Rectocele repair in obstructed defecation :...
30
I Rectocele repair in obstructed defecation : randomized comparative study BY MOHAMED FARID MD.TAREK MAHDY MD. HESHAM A. MONEIM MD. WALEED OMAR MD. FROM COLORECTAL SURGERY UNIT, MANSOURA UNIVERSITY HOSPITAL, MANSOURA, EGYPT ---------------------------------------------------------------------------------- ADRESS FOR CORRESPONDANCE: MOHAMED FARID Professor of general surgery & Head of Colo-Rectal Surgery Unit, Mansoura University Hospital, Mansoura, EGYPT. P.O BOX: 324, MANSOURA, EGYPT. TEL. 050/ 2219403 FAX: 050/ 2267016 E-mail : [email protected]
Transcript of Rectocele repair in obstructed defecation :...

I
Rectocele repair in obstructed defecation : randomized comparative
study
BY
MOHAMED FARID MD.TAREK MAHDY MD.
HESHAM A. MONEIM MD. WALEED OMAR MD.
FROM
COLORECTAL SURGERY UNIT, MANSOURA UNIVERSITY
HOSPITAL, MANSOURA, EGYPT
---------------------------------------------------------------------------------- ADRESS FOR CORRESPONDANCE: MOHAMED FARID Professor of general surgery & Head of Colo-Rectal Surgery Unit, Mansoura University Hospital, Mansoura, EGYPT. P.O BOX: 324, MANSOURA, EGYPT. TEL. 050/ 2219403 FAX: 050/ 2267016 E-mail : [email protected]

I
ABSTRACT
Purpose: this study was undertaken to evaluate the results of
transperineal repair with or without levator ani repair and transrectal repair
of rectocele as regards both anatomic and symptomatic concerns. Methods:
between December 1998 and December 2000, we performed a prospective
study of 48 female patients with obstructed defecation due to rectocele. All
patients were studied prospectively according to a fixed protocol that
included clinical evaluation, defecography, and manometric studies, which
were performed preoperatively, and 6 months postoperatively. Transperineal
repair was done in 31 patient (15 with levator ani repair) and transrectal
repair in 17 patients. Results: six months postoperatively there was a
significant clinical improvement in all patients except those who underwent
transrectal repair. Postoperative defecography showed decrease of rectocele
size in all patients but significant improvement in rectal evacuation occurred
only in patients with transperineal repair. Postoperative manometric studies
showed a significant decrease in the Urge To Defecate Volume (UTDV) and
Maximum Reflex Volume (MRV) in transperineal approaches. There was a
significant difference between patients who did or did not feel improved by
surgery in the percentage reduction in the volume at which an urge to
?
defecate was elicited (UTDV) and the Maximal inhibitory anal Reflex
Volume (MRV) in all surgical approaches. Conclusion: Rectocele repair
improves anorectal function by improving the rectal urge sensitivity. This
study displays the efficacy of transperineal approach with levator ani repair.
Decrease of UTDV, MRV, reduction of rectocele size and complete
evacuation were considered the convenient parameters for the success of
surgery.

?
Introduction
Rectocele is a common finding in patients with defecation disorders,
and its role in these disorders remains debated (1,2). Up to 30 percent of
middle aged and elderly adults feel constipated (3). Seventeen percent of
adults, strain excessively at stool and 12 percent use laxative (4). Difficulty in
rectal evacuation is frequently seen in multiparous women. Obstetric
damage and increasing laxity of tissues with increasing age are possible
patho-genetic factors (5,6). Rectocele can give rise to a variety of symptoms,
such as blood loss, pain, pruritis, fecal incontinence, and digital (rectal or
vaginal) assistance to defecate. These symptoms may be caused by damage
to the anterior rectal wall, a nonspecific inflammatory reaction as well as
anatomic and physiological changes in rectal accommodation (7).
In clinical practice, the relationship between anatomic abnormalities and
symptoms is not clear. Rectocele occurs in 20 to 81 percent of both
asymptotic females and patients with constipation (8). Only 23 to 70 percent
of unselected patients with rectocele have symptoms related to difficulty in
defecation (9,10). It is important to identify a rectocele when it is the cause of
obstructive defecation and proper repair of recto-vaginal septum results in
gratifying improvements in constipation problem (11). Symptoms are not
?
always alleviated by either vaginal, transperineal or transrectal rectocele
repairs (1,10,12,13,14). It is not known whether failure of surgical repair in these
patients relates to the failure to correct or there are other factors.
The principal aim of our study is to evaluate the results of
transperineal repair with or without levator ani repair and transrectal repair
of rectocele considering the anatomic and symptomatic improvements.

?
Patients & Methods
From December 1998 to December 2000. A prospective randomized
study was followed. During this period 60 female patients with obstructed
defecation underwent operation for rectocele. Of those screened, 55 patients
passed the exclusion criteria (slow- transit constipation using radio opaque
markers and abnormal thyroid function) and were fully informed about
transrectal and transperineal repair with or without levator repair. Inclusion
criteria involved rectocele size more than 2 cm that were associated with one
or more of the following symptoms (digital manipulation during defecation,
incomplete evacuation, excessive straining or sexual function disturbances
mainly dysparaunia). Of the 55 patients meeting the inclusion criteria, 48
patients [median age, 42 (range 26 - 61) years] were agreed to randomization
and signed an informed consent. Drawing sealed envelopes containing the
transrectal participants, the transperineal participants and transperineal with
levator repair participants were blinded the randomization. The sample size
was estimated on the basis of the number of patients predicted to present
with obstructive defecation due to rectocele over a predefined recruitment
period of 2 years. All patients were evaluated preoperatively according to a
standardized protocol. This included a detailed questionnaire, with special
reference to defecation frequency, use of laxative, excessive straining,

O
digital manipulation during defecation, sensation of incomplete evacuation,
frequency of incontinence, stool consistency, blood loss, dysparaunia and
past history of pelvic or anorectal surgery. All patients had been studied
preoperatively with digital assessment, rigid proctoscope and defecography
was performed as described by Ginai (15). Defecographic findings included
rectocele size and contrast evacuation of the rectocele (grade 0: no
evacuation, grade 1,2,3,4: evacuation was poor, moderate, subtotal and total)
(16). Rectal evacuation was evaluated using the same grading of rectocele.
Perineal descent and anorectal angle were also evaluated (17,18). Anorectal
manometry using perfusion catheter systems (Synectics, Stockholm,
Sweden) (19,20) was done for all patients with the evaluation of maximum
anal resting pressure (MRP), maximum anal squeezing pressure (MSP),
rectal sensitivity threshold volume (STV), urge to defecate volume (UTDV),
maximum tolerable volume (MTV), anal inhibitory reflex threshold (RTV),
maximum reflex volume (MRV) and functional anal canal length (cm).
Transperineal repair was done for thirty- one patients (15 with levator ani
repair) and transrectal for seventeen patients (2,12,21,22). Patients were followed
up routinely for one to two months after surgery. Functional results were
evaluated after six months (by examiners blinded the type of operative
treatment for each patient) by anal manometry, defecography and

?
questionnaire reflecting the symptomatic results. Outcome was considered
(improved) if the main symptoms disappeared and not improved if it
persisted. Statistical analysis was performed using nonparametric tests for
comparisons. For qualitative data, chi- square or fisher’s exact probability
tests (two samples, unpaired) or Mc Nemar test (two samples, paired) was
used. For quantitative data Wilcoxon`s signed rank test (two samples,
paired) with correction for ties was used. To investigate the relationship
between change in rectocele size dimension and symptoms or the type of
surgery the Mann Whitney test with correction for ties was used. Two-sided
values ? 0.05 were considered significant.
?
Results
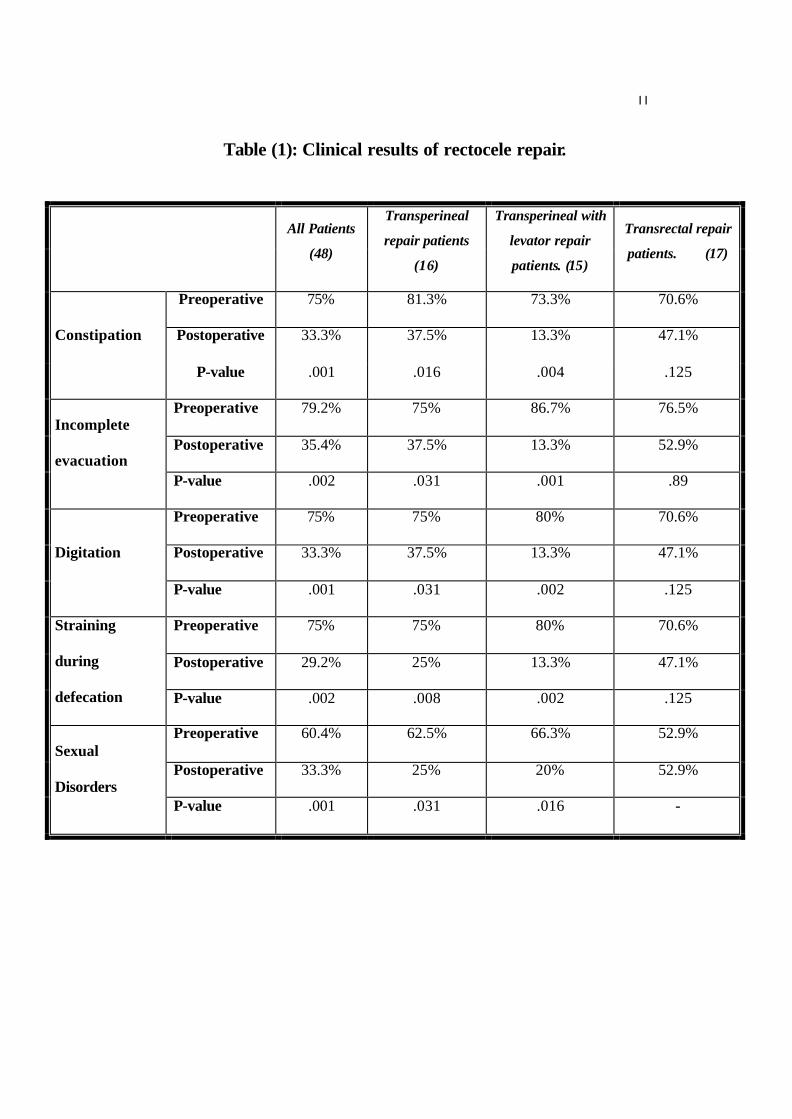
As shown in table (1), 75 percent of patients were complaining of
constipation and straining during defecation. 79.2 percent of patients
experienced a feeling of incomplete emptying. 75 percent of patients
digitally assisted defecation through vagina and 60.4 percent of patient
experienced dysparaunia. Postoperatively there was a significant
improvement of symptoms in patients with transperineal repair.
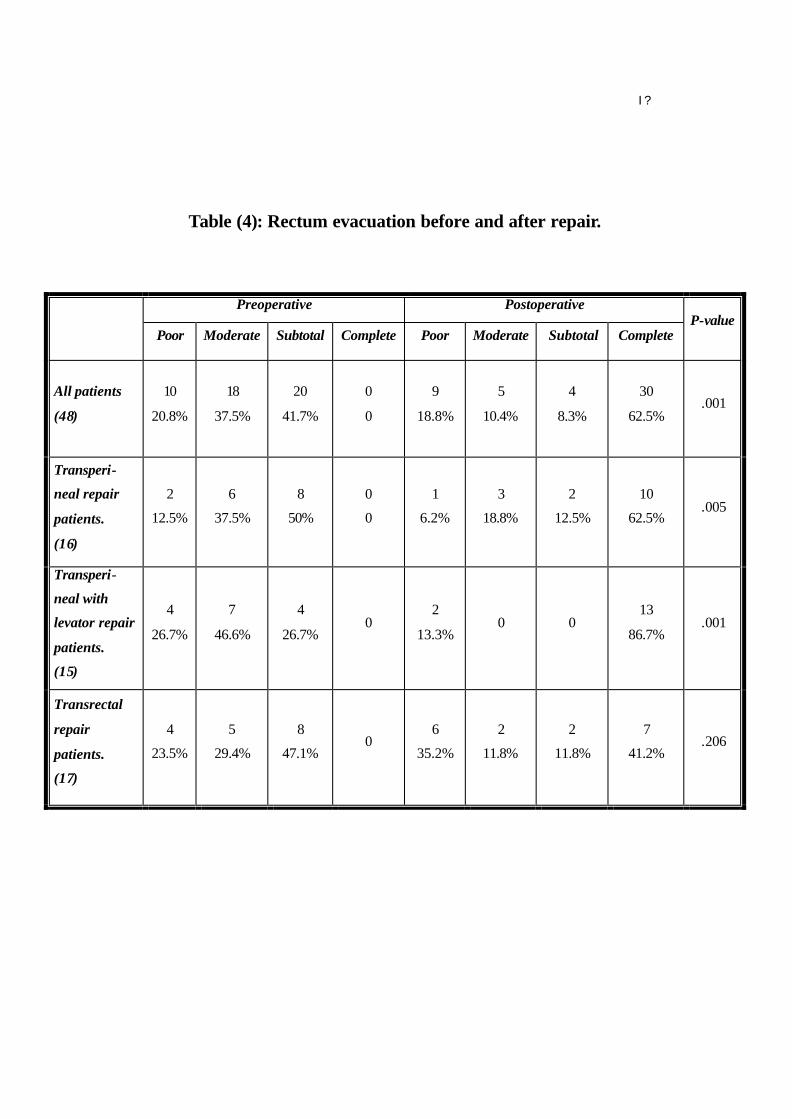
As regards the defecographic findings, there was a significant
decrease in the rectocele size in all surgical approaches (table 2) and
significant improvement of rectocele evacuation after transperineal repair on
the contrary in transrectal repair patients (Table 3). Moreover, there was also
a significant improvement in rectal evacuation following transperineal repair
(table 4).
There was significant difference between patients (who did or did not
feel improved by surgery) in the percentage reduction in rectocele size and
evacuation (table 5,6) in all surgical approaches. In table (7) there were
significant changes in the MARP, UTDV and MRV in transperineal
approach with or without levator ani repair but not with transrectal repair.
On the other hand, there was significant difference between patients
(who did or did not feel improved by surgery) in the percentage reduction in
I ?
the volume at which an urge to defecate was elicited (UTDV) and the
maximal inhibitory anal reflex volume (MRV), in all surgical approaches. It
was also noticed that, in the transperineal approach with levator ani repair,
there was significant differences between improved and not improved
patients in the percentage reduction in the MARP (table 8).
It is noted from table (9) that, there was significant improvement in
patients who had transperineal approach with levator ani repair versus the
transrectal repair.
I I
DISCUSSION
Normal defecation is a complex neuromuscular process that requires the
integration of neuromuscular activity of large bowel, rectum and pelvic
floor muscles, together with the absence of anatomical factors that inhibit
this process (23). A rectocele is a herniation of the anterior rectal wall
through the rectovaginal septum into the vagina (11). The most important
risk factors are a previous hysterectomy, obstetric injuries and the
descending perineum syndrome (5,6). In some patients the rectocele
becomes symptomatic because of defecation disorders (9,10). The patients
have to give manual vaginal or perineal help during defecation (24). Many
authors have recognized that the relationship between impaired defecation
and the presence of a rectocele is a complex one (25, 26). We believe that
rectocele repair produces symptomatic benefits through anatomical
improvement and mechanisms that alter rectoanal evacuation, as it could
be notified from our results that there is significant improvement in
evacuation although the rectocele did not disappear completely.
We consider defecography has an impact on the diagnosis and estimation of
outcome after surgery. Sarles et al (27) advocated that retention of contrast

I I
medium in the rectocele could be used for selection of patients for rectocele
repair. The present study shows, significant reduction in size of rectocele in
the three surgical approaches, but complete evacuation of rectocele was
significant only in the two-transperineal approaches, probably this could be
explain the significant improvement in symptoms after transperineal
approach specially with levator ani repair rather than patients with
transrectal repair. Concerning manometric studies, we think that changes in
UTDV are a sensible predictor for improvement after surgery. This concept
is reinforced by the idea that continence during the daytime is more
dependent on rectal sensation of urge than on the sphincter pressure. Thus on
looking to the results and considering this view, we can find that
transperineal with levator repair leads to a more significant reduction in
UTDV, in comparison with other approaches a finding probably not
popularized too much by other investigators. Our findings revealed that
postoperative MARP did not differ significantly from preoperative MARP
value except in transperineal with levator repair. Moreover, the latter
observation suggests that contribution of MARP provided by the external
sphincter tonus was decreased substantially by the operation. We suppose
that, this could be related to a better awareness of urge and sphincter control
without the need for a compensatory protective increase in resting pressure.

I ?
Another significant finding is that the MRV required to induce maximum
anal relaxation is decreased after surgery and is more significantly decreased
after transperineal with levator repair rather than transrectal repair. This may
suggest that obstructed defecation by a large rectal volume is positively
influenced by the repair. This is supported by the finding that outlet -
obstructed patients show a significant increase in stool frequency shortly
after operation. This could be due to the combined significantly improved
rectal sensation (UTDV) with a significantly lowered MRV, and this
probably give an impact in patients with obstructed defecation rather than
the effect of rectoanal inhibitory reflex alone. In most studies (22,24,28), there is
a group of patients who do not benefit from operation. In our study, there is
only 13.3% did not improve after transperineal approach with levator ani
repair which is less than the reports in published series. The results of
rectocele surgery are reported to be satisfactory (1,2, 22). In our study, 86.7% of
rectocele patients were improved after transperineal with levator repair in
contrary to 62.5% and 41.2% improvement after transperineal and
transrectal repairs respectively. This satisfactory clinical data combined with
improvement in anorectal manometry and defecographic findings after
transperineal with levator repair could encourage us to perform this kind of
surgery in management of rectocele. From our results it is noted that
I ?
transrectal repair showed a worse outcome. This could be due to its
dependence only on plicating the rectum up to 10 cm. on the contrary of
transperineal with levator repair which gives a firm rectovaginal septum
with better and accurate access to the apex of rectocele

I ?
Conclusions
Rectocele repair improves anorectal function by improving UTDV, MRV,
reduction of rectocele size and improvement of rectal – rectocele evacuation.
Transperineal with levator repair looks to give a satisfactory outcome rather
than transperineal without levator repair or transrectal repair.

I ?
References
(1) Arnold MW, Stewart WR, Aguilar PS.
Rectocele repair. Four years experience.
Dis Colon Rectum (1990); 33: 684-7.
(2) Khubchandani IT, Clancy JR, Rosen L, et al.
Endorectal repair of rectocele revisited.
Br J surgery (1997); 84: 89-91.
(3) Whitehead WG, Drink water D, Cheskin LJ, et al
Constipation in The elderly living at home: definition, prevalence and
relationship to Lifestyle and health status.
JA M Geriatr soc. (1989); 37: 423 - 9
(4)Sonnenberg A, Everhart JE, Brown DM.
The economic cost of constipation. In: Kamm MA. Lennard-Jones JE,
Eds. Constipation. Petersfield, united kindom: Wrightstown Biomedical
publishing, 1994: 19-29.
(5) Sehapayak S.
Transrectal repair of rectocele: an extended armamentarium of
colorectal surgeons. A report of 355 cases.
Dis Colon Rectum (1985); 28:422-33
I O
(6) SarlesJc, Arnaud A, Selezneff I, et al.
Endorectal repair of rectocele.
Int J colorectal Dis (1989); 4: 167-71.
(7) Bouchacha M, Denis P, Arhan P, et al.
Morphology and rheology of the rectum in patients with chronic
idiomatic Constipation.
Dis Colon Rectum 1989; 32:788-92
(8) Siproudhis L, Dautreme S, Robert A, et al.
Dyschezia and rectocele-a marriage of inconvenience?
Psychological evaluation of the rectocele in a group of 52 women
complaining of difficulty in evacuation.
Dis Colon Rectum 1993;36:1030-6
(9) Yoshioka K, Matsui Y, Yamade O, et al.
Physiological and anatomic assessment of patients with rectocele.
Dis Colon Rectum 1991
(10) Van laarhoven C, Kamm M, Bartram C, et al.
Relationship between anatomic and symptomatic long-Term results
after rectocele repair for impaired defecation.
Dis Colon Rectum 1999; 42:204-10.

I ?
(11) Richardson Ac.
The rectovaginal septum revisited: its relationship to rectocele
repair.
Clin Obstet Gynaecol 1993; 36:976-83.
(12) Sullivan ES, Leaverton GH, Hardwick CE.
Transrectal perineal repair: an adjunct to improved function after
anorectal surgery.
Dis Colon Rectum 1968; 11:106-14.
(13) Janssen LW, Van Dijke CF.
Selection criteria for anterior rectal wall repair in symptomatic
rectocele and anterior rectal wall prolapse.
Dis Colon Rectum 1994; 37:1100-7.
(14) Infantino A, Masin A, Melega E, et al.
Does surgery resolve outlet obstruction from rectocele?
Int j Colorect Dis 1995;10:97-100
(15) Ginai AZ.
Technical report: evacuation proctography (defecography) a new seat
and method of examination.
Clin Radiol. 1990; 42:214-6.

I ?
(16) Kelvin FM, Maglinte DD, Hornback JA,
Pelvic floor prolapse : assessment with evacuation
proctography ( defecography).
Radiology 1992; 184: 547-51.
(17) Halligan S, McGee S, Bartram CI.
Quan Tification of evacuation proctography.
Dis Colon Rectum 1994; 37:1151-4.
(18) Van Dam JH, Ginai AZ, Gosselink MJ, et al.
Role of Defecography in predicting clinical outcome of rectocele
repair.
Dis Colon Rectum 1997; 40:201-7.
(19) HO YH, Goh HS.
Current value of anorectal physiology and biofeedback in clinical
practice.
Asian J surg 1995; 18:244-56.
(20) HO YH, Goh HS.
Anorectal physiological parameters in chronic constipation of
unknown etiology (primary) and of cerebrovascular accidents : a
preliminary report.
Ann Acad Med Singapore 1995; 24:376-8.
I ?
(21) Karlbom U, Graf W, Nilsson S, et al.
Does surgical repair of rectocele improve rectal emptying?
Dis Colon Rectum 1996; 39:1296-1302.
(22) Mellgren A , Anzen B , Nilsson B , et al.
Results of rectocele repair : a prospective study.
Dis colon rectum 1995 ; 38 : 7 – 13.
(23) Kamm MA, Vander Sijp JR, Lennard-Jones JE.
Colorectal and anal motility during defecation.
Lancet 1992; 339:820.
(24) Lucas W , Cornelis F.
Selection criteria for anterior rectal wall repair in symptomatic
rectocele and anterior rectal wall prolapsed.
Dis colon rectum 1994 ; 37 : 1100 – 7 .
(25) Van dam JH , Schouten WR , Ginai AZ . et al .
The impact of anismus on Clinical outcome of Rectocele repair .
Int. J Colorectal Dis 1996; 11: 238 – 42.
(26) Van dam JH , Hop WC and Schouten WR .
Analysis of patients with Poor Outcome of Rectocele repair.
Dis colon rectum 2000 ; 43 : 1556 – 60
I I
( 27) Sarles JC, Arnaud A, Sicelezneff I, et al.
Endo-rectal repair of rectocele.
Int j colorectal Dis 1989; 4:167-71.
(28) Block IR .
Transrectal repair of rectocele using obliterative sutures.
Dis colon rectum 1986 ; 29 : 707 – 11
I I
Table (1): Clinical results of rectocele repair.
All Patients
(48)
Transperineal
repair patients
(16)
Transperineal with
levator repair
patients. (15)
Transrectal repair
patients. (17)
Preoperative 75% 81.3% 73.3% 70.6%
Postoperative 33.3% 37.5% 13.3% 47.1% Constipation
P-value .001 .016 .004 .125
Preoperative 79.2% 75% 86.7% 76.5%
Postoperative 35.4% 37.5% 13.3% 52.9% Incomplete
evacuation P-value .002 .031 .001 .89
Preoperative 75% 75% 80% 70.6%
Postoperative 33.3% 37.5% 13.3% 47.1% Digitation
P-value .001 .031 .002 .125
Preoperative 75% 75% 80% 70.6%
Postoperative 29.2% 25% 13.3% 47.1%
Straining
during
defecation P-value .002 .008 .002 .125
Preoperative 60.4% 62.5% 66.3% 52.9%
Postoperative 33.3% 25% 20% 52.9% Sexual
Disorders P-value .001 .031 .016 -

I ?
Table (2): Rectocele size before and after repair.
Preoperative Postoperative
Mean.
(cm) Minim. Maxim.
Mean
(cm) Minim. Maxim.
P-value
All patients.
(48)
3.79
? .819 2.4 5.5
1.23
?1.259 0 4 .001
Transperineal
repair patients.
(16)
3.8
? .983 2.4 5.4
.937
?.750 0 2 .001
Transperineal
with levator
repair patients.
(15)
4.18
? .770 3 5.5
.937
?.736 0 2 .001
Transrectal
repair patients.
(17)
3.45
? .536 2.9 5
2.08
?1.577 0 4 .002

I ?
Table (3): Rectocele evacuation before and after repair.
Preoperative Postoperative
Poor Moderate Subtotal Complete Poor Moderate Subtotal Complete P-value
All patients.
(48)
1
2.1%
15
31.3%
26
54.2%
6
12.5% 0
7
14.6%
10
20.8%
31
64.6% .001
Transperineal
repair
patients.
(16)
0 4
25%
7
43.8%
5
31.3% 0
1
6.3%
4
25%
11
68.7% .003
Transperineal
with levator
repair
patients.
(15)
1
6.7%
5
33.3%
9
60% 0 0
1
6.7%
1
6.7%
13
86% .001
Transrectal
repair
patients.
(17)
0 6
35.3%
10
58.8%
1
5.9% 0
5
29.4%
5
29.4%
7
41.2% .157
I ?
Table (4): Rectum evacuation before and after repair.
Preoperative Postoperative
Poor Moderate Subtotal Complete Poor Moderate Subtotal Complete P-value
All patients
(48)
10
20.8%
18
37.5%
20
41.7%
0
0
9
18.8%
5
10.4%
4
8.3%
30
62.5% .001
Transperi-
neal repair
patients.
(16)
2
12.5%
6
37.5%
8
50%
0
0
1
6.2%
3
18.8%
2
12.5%
10
62.5% .005
Transperi-
neal with
levator repair
patients.
(15)
4
26.7%
7
46.6%
4
26.7% 0
2
13.3% 0 0
13
86.7% .001
Transrectal
repair
patients.
(17)
4
23.5%
5
29.4%
8
47.1% 0
6
35.2%
2
11.8%
2
11.8%
7
41.2% .206

I ?
Table (5): Results of postoperative rectocele size in relation to improvement.
Improved Not improved
No Mean Minim Maxim No Mean Minim Maxim
P-value
All patients
(48) 30/48 .423
?.459 0 1.5 18/48
2.483
? .761 1 4 .001
Transperineal
repair patients.
(16) 10/16
.45
?.371 0 1 6/16
1.75
? .418 1 2 .001
Transperineal
with levator
repair patients.
(15)
13/15 .23
?.388 0 1 2/15 2 2 2 .01
Transrectal
repair patients.
(17) 7/17
.742
?.565 0 1.5 10/17
3.02
? .518 2.2 4 .001

I O
Table (6) Results of postoperative rectocele evacuation in relation to
improvement.
All patients.
(48)
Transperineal
repair.
(16)
Transperineal with
levator repair. (15)
Transrectal
repair.
(17)
Improved
patients
Complete 30 (100 %) 10 (100 %) 13 (100 %) 7 (100 %)
Poor 0 0 0 0
Moderate 7 (38.9 %) 1 (16.7 %) 1 (50 %) 5 (50 %)
Subtotal 10 (55.6 %) 4 (66.7 %) 1 (50 %) 5 (50 %) Not
improved
patients Complete
1 (5.6 %) 1 (16.7 %) 0 0
P-value
.001 .002 .001 .001

I ?
Table (7): anorectal manometric findings before and after rectocele repair.
Preoperative Postoperative
Mean Mean
P-value
MARP
(mmHg)
87.12
? 13
80.64
? 16.34
.001
UTDV
(ml)
225.41
? 25.76
199.47
? 33.5
.001 All Patients.
(48)
MRV
(ml)
225.83 ? 27.52 194.02
? 33.2
.001
MARP
(mmHg)
87.31
? 13.54
83.12
? 13.76
.035
UTDV
(ml)
223
? 30.74
196.56
? 36.08
.013 Transperineal repair
patients. (16)
MRV
(ml)
220
? 30.73
176.87
? 22.72
.002
MARP
(mmHg)
85
? 13.75
66. 4
? 14.59
.002
UTDV
(ml)
228
? 25.19
176.66
? 23.11
.001 Transperineal
With levator repair
patients. (15) MRV
(ml)
230.66
? 30.25
176.33
? 24.80
.001
MARP
(mmHg)
88.82
? 12.31
90.88 ? 10.64 .249
UTDV
(ml)
224.41
? 22.69
222.35
? 23.59
.350 Transrectal repair
patients. (17)
MRV
(ml)
226
? 22.14
225.35
? 25.37
.258

I ?
Table ( 8 ) : Results of postoperative anorectal manometric findings in relation to improvement of the three surgical repair patients.
Improved Not improved
Mean Mean
P-value
MARP
(mmHg)
75.7
? 15.84
88.88
? 13.99 .014
UTDV
(ml)
179.16
? 19.96
233.33
? 21.96 .001
All patients.
(48)
MRV
(ml)
178
? 22.99
220
? 31.34 .001
MARP
(mmHg)
81.5
? 10.81
85.83
? 18.55 .912
UTDV
(ml)
177.5
? 20.44
228.33
? 34.88 .006
Transperineal repair
patients.
(16)
MRV
(ml)
166
? 8.43
195
? 28.1 .025
MARP
(mmHg)
62.76
? 11.16
90
? 14.14 .032
UTDV
(ml)
170
? 16.2 220 .025
Transperineal with
levator repair patients.
(15)
MRV
(ml)
169.61
? 15.6
220
? 28.78 .026
MARP
(mmHg)
91.42
? 8.99
90.5
? 12.17 .692
UTDV
(ml)
198.57
? 12.14
239
? 11.97 .001
Transrectal repair
patients.
(17) MRV
(ml)
210.71
? 17.89
235
? 25.71 .34

? ?
Table (9): Comparison of three surgical procedures in relation to improvement.
Improved Not improved P-value
Transperineal with or
without levator repair
VS Transrectal
Repair.
23/31 (74.2%)
7/17 (41.2%)
8/31 (25.8 %)
10/17 (58.8 %) .024
Transperineal with
levator repair VS
Transrectal.
13/15 (86.7 %)
7/17 (41.2 %)
2/15 (13.3 %)
10/17 (58.8 %) .008
Transperineal without
levator repair VS
Transrectal.
10/16 (62.5 %)
7/17(41.2 %)
6/16 (37.5 %)
10/17 (58.8 %) .221







![Proctitis after stapled hemorrhoidopexy is an ... · obstructed defecation [16]. Surgical management is the main stay of treatment after failure of nonoperative options. PPH is associated](https://static.fdocuments.net/doc/165x107/5f0789f37e708231d41d7b92/proctitis-after-stapled-hemorrhoidopexy-is-an-obstructed-defecation-16-surgical.jpg)