
Rectal Cancer - 2005 M62 Coloproctolgy course, Huddersfield
92
Rectal Cancer - 2005 Coloproctolgy course, Huddersfi Lars Påhlman Dept Surgery, Colorectal unit University Hospital, Uppsala, Sweden
-
Upload
paula-harris -
Category
Documents
-
view
22 -
download
0
description
Rectal Cancer - 2005 M62 Coloproctolgy course, Huddersfield. Lars Påhlman Dept Surgery, Colorectal unit University Hospital, Uppsala, Sweden. Why focus on surgery ? The only curative option Big variation among surgeons Training mandatory - PowerPoint PPT Presentation
Transcript of Rectal Cancer - 2005 M62 Coloproctolgy course, Huddersfield
Rectal Cancer - 2005
M62 Coloproctolgy course, Huddersfield
Lars PåhlmanDept Surgery, Colorectal unitUniversity Hospital, Uppsala,
Sweden

Rectal Cancer - focus on surgery
Why focus on surgery ?
The only curative option Big variation among surgeons Training mandatory Surgical strategy important

Rectal cancer surgeryTwo main options
Local excision Abdominal resection

TEM surgery - adenomas
Transanal Endoscopic
Microsurgery
Full thickness excision
Up to 20 cm Perfect view

Rectal cancer surgeryLocal excision
T 1 tumours ‘Early’ T 2 tumours ‘Any T’ fragile patients TEM - technique crucial
Rectal cancer surgeryLocal tumour control
Mesorectum Lateral spread Intramural spread Implantation metastases Nodal involvement

Rectal Cancer - focus on surgery
Standard surgery
TME
the gold standard





Rectal cancer surgeryLateral resection margins
Local recurrences / number of patients
Pos. lat. marg. Neg. lat. marg.
11/13 (85%) 1/38 (3%)p < 0.001
Quirke et al. Lancet, nov 1; 1986

Rectal cancer surgeryIntramural spread
Hardly ever extend more than
0.5 cm
Grinell R. Surg Gynecol Obstet 99: 421-430; 1954

Swedish Rectal Cancer Register5 years follow-up (1995 - 97)
Local recurrence rate
Irrigation Ant. Resection Hartmann
Yes 96 / 1464 7 % 8 / 71 11 %
No 44 / 398 11 % 11 / 115 10 %
Unknown 7 / 65 11 % 1 / 17 6 %
p < 0.001 n.s.

Rectal cancer surgeryNodal involvement
Proximal Lateral Distal

Rectal cancer surgeryProximal lymph node clearance
High-tie
No effect on survival + nodes = disseminated disease
Grinell; Surg Gynecol Obstet 120:1031, 1965
Pezim and Nicholls; Ann Surg 200:729, 1984
Rectal cancer surgery
Lateral lymph node clearanceSuper radical surgery
Extended pelvic lymphadenectomy Retro-peritoneal clearance Extra mesenteric clearance
Hojo et al; Dis Colon Rectum 32:307, 1989

Rectal cancer surgery
Lateral lymph node clearanceSuper radical surgery
Positive nodes indicates disseminated disease
Hojo et al; Dis Colon Rectum 32:307, 1989
Rectal cancer surgery
Lateral lymph node clearanceMorbidity
Impotence > 60 % Voiding problem > 40 % Prolongs surgery
Rectal cancer surgery
Lateral lymph node clearanceThe pivotal trial !
TME + lateral LN clearance
vs
Neo - adj. irrad. + TME

Rectal cancer surgery
Distal lymph node clearance
Total mesorectal excision
How important ?
Heald et al; Br J Surg 1982

Rectal cancer surgery
Distal lymph node clearanceTotal Mesorectal Excision
In all cases ? What is the upper limit ? Morbidity increased !

Rectal cancer surgery
Low rectal cancersAbdominoperineal Excision
Very difficult surgery ! Important to have correct strategy Avoid ‘coning’ ! Start early from below !


Rectal cancer surgeryConclusion
Well - trained surgeons ! TME gold standard ! Lateral lymph nodes - radiotherapy APR very tricky ! Cone - effect must be avoided


Role of radiotherapy in rectal cancer
To lower local failure rates and improve survival in resectable cancers
To allow surgery in non-resectable cancers
To facilitate a sphincter-preserving procedure in low-lying cancers ?
To cure patients without (major) surgery
Resectable Rectal Cancer
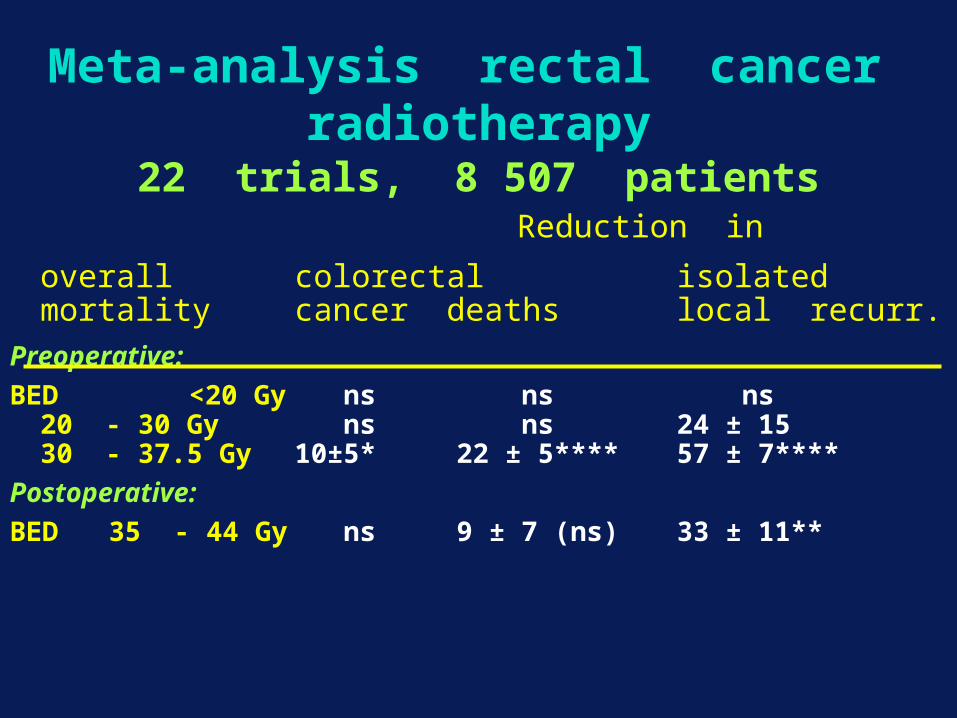
22 trials, 8 507 patients Reduction in
overall colorectal isolatedmortality cancer deaths local recurr.
Preoperative:
BED <20 Gy ns ns ns20 - 30 Gy ns ns 24 ± 1530 - 37.5 Gy 10±5* 22 ± 5**** 57 ± 7****
Postoperative:
BED 35 - 44 Gy ns 9 ± 7 (ns) 33 ± 11**
Meta-analysis rectal cancer radiotherapy
Radiotherapy in resectable cancerConclusions from the meta-analysis
Radiotherapy works (with standard surgery)lowers local failure ratesimproves survival
Dose-response relationship (for preop RT) low doses ineffective
Preop RT is more dose-efficient than postop seen in the Uppsala-trial comparing pre- and postop RT
Rectal Cancer Surgery
Neoadjuvant radiotherapy
will always reduce the
local recurrence rate with 50 %
Irrespective of type of surgery

Rectal Cancer Surgery
Type of surgery Local recurrence
RT - RT +
‘sloppy’ 30 % 10 %
TME 13 % 6 %

Adjuvant radiotherapyRadiation schedule
Conventional fractionation:45 - 50 Gy in 4 - 5 weeks
Accelerated fractionation:25 Gy in 1 week

Adjuvant radiotherapyOngoing trial in Sweden
3-armed trial
25 Gy / 1 week immediate surgery
25 Gy / 1 week delayed surgery
50 Gy / 5 weeks delayed surgery

Dutch trial - Local recurrence Patients with R 0 (n=1789)
5.8% vs 11.4% p < 0.001
Years since surgery
86420
Lo
cal r
ecu
rre
nce
(%
),20
,15
,10
,05
0,00
TME alone
RT + TME

Overall Survival eligible patients (n=1809)
Years since surgery
86420
Cu
m S
urv
iva
l
1,0
,9
,8
,7
,6
,5
,4
,3
,2
,1
0,0
64.2% vs 63.4% p = 0.87
TME alone
RT + TME

Cancer specific survival eligible patients (n=1809)
76.1% vs 73.0% p = 0.18
Years since surgery
86420
Ca
nce
r sp
eci
fic s
urv
iva
l1,0
,8
,6
,4
,2
,0

Dutch trial - Local recurrence rate
Level from the anal verge
10.5% vs 11.9% p = 0.53
Years since surgery
86420
Loca
l rec
urre
nce
(%)
,20
,15
,10
,05
0,00
Years since surgery
86420
Loca
l rec
urre
nce
(%)
,20
,15
,10
,05
0,00
Years since surgery
86420
Loca
l rec
urre
nce
(%)
,20
,15
,10
,05
0,00
0 - 5 cm 6 - 10 cm 11 - 15 cm

SWEDISH RECTAL CANCER TRIAL
Local recurrence rate (min. 5 years)
(patients operated on for cure)
Preop. irrad . Surgery alone p-value
Ant. res. 9 % (18 / 206) 21 % (41 / 194) < 0.001
Abd. per. 9 % (22 / 243) 25 % (65 / 256) < 0.001
Other op. 33 % ( 2 / 6 ) 38 % ( 3 / 8 )

Local recurrence rate
Trial / level Local recurrence
RT - RT + p value
SRCT < 5 cm 27 % 10 % 0.003 TME < 5 cm 11 % 12 % 0.53
SRCT 6 - 10 cm 26 % 9 % < 0.001 TME 6 - 10 cm 15 % 4 % < 0.001
SRCT > 10 cm 12 % 8 % 0.3 TME > 10 cm 6 % 4 % 0.15

Swedish Rectal Cancer RegisterData report
1995 - 2004
15,000 patients ( 1,500 yearly)
Base - line data Trends in treatment 5-year oncological data

Local recurrence % (1995 - 98)
All patients R 0 surgery
0 1 2 3 4 5
Överlevnadstid (år)
0
2
4
6
8
10
12
Ej preoperativ strålbehandling (1495 pat)Preoperativ strålbehandling (1353 pat)
0 1 2 3 4 5
Överlevnadstid (år)
0
2
4
6
8
10
12
Ej preoperativ strålbehandling (1981 pat)Preoperativ strålbehandling (1597 pat)
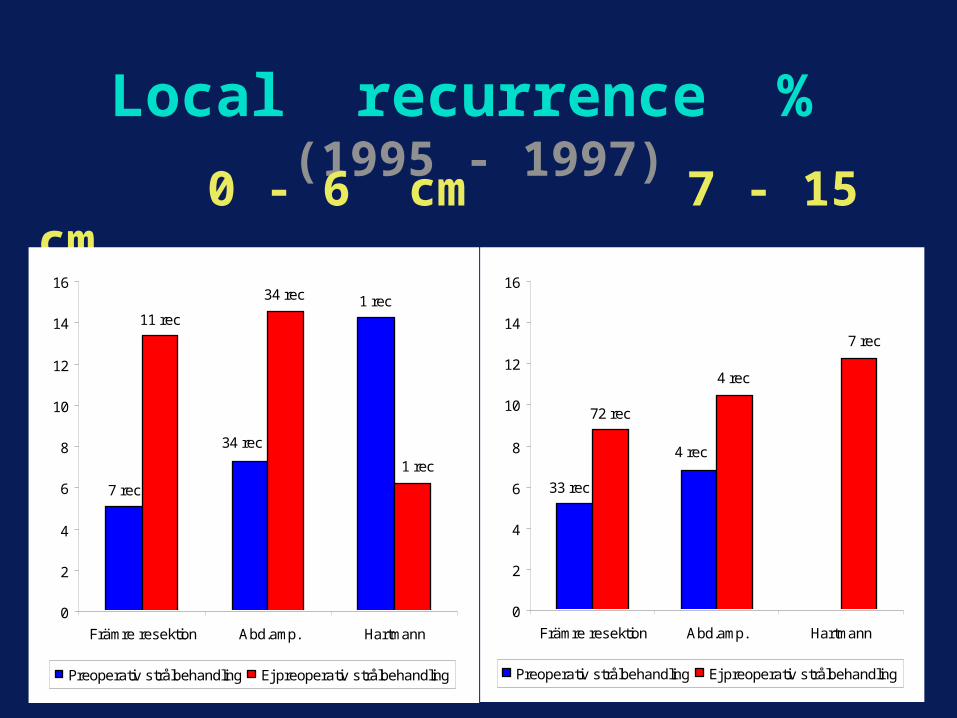
Local recurrence % (1995 - 1997)
0 - 6 cm 7 - 15 cm
7 rec
34 rec
1 rec11 rec
34 rec
1 rec
0
2
4
6
8
10
12
14
16
Främre resektion Abd.amp. Hartmann
Preoperativ strålbehandling Ej preoperativ strålbehandling
33 rec
4 rec
72 rec
4 rec
7 rec
0
2
4
6
8
10
12
14
16
Främre resektion Abd.amp. Hartmann
Preoperativ strålbehandling Ej preoperativ strålbehandling

Rectal cancer treatment - what have we learned ?
Local failures can more or less be eliminated; < 3 % (not only 10 %)
Survival slightly improved about 10 % with some morbidity (TME + RT)
The challenge is to preoperatively find those who need more than surgery and predict where the tumour cells are (to use radio-therapy on an individual level)

Preoperative chemo-radiotherapyin rectal cancer
Is RT/CT superior to RT in resectable rectal cancer ?
Probably, but the evidence is low
Two ! trials are ongoing (EORTC) (France)

Non - Resectable Rectal Cancer

Rectal cancerNon-resectable
Must be identified preop.
Malpractice if not treated with preoperative irradiation
Non-resectable rectal cancer No uniform definition
(T4’s growing into a another often non-resectable organ/tissue)
10 - 15%, half without distant metastases
Causes much suffering
Surgery alone likely cures very few
Preop. prolonged radio(chemo)therapy is mandatory

Non-resectable rectal cancer
Evidence for chemo-radiotherapy ?
one positive? randomised trial (Moertel 1969)
two negative randomised trials with increased toxicity (RTOG 1985, Danish 1993)
one positive? randomised trial (Swedish, 2001)
lots of phase II data (data are impressed !)
Non-resectable rectal cancerUppsala trial 1988 - 96
Prospective randomised trial
46 Gy
vs
40 Gy + MFL
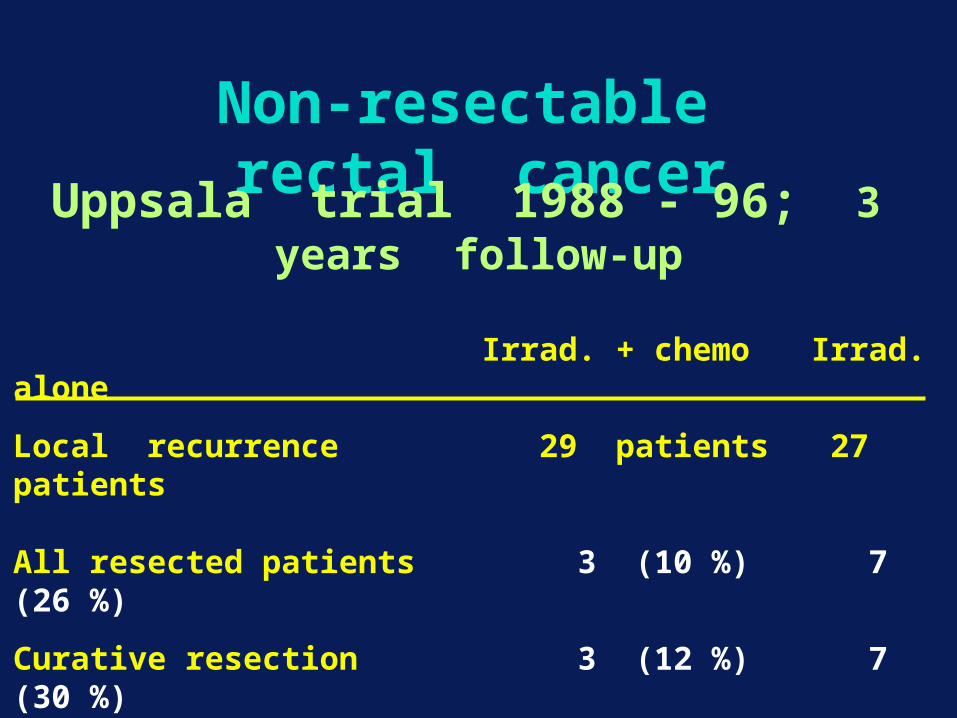
Non-resectable rectal cancerUppsala trial 1988 - 96; 3 years follow-up
Irrad. + chemo Irrad. alone
Local recurrence 29 patients 27 patients
All resected patients 3 (10 %) 7 (26 %)
Curative resection 3 (12 %) 7 (30 %)
Local control 26 (89 %) 20 (74 %)
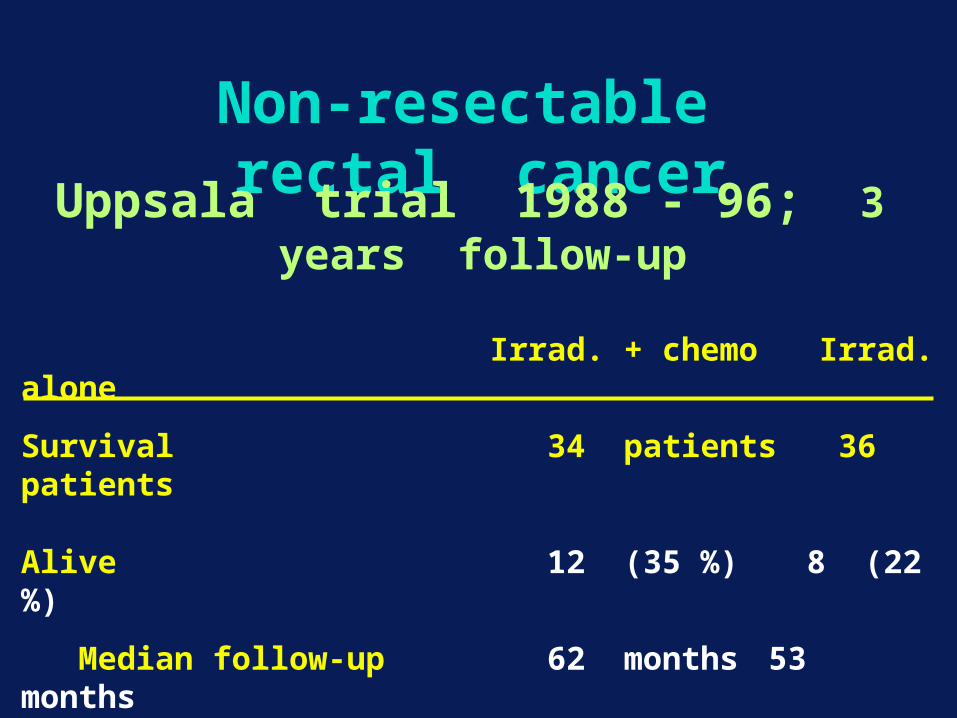
Non-resectable rectal cancerUppsala trial 1988 - 96; 3 years follow-up
Irrad. + chemo Irrad. alone
Survival 34 patients 36 patients
Alive 12 (35 %) 8 (22 %)
Median follow-up 62 months 53 months
Dead 22 (65 %) 28 (78 %)
Median survival 27 months 21 months
Non-resectable rectal cancerUppsala trial 1988 - 96
Conclusion
The trial was under-powered
Chemo-radiotherapy more toxic
A trend favouring irrad. + MFL

Non-resectable rectal cancer
Is RT/CT superior to RT in non-resectable rectal cancer ?
Probably, but the evidence is low
One ! trial is ongoing (Nordic)
Non-resectable rectal cancer
LARCS
Nordic prospective randomised trial
50 Gy (during 5 weeks)
vs
50 Gy + 5-FU / Lv
Non-resectable rectal cancer
Preop. prolonged chemo - radiotherapy
40 - 70 % resectable
20 - 30 % long-term cure

Sphincter Preservation

Adjuvant radiotherapy
Rectal cancer
Sphincter preservation
A myth or reality ?
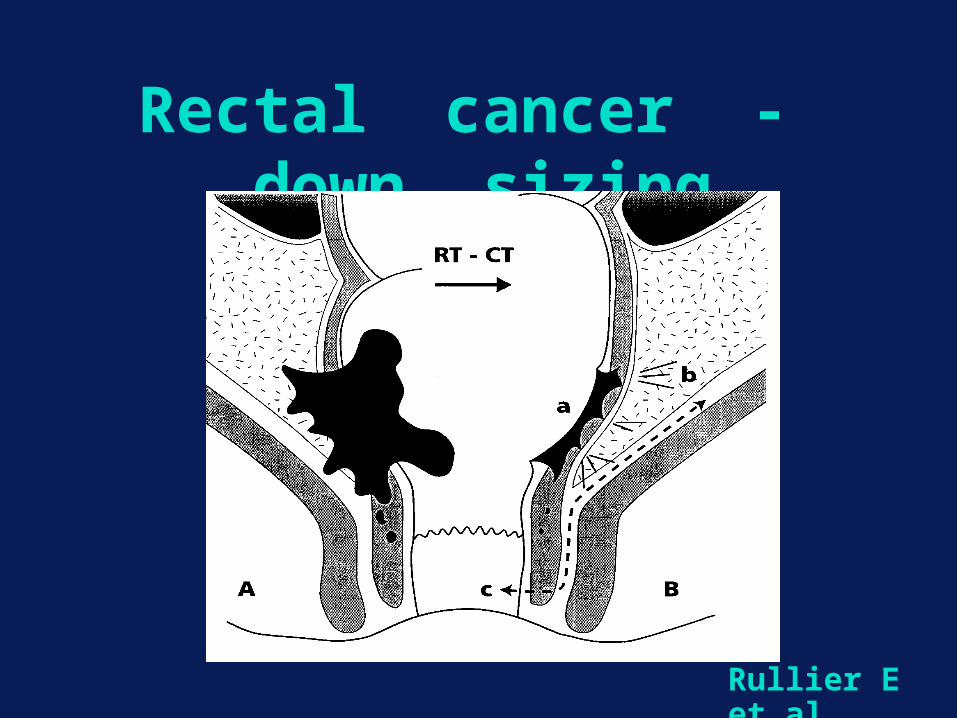
Rectal cancer - down sizing
Rullier E et al

The Lyon R90-01 Trial
Study design
T2- /T3- tumours
39 Gy (13 x 3 Gy)
Randomised to immediate surgery or surgery 5 weeks after irradiation
J Clin Oncol 1999; 17: 2396-2402

The Lyon R90-01 Trial
Study design
Surgeons where asked before any treatment to evaluate the possibility for performing a sphincter saving
procedure
J Clin Oncol 1999; 17: 2396-2402

The Lyon R90-01 Trial
Local recurrence
Overall 9 %
12 % in the group of patients where the surgeon had planned a
APR but it was changed after irradiation
J Clin Oncol 1999; 17: 2396-2402

CAO/ARO/AIO - trial in Germany
Trial design
Preop. chemorad.
Postop. chemorad.
Randomisation
Local
Recurr
Survival

CAO/ARO/AIO - trial in GermanyDown staging
Preop. chemorad. Postop. chemorad.
No tumour 8 % -
Stage I 26 % 18 %
Stage II 30 % 30 %
Stage III 29 % 43 %
Stage IV 6 % 8 %

CAO/ARO/AIO - trial in GermanyLocal recurrence rate
N Engl J Med 2004; 351: 1731-40

CAO/ARO/AIO - trial in GermanyOverall Survival
N Engl J Med 2004; 351: 1731-40

CAO/ARO/AIO - trial in Germany
Sphincter preservation
Preop. Postop.
chemorad. chemorad.
Preserved spincters 26/75 35 % 13/74 18 %
Total material 69 % 71 %
EORTC 22921 (1011 patients)
Trial design
Preop. Radiotherapy
45 Gy
Preop. chemorad.
45 Gy + 5-Fu/Lv
Randomisation
Local
Recurr
Survival

EORTC 22921 (1011 patients)
Down staging
Preop. irrad. Preop. chemorad.
Path. compl. resp 14 % 5.3 %
p < 0.001

EORTC 22921 (1011 patients)
Sphincter preservation
Preop. irrad. Preop. chemorad.
Ant. resection 55.6 % 52.4 %
p = 0.05

FFCD 9203 (762 patients)
Trial design
Preop. Radiotherapy
45 Gy
Preop. chemorad.
45 Gy + 5-Fu/Lv
Randomisation
Local
Recurr
Survival

FFCD 9203 (762 patients)
Down staging
Preop. irrad. Preop. chemorad.
Path. compl. resp 11 % 3 %
p = 0.05

FFCD 9203 (762 patients)
Sphincter preservation
Preop. irrad. Preop. chemorad.
Ant. resection 52 % 52 %
p > 0.05

Sphincter preservation - Polish trial
Trial design
Preop. chemorad. 25 x 2 Gy
Preop. radiotherapy 5 x 5 Gy
Randomisation
Local
Recurr
Survival
Sphincter
preserv
Sphincter preservation - Polish trial
Entry criteria
Tumour reached by digital exam but no sphincters infiltration
T3 and resectable T4
1 cm macroscopic distal margin is sufficient

Sphincter preservation - Polish trial
Sphincter preservation according to allocated radiotherapy
Planned 5x5 Gy RT/CT
APR 26 % 21 %
APR/AR 68 % 61 %
AR 85 % 88 %

Sphincter preservation - Polish trial
Sphincter preservation according to allocated radiotherapy
5x5 Gy N = 155 RT/CT N = 156
61 % 58 %

Adjuvant radiotherapy
Rectal cancer
Sphincter preservation
Still a myth ?

Neo - adjuvant radiotherapy
To whom ?
Better preop. staging !

Neo - adjuvant radiotherapy
Preop. local staging Rectal examination
Ultrasound
MRI

Neo - adjuvant radiotherapyRectal cancer
No preop. radiotherapy
Stage I tumours i.e. uT 1 or uT 2
Rectal Ultrasound very good
Neo - adjuvant radiotherapyRectal cancer
Preop. Short - term radiotherapy
Stage II and III tumours i.e. > uT 2
All APR´s
Rectal Ultrasound not so useful
MRI for the circumferential margin
Neo - adjuvant radiotherapyRectal cancer
Neo adjuvant chemo - radiotherapy
Large tumours i.e. advanced T 3 and T 4
Rectal Ultrasound not good
MRI best

Neo - adjuvant radiotherapyTo whom ?
Large bulky tumour
Narrow male pelvis
Tumours growing anteriorly
Abdominoperineal excision

Neo - adjuvant radiotherapyWhy APR´s ?
Very tricky surgery
A low cancer has the highest risk for lateral lymph node involvement
No anastomosis with less risk of late adverse effects
Neo - adjuvant radiotherapyRadiation biology
P 53 an important marker
A tumour with mutated P 53 responds less good to radiotherapy and 5-Fu based chemotherapy
Kressner et al, J Clin Oncol 1999
Neo - adjuvant radiotherapyConclusion
Tailored treatment based upon MRI and ultrasound Consider P 53 measurement Local recurrence rates (over all) should not be more than 10 % ! Local recurrence rates after R0 resections less than 3 % !

Rectal Cancer 2005Conclusion
Appropriate staging !
Consider radiotherapy !
Well trained surgeon !!
Chemotherapy ?


Colorectal Tripartite Meeting
Royal Dublin Society 5th-7th July 2005
Further details from www.tripartite.org.uk
Closing date for abstracts 10th December 2004


















