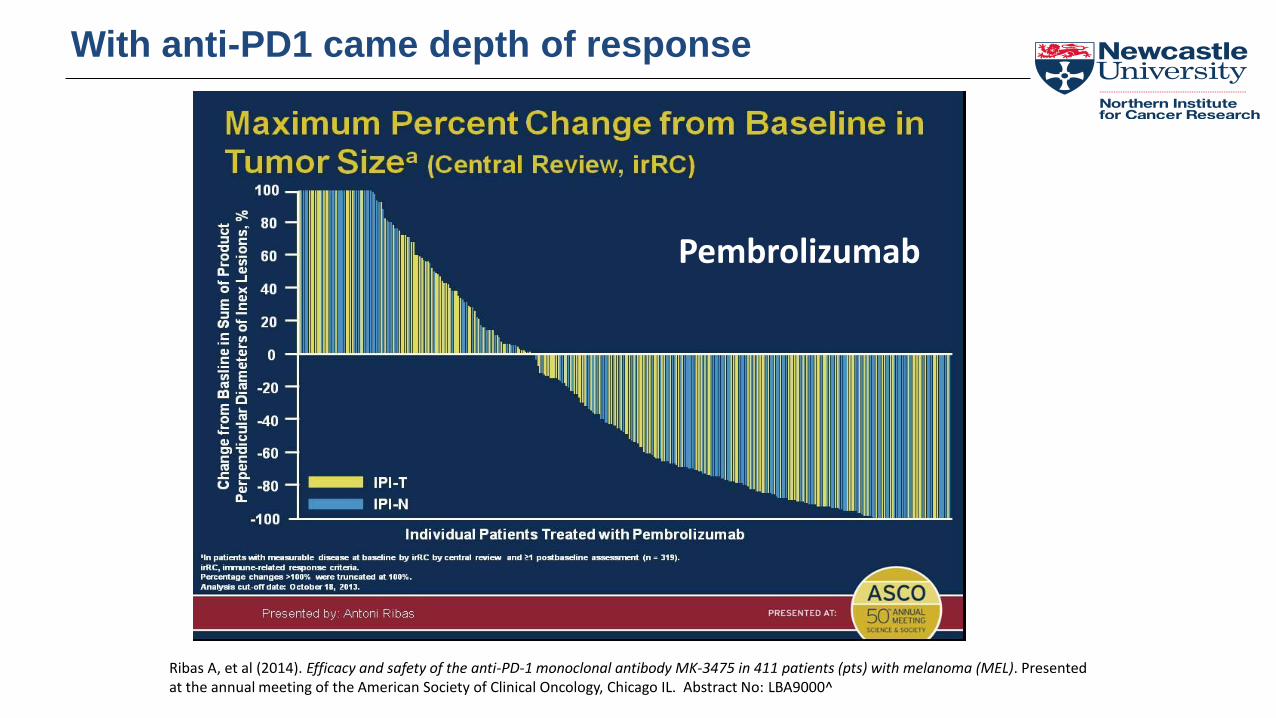
Pembrolizumab
Ribas A, et al (2014). Efficacy and safety of the anti-PD-1 monoclonal antibody MK-3475 in 411 patients (pts) with melanoma (MEL). Presentedat the annual meeting of the American Society of Clinical Oncology, Chicago IL. Abstract No: LBA9000^
With anti-PD1 came depth of response

Slide 16
Ribas A, et al (2014). Efficacy and safety of the anti-PD-1 monoclonal antibody MK-3475 in 411 patients (pts) with melanoma (MEL). Presented
at the annual meeting of the American Society of Clinical Oncology, Chicago IL. Abstract No: LBA9000^

14
CHECKMATE-067 pivotal study design
Wolchok et al (2016). Updated Results From a Phase III Trial of Nivolumab Combined With Ipilimumab in Treatment-naïve Patients With Advanced Melanoma (Checkmate 067). Presented at the annual meeting of the American Society of Clinical Oncology. Chicago IL. AbstractNumber: 9505

Most recent overall survival data
15
Updated 4 year OS data Hodi et al Lancet Oncol 2018 19:1480-925 year data presented at ESMO 2019 and median not yet reached in combination arm
“It’s all about the tail on the curve”

Brahmer et al N Engl J Med. 2015 May 31.
CheckMate-017; Nivolumab vs Docetaxel in Squamous NSCLC

Overall Survival by PD-L1 Expression in Checkmate 057 (Non Squamous NSCLC)
mOS (mos)
Nivo 17.7
Doc 9.0
mOS (mos)
Nivo 19.4
Doc 8.1
mOS (mos)
Nivo 19.9
Doc 8.0
mOS (mos)
Nivo 10.5
Doc 10.1
mOS (mos)
Nivo 9.8
Doc 10.1
mOS (mos)
Nivo 9.9
Doc 10.3
≥1% PD-L1 expression level
Time (mos)
100
90
80
70
60
50
40
30
10
0
20
3024211815129630 27
OS
(%)
NivoDoc
HR (95% CI) = 0.58 (0.43, 0.79)
≥5% PD-L1 expression level100
90
80
70
60
50
40
30
10
0
20
3024211815129630 27
Time (mos)
HR (95% CI) = 0.43 (0.30, 0.62)
≥10% PD-L1 expression level100
90
80
70
60
50
40
30
10
0
20
3024211815129630 27
Time (mos)
HR (95% CI) = 0.40 (0.27, 0.58)
<1% PD-L1 expression level100
90
80
70
60
50
40
30
10
0
20
3024211815129630 27
Time (mos)
OS
(%)
NivoDoc
<10% PD-L1 expression level100
90
80
70
60
50
40
30
10
0
20
3024211815129630 27
Time (mos)
<5% PD-L1 expression level100
90
80
70
60
50
40
30
10
0
20
3024211815129630 27
Time (mos)
HR (95% CI) = 0.87 (0.63, 1.19) HR (95% CI) = 0.96 (0.73, 1.27) HR (95% CI) = 0.96 (0.74, 1.25)
Based on a July 2, 2015 DBL; symbols represent censored observations.17
"Copyright permission has been obtained for this figure. From The New England Journal of Medicine, Borghaei H, et al., Nivolumab versus Docetaxel in Advanced Nonsquamous Non–Small-Cell Lung Cancer [Epub ahead of print; DOI: 10.1056/NEJMoa1507643]. Copyright © 2015 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society."

Trial design changing the face of phase I
18Total recruitment to this “phase I” stands at >1700 patients currently

CLINICAL TRIAL LANDSCAPE FOR PD1/PDL1 SEPTEMBER 2018 – 2250 ACTIVE TRIALS COMPARED TO 1502 IN SEPTEMBER 2017
Nat Rev Drug Disc. 2018Yu, Hubbard-Lucey, Tang

NUMBER OF TRIALS AND NUMBER OF PATIENTS REQUIRED TO COMPLETE THEM IS OUTSTRIPPING CAPACITY
Annals of Oncology, Dec 2017Tang, Shalabi, Hubbard-Lucey
Nat Rev Drug Disc. 2018Yu, Hubbard-Lucey, Tang

CHALLENGES FOR TRIAL ENDPOINTS
Applying the standard model does not work
21

Phase I and safety
• Dosing– Majority of clinically approved agents are monoclonal
antibodies or biological/vaccines– Dose response and dose-toxicity relationships are not direct
or dose proportional• Recent change from weight based to flat dosing pembro and nivo
post approval• Change in dose frequency post approval• Change in posology without clinical data
– Preclinical models have struggled to predict toxicity– Most phase I studies have used 3+3 design
• Issues with late emergence of toxicity• MTD unlikely to be the appropriate dose• Receptor occupancy means biological effect can continue long after
dose
– Studies with multiple expanded cohorts have lacked statistical design for safety/futility
22

Biomarkers and patient selection
• PDL1 expression appears to be predictive of response (but not good enough)
– Responses seen in PDL1 negative melanoma
– Various assays and no standardisation yet
– Tumour or TME expression?
• Ideal biomarker appears to be in tumour
– Challenges of fresh biopsy
– Effects of previous treatment if archival
23

CHALLENGES FOR TRIAL ENDPOINTS
Time to response
24

Slide 16
Ribas A, et al (2014). Efficacy and safety of the anti-PD-1 monoclonal antibody MK-3475 in 411 patients (pts) with melanoma (MEL). Presented
at the annual meeting of the American Society of Clinical Oncology, Chicago IL. Abstract No: LBA9000^

Patterns of response
26
Hodi et al, JCO 2016327 patients in KEYNOTE001 ≥ 28 week imaging f/u33 had pseudo progression

irRECIST
• Based on total measurable tumour burden and new lesions not automatic PD
– irCR – complete disappearance of all lesions in 2 observations 4 weeks apart
– irPR - ≥50% decrease in tumour burden in 2 observations 4 weeks apart
– irSd – not irCR, irPR or irPD!
– irPD - ≥25% increase in tumour burden over nadir
• Trials tend to include RECIST and irRECIST until this latter is fully validated
27Wolchok et al CCR 2009
Other challenges for response-based endpoints
• Many studies now allow continuation of treatment on PD if clinically benefitting
– Estimated ~8% subsequent RR in lung cancer for patients treated after progression
• Toxicity and later good response can go hand in hand
28

Challenges
• In the early trials patients were probably taken off who might have benefitted– ~10% patients with PD on first ipilimumab trials went on to have durable
clinical benefit
• Understanding pseudo-progression and how it should be consistently reported
• Knowing if hyper-progression occurs is critical– Initially reported in 9% (12/131) patients across tumour types (single
centre)
– ~16% NSCLC treated with anti-PD1 (multicentre)
29

CHALLENGES FOR TRIAL ENDPOINTS
Emergence of toxicity
30

Toxicity – mirrors auto-immune disease
Skin
Gastrointestinal
Hepatic
Neurologic
Endocrinopathies
Pneumonitis
Heart

Most important challenge of IO treatment
• Diarrhoea – colitis– Prophylactic loperamide given
– Patient warned to contact us if they have diarrhoea
– May need admission for intravenous steroids and infliximab
– Bowel perforation and death
• Rash– Various skin rashes – respond to moisturising and steroid creams
– Vitiligo and hair colour loss in long term
• Auto-immune endocrine disturbance– Thyroiditis
– Pan-hypothesitis with Addisonian crisis!!
• Liver function abnormalities
• Neurological side effects– Peripheral nerve motor or sensory loss
– Guillain Barre type syndrome
– Multiple cranial nerve palsies
32
55% of patients on combination IO treatment with ipi/nivo had a CTCAE grade 3 or 4 autoimmune side effects
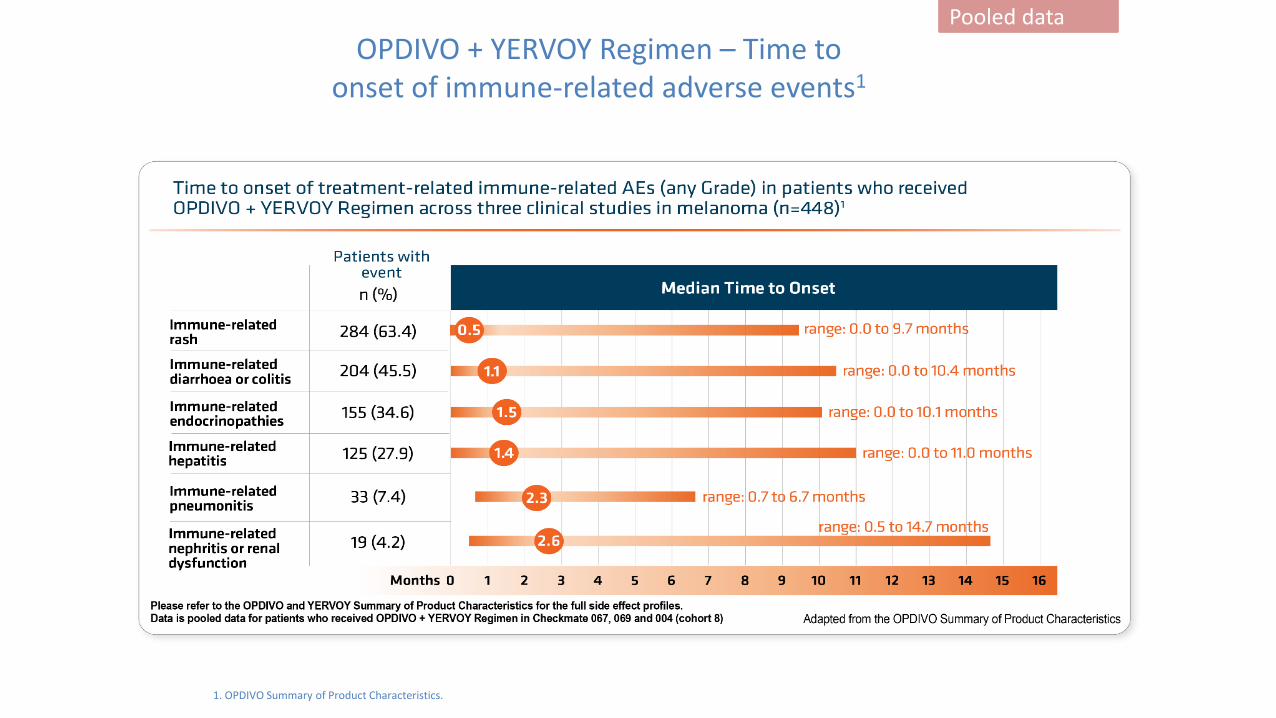
1. OPDIVO Summary of Product Characteristics.
OPDIVO + YERVOY Regimen – Time toonset of immune-related adverse events1
Pooled data
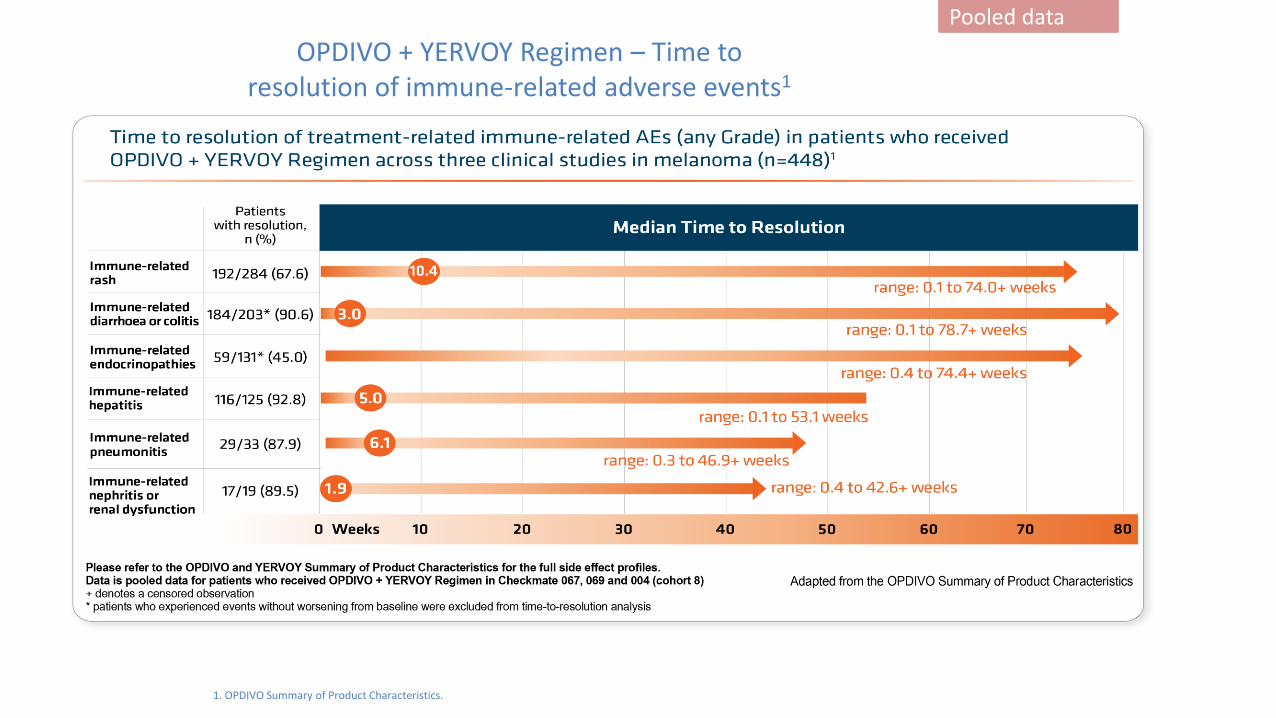
1. OPDIVO Summary of Product Characteristics.
OPDIVO + YERVOY Regimen – Time toresolution of immune-related adverse events1
Pooled data

Challenges in early phase safety studies
• Are DLT periods long enough?
– is the toxicity now predictable so we just need an idea of the safe dose
• Low grade but life long toxicity
– ?more of an issue in adjuvant setting
• Exclusion of sub-sets of patients
– Previous auto-immune disease
• Current evidence 30-35% such patients flare but RR similar to “normal” population
35

CHALLENGES FOR TRIAL ENDPOINTS
Combination therapy
36

“The pace of cancer immunotherapy clinical studies is such that they have outstripped our progress in understanding the underlying basic science.”
Chen and Mellman Nature 541, 321–330

Challenges
• What should we combine– Based on science
– Based on our drugs
– Based on standard of care in selected tumour
• Toxicity may be worse, or just additive– Ipi/nivo
– Ipi/vemurafenib
• Finding an optimal and efficient trial design– Randomised Bayesian phase I (SA v combo) with dose
model in difference in probability of DLT
38

CONCLUSIONS
39
Conclusions – challenges for early phase IO trials
• Doses and schedules explored need to make pharmacodynamic sense and we are very far from this
• We need better biomarkers for patient stratification
• Response patterns need better evaluation– Should combination studies be aimed at driving to CR or
overcoming resistance?
• Duration of treatment – can we stop earlier?
• Long term consequences late toxicity awaited
40

Thank you
41


















