recurrent dislocation patella.pptx
16
-
Upload
sunil-kumar-pd -
Category
Documents
-
view
20 -
download
0
Transcript of recurrent dislocation patella.pptx

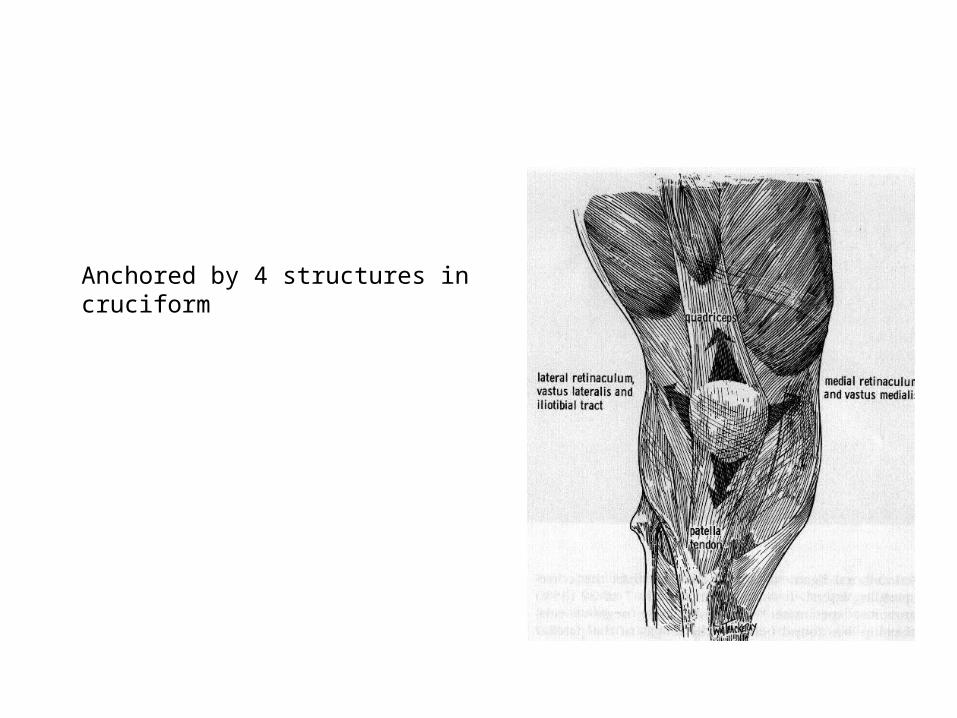
Anchored by 4 structures in cruciform

Static stabilizers
• Lateral retinaculum– Superficial and deep – Deep –superior ,middle and inferior
• Medial retinaculum– Medial patellofemoral ligament ( most imp)– Medial patellotibial ligament
• Ligamentum Patellae
types
• Acute• Recurrent• Habitual• Permanent

Chronic dislocation
• Knees in which patella dislocates laterally each time knee is flexed and returns to midline in extension(Habitual dislocation)
• More severe –patella permanently dislocated –(Permanent dislocation)
• Etiology:– Congenital
• Lig. Laxity• hypoplasia of lat. Femoral condyle• Flattening of Intercondylar groove• Patellar maldevelopment• Primary muscle defect• Genu valgum
– Acquired• Genu valgum• Inequality of growth of condyle• Weakness of Quads• Contracture• fibrosis
Clinical features
• Diffuse pain• Giving away sensation • Patellar crepitus and swelling
Q angle
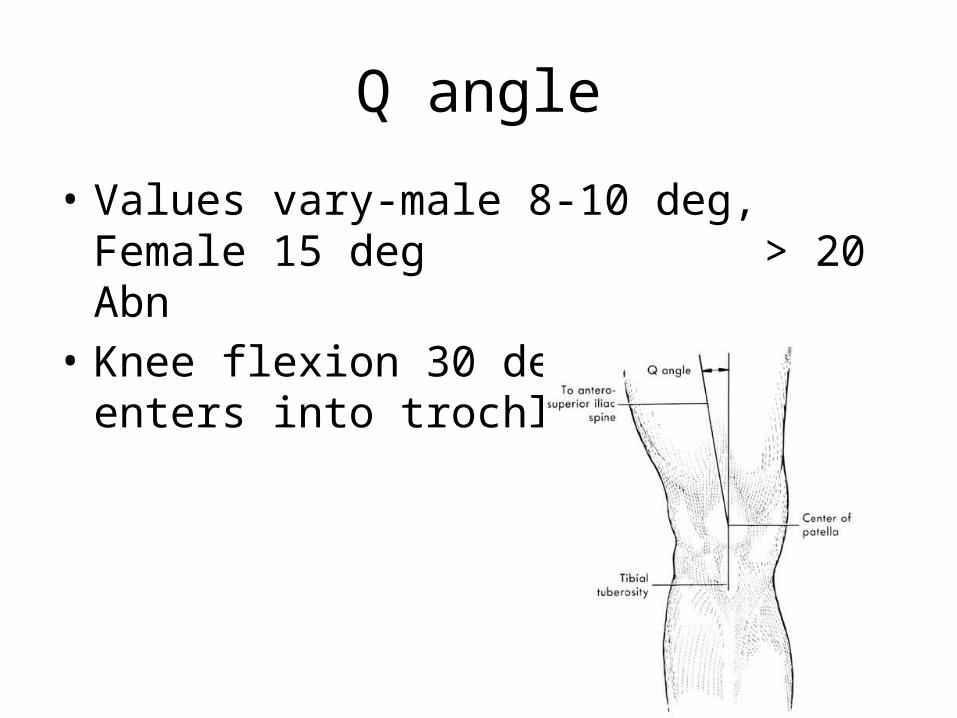
• Values vary-male 8-10 deg, Female 15 deg > 20 Abn
• Knee flexion 30 deg –Patella enters into trochlear sulcus.

Apprehension test of Fairbank
• Patella pushed laterally in 20-30 deg of flexion
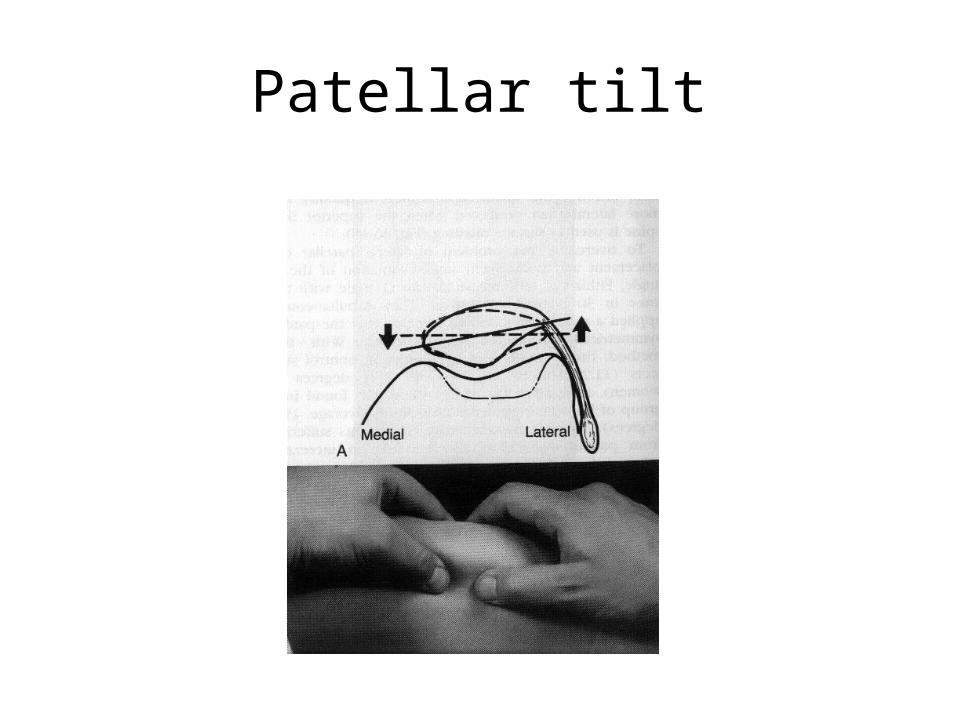
Patellar tilt
Management• Non Operative management– To be attempted in all patients.– Goals –Balanced quadriceps strength,
Stretching of tight lateral structures– Most important component –Quadriceps
training
Quadriceps Training• Most essential component• Strengthening of quads esp. VMO• Isometric and progressive resistive ex. with knee
in extension• With increase in strength,Short arc exercises in
last 300
• Knee braces with patella cut outs and lateral padding –some relief.

Surgical treatment• Once a specific malaligment problem has
been identified a surgical option can be selected
• Almost all techniques include Lateral release.
• Procedures to decrease laterally directed vector may be proximal, distal or combined realignment
Treament
• Based on pathology– Patella alta- distalization– Trochlear dysplasia- MPFL reconstruction– Patellar dysplasia- MPFL reconstruction
• Based on soft tissue imbalance– Dynamic (VMO dysfunction) – TT-TG <20 mm –
rehab– Sattic • Incompetant MPFL/ generalozed hyperlaxity -
medial imbrication or MPFL reconstruction

• Lateral release • Medial imbrication/ repair