Recurrent Complete Proximal Tibial Stress Fracture in a ... · PDF fileVol. 33, No. 12, 2005...
4
1914 The tibia is the most common site of stress fractures in athletes. 9 Anterior cortex midshaft tibial stress fractures are often associated with significant morbidity, including delayed union, nonunion, and complete fracture. 1,2,7,11 Stress fractures of the posteromedial tibial shaft and proximal tibial metaphysis are common and have been reported to heal readily with rest. 3,4,6,7 Although there are reports of isolated stress fractures of the medial or lateral tibial plateau, 5,10 there is little mention in the literature regarding stress fractures of the anterior proximal tibial metaphysis. 1,8 We report on a basketball player with a recurrent, complete stress fracture of the proximal tibial metaphysis. CASE REPORT A 21-year-old Division I college basketball player with a history of bilateral knee pain was evaluted with increasing pain in the tibial tubercle region. His medical history was significant for a right ankle fracture in grade 9 that was treated nonoperatively. He began developing symptoms consistent with bilateral patellar tendinitis in grade 11 and had increasing right ankle pain consistent with ankle impingement in grade 12. Before his entrance to college, he underwent ankle surgery to remove “bone spurs.” In col- lege, he was evaluted with a varus hindfoot and continued limitations in dorsiflexion and subtalar motion. Passive range of motion of his right ankle was 0° of dorsiflexion, 30° of plantar flexion with the knee extended, and no change in passive dorsiflexion with knee flexion. He com- plained of pain in both knees, and there was tenderness to palpation over his tibial tubercles, which was greater for the left knee. Because of his increasing left knee pain, an MRI scan was obtained that confirmed patellar tendinitis. No MRI was obtained on the right knee. The athlete con- tinued to engage in practices and games with no com- plaints to the athletic trainer or team physician of pain in either knee. While leaping for a rebound during a game, the athlete experienced acute pain on takeoff, suffering knee/leg col- lapse on landing. Subsequent examination and plain radi- ographs revealed a proximal tibial fracture with some scle- rosis at the proximal tibial cortex (Figure 1). This finding was thought to be suspicious for a previous stress reaction, and a CT scan was ordered that revealed sclerosis at the fracture site (Figure 2). These findings were consistent with acute completion of a proximal tibial stress fracture at the level of the tibial tubercle. Although the growth plates were closed, the pattern of injury seemed to follow the anatomy of the proximal tibial physis/apophysis. The patient underwent open reduction and internal fix- ation with 3 screws (Figure 3). This type of fixation was chosen by the operating surgeon, a board-certified trau- matologist, for 2 reasons. First, it provided adequate reduction of the fracture with no motion at the fracture site with intraoperative radiographic stressing. Second, there was a concern that more rigid forms of fixation (plate and screws) might be associated with a higher incidence of tibial pain when the athlete returned to jumping or high- impact sports. Four months postoperatively, the patient returned to some conditioning activities with no discomfort but did not resume jumping or running. Routine radiographs and a CT scan revealed a persistent anterior cortical lucency (Figure 4). At this time, it was midsummer, 4 months before the start of formal basketball practice, and an autol- ogous iliac crest bone grafting procedure was performed to maximize the potential for healing over the next 2 to 3 months (Figure 5). Two to 3 months after the bone graft- Recurrent Complete Proximal Tibial Stress Fracture in a Basketball Player Christopher M. Larson,* † MD, Steven M. Traina, ‡ MD, David A. Fischer, § MD, and Elizabeth A. Arendt, ll MD From the † Minneapolis Sports Medicine, Minneapolis, Minnesota, ‡ Orthopedic Associates, Denver, Colorado, § The Orthopaedic Center, Eden Prairie, Minnesota, and the ll University of Minnesota, Minneapolis, Minnesota Keywords: stress fracture; knee; tibia; basketball; recurrent fracture *Address correspondence to Christopher M. Larson, MD, Flagship Corporate Center, 775 Prairie Center Drive #250, Eden Prairie, MN 55344 (e-mail: [email protected]). No potential conflict of interest declared. The American Journal of Sports Medicine, Vol. 33, No. 12 DOI: 10.1177/0363546505274715 © 2005 American Orthopaedic Society for Sports Medicine
Transcript of Recurrent Complete Proximal Tibial Stress Fracture in a ... · PDF fileVol. 33, No. 12, 2005...
1914
The tibia is the most common site of stress fractures inathletes.9 Anterior cortex midshaft tibial stress fracturesare often associated with significant morbidity, includingdelayed union, nonunion, and complete fracture.1,2,7,11
Stress fractures of the posteromedial tibial shaft andproximal tibial metaphysis are common and have beenreported to heal readily with rest.3,4,6,7 Although there arereports of isolated stress fractures of the medial or lateraltibial plateau,5,10 there is little mention in the literatureregarding stress fractures of the anterior proximal tibialmetaphysis.1,8 We report on a basketball player with arecurrent, complete stress fracture of the proximal tibialmetaphysis.
CASE REPORT
A 21-year-old Division I college basketball player with ahistory of bilateral knee pain was evaluted with increasingpain in the tibial tubercle region. His medical history wassignificant for a right ankle fracture in grade 9 that wastreated nonoperatively. He began developing symptomsconsistent with bilateral patellar tendinitis in grade 11and had increasing right ankle pain consistent with ankleimpingement in grade 12. Before his entrance to college,he underwent ankle surgery to remove “bone spurs.” In col-lege, he was evaluted with a varus hindfoot and continuedlimitations in dorsiflexion and subtalar motion. Passiverange of motion of his right ankle was 0° of dorsiflexion,30° of plantar flexion with the knee extended, and nochange in passive dorsiflexion with knee flexion. He com-
plained of pain in both knees, and there was tenderness topalpation over his tibial tubercles, which was greater forthe left knee. Because of his increasing left knee pain, anMRI scan was obtained that confirmed patellar tendinitis.No MRI was obtained on the right knee. The athlete con-tinued to engage in practices and games with no com-plaints to the athletic trainer or team physician of pain ineither knee.
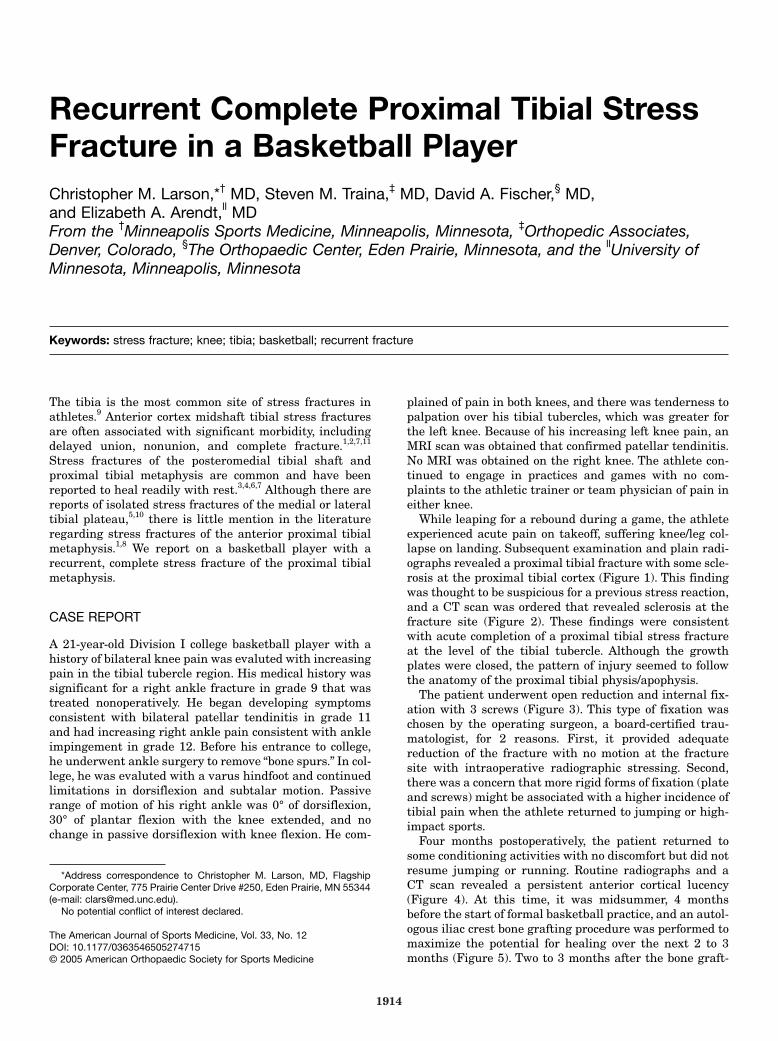
While leaping for a rebound during a game, the athleteexperienced acute pain on takeoff, suffering knee/leg col-lapse on landing. Subsequent examination and plain radi-ographs revealed a proximal tibial fracture with some scle-rosis at the proximal tibial cortex (Figure 1). This findingwas thought to be suspicious for a previous stress reaction,and a CT scan was ordered that revealed sclerosis at thefracture site (Figure 2). These findings were consistentwith acute completion of a proximal tibial stress fractureat the level of the tibial tubercle. Although the growthplates were closed, the pattern of injury seemed to followthe anatomy of the proximal tibial physis/apophysis.
The patient underwent open reduction and internal fix-ation with 3 screws (Figure 3). This type of fixation waschosen by the operating surgeon, a board-certified trau-matologist, for 2 reasons. First, it provided adequatereduction of the fracture with no motion at the fracturesite with intraoperative radiographic stressing. Second,there was a concern that more rigid forms of fixation (plateand screws) might be associated with a higher incidence oftibial pain when the athlete returned to jumping or high-impact sports.
Four months postoperatively, the patient returned tosome conditioning activities with no discomfort but did notresume jumping or running. Routine radiographs and aCT scan revealed a persistent anterior cortical lucency(Figure 4). At this time, it was midsummer, 4 monthsbefore the start of formal basketball practice, and an autol-ogous iliac crest bone grafting procedure was performed tomaximize the potential for healing over the next 2 to 3months (Figure 5). Two to 3 months after the bone graft-
Recurrent Complete Proximal Tibial StressFracture in a Basketball PlayerChristopher M. Larson,*† MD, Steven M. Traina,‡ MD, David A. Fischer,§ MD, and Elizabeth A. Arendt,ll MDFrom the †Minneapolis Sports Medicine, Minneapolis, Minnesota, ‡Orthopedic Associates,Denver, Colorado, §The Orthopaedic Center, Eden Prairie, Minnesota, and the llUniversity ofMinnesota, Minneapolis, Minnesota
Keywords: stress fracture; knee; tibia; basketball; recurrent fracture
*Address correspondence to Christopher M. Larson, MD, FlagshipCorporate Center, 775 Prairie Center Drive #250, Eden Prairie, MN 55344(e-mail: [email protected]).
No potential conflict of interest declared.
The American Journal of Sports Medicine, Vol. 33, No. 12DOI: 10.1177/0363546505274715© 2005 American Orthopaedic Society for Sports Medicine

Vol. 33, No. 12, 2005 Recurrent Complete Proximal Tibial Stress Fracture 1915
ing, the patient was pain free, with decreased but persist-ent lucency noted only anteriorly, and was allowed toprogress to full sporting activity as tolerated (Figure 6).
The athlete returned to full workouts commensuratewith the formal start of the season (mid-October). He com-peted fully in all practices and games without any com-
plaints of pain, discomfort, or disability. In February, afternearly 5 months of full competition, the patient sustaineda refracture through the proximal tibial tubercle regionduring a noncontact, power-takeoff maneuver (Figure 7).
Figure 1. Plain radiograph revealing a proximal tibial fracturewith some sclerosis about the fracture.
Figure 2. A CT scan after initial injury revealing sclerosisabout the fracture, which was consistent with a stress fracture.
Figure 3. Initial postoperative radiograph revealing reductionand fixation of the fracture with 3 screws.
Figure 4. A CT scan 4 months postoperatively revealing per-sistent lucency. The screws were still in place but not visibleon this particular image.

1916 Larson et al The American Journal of Sports Medicine
He then underwent a repeat open reduction and internalfixation with a plate and lag screw technique. This proce-dure led to complete union, as shown on radiographs, andthe patient was able to return to basketball activities 5 to6 months postoperatively. There were no further sequelaeat the most recent follow-up of 3 years postoperatively(Figure 8).
DISCUSSION
The tibia is reported to be the most common location forstress fractures in athletes.9 Proximal metaphysial tibialstress fractures are typically posteromedial (compressionside) in location and heal readily with activity modifica-tion and rest.3,4,6,7
Stress fractures of the anterior cortex in the mid-diaphysisare much less common than those of the proximal postero-medial tibia.2,6,7,11 There have been several reports ofdelayed union, nonunion, and complete fracture as a resultof these anterior tibial stress fractures.1,2,7,11 Rettig et al11
evaluated 8 patients with middle-third anterior cortex tib-ial stress fractures, and all patients participated in bas-ketball activity. The middle third of the tibia is under ten-sion rather than compression as a result of forces causedby the large posterior muscle groups, and this tension isthought to lead to prolonged healing times.2,6,7,11 Anterior
cortex stress fractures often require surgical interventionsuch as excision and bone grafting or intramedullary nail-ing to achieve union.2,7
Although there have been several reports of isolatedmedial and lateral tibial plateau stress fractures,5,10 thereis little in the literature with regard to anterior proximalmetaphysial tibial stress fractures. There are 2 reports ofbasketball players with anterior proximal tibial stressfractures just distal to the tibial tuberosity.1,8 One of thesefractures resulted in a complete fracture that healed withimmobilization,8 and the other healed after open reductionand internal fixation with a plate and screws.1 Althoughthese fractures were more distal than was the level of frac-ture in the current case, they suggest a relationshipbetween repetitive jumping activity and anterior cortextibial stress fractures.
The persistent restrictions for dorsiflexion and subtalarrange of motion, combined with repetitive jumping, mayhave predisposed the patient to this injury. It is also inter-esting to note the pattern of injury that seemed to followthe anatomy of the proximal tibial physis/apophysis. Itmay be that the increased stresses across the physisresulted in incomplete closure and stress reaction throughthe growth center. This reaction may have then led to com-plete fracture. Although we have no radiographs beforeinjury of the right knee to verify incomplete closure of the
Figure 5. Intraoperative plain radiograph showing localiza-tion of the fracture with a needle. Autogenous bone graftingand removal of a prominent screw were performed at this time.
Figure 6. Plain radiograph 3 months after the bone graftingprocedure revealing consolidation of the posterior portion ofthe original fracture and persistent anterior lucency.

Vol. 33, No. 12, 2005 Recurrent Complete Proximal Tibial Stress Fracture 1917
physis/apophysis or chronic stress injury, the timing of theankle injury and development of knee pain would coincidewith the time of growth plate closure.
In retrospect, the technique of initial fixation and per-sistent anterior tibial lucency may have contributed to therecurrent fracture. Initial internal fixation of maximalrigidity and complete healing, as shown on radiographs,may be critical to prevent the development of a nonunionor recurrent injury with this unusual fracture pattern.
Proximal metaphysial tibial stress fractures can be dif-ficult to diagnose because of their proximity to the kneejoint and its surrounding structures. The diagnosis in thecurrent case was initially delayed because of the fracture’slocation at the tibial tuberosity, with a long history of bilat-eral patellar tendinitis. We are not aware of any otherreports of a complete tibial stress fracture at the level ofthe tibial tuberosity.
CONCLUSION
The current case shows the difficulties in managing thisfracture and that a high index of suspicion may be impor-tant in making an early diagnosis. Chronic restriction of
ipsilateral ankle dorsiflexion and subtalar range of motionin this case may have been a contributing factor. Onlyafter rigid internal fixation was achieved did the fractureheal. We believe that it is essential to obtain completehealing of this fracture before a return to competitivejumping activities. Rigid internal fixation of maximumrigidity appears to be optimal to achieve union with thisparticular fracture.
REFERENCES
1. Blank S. Transverse tibial stress fractures: a special problem. Am JSports Med. 1987;15:597-602.
2. Chang PS, Harris RM. Intramedullary nailing for chronic tibial stressfractures: a review of five cases. Am J Sports Med. 1996;24:688-692.
3. Collier DB, Johnson RP, Guillerma FC, Akhtar K, Isitman AT.Scintigraphic diagnosis of stress-induced incomplete fractures of theproximal tibia. J Trauma. 1984;24:156-160.
4. Daffner RH, Martinez S, Gehweiler JA, Harrelson JM. Stress fracturesof the proximal tibia in runners. Radiology. 1982;142:63-65.
5. Engber WD. Stress fractures of the medial tibial plateau. J Bone JointSurg Am. 1977;59:167-169.
6. Friedenberg ZB. Fatigue fractures of the tibia. Clin Orthop.1971;76:111-115.
7. Green NE, Rogers RA, Lipscomb AB. Nonunions of stress fracturesof the tibia. Am J Sports Med. 1985;13:171-176.
8. Lambros G, Alder D. Multiple stress fractures of the tibia in a healthyadult. Am J Orthop. 1997;26:687-688.
9. Matheson GO, Clement DB, Mckenzie DC, Taunton JE, Loyd-SmithDR, MacIntyre JG. Stress fractures in athletes: a study of 320 cases.Am J Sports Med. 1987;15:46-58.
10. Mizuta H, Sakata H. An unusual stress fracture of the lateral tibialplateau. Arch Orthop Trauma Surg. 1993;112:96-98.
11. Rettig AC, Shelbourne KD, McCarroll JR, Bisesi M, Watts J. The nat-ural history and treatment of delayed union stress fractures of theanterior cortex of the tibia. Am J Sports Med. 1988;16:250-255.
Figure 7. Plain radiograph revealing a refracture of the prox-imal tibia.
Figure 8. Anteroposterior (A) and lateral (B) radiographsrevealing complete healing of the fracture 3 years after rigidopen reduction and internal fixation with a plate and lagscrew technique.
A B