Pelvic bone tumor Quiz 3. Female 32 C/C: vague pelvic pain P/I: about 6-7 months ago.
Reconstruction of 3D Models from Medical Images: Application to Female Pelvic Organs
Soraia Pimenta, João Manuel R. S. Tavares, Renato Natal Jorge Faculdade de Engenharia da Universidade do Porto, Porto, Portugal
Fátima Alexandre IDMEC - Faculdade de Engenharia da Universidade do Porto, Porto, Portugal
Teresa Mascarenhas Hospital S. João - Faculdade de Medicina da Universidade do Porto, Porto, Portugal
Rania F El Sayed Faculty of Medicine, University of Cairo, Cairo, Egypt
ABSTRACT: Physical anatomic models obtained from medical images can be a powerful aid in the treatment of several medical situations. In this work, a complete methodology, from the acquisition of medical images to materialisation of three-dimensional models, with a particular emphasis on image segmentation techniques, was studied, developed and applied to organs of the female pelvic cavity. This methodology is presented in this paper, including several experimental results of each involved step.
Keywords: models; segmentation; 3D objects reconstruction; prototyping; pelvic cavity; pelvic organs.
1 INTRODUCTION
Physical models of anatomic systems, organs and tissues can be extremely useful tools in many com-plex medical situations, referring to knowledge ac-quisition, diagnostic, simulation and even treatment of the related diseases. In this work the reconstruction of three-dimensional models from medical images was applied to the fe-male pelvic cavity. The main objective was to study, develop, employ, test and compare some available approaches for the three-dimensional reconstruction and building of physical models for medical pur-poses.
2 FEMALE PELVIC CAVITY
The female pelvic cavity is an interesting and chal-lenging application for the reconstruction of virtual and physical models, both from medical and techni-cal perspectives, [1-3]. Pelvic floor dysfunction is consistently associated to urinary incontinence and pelvic organ prolapse due to injuries and deterioration of the muscles, nerves and connective tissues that support and control nor-mal pelvic organ function. The knowledge already achieved on the causers of pelvic floor disorders shows a great diversity of risk factors, as anatomic
predisposition, childbirth, muscular and general inju-ries, surgeries, and the simple ageing. Urinary Incontinence (UI) affects a large percentage of the adult world population, imposing significant adverse physical, psychological and financial effects on individuals, their families and caregivers (see Refs [1-3]). In the USA, studies show that more than 53% of the aged suffer from this disorder, and even among the people under 60 the incidence of the UI can reach 35%. Besides the decrease of the quality of life it imposes to the patients, the economic cost of the UI is very high, surpassing the 3500€ per pa-tient and year. In addition to these medical motivations, the female pelvic cavity also presents some characteristics that make it very interesting from technical point of view. In fact, pelvic cavity is a complex set of or-gans and tissues, presenting therefore some exam-ples of both easily and hardly extracted (segmented) structures from medical images, which allows a pro-gressive comprehension of the methodologies and procedures available to develop virtual and physical models as well as to identify their potentialities and limitations.
3 PROCEDURES
Usually, the methodologies used to obtain physical models of an anatomic structure represented in medical images follow a sequence of four funda-
mental procedures: 1) acquisition of the medical im-ages of the structure to be reconstructed, namely sets of 2D slices; 2) segmentation of the interesting or-gans in each 2D slice; 3) construction of virtual 3D models from the segmentation results; and, finally, 4) materialization of the physical models, for in-stance, by rapid prototyping.
3.1 Acquisition of medical images The acquisition of medical images, as the first stage of the process, has a preponderant role in the final result. In fact, the quality of the images of the struc-ture to be reconstructed will dictate the success of the segmentation process, which is a critical stage of the complete procedure. The medical images used in this work were acquired using systems of Magnetic Resonance Imaging (MRI). This radiology technique, characterized by the patient’s exposition to magnetic fields and radio waves, is capable of recognizing accurately complex and thin objects, and is therefore widely used for the pelvic cavity, [3].
3.2 Segmentation Image segmentation is usually the most complex procedure in the process of objects reconstruction from images, as it involves the identification of the shape to be extracted and its adequate partitioning in the image, in order to detach the same from its neighbourhood, [4-7]. This can be achieved using ei-ther manual or automatic methods, both presenting benefits and disadvantages. Manual segmentation consists in the manual draw-ing of the shape to be extracted from each medical image, using the image as background. This process can make use of the tools provided by specific soft-ware for analysis of medical images or by a general CAD software, but the effort to identify the contours is completely done manually. Therefore, this tech-nique is very versatile, but it demands a high man-power that might not be always available or justi-fied. Automatic segmentation avoids the greatest part of the manual process, as it appeals to the properties of the image to perform the identification of the shape to extract. The basic principles for automatic seg-mentation were established in [11], and are based on a dynamic contour that is attracted to the desired border of the object to be segmentd by the minimiza-tion of its energy, under image forces (such as image gradients). In addition, several other techniques were studied in order to develop different technologies to increase the potential of the automatic segmentation, as using, for instance, statistical pattern recognition
or 3D segmentation, [7]. Currently, the automatic segmentation is widely used in image processing, as it is very inexpensive both from time and manpower aspects. However, automatic segmentation procedures cannot be faced as universal solutions for all anatomical structures: although able to present reliable results and be very efficiently when applied to organs with high contrast in images, it is ineffective if the organs to extract are thin, complex and/or hardly distin-guished in the input images. Under these circum-stances, semi-automatic or even manual segmenta-tion is required, even though with a higher effort of the user and time consumption. As it can be easily understandable, the major prob-lem presented by the automatic methods for image segmentation is related to technical issues; it is sometimes very difficult to perform the segmenta-tion with good quality without the knowledge of an experienced professional about the object to be seg-mented. Therefore, and regarding the greatest advan-tages presented by the automatic segmentation in comparison to the manual procedures, the study and development of methodologies for automatic seg-mentation procedures is a field currently in high progress. As mentioned before, the female pelvic cavity pre-sents a high variety of organs and characteristics that influence the segmentation process. Therefore, in this work both automatic and manual image segmen-tation techniques were applied.
3.3 Virtual 3D models After the segmentation step, several 2D shapes rep-resenting the organ at different levels (slices) are available to be assembled in one 3D set; thus, the segmented contours are used to create a virtual three-dimensional body representing the extracted organ. In this work, the technique to create a virtual organ cannot be detached from the one applied at the seg-mentation step. In fact, if the segmentation is done, whether manually or automatically, using specific software for analysis of medical images, the extrac-tion of the organ from the set of images is com-pletely automatic, but the quality of the 3D model is not very high, especially in terms of smoothness. On the other hand, if the segmentation is done manually using a CAD software, the 3D model might need also some manual work to align correctly the several slices and to produce the correct surface; however, this process has two great advantages: its high flexi-bility (allowing the model to be iteratively improved even respecting the segmentation process) and the
high quality and smoothness of the 3D surface ob-tained. Besides its application to the production of physical models, virtual 3D models can also be used as inputs for visualization, simulation and computational analyses, for instances, to be used in biomechanics analysis using finite elements packages. This last technique is a very interesting tool to study the me-chanical behaviour of the muscles and tissues and damage resulting from several solicitations, provid-ing a non-invasive methodology useful for preven-tion and treatment of diseases; in addition, it can also be used to simulate corrective surgical proce-dures.
3.4 Physical 3D models Rapid prototyping is a modern technology especially indicated for production of prototype systems de-signed using CAD software. This technique uses the virtual 3D geometrical model to create a set of layers that will be materialized sequentially, creating a physical model almost identical to the virtual one. This process is recognizable for being flexible, fast and producing prototypes with a very good quality that can be transparent or coloured according to some purpose, which are fundamental requirements for the production of physical models of anatomical structures.
4 APPLICATION TO FEMALE PELVIC ORGANS
The previously exposed methodologies were applied in this work to female pelvic organs, using medical images obtained from one volunteer and one patient. When automatic image segmentation was possible, the commercial software for visualization and analy-sis of medical images Analyze 6.0, [8], was used for the whole process of the desired structures extraction from the input images. However, the pelvic floor proved to be impossible to segment automatically and, therefore, a different approach using the 3D CAD software Autodesk Inventor was applied, [9].
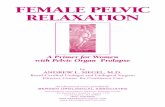
4.1 Bladder Bladder is probably the easiest organ of the human’s pelvic cavity to extract, because of its well defined contour and high contrast in the input medical im-ages. Therefore, an automatic segmentation tech-nique was successfully applied to this organ, using the tools provided by Analyze, Figure 1.
a) b)
c)
Figure 1 – Segmentation of the bladder: a) bladder repre-sented in a slice (white area); b) automatic segmentation obtained; c) virtual 3D model reconstructed. Although the results obtained with this process were considered adequate, for comparison purposes the manual technique (using the CAD software Auto-desk Inventor) was also applied, Figure 2. In this image, it is easily verified that the quality of the model obtained using manual segmentation is con-siderably superior, but the higher effort required by this image segmentation procedure makes of course the first solution much more attractive.
Figure 2 – 3D model obtained for the bladder using the manual segmentation technique.
4.2 Pelvic floor The pelvic floor is the main responsible organ for supporting the intestines, the bladder and the uterus. It is composed by muscle fibres, and is thus a very thin, heterogeneous and badly defined structure, very difficult to distinguish in medical images, Figure 3. Consequently, all the attempts to segment automatically the pelvic floor did not produce ac-ceptable results, so manual segmentation had to be applied.
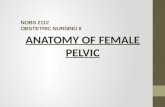
Figure 3 – An example slice showing the pelvic floor (sur-rounded in green). Although Analyze has the required tools for manual image segmentation also, they are not as powerful, flexible and user-friendly as the tools offered by common 3D CAD software to construct and manipu-late graphical entities (polylines, splines, bsplines, etc.), [9, 10]. Therefore, the segmentation of the pel-vic floor in the input images was achieved using the Autodesk Inventor software. The building of a 3D virtual model of this organ started with the adequate alignment of all medical images representing slices of the pelvic floor. After that, each slice was manually segmented using the Sketch tools (particularly Splines) of the Autodesk Inventor software, and then the corresponding 3D model was built using the Loft operation, that links all contours previously defined by an interpolate sur-face, Figure 4.
a) b)
c)
Figure 4 – Extraction of the pelvic floor: a) a set of slices; b) manual segmentation done in a slice; c) 3D virtual model obtained. Besides the advantage of producing very smooth models, this technique evidenced an extremely use-ful advantage in the creation of virtual models by
manual segmentation: its flexibility. With this pro-cedure, it is possible to create a rough model at first and then refine and correct it, improving the seg-mentation of several slices accordingly to the needs evidenced by the 3D model obtained, by a fully it-erative process. This flexibility is not possible using the usual medical software packages. Two virtual three-dimensional models of the pelvic floor obtained using the Autodesk Inventor software from images of different women, can be seen in Figure 5.
Figure 5 – Two virtual 3D models of the pelvic floors ob-tained using manual segmentation.
4.3 Urethra In terms of easiness of image segmentation and ex-traction, urethra is an intermediate case between the bladder and the pelvic floor: it has a regular and well defined shape, but its contrast in the input images, relatively to its neighbourhoods, is not very high. For that reason, and although it is not impossible to segment automatically the urethra, the manual pro-cedure previously described was applied, Figure 6.
a) b)
Figure 6 – Extraction of the urethra: a) manual segmenta-tion; b) 3D virtual model built.
5 CONCLUSION
The work described in this paper is an introduction to medical image processing and bioengineering ap-plied to the study of anatomic structures. It allowed the understanding of the basic concepts involved in the 3D reconstruction of organs and tissues from medical images, especially concerning the image segmentation process.
It was recognized that usual medical imaging soft-ware is a useful tool for those cases where automatic segmentation is possible, allowing a fast and effec-tive creation of 3D virtual models. However, when manual segmentation is required, the medical imag-ing software (Analyze 6.0, in this work) has not the required flexibility and, for that reason, the use of a common 3D CAD software may present important advantages in the segmentation process, and thus in the quality of the obtained final 3D models. Nevertheless, manual segmentation has a high cost, and therefore any effort to improve the automatic segmentation methodologies is a valuable help in this field.
6 ACKOWLEDGEMENTS
This work was partially done in the scope of the pro-ject “Segmentation, Tracking and Motion Analysis of Deformable (2D/3D) Objects using Physical Prin-ciples”, with reference POSC/EEA-SRI/55386/2004, financially supported by FCT – Fundação para a Ciência e a Tecnologia from Portugal. In addition, the support of Ministério da Ciência e do Ensino superior (FCT and FSE) (Portugal) and the funding by FEDER under grant POCTI/ESP/46835/2002, are gratefully acknowl-edged.
7 REFERENCES
[1] - T. Mascarenhas, R. Coelho, “Quality of life and psycho-logical factors of urinary incontinence”, Pelvic floor dys-function-Investigations and conservative treatment, 423-427, Italy, 1999.
[2] - L. Viktrup, G. Lose, M. Rolf, K. T. Barfoed, “The fre-quency of urinary symptoms during pregnancy and puer-perium in the primipara”, Int. Urogynaecology, 4:27-30, 1993.
[3] - L. Hoyte, “MR-Based 3D Female Pelvic Foor Anatomy”, USA, 2001.
[4] - Tim McInerney, D. Terzopoulos, “Deformable models in medical image analysis: a survey”, Medical Image Analy-sis, 1996
[5] - D. L. Pham, C. Xu, J. L. Prince, “Current Methods in Medical Image Segmentation”, Annu. Rev. Biomed. Eng. 2000. 02:315–37
[6] - A. Blake, Michael Isard, “Active Contours”, Springer-Verlag, 1998.
[7] - T. S.Yoo, “Insight into Images – Principles and Practise for Segmentation, Registration, and Image Analysis”, USA, 2004.
[8] - AnalyzeDirect, Inc – Mayo Clinic, “Analyze 6.0 - Users Manual”, USA, 2004.
[9] - J. D. Bethune “Engineering Design and Graphics with Autodesk Inventor(R) 10”, Prentice Hall, 2005.
[10] - G. Farin, “Curves and Surfaces for CAGD: A Practical Guide”, Academic Press, 2001.
[11] - M. Kass, A. Witkin, D. Terzopoulos, “Snakes: Active Countour Models”, Kluwer Academic Publishers, 1987.
1 INTRODUCTION2 FEMALE PELVIC CAVITY3 PROCEDURES3.1 Acquisition of medical images3.2 Segmentation3.3 Virtual 3D models3.4 Physical 3D models
4 APPLICATION TO FEMALE PELVIC ORGANS4.1 Bladder4.2 Pelvic floor4.3 Urethra
5 CONCLUSION6 ACKOWLEDGEMENTS7 REFERENCES
/ColorImageDict > /JPEG2000ColorACSImageDict > /JPEG2000ColorImageDict > /AntiAliasGrayImages false /CropGrayImages true /GrayImageMinResolution 300 /GrayImageMinResolutionPolicy /OK /DownsampleGrayImages true /GrayImageDownsampleType /Bicubic /GrayImageResolution 300 /GrayImageDepth -1 /GrayImageMinDownsampleDepth 2 /GrayImageDownsampleThreshold 1.50000 /EncodeGrayImages true /GrayImageFilter /DCTEncode /AutoFilterGrayImages true /GrayImageAutoFilterStrategy /JPEG /GrayACSImageDict > /GrayImageDict > /JPEG2000GrayACSImageDict > /JPEG2000GrayImageDict > /AntiAliasMonoImages false /CropMonoImages true /MonoImageMinResolution 1200 /MonoImageMinResolutionPolicy /OK /DownsampleMonoImages true /MonoImageDownsampleType /Bicubic /MonoImageResolution 1200 /MonoImageDepth -1 /MonoImageDownsampleThreshold 1.50000 /EncodeMonoImages true /MonoImageFilter /CCITTFaxEncode /MonoImageDict > /AllowPSXObjects false /CheckCompliance [ /None ] /PDFX1aCheck false /PDFX3Check false /PDFXCompliantPDFOnly false /PDFXNoTrimBoxError true /PDFXTrimBoxToMediaBoxOffset [ 0.00000 0.00000 0.00000 0.00000 ] /PDFXSetBleedBoxToMediaBox true /PDFXBleedBoxToTrimBoxOffset [ 0.00000 0.00000 0.00000 0.00000 ] /PDFXOutputIntentProfile () /PDFXOutputConditionIdentifier () /PDFXOutputCondition () /PDFXRegistryName () /PDFXTrapped /False
/Description > /Namespace [ (Adobe) (Common) (1.0) ] /OtherNamespaces [ > /FormElements false /GenerateStructure true /IncludeBookmarks false /IncludeHyperlinks false /IncludeInteractive false /IncludeLayers false /IncludeProfiles true /MultimediaHandling /UseObjectSettings /Namespace [ (Adobe) (CreativeSuite) (2.0) ] /PDFXOutputIntentProfileSelector /NA /PreserveEditing true /UntaggedCMYKHandling /LeaveUntagged /UntaggedRGBHandling /LeaveUntagged /UseDocumentBleed false >> ]>> setdistillerparams> setpagedevice