
Reconciling Medications Safe Practice Recommendations and Implementation Strategies.
58
Reconciling Medications Safe Practice Recommendations and Implementation Strategies
-
date post
20-Dec-2015 -
Category
Documents
-
view
218 -
download
0
Transcript of Reconciling Medications Safe Practice Recommendations and Implementation Strategies.

Reconciling Medications
Safe Practice Recommendations
and
Implementation Strategies

Medication Safety Facts
Medication errors account for more than 7,000 deaths annually
Approx. two out of every 100 patients admitted to the hospital will experience a preventable adverse drug event
Over 12% of patients with an ADE within 2 weeks of discharge

“Reconciling Medications”
A systematic process to reduce the number of medication events occurring at interfaces of careCreating the most complete and accurate list possible of all home medications for each patient and then comparing that list against the physician’s admission, transfer, and/or discharge orders. Discrepancies are brought to the attention of the physician and, if appropriate, changes are made to the orders. Any resulting changes in orders are documented.

RESEARCH:
Errors that are the result of an omission are often not reported as errors, although they may result in an adverse outcome for the patient.
They may manifest themselves as: Unexplained elevated lab values
Due to inaccurate dosing Missed medications
Readmissions due to: Doubling up of medications Missed medications at discharge Contraindication to unknown OTC or herbal meds

Problem identified
Info on patients’ home meds not being systematically collected; in multiple places in the chart, often incomplete
Poor or inadequate processes to compare list of pre-admit medications to orders
Research study demonstrated that over half of all hospital medication errors occurred at the interfaces of care[Rozich, Resar 2001]

Medication errors based on chart review
56%
21%
14%
9%
Interface Errors
Drug Distribution orDocumentation ErrorsAllergy Documentation
Others
Source: Luther Midelfort Hospital -- Mayo Health System chart review
“We found that the list of medications that details current drug use was either nonexistent or wrong more than 85% of the time” [Rozich/Resar 2004, p.8]

Examples of errors
No orders for needed home meds Missed or duplicate doses from inadequate
records of frequency/last administration time Surgeon inadequately addressing meds for
chronic conditions Failure to restart meds at transfers Doubling up (brand/generic combinations,
formulary substitutions)

Unintended medication discrepancies at admission
Studies show over half of patients have discrepancies between home medications and medications ordered at admission, many with potentially serious results 54% of patients; 39% potentially serious [Cornish Arch Intern Med 2005] More than half; 59% could have caused harm if the error continued after discharge [Gleason Am Jnrl H-Sys Pharm 2004]
More evidence on impact:Johns Hopkins Surgical ICU
Dramatic reduction in medication errors resulted from reconciling: Baseline: 31 of 33 (94%) of patients with MD
changing orders when discrepancies brought to their attention
By week 24, nearly all medication errors in discharge orders eliminated
As a result of routine reconciling, average of 10 orders per week are changed
[Pronovost, 2003]

The
Reconciling Process
THE PROPOSED SOLUTION
A process to obtain the best home medication list possible through a defined resource list and active review of the patient’s medical history.
Patient Pharmacy Family Patient’s Med List PCP VNA
Utilize strategic interviewing practices.
Ask open ended questions to obtain info on OTC meds & herbals.

Reconciling process: admissionGetting the home med list (at intake)
Interviewing strategies to promote accuracy Input from patient/family/alternative sources Outreach: patients arrive with accurate list
Writing medication orders Goal: work from accurate home med list
Identify and reconcile discrepanciesOrder (no omissions, no duplicates, right med/dose/
frequency/route)
Communicate (to next level of service)

BECOMING A STATEWIDE INITIATIVE The Massachusetts Hospital Association in
collaboration with the Massachusetts Coalition for the Prevention of Medical Errors reviewed evidence of medication reconciliation to determine:
Importance – How much can we impact safety? Feasibility – Is this a doable process? Measurability – Can we monitor our progress?
Statewide advisory board voted to accept this initiative!

Getting started
1) Initiate leadership dialog – resource commitment, regular reporting channels
2) Form a multidisciplinary team
3) Risk assessment/baseline measurement
4) Aim statement, timeline
5) Pick pilot unit
6) Begin testing

Define Aim / Obtain Baseline Measure
Aim: To reduce the rate of unreconciled medications
at admission by 50 % within 9 months. Measure:
Baseline measurement of 20 charts, subsequent measures performed on 30 charts per month for the first 3 months after implementation of form. Evaluate the frequency of the measure after the first three months.

1. Getting the home med list
What have we learned? Adopt standardized form Share responsibilities, ordering prescriber
accountable... crew resource management principles
Validate with the patient Don’t let perfection be the enemy of the good

1. Getting the home med list
Who? Shared responsibilities, always someone with sufficient expertise:
RN who completes the initial admission history Pharmacist/pharmacist technician
[Michels/Meisel 2003; Gleason/Groszek 2004]
MD if reconciling form not complete when ready to write orders

1. Getting the home med list
What? Current home meds Include OTCs & herbals Dose, frequency, time of last dose Optional: route, source of information, compliance,
purpose Many building collection of patient allergies into the
process
2. Using home list when writing orders
What have we learned? Make highly visible Provide access at point when orders are written Have reconciling form serve as an order sheet.
benefits and issues...

Project phasing
Pilot testing: identify changes, measure to know if the changes are an improvement
Implementation: take a successful change and build it into the way the entire pilot population/pilot unit does their work
Spread: replicating a change/package of changes beyond the pilot unit into other parts of the organization
Maintain the gains

3. Identifying, reconciling discrepancies
Who? Generally nursing assigned responsibility of
comparing the home list to the admit orders, identifying variances, and reconciling all differences
Pharmacist involvement can be productive, especially for organizations with decentralized pharmacy
Need strategy for handing off any unresolved differences at shift change

Implementation Strategies

Resource requirements
During testing/implementation phase Make explicit allocation for those with patient care
responsibilities Managers need to pay attention to workloads; don’t
assign tests to someone overloaded Ongoing
Build into regular workflows Collecting home history IS time consuming; some
have added resources to support that (e.g. pharmacy techs)

Post Team Members- Encourage Input
Contact any of the following Medication Reconciliation PI Team members to answer any of your questions:
Melissa Bartick, MD - X9335 Jennifer Fexis, Quality - X9406 Darlene Civita, RN ICU- X9350 Vicky Casto, RN ACU - X9335 Deb Wilkinson, RPh - X9363

Tips for engaging MDs
Personal appeals from VP of Medical Affairs and/or Chiefs of services
Trial with key leaders on each unit; get their input via “hallway consultations” not meetings
Identified “Ambassadors” from engaged hospitalists; they then educated others
Developed into CME risk program MDs from key committees (P&T, Medical Records)
Chief Medical Resident on the team, with responsibility to report back to other residents

Baseline risk assessment
Chart review Institution-wide
Mini-FMEA, flow charting existing processes
Do in conjunction with initial tests of change
Just-enough measurement/analysis Don’t get bogged down here!!

Mission
Every patient will receive all medications they have been taking at home unless they are held/discontinued by their caregiver(s) and all new medications as ordered -- correct drug, dose, route, and schedule.
The goal of reconciling is to design a process that will ensure the most accurate patient home medication list available, thus reducing the number of medication events upon admission, transfer and discharge

Choosing where to start
Use risk assessment process Willing volunteers At admission logical place
Pros & cons: Med vs Surg units Some success starting @ transfer: ICU,
CCU, telemetry units Probably not ED

Start small, focus on one unit
Small tests... 1 unit, 1 RN, 1 MD, 1 patient Add more staff, more shifts, refining process and form Keep testing on that one unit until you refine the
process and can show that it works (test on all shifts, patients coming in as direct admits, from ED, transfers, etc)

Pilot unit
1) Mini-team including nurse managers, front-line nurses, MD champion
2) Project introduction, staff education
3) Baseline measurement for the unit4) Pick reconciling form to test (steal shamelessly...)
5) Begin testing

Piloting a reconciling form
Testing; avoid forms committees... Simple vs complex
Reconciling status Orders: continue, change, d/c, hold Optional: data sources, purpose/indication,
date/time of last dose, amt of non-compliance Columns for reconciling at discharge? Signature lines



Get support of your CEO; cannot do it without leadership at the top
Use data (to motivate, to know if changes are leading to improvement)
Strong representation from leadership of the 3 key stakeholder groups: MD, RN, pharmacy
Start small
Fundamental ingredients...

Culture...
Core issues of teamwork and communi-cation... organizational culture matters
Changing the way people do work; every time you try to change behavior, it’s only natural to be met with resistance Recognize that this is HARD;
Difficult task: but not impossible Unit briefings/pharmacy rounding


Challenges and barriers
Time and resources “How can we find the time to do this?”
Roles and responsibilities “It’s not my job” “I’m not going to sign that form”
Data collection Need data... but don’t let data collection delay
testing, overwhelm

Medication ChecklistHere’s how patients can help the ‘medication reconciliation’ process:
Keep an updated list of all medications including herbals, vitamins and OTC. Including dosage and reason for taking the drug
Include all allergies and describe reaction Include immunization history Take the list to all doctor visits and medical testing labs, as
well as pre-assessment visit for admission or surgery and all hospital visits including ER
When you leave the hospital, be sure to update your list with new medications and ask if any medications are duplicated
Keep this list in with you at all times

Staff education
Include staff ed rep on your team Create simple template clarifying the steps to be taken to
complete reconciling Lead off with examples of errors from your own hospital Use front line staff from pilot unit to educate staff on
subsequent units Build into orientation, ongoing staff ed Publish your data and progress in your organizations
newsletter
Measurement

Just-enough measurement
Core measure Percent Medications Unreconciled
Orders changed, “great catches”, stories Measures linked to each test, for example:
% patients with reconciling form in chart RN/MD assessments of process
Spread: % patients on units w/ reconciling Context of institution-wide ADE reduction

# Medications Unreconciled(per 100 Admissions)
0
50
100
150
200
250
300
1/5/
98
1/12
/98
1/19
/98
1/26
/98
2/2/
98
2/9/
98
2/16
/98
2/23
/98
3/2/
98
3/9/
98
3/16
/98
3/23
/98
3/30
/98
4/6/
98
4/13
/98
4/20
/98
4/27
/98
5/4/
98
5/11
/98
5/18
/98
5/25
/98
6/1/
98
6/8/
98
6/15
/98
6/22
/98
6/29
/98
7/6/
98
Admission reconciliation
Transferreconciliation
Dischargereconciliation
Luther Midelfort Implementation Impact

Baseline data collection
GOAL: Identify current safety risks
How complete is info on patient’s pre-admission meds? How hard to find? In multiple places?
How often are home meds omitted from admit orders? not re-started after transfer, at discharge? duplicate therapies at discharge?

Example: Why is it Needed?
In a chart review of our admit orders, we found an average of over 4 discrepancies per patient, with omitted medications the most significant error.
Source: University of Kansas Hospital
Terry Rusconi [2003]
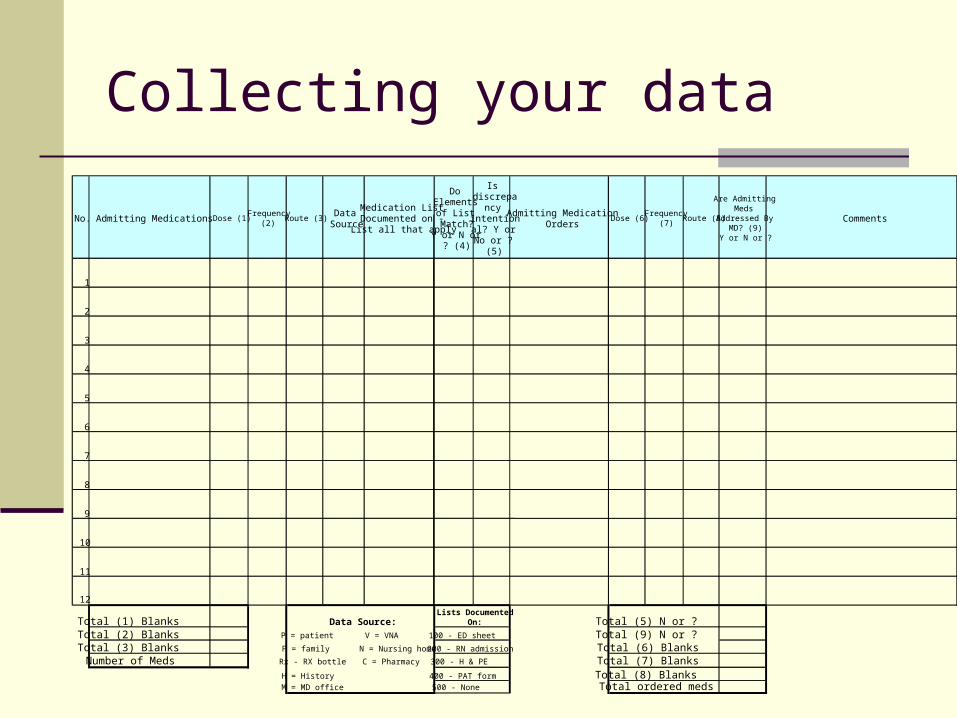
Collecting your data
No. Admitting Medications Dose (1)Frequency
(2) Route (3)
Data Source
Medication List Documented on - List all that apply
Do Elements
of List Match?
Y or N or ? (4)
Is discrepa
ncy intentional? Y or No or ?
(5)
Admitting Medication Orders
Dose (6)Frequency
(7)Route (8)
Are Admitting Meds
Addressed By MD? (9)
Y or N or ?
Comments
1
2
3
4
5
6
7
8
9
10
11
12
Total (1) BlanksTotal (2) Blanks P = patient V = VNA 100 - ED sheet Total (9) N or ?Total (3) Blanks F = family N = Nursing home 200 - RN admission Total (6) BlanksNumber of Meds Rx - RX bottle C = Pharmacy 300 - H & PE Total (7) Blanks
H = History 400 - PAT form Total (8) Blanks M = MD office 500 - None Total ordered meds
Lists Documented On:Data Source: Total (5) N or ?

12345678910111213141516171819202122232425262728293031323334353637383940414243444546
A B C D E F G
Chart Review
Total Admission Medications
Total Blanks (1) (2) (3)
Number of Discrepancy's (5)
Number of Admitting Meds Not Addressed by
MD (9)Total Ordered Medications
Total Blanks (6) (7) (8)
1 5 0 2 1 5 02 1 3 1 1 4 03 13 10 2 2 11 34 10 12 0 0 9 05 2 2 0 0 7 06 10 30 0 0 9 07 13 13 2 0 13 38 7 3 0 0 8 09 9 0 3 0 8 0
10 10 14 2 1 10 211 13 4 0 0 19 1912 10 0 0 0 11 013 0 0 8 8 8 014 12 23 4 5 9 015 11 16 10 1 10 1016 15 6 11 0 18 217 10 14 10 7 3 418 9 4 3 1 12 619 11 15 6 10 6 020 2 2 1 1 5 0
Sum 173 171 65 38 185 49Summary Statistics - Admit Orders
# discrepancy errors: Sum of (5) 65# patients: # charts reviewd: 20Discrepancy errors/100 admissions: 325Average error per patient 3.25
Summary Statistics- H & P
# reconciliation errors: Sum of (9) 38# patients: # charts reviewd: 20Reconciling errors/100 admissions: 190Average error per patient 1.9
Summary Statistics - Admit Orders
# dose, freq, route omission errors: Sum of (C) 171
Total admission medications: Sum of (B) 173
Admitting Omission errors?100 admissions 99
Average error per med 0.99
Summary Statistics - H & P
# dose, freq, route omission errors: Sum of (G) 49
Total ordered medications: Sum of (F) 185
Order Omission errors?100 admissions 26
Average error per med 0.26

Baseline: practical process
Multidisiplinary team of reviewers RN, MD, Pharm... QI rep to combine
Minimum 20 charts Institution-wide, random or stratify to ensure all
units represented Minimum stay of 3 days Can be fruitful to include re-admits
Find home meds and list on form Compare to admit orders Identify “unreconciled medications”

Ongoing data collection
Need frequent measurement on every unit where you are testing: monthly charts to display on unit
Process: easy for patients where the reconciling form has been completed; follow process used in baseline data collection when no reconciling form
DON’T CHEAT: Don’t skip patients without a reconciling form Don’t just look for home med list; the question is,
have the home meds been RECONCILED?

TIPS on collecting your data...
Share responsibilities, engaging implementers Limit sample: 20 charts Real-time review: patients on unit for 24 hours Establish rules for consistent treatment where judgment
required (omission or obvious hold or d/c based on patient condition; but strategy should encourage increased documentation by prescriber)
Set time limit (when unable to find home meds, use list from admit orders and indicate that all are unreconciled)
Share “Great Catches”: examples of orders changed, errors prevented

Beyond Admission
and
Longer-term Considerations

Reconciling at Transfer
Compare most recent med record (MAR) and home med list against transfer orders. Issues:
Access to reconciling form with home med history at point when new orders written
Need to modify reconciling form to add columns for reconciling at transfer?
Identifying responsibilities of both the transferring and the receiving unit
Embedding into workflow: Who writes transfer orders? When? Where?

Reconciling at Discharge
Patients especially vulnerable immediately post-discharge Over 12% of patients with an ADE within
2 weeks of discharge [Forster 2003] Address potential for doubling up based
on formulary substitutions or other brand/generic name confusions
Prohibit “resume home meds”!!! Verification of dosing instructions

Outpatient Settings
Applies to settings where the outpatient: may receive medication where patient's response to treatment might be
affected by medications they are on where a practitioner who can review and modify the
patient's medications is a part of the outpatient service
Examples include outpatient oncology services, GI laboratories, emergency department, urgent care clinics, certain imaging procedures.

Using as an order sheet
Proceed with caution, but efficiency gains Most MDs find it very helpful; makes their life
easier, decreases duplication Timing: 6-10 months into the process? Modifications to reconciling form:
Add MD signature line(s) Columns to indicate “continue” or “discontinue” Amendment form

Automation
If you can’t do it on paper,
don’t even try it in vapor First must have a stable process: adequate
testing of the form, implementation on multiple units
Careful design required; who enters info, who can update/change, may introduce new errors

Automation: John Hopkins ICU project Revised form to strike balance between
burden of data collection and comprehensiveness of medication information
Automated process after 48 weeks, paper forms converted to electronic form
Intervention now takes 20 minutes on admission and 20 minutes at discharge with minimal marginal costs
Better access to medication histories
Promote patients maintaining medication cards Provide in ED, at discharge Disease specific support groups Pharmacy medication review Senior center (file of life) Partner with PCPs, nursing homes, VNA,
health plans

Better access to medication histories
Interview strategies including increased use of open ended questions
Link medications to conditions, prescribing physicians
Checklists of OTCs/herbals and commonly missed meds
Leverage expertise of VNAS Shared databases


















