Recognizing Rift Valley Fever · described in Egypt and also an ocular syndrome with macular...
23
Introduction Rift Valley Fever (RVF) is an acute arthropod- borne virus infection with a wide range of vertebrate disease hosts. This is a zoonotic disease problem. Until relatively recently, the range of RVF had been confined to the Ethiopian faunal region of Africa, but the disease was identified in Egypt in 1977 and in the Arabian Peninsula in 2000. The virus is a member of the Phlebovirus genus of the Bunyaviridae family. It is an RNA virus, which is related to some other members of the group by haemagglutination or by indirect fluorescent antibody tests at low titres and from which it may be readily distinguished by virus-serum neutralization tests. The virus is transmitted by mosquitoes of at least six genera and probably over 30 different species. It is transmitted transovarially by some of the Aedes spp. of the Neomelaniconium group of mosquitoes. These are floodwater breeding species, which emerge in enormous numbers in floodplains and other habitats where they oviposit. The disease was first recognized and characterized in the Great Rift Valley in Kenya in 1931 - hence its name - although it may have occurred earlier. Several thousand ewes aborted and there was 90 percent mortality in young lambs. While the problem was first identified in sheep, cattle were also affected, although the abortion rates and mortality in calves were much lower. The affected animals were of breeds that had been imported from Europe or elsewhere into Africa to improve livestock production. Indigenous breeds on adjacent farms were unaffected. A further point of some interest was that humans associated with the affected animals suffered an influenza-like disease with fever, headaches and muscle and joint pains. The investigations carried out during this outbreak showed that the disease was being transmitted by mosquitoes. The movement of livestock to the top of the escarpment above the Rift Valley resulted in a cessation of transmission and no new cases of the disease since the location is at a much greater Recognizing Rift Valley Fever F. Glyn Davies 1 & Vincent Martin 2 Veterinaria Italiana, 42 (1), 31-53 1 Consultant, EMPRES/Infectious Diseases Group - FAO, Viale delle Terme di Caracalla - 00100 Rome - Italy 2 Animal Health Officer, EMPRES/Infectious Diseases Group - FAO, Viale delle Terme di Caracalla - 00100 Rome - Italy 31 © IZSA&M 2006 www.izs.it Vol. 42 (1), Vet Ital The Rift Valley
Transcript of Recognizing Rift Valley Fever · described in Egypt and also an ocular syndrome with macular...
Introduction
Rift Valley Fever (RVF) is an acute arthropod-borne virus infection with a wide range ofvertebrate disease hosts. This is a zoonoticdisease problem. Until relatively recently, therange of RVF had been confined to the Ethiopianfaunal region of Africa, but the disease wasidentified in Egypt in 1977 and in the ArabianPeninsula in 2000. The virus is a member of thePhlebovirus genus of the Bunyaviridae family.It is an RNA virus, which is related to someother members of the group byhaemagglutination or by indirect fluorescentantibody tests at low titres and from which itmay be readily distinguished by virus-serumneutralization tests. The virus is transmittedby mosquitoes of at least six genera and probablyover 30 different species. It is transmittedtransovarially by some of the Aedes spp. of theNeomelaniconium group of mosquitoes. Theseare floodwater breeding species, which emergein enormous numbers in floodplains and otherhabitats where they oviposit.The disease was first recognized and characterizedin the Great Rift Valley in Kenya in 1931 - henceits name - although it may have occurred earlier.Several thousand ewes aborted and there was90 percent mortality in young lambs. While theproblem was first identified in sheep, cattlewere also affected, although the abortion ratesand mortality in calves were much lower. The
affected animals were of breeds that had beenimported from Europe or elsewhere into Africato improve livestock production. Indigenousbreeds on adjacent farms were unaffected. Afurther point of some interest was that humansassociated with the affected animals sufferedan influenza-like disease with fever, headachesand muscle and joint pains. The investigationscarried out during this outbreak showed thatthe disease was being transmitted by mosquitoes.The movement of livestock to the top of theescarpment above the Rift Valley resulted in acessation of transmission and no new cases ofthe disease since the location is at a much greater
Recognizing Rift Valley Fever
F. Glyn Davies1 & Vincent Martin2
Veterinaria Italiana, 42 (1), 31-53
1Consultant, EMPRES/Infectious Diseases Group - FAO, Viale delle Terme di Caracalla - 00100 Rome - Italy2 Animal Health Officer, EMPRES/Infectious Diseases Group - FAO, Viale delle Terme di Caracalla - 00100 Rome - Italy
31© IZSA&M 2006 www.izs.it Vol. 42 (1), Vet Ital
The Rift Valley

altitude with few insect vectors present.Subsequently the disease has been recognizedin an enzootic or epizootic form in many tropicaland subtropical African countries, and inMadagascar. However, the absence of anylivestock disease problems has resulted in fewsearches for RVF virus activity in many othercountries in Africa. In some of these countries,clinical RVF has not been encountered, eitherin humans or animals, and yet there is evidenceof the existence of a cryptic cycle for RVF virusmaintenance involving mosquitoes and variousvertebrate hosts. Sporadic human cases havesometimes been encountered.Subsequent RVF epizootics were experiencedin South Africa in the 1950s, when huge losseswere sustained in the wool sheep populations,and subsequently in most of the neighbouringsouthern African countries. Epizootic RVF hasbeen seen in the Sudan, at the Gezira irrigationscheme in 1973-74 and in Egypt in 1977-79 and1993-94, where hundreds of thousands of humancases were reported, with at least 600 deaths.A highly fatal haemorrhagic syndrome wasdescribed in Egypt and also an ocular syndromewith macular degeneration, in some cases leadingto blindness. There were enormous losses insheep, goat and cattle populations, with abortionin camels. In Mauritania and Senegal, there wasan epizootic associated with the creation of abarrage on the Senegal River in 1987-88. Bothhumans and animals were affected and, in thisinstance, neurological signs were detected inhumans. In 1997-98, a major epizootic of RVFoccurred, which affected countries in the Hornof Africa. There were hundreds of human cases,with some mortality, and abortion storms andneonatal deaths in domestic animals, includingcamels. This was probably the most dramaticepisode of RVF ever encountered.
In 2000, RVF was recognized in humans andanimals in the Arabian Peninsula. Both Yemenand Saudi Arabia simultaneously experiencedan epizootic, which principally involved theTihama region of the country, adjacent to theRed Sea. The Red Sea forms the floor of the RiftValley in this region and the Tihama is the floorof the Rift in the east with an escarpment runningfrom north to south 40-70 km inland. There weresome 100 human fatalities and many thousands
of deaths and abortions in domestic animals.RVF is one of the most significant zoonoticdisease problems in Africa. The occurrence ofthe highly fatal haemorrhagic human diseasesyndrome, similar to Ebola and otherhaemorrhagic fevers, generates a degree of panicamong the human populations at risk. RVF ishighly contagious for humans if animals areviraemic at the time of slaughtering. However,one of RVF’s greatest impacts is upon trade inlivestock. Even if the disease tends to disappearafter epizootics, livestock bans may last forseveral years, severely affecting the livelihoodof pastoralists. Indeed, viraemic animals constitute
32 Vol. 42 (1), Vet Ital www.izs.it © IZSA&M 2006
Recognizing Rift Valley Fever F. Glyn Davies & Vincent Martin
Saudi Arabia: typical swamp area susceptible
to mosquito breeding during the epidemic

a serious hazard during epizootic periods andall trade in livestock from the affected countriesand their neighbours ceases. In the pastoralregions of eastern Africa, incomes are almostentirely derived from the sale of mature malesheep and goats for the religious festivals inMecca. Cessation of this trade has had disastrouseffects upon the livelihood of highly vulnerablepopulation groups.RVF also has the potential to extend its rangeto other receptive regions to the north andnortheast outside Africa, such as theTigris/Euphrates Delta zone, which would bereceptive for RVF virus transmission. Delta areassuch as the Indus in the Indian subcontinentare also at risk. Aerial transport of vectors andincreased animal movements facilitate theintroduction of the disease.
Nature of the disease
Rift Valley fever is a zoonotic disease, whichaffects humans, ruminants and camels. It maymanifest itself as a fatal haemorrhagic diseasesyndrome in humans, either as sporadic casesor during a major epizootic involving animals.
There may also be many severeinfluenza/malaria-like cases, some with ocularor neurological lesions. Hepatitis is a feature ofboth human and animal RVF cases. In animals,RVF manifests itself with a sudden onset ofabortion in a large proportion of the herd/flock,
associated with high neonatal mortality. Clinicalexamination of individual animals reveals abiphasic febrile reaction with severe prostrationand collapse in young animals, agalactia in milkanimals, lymphadenitis, debility with jaundiceand deaths in older age groups.RVF is caused by an arbovirus of the genusPhlebovirus of the Bunyaviridae family. The virusreplicates in mosquitoes and in vertebrates. Ithas a lipid envelope and two surface glycoproteinsG1 and G2; the genome has three segments L,M and S. Genetic characterization suggests thatall strains are closely related but there are someregional differences, suggesting two or threeregional virus types. The RVF virus is serologically
33© IZSA&M 2006 www.izs.it Vol. 42 (1), Vet Ital
Recognizing Rift Valley FeverF. Glyn Davies & Vincent Martin
Trade of livestock between the Horn of Africa
and the Arabian Peninsula (Port of Berbera,
northern Somalia)
RVF virus
CAUSES · An arbovirus
· Phlebovirus
· Bunyaviridae
· RNA virus

resistant to RVF compared with cattle.Human disease has frequently been the indicatorsystem signalling epizootic RVF virus activityin many African countries. This is particularlythe case in semi-arid and arid zones such as theHorn of Africa, Sahelian West Africa and theArabian Peninsula.Horses experience an infection that is inapparentwith RVF. There is a brief period of viraemiaand the antibody develops. Pigs are relativelynon-susceptible, but do respond with a viraemiaafter a high titre parenteral inoculation withRVF virus. Poultry and wild birds are non-susceptible to RVF.
Geographic Distribution
Rift Valley fever has occurred in:• the sub-Saharan region of Africa• Egypt
• the Arabian Peninsula - Yemen and Saudi Arabia• Madagascar
The natural distribution of RVF is throughoutthe Ethiopian faunal region of sub-SaharanAfrica. In Saudi Arabia and Yemen, the ecologyof the RVF-affected Tihama regions (eastern RiftValley zone) is identical with those of the westfloor of the Rift Valley in Ethiopia and Eritrea,across the Red Sea. The occurrence of RVF inEgypt in 1977 was thought to result frommovement of the infection from RVF enzooticareas in Africa to the south. This may or maynot be the case. There are descriptions in theBible of a plague in Egypt, which clinicallyappears very similar to RVF.Throughout much of its range, RVF virus infectionremains cryptic. Evidence of its existence maybe found in sporadic cases of human disease,virus isolation from mosquito pools or serumantibody prevalence to RVF of 2-15 percent ormore in domestic animals. Such virus activitytakes place with no manifestation of clinicaldisease in these animals.
34 Vol. 42 (1), Vet Ital www.izs.it © IZSA&M 2006
Recognizing Rift Valley Fever F. Glyn Davies & Vincent Martin
Typical ecosystem close to the mountains
where RVF was prevalent in Saudi Arabia in
2000

35© IZSA&M 2006 www.izs.it Vol. 42 (1), Vet Ital
Recognizing Rift Valley FeverF. Glyn Davies & Vincent Martin
related, by Immunofluorescence Assay Test(IFAT) and inhibition of haemagglutination(IHA), to some other Phleboviruses from SouthAmerica, but can be readily distinguished fromthese by virus-serum neutralization tests, whichare specific. There is only one serological andimmunological type of RVF virus.Sheep, goats, cattle and camels are the domesticanimal species most affected by RVF. However,there is considerable variation in the levels ofsusceptibility of the different breeds to the virus,from infections that are inapparent and haveno sickness or febrile reactions, to hightemperatures, severe prostration and death inanimals that are most susceptible. In general,
breeds that are non-susceptible are thoseindigenous to the tropical and subtropical zonesin Africa, while those highly susceptible are theEuropean or imported genotypes exotic to thecontinent. Birds and pigs are not affected.The small ruminants in the arid and semi-aridecozones, where RVF virus activity only occursafter long intervals, appear to be more susceptiblethan the sheep and goats in the Guinean andSudanese zones of Africa. RVF virus activityoccurs more frequently in the Sudan.The indigenous cattle breeds show a markedresistance to RVF, compared with importedbreeds. There may be no abortions in pregnantcattle in indigenous herds while there are highabortion rates in exotic breeds on the same farm.RVF infection in adult camels can manifest itselfas a clinical disease, with abortion rates thatmay reach 100 percent of pregnant animals.Some neonatal mortality may occur in camelfoals.Primates, rodents and carnivores are susceptibleto experimental infections with some deaths,but no mortality has been observed in the wild.The many wild ruminant species in Africa sustaina brief period of viraemia and abortions havebeen reported. The African buffalo (Syncerus
caffer), for example, develops a transient viraemiaand may abort. Many wild ruminant specieshave antibodies to RVF virus and show evidenceof contact with the virus. The Asian water buffalo,Bubalis bubalis, appears to be relatively resistantto RVF, but specific antibodies to RVF have beendocumented. Buffalo herds mixing with cattlethat evidence high abortion rates caused byRVF, have a much lower number of abortions.Some neonatal mortality and abortions inbuffaloes were attributed to RVF during theEgyptian RVF outbreak. Although this may havebeen true, buffaloes still appear to be relatively
1977 outbreak in Egypt: petechialhaemorrhages and hyphema in a woman’sface
ANIMALS AFFECTED• Sheep, goats and cattle
• Camels
• Buffaloes (mild)
• Carnivores (dogs, cats) and rodents
(viraemic)
• Other primates - usually subclinical
• Horses (inapparent)

RVF manifests itself as a serious disease problemfor livestock production systems in those countrieswhere exotic breeds of sheep, goats and cattlehave been imported. Such highly susceptibleanimals then act as an indicator host system forRVF virus activity, since they show obvious
signs of disease. Regions such as East Africa(Kenya, the United Republic of Tanzania andUganda) and southern Africa (Zambia, Zimbabweand South Africa) have introduced such bloodlinesand have been most severely affected. Manyother neighbouring countries have also imported
36 Vol. 42 (1), Vet Ital www.izs.it © IZSA&M 2006
Recognizing Rift Valley Fever F. Glyn Davies & Vincent Martin
ECOLOGICAL CONSIDERATIONS THE WADI BIOTOPE IN THE ARABIAN PENINSULA
The Tihama describes the whole of the coastal plain in the Arabian Peninsula in the west and southwest
of Saudi Arabia and Yemen. It consists of low hillocks bordering the north-south mountain chain.
Wadis or river valleys occur in the Tihama and constitute the alluvial floodplains of the rivers as they
emerge from the mountains. These soils are sands, loamy silts and clays, of very low salt content, with
little humus or nitrogen. The first ecozone is of Panicum and Cyperus grasslands, which are seasonally
flooded. In many areas, terraced catchments have improved the utilization of water from the rivers at
these points. The second and larger zone borders the rivers as they proceed to the sea, and consists of
Acacia zizyphispina and Dobera spp., with some grasses and bare earth. The riverine zones are
characterized by the presence of Dactyloctenium grasses and are altered in some wadis by lateral canal
systems extending north and south of the rivers. The rivers are seasonal in flow, largely fed by the
mountain catchment areas, and are dry for much of the year. Towards the sea is a belt of land with a
high salt content, planted with Salsola spp.
The Tihama biotope has been the focus of extensive agricultural development over the last 20 to 30
years as greater use is made of the available water resources for cultivation. These changes have a direct
impact upon the environment, creating a more extensive habitat for RVF virus mosquito vectors. In
Yemen, for example, the largest wadi (Wadi Mawr) covers some 18 000 hectares watered by the canal
systems.
The methods used for the utilization of the spate flow in the wadis are very similar in Saudi Arabia
and Yemen. Agriculture is practised in the riverine alluvial deposits and surrounding sandy soils.
Water flow is directed by channel systems into field units, and new areas are flooded sequentially.
Together with the rainfall, this results in many large and small water pools suitable as breeding sites
for certain mosquito species.ù
The changes in the wadi systems, which have been made to ensure more effective use of the available
water, are also those that favour the development of more extensive breeding sites for the mosquito
species that are believed to be of greatest importance in amplifying and transmitting the RVF virus.
Additional ecozones where primary RVF virus amplification may take place following the emergence
of Aedes mosquitoes are in the wet highland plateau grasslands planted with Acacia combretum and
allied species. These are found in Thaiz and Ibb Governorates and possibly also in Sa’dah. The virus
may also be expected to occur along the wadi river beds far up into the mountain zones, especially
where these broaden out into alluvial plains with pockets of clay soil.

exotic ruminants at different times and haveexperienced RVF problems. Epizootic RVF diseasealso occurs in domestic animals in the arid andsemi-arid Sahelian zones in the north and southof the continent; they appear to be moresusceptible than those in bushed and woodedgrasslands and forest zones. Animals, particularlysheep, goats and camels have been affected inthe Sudan, Mauritania and Senegal. They sufferabortion storms but at lower levels than theexotic breeds - usually 5-40 percent abortionrates in small ruminants and low levels or noabortions in cattle. Some neonatal mortalitymay also occur.Camels are probably the best animal indicatorhost system for RVF in the arid and semi-aridzones of Africa. Virtually all pregnant femalesare likely to abort if there is a high level of RVFvirus amplification associated with extensiveflooding in the riverine floodplains. Surveillancefor RVF should be established in areas to thenorth of the existing epizootic range for thedisease. Areas considered to be at high risk forthe extension of RVF are the Tigris/EuphratesDelta in Iraq/Islamic Republic of Iran and all
irrigation project zones in Arabian countries,whether wellhead, oasis or catchment systemsfor water conservation are utilized. Further east,the riverine delta systems in Pakistan and Indiamay be considered potential extension zonesfor RVF, although at a lower level of risk thanthose mentioned above because of their greaterdistance from the enzootic areas and the prevailingwind currents and trade in animals.
37© IZSA&M 2006 www.izs.it Vol. 42 (1), Vet Ital
Recognizing Rift Valley FeverF. Glyn Davies & Vincent Martin
Theoretical cycle of RVF virus transmission
CAUSES OF TRANSMISSION• By mosquitoes
• Primary vectors - Aedes spp. of the
Neomelaniconium group
• Many secondary vectors - Culex,
Anopheles, Aedes (Stegomyia),
Mansonia, Eretmopodites species
• Some mechanical spread - Culicoides
spp. and other biting flies
• Not spread by animal to animal contact
• Aerosol of blood from infected tissues
such as foetuses/slaughtered infected
animals, to humans
• Meat at time of slaughter

38 Vol. 42 (1), Vet Ital www.izs.it © IZSA&M 2006
Recognizing Rift Valley Fever F. Glyn Davies & Vincent Martin
Transmission and spread
As stated previously, RVF is an arbovirus,transmitted transovarially by Aedes mosquitoesof the Neomelaniconium group. These mosquitoesbreed in the temporary floodwater pools andfloodplains that occur throughout the range ofthe Rift Valley. They are found in tropical forest,Guinean and Sudanese zones and out into thesemi-arid and arid zones wherever these areassociated with alluvial riverine floodplains.Flooding is clearly dependent upon rainfallpatterns and occurs frequently in the moist highrainfall zones and infrequently in the arid andsemi-arid zones. However, forest zones whereannual or biannual emergence of RVF virusinfected vectors may occur, do not havesusceptible disease hosts to act as indicators ofRVF virus activity. These are found principallyin the bushed and wooded grasslands and semi-arid zones, which occur throughout the Africancontinent to the north and south.It is in the latter zones that RVF is an epizooticdisease problem. Epizootic virus activity hasbeen associated with periods of more thanaverage persistent heavy rainfall. This raisesthe water table to a level where the water pans,
dambo, walo or dieri, as they are called in differentparts of the continent, are flooded. These floodslast for several weeks. Riverine floodplains maybe flooded as a result of distant rainfall in theircatchment areas and not as a result of local rains.This flooding results in the emergence of a singlegeneration of Aedes (Neomelaniconium)mosquitoes, such as A. lineatopennis, macintoshi
and vexans. A proportion of these mosquitoesmay be infected with the RVF virus and seedthe virus in ruminants or camels that are exposedwhen they drink from or feed close to the waterpools. Whether these infections generate intoepizootics depends upon the water poolsremaining for four to six weeks or more, thusenabling the secondary vector mosquitoes tobreed rapidly and generate the huge mosquitopopulations seen during RVF epizootic periods.These mosquitoes are of several genera: Culex,
Anopheles, Aedes (Stegomyia) and Mansonia. It isalso known that other biting flies may transmitthe RVF virus mechanically. The mostpredominant “flying needles” are likely to beCulicoides spp., Stomoxys spp. and tabanids.Glossina spp. (tsetse flies) can also transmit RVFmechanically.
Spread of RVF
The climatic conditions that predispose majorRVF epizootics are likely to be of a regionalnature. Determinants of climate such as theintertropical convergence zone (ITCZ) arecontinental features. This explains thesimultaneous multifocal origin of RVF duringthe early days of an epizootic. The disease doesnot spread in the manner of classical contagiousdiseases. It occurs in several countries in a regionat one and the same time. Some local spreadmay occur from the initial foci through the
Flooded dambo in Kenya

movement of infected vectors, but epizooticRVF virus activity requires the presence of hugenumbers of vectors and the potential for this tooccur is clearly limited.The disease persists for periods of 8-16 weeks,when the infection rate may decline anddisappear. The full epidemic curve is oftencompleted in 16-20 weeks in semi-arid and aridsituations but cases may continue to occur forone to two years in more temperate coastal ormoist highland areas.RVF has not been known to spread by themovement of infected animals from infected touninfected areas. However, in theory this couldhappen and has in fact been put forward as themechanism for the occurrence of the disease inEgypt and the Arabian Peninsula, although thereis no evidence to support this idea. Theglobalization of trade and the reduction intransportation times have also created newpossibilities of disease spread that must be takeninto consideration in the epidemiology oftransboundary animal diseases.Direct animal to animal or contact transmissionof RVF has been difficult to demonstrate. Thereis no evidence from the field that this transmissionroute is significant in epizootics. Movement ofa flock of infected and susceptible sheep awayfrom the mosquito challenge results in thecomplete disappearance of RVF within days.RVF is a vector-propagated virus disease inanimals.
Signs of Rift Valley Fever
RVF epizootics may develop after the climaticchanges described in the previous chapter,usually associated with persistent heavy rainfalland flooding and subsequent occurrence of hugemosquito populations. The onset of disease is
sudden and dramatic. The initial signs willdepend upon the breed and genotype of thetarget animals. However, a sudden onset ofabortions among sheep, goats, cattle or camelsover a wide area is probably the most significantsign. There will also probably be sudden deathsand disease with many fatalities in all species,especially in the early post-natal period. Nearly100 percent of young lambs of susceptible breedsmay die. Older animals at one to four monthsmay suffer an acute febrile disease withprostration and 10-40 percent fatalities. Adultanimals in a milking herd show a febrile diseasewith agalactia. Some deaths occur, however, inall age groups. Young adult exotic sheep, for
39© IZSA&M 2006 www.izs.it Vol. 42 (1), Vet Ital
Recognizing Rift Valley FeverF. Glyn Davies & Vincent Martin
Ewe aborting as a result of RVF
CLINICAL SIGNS OF RVF• Sudden onset of abortion storms
• Up to 100 percent mortality in lambs
under five to six days old
• High fever, lymphadenitis, nasal and
ocular discharges in mature animals
• Profuse fetid diarrhoea (often
haemorrhagic)
• Vomiting, abdominal colic
• Severe prostration, dysgalactia, jaundice
• Epizootic period of 8-16 weeks

40 Vol. 42 (1), Vet Ital www.izs.it © IZSA&M 2006
Recognizing Rift Valley Fever F. Glyn Davies & Vincent Martin
example, may die with acute hepatitis andjaundice. The simultaneous occurrence of aninfluenza-like disease among people workingwith livestock is an additional feature of RVFepizootics.It should be noted that resistant genotypes ofindigenous African cattle and sheep often showno clinical signs of illness, despite having a briefperiod of viraemia. However, in some situationsthe cattle or sheep will have abortions that maybe wrongly diagnosed. The abortion rate mayreach 30 percent of the flock in small ruminantspecies, but is rarely more than this in indigenousbreeds.RVF in sheep and goatsThe clinical signs of RVF in sheep and goatshave been classified into four groups accordingto the severity of the disease. These arehyperacute, acute, subacute and inapparent.Each group is considered separately. In general,goats are less severely affected than sheep, with
much lower morbidity and mortality, with fewerabortions and less severe clinical signs.Hyperacute RVF
Susceptible sheep breeds may suffer 90-100percent abortion during periods of intense RVFvirus transmission in epizootic situations. Some80-100 percent of lambs under ten days of age,which are born during such periods, die fromRVF. Most deaths are sudden and occur within12 hours after the onset of a pyrexia (40-42°C).Collapse and death are all that may be seen.Other lambs may be depressed, too weak tosuckle or stand, and die within 24-48 hours,without showing clinical disease other thanfever, an elevated respiratory rate and prostration.Acute RVF
Older lambs, from two to three weeks of ageand all susceptible breeds, may show severeclinical signs with high fever and an elevatedrespiratory rate, mucopurulent or sero-sanguineous nasal discharges, injectedconjunctivae, vomiting and often abdominalpain.A generalized lymphadenitis and gaitabnormalities may be detected. Animals aredisinclined to move, become recumbent andoften develop a haemorrhagic diarrhoea, andabortion. Deaths occur after 24-48 hours andmay continue throughout the flock for up to tendays. Mortality rates may be from 10 to 60percent. Sick and recovering animals generallyshow moderate to severe signs of jaundice.Subacute RVF
This is more frequent in adult animals. A febrilereaction develops of 40.5- 42°C and persists forone to five days. Anorexia, injected conjunctivae,nasal discharges, vomiting and other signs areseen but are generally less severe than in younganimals. Abortion is a feature, as is diarrhoea.The colic may be less obvious, there may be
Abortion resulting from RVF infection

some lack of coordination of movement, animalsare weak or recumbent for several days but mostrecover. Many will be jaundiced and may remainunthrifty and weak for several months. Themortality rates are of the order of 5-20 percent.Inapparent RVF
This occurs in older or resistant animals. Theremay be transient periods of fever, which are notdetected. The fever may be accompanied bydepression or a brief period of inappetence,which are unremarkable. These infections areonly detected by subsequent serological testing.Abortions may, however, follow such infections.
RVF in cattleHyperacute RVF
Calves under ten days of age may suffer fromthis form of the disease and die within 20-24hours with few, if any, premonitory signs. Signsthat may be observed are sero-sanguineous nasaland lachrymal discharges, an elevated respiratoryrate and a temperature of 41.5-42°C. Totalprostration occurs with the animal lying on itsside, with opisthotomus and progressivelygreater respiratory distress. The course of thedisease is rapid and death occurs within 48hours. Up to 70 percent mortality has beenexperienced in genetically susceptible breeds.Acute RVF
Older calves, yearlings and even adult animalsshow a high febrile reaction of 41.5-42°C, nasaland lachrymal discharges that may be blood-tinged, partial or total anorexia, some depressionand possibly prostration. The animals may havecolic with a profuse fetid haemorrhagic diarrhoeathat persists for several days. A moist coughmay develop with evidence of respiratory distressand rhales. The superficial lymph nodes generallybecome enlarged and there is a dysgalactia inmilking animals. Animals may haemorrhage
from the mouth or nose. Abortion commonlyoccurs. The temperature reaction and sicknessmay persist for three to ten days during whichmany animals die. Jaundice developssubsequently and, if this is severe, furthermortality occurs.Animals of any age, from three months to matureadults, may show all or some of the above signsand experience mortality, most commonly inthe younger age groups. Mortality varies from10 to 40 percent, depending on the age groupsexposed. From 5 to 10 percent mortality hasbeen experienced among older cattle of susceptiblegenotypes.Subacute RVF
Older cattle generally show a less obviousresponse to RVF, which may be manifest as abrief period of temperature rise, with nasal andlachrymal discharges and a dysgalactia of threeto seven days duration. There may be a briefperiod of profuse watery diarrhoea, oftenaccompanied by colic. Some respiratory signsmay be noticed, a raised rate and a moist coughwith some rhales. Abortion is perhaps the mostcommon consequence and this may occur duringthe acute phase of the disease or up to six toeight weeks later. Some deaths may occur. Apersistent ill thrift may follow such mild infections,which is usually associated with moderate tosevere jaundice and liver damage.Photosensitization is a common sequel to RVFvirus infections.Inapparent RVF
RVF is usually inapparent in the majority of theadult susceptible and indigenous bovids inAfrica, which are relatively resistant to RVF.Abortion may follow this infection in thesusceptible genotypes but is rare in the indigenousanimals in the classical RVF enzootic zones ofthe continent. This is the most common
41© IZSA&M 2006 www.izs.it Vol. 42 (1), Vet Ital
Recognizing Rift Valley FeverF. Glyn Davies & Vincent Martin
presentation of RVF in epizootics, where onlya retrospectively noted fall in milk production,abortions and serological testing reveal the trueextent of the infections.
RVF in camelsCamels do not normally show any clinicalsigns following RVF infections and fall intothe inapparent infection group. They have abrief period of viraemia. Abortion is a commonconsequence of the infection, however, andpastoralists complain of “all their camelsaborting”. The infections can be confirmedserologically. Deaths do occur in the earlypost-natal period in camel foals born duringRVF epizootic periods, probably as a resultof RVF.
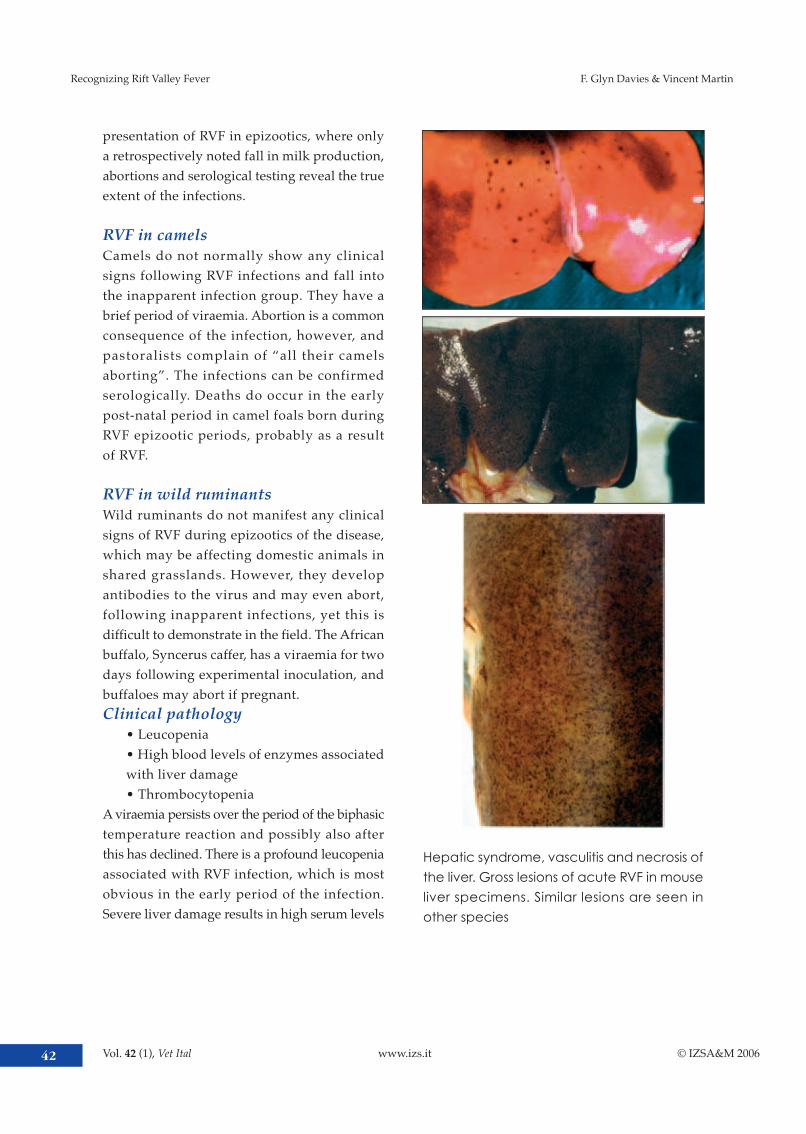
RVF in wild ruminantsWild ruminants do not manifest any clinicalsigns of RVF during epizootics of the disease,which may be affecting domestic animals inshared grasslands. However, they developantibodies to the virus and may even abort,following inapparent infections, yet this isdifficult to demonstrate in the field. The Africanbuffalo, Syncerus caffer, has a viraemia for twodays following experimental inoculation, andbuffaloes may abort if pregnant.Clinical pathology
• Leucopenia• High blood levels of enzymes associatedwith liver damage• Thrombocytopenia
A viraemia persists over the period of the biphasictemperature reaction and possibly also afterthis has declined. There is a profound leucopeniaassociated with RVF infection, which is mostobvious in the early period of the infection.Severe liver damage results in high serum levels
42 Vol. 42 (1), Vet Ital www.izs.it © IZSA&M 2006
Recognizing Rift Valley Fever F. Glyn Davies & Vincent Martin
Hepatic syndrome, vasculitis and necrosis of
the liver. Gross lesions of acute RVF in mouse
liver specimens. Similar lesions are seen in
other species

of the enzymes associated with this pathology,e.g. glutamic dehydrogenase (GLDH).Postmortem signs of RVF
• Liver enlargement and necrosis, initiallyfocal then often pannecrosis• Liver congestion, then later a bronze toyellow colour• Petechial and ecchymotic haemorrhagesthroughout the carcass• Often severe haemorrhagic gastroenteritis• Generalized lymphadenopathy• Pulmonary oedema and emphysema• Similar pathology in foetus, with autolysis
The most important pathological changes areto be found in the liver. The severity of thelesions that develop will depend upon the agegroup and susceptibility of the animals affected.They are likely to be more severe in young lambsand less severe in older animals.Hepatic necrosis is present in all RVF carcasses,for the lesions develop early in the course ofthe disease. In the early stages the liver iscongested, swollen and engorged with roundededges and many scattered petechialhaemorrhages. Later, the necrosis may be evidentas small 1-3 mm foci, which coalesce to formlarger areas of necrosis and these changes involve
43© IZSA&M 2006 www.izs.it Vol. 42 (1), Vet Ital
Recognizing Rift Valley FeverF. Glyn Davies & Vincent Martin
Haemorrhage and bloody discharge from
nostrils
Intestine showing petechial haemorrhages
on the serosal surface
Mucosal haemorrhages in the abomasum
Haemorrhagic and oedematous lymph node

the whole of the liver.There may be widespread petechial andecchymotic haemorrhages throughout theparenchyma and visible in subcapsular tissues.The necrotic changes induce jaundice and astage is reached when the liver has a bronzeappearance as the congestion, necrotic areasand icterus develop. At later stages the liverwill be completely yellow with jaundice.Petechial and ecchymotic haemorrhages maybe found throughout the carcass in lambs. Theyare especially noticeable on the serosal andpleural surfaces of the body cavities, and on theheart, gall bladder, kidneys, bladder and otherorgans. There may be some bloodstained asciticfluid.The alimentary tract usually shows some levelof inflammation from catarrhal to haemorrhagicand necrotic. The serosal surfaces may havehaemorrhages and also the mucosal lining ofthe bowel, particularly of the abomasum andsmall intestine and ileo-caecal areas.The lungs may be congested with oedema andemphysema and subpleural haemorrhages arecommonly found. The heart will showsubepicardial and endocardial haemorrhages.There is a generalized lymphadenopathyinvolving the superficial and visceral lymphnodes. These are oedematous with petechialhaemorrhages.The spleen may or may not be enlarged withsubcapsular haemorrhages.
Similar changes will be found in the foetuses,particularly of the liver where various levels ofnecrosis will be seen. There is also a necroticplacentitis.
Differential diagnosis
Single cases of RVF can be confused with manyviral diseases, which cause sudden death insheep and produce generalized lymphadenopathyand petechial and ecchymotic haemorrhagesthroughout the carcass. However, RVF manifestsitself in a dramatic fashion with the following:
• a sudden onset of many abortions at allstages of pregnancy; these may affect anextensive area or be countrywide• an acute febrile disease with high fatalityrates in young animals• liver lesions are present in all cases• associated with high mosquito populationsand/or flooding of grasslands
44 Vol. 42 (1), Vet Ital www.izs.it © IZSA&M 2006
Recognizing Rift Valley Fever F. Glyn Davies & Vincent Martin
Varying levels of liver necrosis produced by
RVF infection• Nairobi sheep disease - no hepatitis, not
in newborn lambs
• Bluetongue - mouth and foot lesions
(coronitis)
• Heartwater - serous fluids in body cavities;
neurological signs
• Ephemeral fever - recumbency and rapid
recovery
• Wesselbron - rare viral disease, less severe
than RVF
• Toxoplasmosis, leptospirosis, brucellosis,
Q fever, salmonellosis - basic diagnostic
methods for differentiation
• Peste des petits ruminants - high mortality
in lambs
• Foot-and-mouth disease - neonatal
mortality and abortions in small ruminants

•may be associated with an influenza-likedisease in humans.
The diseases that may be manifested in thismanner are described below.Nairobi sheep disease causes abortions, highfatality rates and produces gastroenteritis insheep and goats. This does not show a higherpathogenicity for neonates, however, which isa feature of RVF, and while it does cause abortions,these and the clinical disease are of a moresporadic nature. Deaths are usually in olderanimal age groups, and the carcasses have similarhaemorrhages, but there is no hepatitis.Bluetongue causes a febrile disease oftenwith diarrhoea, but also causes muzzleoedema and mouth lesions, which will beobvious in some cases. Hyperaemia anderosion of the buccal mucosae, lameness andcoronitis with skin hyperaemia will assist
in making a clinical differentiation. Suddendeaths at the viraemic stage producegeneral ized petechial and ecchymotichaemorrhages, which on postmortem appearsimilar to RVF. There is no hepatitis.Heartwater can cause sudden death withlymphadenopathy and generalized haemorrhagesthroughout the carcass. There is no hepatitisand usually the fluid in the serous cavities willbe excessive and obvious. Neurological signscan be seen. Brain smears can be prepared tomake a definitive diagnosis.Ephemeral fever produces a clinical syndromein dairy cattle that is very similar to RVF. Thereis a sudden onset of fever of a similar nature toRVF but generally more severe. The dysgalactiathat occurs is the same, together with nasal andocular discharges. However, the muscle weaknessand recumbency, which are a feature of ephemeral
45© IZSA&M 2006 www.izs.it Vol. 42 (1), Vet Ital
Recognizing Rift Valley FeverF. Glyn Davies & Vincent Martin
Varying levels of liver necrosis produced by RVF infection

fever cases, do not occur with RVF. Ephemeralfever does not produce any disease in sheep,goats or young cattle.Wesselbron virus has been confused with RVFin South Africa, where it appeared to producesimilar lesions and occurred in similarcircumstances. This has not presented a problemelsewhere in Africa, nor in subsequent epizooticsin South Africa.Toxoplasmosis, leptospirosis, brucellosis, Q fever
and salmonellosis all feature as possible differentialdiagnosis for RVF. However, they are not presentin such an explosive manner over large areassimultaneously. They are not associated withrainfall, nor do they produce such high neonatalmortality. Good supportive laboratory competencyis required to make a diagnosis.
Diagnosis of RVFRVF antigen detection
• Agar gel diffusion test• Virus isolation in mice/hamsters/tissueculture• RT-PCR identification of RVF virus• Capture ELISA test• Immunochemical staining of fixed tissues
RVF antibody detection
• ELISA tests for IgM/IgG• Indirect immunofluorescent/peroxidasetests• Microtitre virus-serum neutralization tests• Indirect haemagglutination tests• Plaque reduction assays
The International Office of Epizootics (OIE)Manual of standards for diagnostic tests and vaccines
contains guidelines on the collection of samplesand the diagnostic techniques for diagnosis ofRVF infection.RVF should be suspected if there is a suddenonset of large numbers of abortions in cattle,
sheep, goat or camel populations associatedwith a high neonatal mortality and the presenceof liver lesions. Cases of disease in peopleassociated with the affected animals also assistin making a tentative diagnosis. A provisionaldiagnosis may be based upon the clinical picture,climatic and ecological factors such as the presenceof huge mosquito populations, together withthe explosive nature and onset of the disease.Laboratory confirmation of RVFRVF is a member of the human haemorrhagicfever group of viruses, such as Ebola and CrimeanCongo haemorrhagic fevers. These virusespresent a serious hazard to all personnel handlinginfected carcasses, blood and other tissues bothin the field abattoir and in the laboratory. Forthis reason it is recommended that fieldveterinarians and laboratory personnel bevaccinated against RVF, if this is possible. Thehandling of RVF infected material should only
46 Vol. 42 (1), Vet Ital www.izs.it © IZSA&M 2006
Recognizing Rift Valley Fever F. Glyn Davies & Vincent Martin
Control of infection in case of haemorrhagicfever in African hospitals
be carried out under P-2/P-3 conditions or withtype II biosafety cabinets and HEPA filteredrespirators, where the security of the staff canbe assured. For this reason, the appropriatediagnostic procedures are dependent upon thefacilities available.
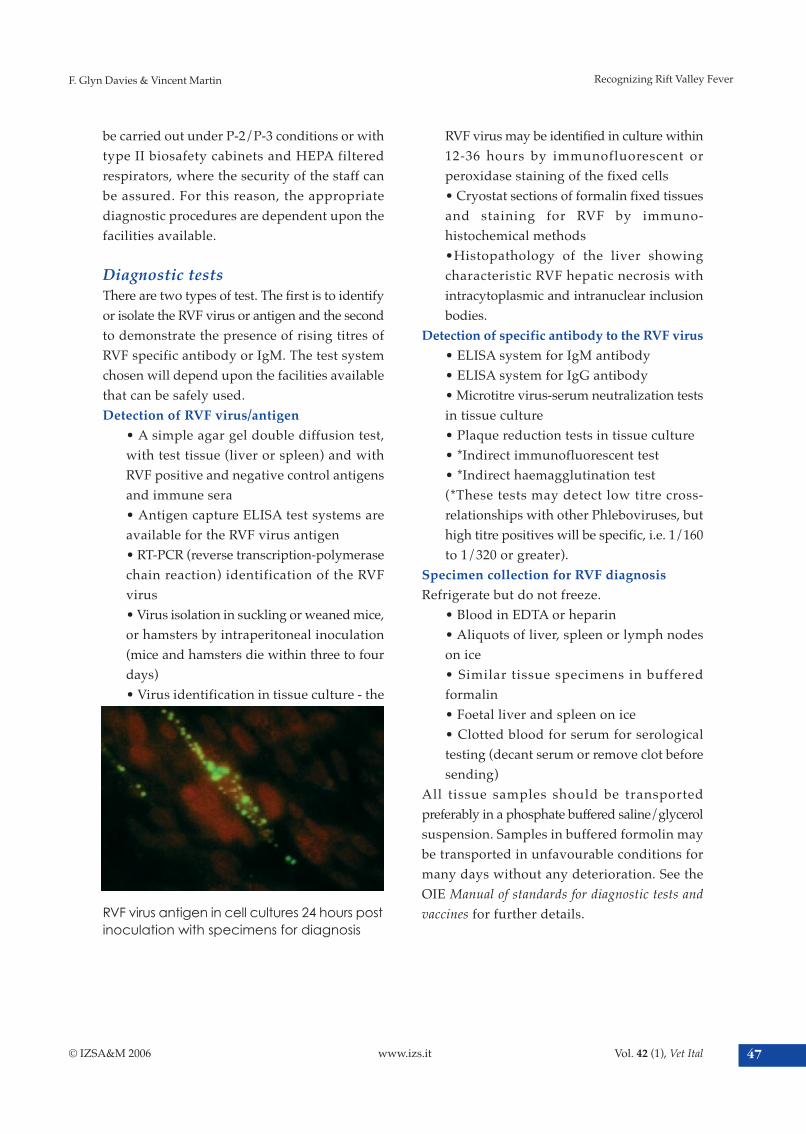
Diagnostic testsThere are two types of test. The first is to identifyor isolate the RVF virus or antigen and the secondto demonstrate the presence of rising titres ofRVF specific antibody or IgM. The test systemchosen will depend upon the facilities availablethat can be safely used.Detection of RVF virus/antigen
• A simple agar gel double diffusion test,with test tissue (liver or spleen) and withRVF positive and negative control antigensand immune sera• Antigen capture ELISA test systems areavailable for the RVF virus antigen• RT-PCR (reverse transcription-polymerasechain reaction) identification of the RVFvirus• Virus isolation in suckling or weaned mice,or hamsters by intraperitoneal inoculation(mice and hamsters die within three to fourdays)• Virus identification in tissue culture - the
RVF virus may be identified in culture within12-36 hours by immunofluorescent orperoxidase staining of the fixed cells• Cryostat sections of formalin fixed tissuesand staining for RVF by immuno-histochemical methods•Histopathology of the liver showingcharacteristic RVF hepatic necrosis withintracytoplasmic and intranuclear inclusionbodies.
Detection of specific antibody to the RVF virus
• ELISA system for IgM antibody• ELISA system for IgG antibody• Microtitre virus-serum neutralization testsin tissue culture• Plaque reduction tests in tissue culture• *Indirect immunofluorescent test• *Indirect haemagglutination test(*These tests may detect low titre cross-relationships with other Phleboviruses, buthigh titre positives will be specific, i.e. 1/160to 1/320 or greater).
Specimen collection for RVF diagnosis
Refrigerate but do not freeze.• Blood in EDTA or heparin• Aliquots of liver, spleen or lymph nodeson ice• Similar tissue specimens in bufferedformalin• Foetal liver and spleen on ice• Clotted blood for serum for serologicaltesting (decant serum or remove clot beforesending)
All tissue samples should be transportedpreferably in a phosphate buffered saline/glycerolsuspension. Samples in buffered formolin maybe transported in unfavourable conditions formany days without any deterioration. See theOIE Manual of standards for diagnostic tests and
vaccines for further details.
47© IZSA&M 2006 www.izs.it Vol. 42 (1), Vet Ital
Recognizing Rift Valley FeverF. Glyn Davies & Vincent Martin
RVF virus antigen in cell cultures 24 hours postinoculation with specimens for diagnosis

What samples should be collected in an
outbreak?
At an outbreak site, where sheep, cattle or camelsare aborting and there are deaths in neonates,itis suggested that the following samples becollected:
• at least 10-20 serum samples from animalsthat have recently aborted• 10-20 samples from animals that have notaborted• blood in anticoagulant from any animalswith a fever of 40.5-42°C• liver and spleen from any freshly deadanimals, on ice, in glycerol buffered salineand/or in buffered formalin• liver, spleen and brain from fresh foetuses
What information is required?
The following basic information should becollected:• sampling site with map reference or fulladdress• owner’s name, contact address, telephone,etc.• herds/flocks/breeds/strains affected,numbers and age groups• date of first case/date sampling• no affected/no dead/no abortions/agegroups• full clinical history• presence/absence of febrile human disease• basic ecological characteristics of affectedarea
Prevention and controlof Rift Valley Fever
Early detection of RVF is a prerequisite to effectivecontrol of the disease. Sentinel herd monitoringhas been used in different parts of Africa to
monitor viral circulation in susceptiblepopulations. It can be enhanced by the additionalmonitoring of climatic parameters (see: Towards
early warning for RVF prevention: satellite imagery,p. 35).
Sentinel herd monitoringActivities should be directed towards activedisease surveillance in order to build up baselineinformation on inter-epidemic virus transmissionpatterns, areas at risk and early warning of anyincreased virus activity or buildup in vectormosquito populations. This surveillance shouldbe carried out by regular field visits and contactwith livestock farmers and communities and
should include periodic purposefully designedand geographically representative serologicalsurveys and participatory epidemiologicaltechniques. The detection of RVF virus activityby serology is usually too late to be of anyrelevance for control.Sentinel herds are an important means ofobtaining baseline epidemiological informationon RVF. These are small ruminant herds locatedin geographically representative areas. Locationswhere mosquito breeding activity is likely to
48 Vol. 42 (1), Vet Ital www.izs.it © IZSA&M 2006
Recognizing Rift Valley Fever F. Glyn Davies & Vincent Martin
Sentinel herd monitoring in Mali

be greatest, e.g. near rivers, swamps and dams,should be selected. Such mosquito breedingsites are typically shallow depressions that areflooded during prolonged periods of rainfalland along irrigation channels.In order to be effective and more reliable, sentinelherds should be monitored in conjunction withthe monitoring of other risk indicators such asclimatic parameters (see paragraphs below).Once herds have been identified, livestockowners are informed about the background andthe importance of the study and asked for theircooperation. Incentives such as free antiparasiticdrugs for internal parasites should be providedduring each visit to ensure the owner ’scooperation. If possible, no acaricides, pour-onor insecticides should be provided since theirapplication will influence the attack rate of theanimals from potential arthropod vectors.About 30 young female sheep or goats (withtwo permanent incisors) are identified andpermanently marked. Choosing young femalesreduces the probability that these animals areslaughtered or sold between visits. The animalsshould be at least one year old, ideally between12 and 15 months. At the first visit, blood samplesare collected from the animals and tested forIgG antibodies and IgM antibodies to the RVF
virus. Only antibody negative animals shouldbe included in the sentinel herd. If some of theanimals are seropositive they should be excludedfrom the monitoring exercise and replaced byseronegative animals.The sentinel herds should be visited at regularintervals. Ideally, animals should be sampledat the beginning of the rainy season and thereafterevery four to six weeks up to the end of therainy season. In a typical year this would involvefour or five visits to each herd. At each visitsome basic information is obtained and bloodis collected from all the sentinel animals. Samplesshould be forwarded to the National CentralVeterinary Laboratory and tested within twodays of arrival for the presence of IgM and IgGantibodies.Attempts should be made to keep the size ofthe sentinel herd above 20 animals at eachlocation. This means that during most visits itwill probably be necessary to identify newanimals since some animals of the establishedherd may have died or have been removed forother reasons. If animals have seroconvertedthey will also be excluded during the next visitand replaced by new fully susceptible animals.The principle here is to maintain at any time abasic number of animals (sheep and goats) thatare well identified and fully susceptible to RVFinfection at the locations prone to the emergenceof RVF epidemics, and to follow these animalsclosely through clinical and serologicalinvestigations to detect the emergence of RVFepidemics in time.
Towards early warning for RVFprevention: Satellite imageryThe three essential prerequisites for an epidemicto occur are a susceptible livestock population,a massive buildup in the populations of vector
49© IZSA&M 2006 www.izs.it Vol. 42 (1), Vet Ital
Recognizing Rift Valley FeverF. Glyn Davies & Vincent Martin
Sentinel herd monitoring in Mauritania

mosquitoes and the presence of the RVF virus.Assuming the continuing presence or at leastthe close proximity of the virus in regions wherethe disease has occurred previously, the firsttwo factors become the key to early forecastingof likely RVF activity.Early work on forecasting was centred at a studysite in Kenya where ground truth data for RVFvirus activity had been generated for manyyears. Periodic outbreaks of RVF over a 40-yearperiod were found to correlate with the positivevalue of a statistic based upon the number ofrain days and the quantity of rainfall.
Correlation of RVF epizooticswith the persistence of rainfallThe three-month rolling mean value formed apositive spike when RVF virus activity occurredand this was a function of cumulative persistentrainfall, rather than heavy precipitation over ashort period. Data were based upon longitudinalrainfall data generated and recorded in the old-fashioned manner. The characteristics of theintertropical convergence zone were alsoimportant as a determinant of prevailingconditions conducive to RVF virus activity. Thesedata allowed forecasting of RVF outbreaks witha four to ten week period during whichvaccination could be carried out before casesoccurred.
More sophisticated studies were possible whenremote sensing satellite data (RSSD) becameavailable. These data enabled national andregional monitoring of rainfall and climaticpatterns and their effects upon the environment.Cold cloud density (CCD) measurements areclosely correlated with rainfall and have replacedthe laborious daily collection of rainfall datafrom many stations. Climatic patterns are regionalin East Africa and the Horn of Africa and maybe studied on this basis. A detailed analysis wasmade with virus isolation data over a 25-yearperiod and the normalized differentiatedvegetation index (NDVI) for the study areas.NDVI data are derived from probes measuringrelative “greenness” and “brownness” of thevegetation. As the water table rises to the pointwhere flooding may occur, the ratio approaches0.43 to 0.45. This point was reached at each ofthe epizootic periods in the study period.More recent retrospective studies using the sameground truth data have included the surfacesea temperatures (SST) for the Indian and PacificOceans. When these were combined with NDVIdata, they approached 100 percent accuracy inpredicting periods of RVF virus activity duringthe study period. This has a pre-epizooticpredictive period of two to five months beforevirus activity occurs.New statistics have been derived from satellitedata, known as basin excess rainfall monitoringsystems (BERMS). These measure rainfall in thecatchment areas of river/wadi systems and arebased upon digital maps of basin and rivernetworks. They can predict periods when floodingmight occur, which is particularly valuable forthe floodplain zones in the Horn of Africacountries and the Arabian Peninsula. Early datasuggest that BERMS might be able to predictvirus activity five months before its occurrence.
50 Vol. 42 (1), Vet Ital www.izs.it © IZSA&M 2006
Recognizing Rift Valley Fever F. Glyn Davies & Vincent Martin
Correlazione tra epizoozie di RVF e persistenzadelle piogge

The advantages of RSSD for RVF predictiveepidemiology are in the relatively low costs ofthe systems used for analysis. These are readilyavailable on a country and regional basis andgive time for preventive measures such as thevaccination of susceptible stock and mosquitolarval control methods, wherever possible.International agencies are best placed to analysesatellite and other data and to provide riskcountries with early warning about likely weatherpatterns conducive to increased RVF activity.FAO, through its Global Information and EarlyWarning System on Food and Agriculture(GIEWS) and the Emergency Prevention Systemfor Transboundary Animal and Plant Pests andDiseases (EMPRES)/Livestock Programmeintends to take a central role in generating thesedata on a continuing basis, thus providing anearly warning/risk assessment service.It must be recorded that little work has been donein other parts of Africa to validate the RSSDsystems because the ground truth data have notbeen available and it takes many years of dedicatedwork to generate such data. Recent outbreaks inSomalia and northeast Kenya in 1997-98 showed
retrospectively that the foci of RVF virus activityin these countries could be correlated with highNDVI values. However, more validation work isneeded before the use of such techniques becomesan operational early warning system (see mapsrepresenting NDVI difference in January 1997,1998 and 1999).
Control strategiesPreventive vaccination
This is the most effective means to control RVF.Early warning of high-risk periods for the diseaseis possible and this information should drivestrategic vaccination campaigns. The mosteffective vaccine is the modified live Smithburnneurotropic strain (SNS). This vaccine isimmunogenic but has the disadvantage that itcan cause foetal pathology and abortion inpregnant sheep of susceptible genotypes. Upto 30 percent of such animals may be affectedby abortion or foetal abnormalities. Inactivatedvaccines have been prepared but are often poorlyimmunogenic. Onderstepoort Biological Productsin South Africa produce an inactivated vaccinethat is based on a bovine virulent RVF isolate,
51© IZSA&M 2006 www.izs.it Vol. 42 (1), Vet Ital
Recognizing Rift Valley FeverF. Glyn Davies & Vincent Martin
Maps representing NDVI difference in January 1997, 1998 and 1999

adapted and produced in cell culture. The vaccineis then inactivated and mixed with aluminiumhydroxide gel as adjuvant. It has the advantageof being suitable for use in pregnant ewes. Giventhe poor antibody response in cattle, theinactivated vaccine is recommended even incows so that they can confer colostral immunityto their offspring. A booster three to six monthsafter initial vaccination is required, followedby annual boosters.Routine vaccination when animals are notpregnant is recommended. The SNS vaccine isperfectly safe and protective in cattle. Vaccinationis NOT recommended once evidence of epizooticvirus activity has been confirmed. Apart frombeing too late, needle propagation of the virusis a real danger.Vaccine development
Other modified live virus and molecular derivedRVF antigens are being developed, but are notcurrently available for field use.
• The MP 12 strain was developed bymutagen induced changes in the ZH 548strain of the RVF virus and Clone-13 is acloned population, obtained from a fieldstrain isolated from a mild human case inthe Central African Republic. Both havebeen shown to be good immunogens in mice,and produce antibodies detectable by ELISAand plaque reduction neutralization assays.The Protective Dose (50 percent) (PD 50) forClone 13 was 100.1 TCID50 and for MP 12was 103. The S segment of the RVF virusdetermines virulence/loss of virulence andthe NSs deletion results in attenuation. Therole of NSs has been elucidated: it is anantagonist of type I interferon production.Indeed, infection of mice with strains thatpossess an efficient NSs does not lead toany production of interferon, whereas high
levels of interferon were observed in miceinfected with the NSs defective Clone 13virus. Clone 13 is of interest because of thelow risk of reversion in thisvirulence/attenuation marker. However,the L and M segments do not contain markersfor attenuation. If animals are vaccinatedwhen virulent strains are circulating, thereis a possibility that reassortment may occur;in this case Clone 13 would induce a viraemia(which is not observed in mice). The majorityof reassortants could become virulent.• An R566 strain has been derived fromClone 13 and MP 12 by reassortment in Verocells: it contains the S segment of Clone 13and the L and M segments of MP12, whichcontain seven and nine point mutationscompared with their virulent parent. Someof them induce attenuation andthermosensitivity. Thus R566 is safe, becauseof its attenuation in the three segments ofthe genome. R566 has been shown to protectmice in the laboratory.
Vector control
Strategic larvicidal treatment of mosquito breedinghabitats is recommended. Both hormonalinhibitors such as methoprene and larvical toxinssuch as those produced by Bacillus thurigiensis
give excellent results and both are commerciallyavailable. However, they may be difficult to usein some places with floods of wide distribution.The widespread use of vehicle or aerial mountedultra low volume insecticide sprays appears tohave limited effect upon RVF transmission ratesor the target adult mosquito species.Movement controls
These do not appear to have any effect uponthe course of an outbreak within an infectedcountry. They may, however, be relevant to themovement of animals for trade from
52 Vol. 42 (1), Vet Ital www.izs.it © IZSA&M 2006
Recognizing Rift Valley Fever F. Glyn Davies & Vincent Martin

enzootic/epizootic areas, where RVF virustransmission is occurring. In this situation,viraemic animals could arrive in an uninfectedcountry within the incubation period for thedisease. If this should happen and there were
large numbers of mosquito vectors present,capable of RVF virus transmission, then thepossibility of introduction of RVF is very real.For this reason, all export of livestock shouldbe banned during RVF epizootic periods.
53© IZSA&M 2006 www.izs.it Vol. 42 (1), Vet Ital
Recognizing Rift Valley FeverF. Glyn Davies & Vincent Martin





![Precision medicine for age-related macular degeneration ... · 3 Age-related macular degeneration (AMD) is the primary cause of irreversible blindness in developed countries [1].4](https://static.fdocuments.net/doc/165x107/5f4c3164835c03225a766e33/precision-medicine-for-age-related-macular-degeneration-3-age-related-macular.jpg)











