
Recognition and Treatment of the Critically Unwell Patient
42
Recognition and Treatment of the Critically Unwell Patient Rebeka Wright PA-R, BSc (Hons), PgDip (Physician Associate studies), PGCert (Critical Care) Physician Associate Critical Care – Guys and St Thomas’ Hospital NHS Foundation Trust
Transcript of Recognition and Treatment of the Critically Unwell Patient

Recognition and Treatment of
the Critically Unwell PatientRebeka Wright PA-R, BSc (Hons), PgDip (Physician Associate studies), PGCert (Critical Care)Physician Associate Critical Care – Guys and St Thomas’ Hospital NHS Foundation Trust

No conflict of interests

Introduction
History of critical care
Recognising the unwell
patient
Respiratory failure
Shock
Renal Failure
Correcting abnormal
physiology in first instance
diagnostic considerations
second
Many simple interventions to
correct abnormal
physiology can occur in
ward setting

Critical Care
“care for patients who have potentially
recoverable conditions who can benefit from
more detailed observation ( with or without invasive treatments) then can be provided safely
in an ordinary ward”. Intensive Care Society
Level 2 – single organ failure, post op, stepdown
from higher levels
Level 3 – advanced respiratory support alone of
monitoring or support two or more organ systems
History of Critical Care Florence Nightingale in her observation of recovery areas near the
operating theatre
1923 – Johns Hopkins Hospital USA – post op neurosurgical patients
WWII and Korean and Vietnam wars
Modern concept after Poli epidemic in 1952 Copenhagen positive pressure ventilation from ‘iron lung’
Further expansion in 1960s
1992 First formation of advisory committee for intensive care medicine
2001 First ICM training programme launched
2010 Faculty of ICM training
Very heterogeneous – variable care nationwide

Recognising the Unwell
Patient
Essential to recognise to
initiate immediate action to
correct abnormal physiology
Anticipation of at risk patients
e.g. post op
ABCDE approach
NEWS2 >5 review by clinician
with critical care experience, >7 MET call/peri-arrest
Airway
Airway obstruction
Impaired airway protection
Breathing
Respiratory arrest RR<8 or >25
SaO2 <90%/paO2 <8Kpa on 50%
FiO2
pCO2 >6.5 or pH <7.3
HR <40 or >130
Lactate >2 BE >-4
UOP <0.5ml/kg/hr
GCS <12 or drop >2
Prolonged siezures

NEWS2
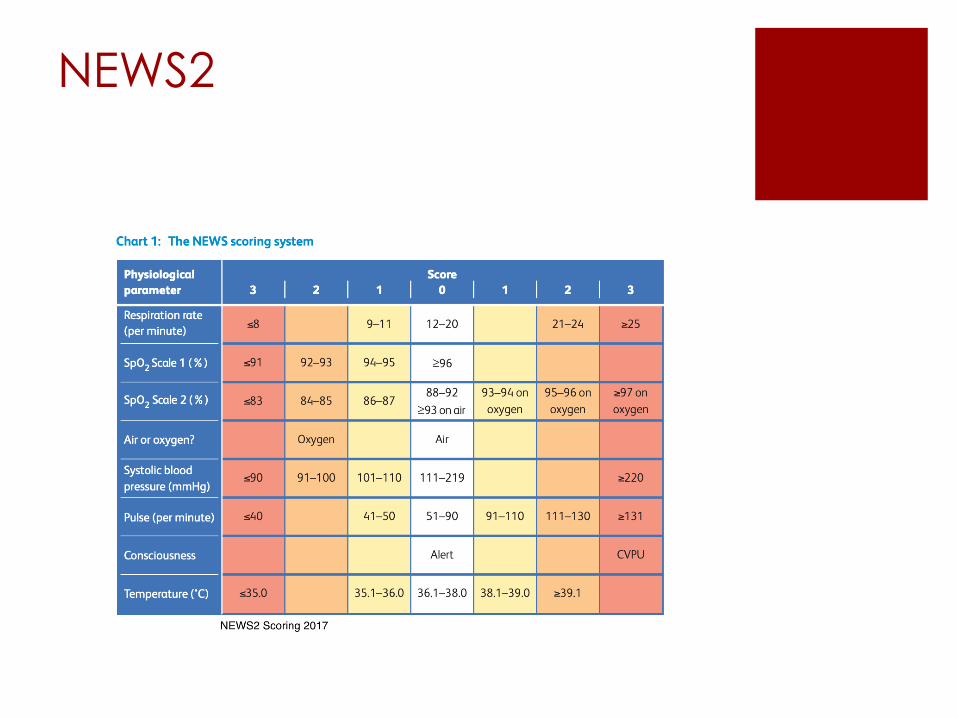
NEWS2

NEWS2

Monitoring

Other equipment

Respiratory Failure
Key Concepts
Causes
Oxygen therapy
HFNC
CPAP
NIV
Invasive Ventilation
VV- ECMO

Key Concepts SaO2 indicator of oxygenation NOT ventilation.
Average person at rest 1L/min TV supply metabolic
demands – we breathe more for CO2 clearance
Minute Ventilation = Tidal Volume (TV) x RR – pCO2
is inversely proportional to MV
Simplified alveolar gas equation
PAO2 = FiO2 (Patm –pH2O) – PACO2/R~0.8
• simply the more CO2 there is the less space there is
for O2
Dead space – 2ml/Kg – part of each breath that
does not take part in gas exchange – anatomical
and alveolar
VA (alveolar volume) = RR x (TV – dead space)

V/Q matching – West Zones
Optimal V/Q = 1
PPV increases
zone 2
V/Q 0.36

Causes respiratory Failure
1. Acute Hypoxaemic – Type 1 pO2 <8 normal or
low pCO2
V/Q mismatching – Pneumonia, PE, pulmonary
oedema, ARDS
2. Ventilatory – Type 2 raised pCO2 >6.5-7
CNS depression, respiratory muscle weakness
3. Post – Op – atelectasis and reduction FRV
4. Type IV respiratory failure – hypoperfusion or
shock.
DO2 = CO x CaO2 = [(Hb x SaO2 x k) + (PaO2 x
0.023)

Oxygen therapy
Nasal specs, venturi
Oxygen therapy in
hypercapnia
o Causes pulmonary
vasodilatation increases
shunt fraction
o Haldane effect –
deoxygenated Hb high
affinity for O2
o Hypoxic drive
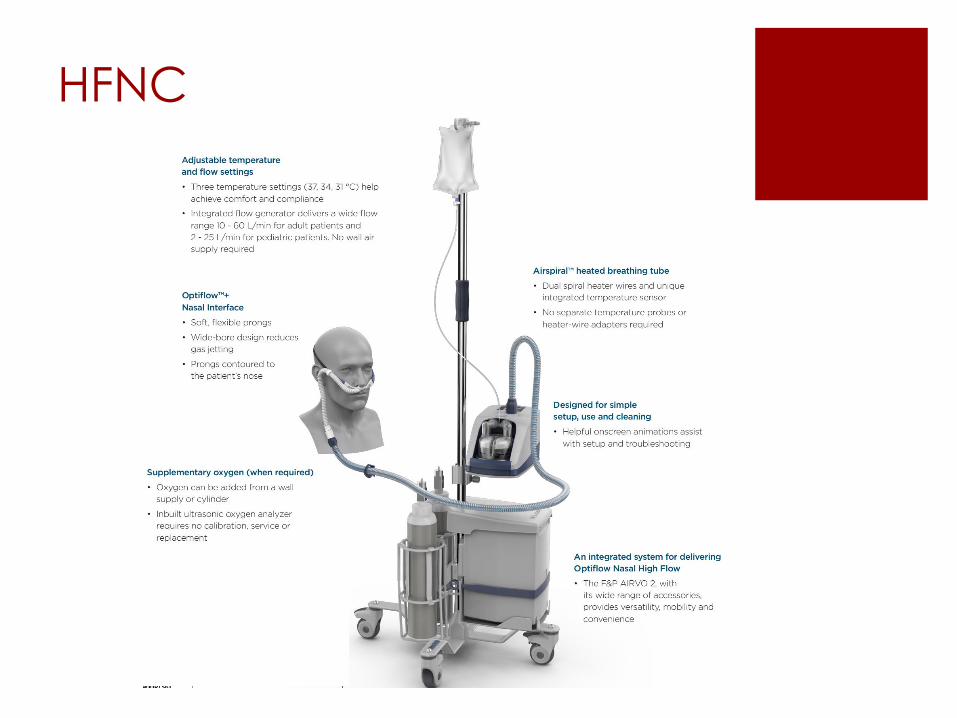
HFNC
CPAP – improved
oxygenation
PEEP
prevents alveolar collapse improving recruitment thus improvement of V/Q mismatching
Decrease in venous return – leading to decrease in preload and
decreased work load

NIV

NIV mask

NIV
BTS guidelines
NIV - non invasive ventilation
Indications – acute hypercapnic respiratory failure
pH <7.25 pCO2>6.5 RR >23 if persisting after bronchodilators and O2
COPD, NM disease/chest wall deformity, OSA/OHS
Contraindications
Absolute – severe facial deformity/burn/upper airway obstruction
Relative pH <7.15 or pH <7.25 + (GCS <8, confused, agitated cognitive
impairment
ICU referral – impending resp arrest, NIV failing to reduce pCO2, SaO2<85% on
NIV, need for sedation to tolerate, pH <7.25 or RR >25 on optimal setting – if fail
NIV then ventilated mortality is increased
Asthma/pneumonia – poor outcomes
Complications – pressure ulcer, gastric distension, PTX

1. Set PC/PS
2. Set
BUR
16-20
3. Set Ti
0.8-1.2
(PC
only
4. IPAP – inspiratory positive airway pressure aid inspiratory
pressure to increase inspiratory pressure – improves PaO2 and
CO2 – 15 (20 if pH <7.25) max 30
5. EPAP – expiratory positive airway
pressure stents upper airways and recruits
underventilated lung – improves PaO2 – 3
unless OSA known or suspected max 8
NIV trouble shooting
Elevated PaCO2 = increase IPAP or decrease EPAP – IPAP – EPAP
= TV and MV is TV xRR
Low PaO2 = increase EPAP/IPAP/both – not home NIV (max FIO2
0.5)
ABG after 30-60mins
Use 24/7 then taper 72hrs

Invasive Ventilation

Invasive ventilation
Indications – RR>35 PaO2 <8
on FiO2 0.5% PaCo2 >7.5 pH
<7.25 GCS <8, poor sputum
clearance, exhaustion,
failure to improve on NIV
RSI – sedative, opiate,
neuromuscular blocker –
preoxygenate-sedative-
NMB-cricoid pressure-
intubation
Cardiovascular response-
Reduces RV preload, LV
afterload
Set up
1. FiO2
2. Mode- Full or partial/ volume or
pressure
3. Full support – RR TV (6ml/Kg) or Pinsp
(to target TV)
4. PEEP
5. I:E
Increase pO2 increase FiO2/PEEP
Decrease pCo2 Increase MV (TV xRR)

VV-ECMO Large bore cannulae venous system through
oxygenator
Allows lungs time to heal
Not haemodynamic support
Rescue method – refractory hypoxaemic respiratory faliure
Potentially reversible aetiology
ShockClinical syndrome when acute circulatory failure
with an inadequate or inappropriately distributed
perfusion results in failure to meet tissue metabolic
demands causing generalized cellular hypoxia
Signs and Symptoms: Confusion, Tachypnoeia,
Hypotension, Cold or cyanosed or warm and
flushed, Decreased UOP
Key concepts
Types
Management
Monitoring

Key Concepts - preload
MAP = CO (SV x HR) x SVR
SV determined by preload, afterload, myocardial contractility
Preload – myocardial sarcomere length prior to contraction – EDV (echo)or EDP ( CVC/PAC)
• Venous return
• Ventricular compliance
• Pericardial compliance
• Valvular disease
• Atrial kick
• Ventricular wall thickness
• Intrathoracic pressure

Key concepts - Afterload
MAP = CO (SV x HR) x SVR
Afterload – sum of the forces opposing
ventricular ejection = Ventricular wall stress
Ventricular wall stress directly proportional to
P x r/ T
P = ventricular transmural pressure (ITP – Ventricular
cavity pressure during ejection)
r = ventricular chamber radius (increased with EDV)
T = Ventricular wall thickness

Key concepts - Contractility
MAP = CO (SV x HR) x SVR
Contractility – factors other than HR, preload and
afterload responsible for changes in myocardial
performance. Primarily dependent on intracellular Ca2+
• Drugs
• Disease – Ischaemia, HF
• Autonomic tone
• Increased HR
• Increased afterload
Types Cardiogenic
• MI and complications
• Myocarditis
• Myocardial contusion
• Takotsubo
• Septic
• Drugs
• Cardiomyopathy
• Dysrhythmias
• Severe AR, AS or MS
• LVOT obstruction
Endocrine/metabolic
• Adrenal insufficiency
• Hypo/hyperthyroid
• DKA
• Severe electrolyte disturbance e.g. low Ca2+
Obstructive
• Massive PE
• Atrial thrombus
• Cardiac tamponade
• Abdominal compartment syndrome
• Tension pneumothorax
• Dynamic hyperinflation – asthma
Hypovolaemic
• Haemorrhage
• Fluid loss
Distributive
• Neurogenic
• Liver failure
• Septic
• Anaphylaxis

Types of Shock
High
Cold
Low
Cardiogenic/obstructive
Septic
Warm
High
Sepsis/ CO2 retention
Fluid overload
Low
Warm
High
Sepsis/anaphylaxis
Cold
Low
Haemorrhage/
Fluid loss
anaphylaxis
Peripheries
Pulse volume
Diagnosis
CVP/JVP
Neurogenic, endocrine

Management Shock
Identify aetiology is key
Correct hypoxaemia
Dependent on aetiology – treat underlying cause
Optimise preload
Minimise Afterload
Increase contractility
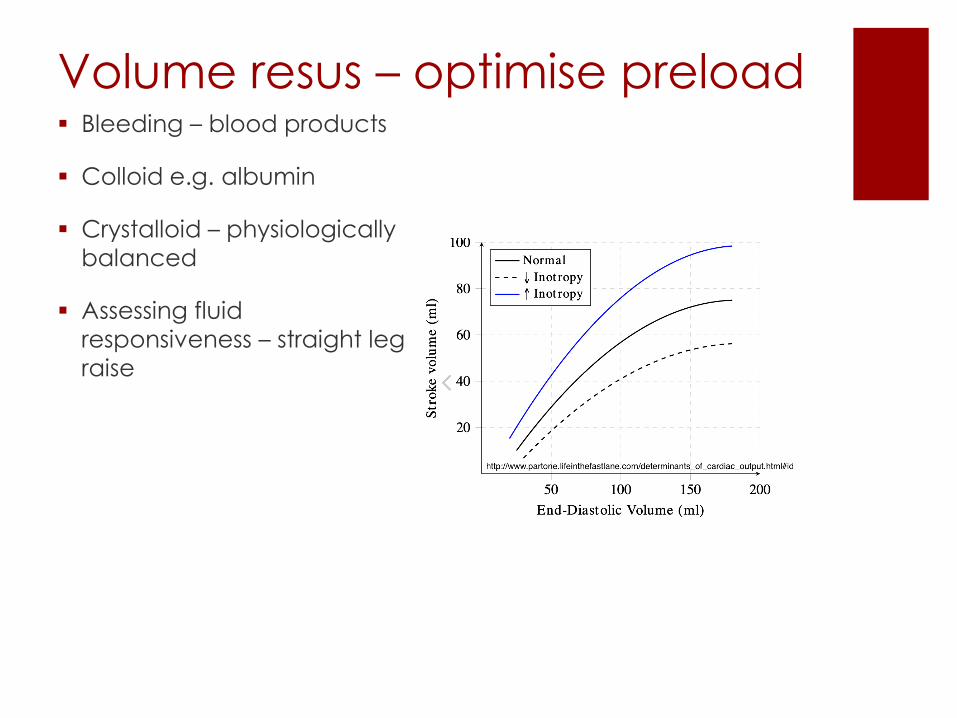
Volume resus – optimise preload Bleeding – blood products
Colloid e.g. albumin
Crystalloid – physiologically
balanced
Assessing fluid
responsiveness – straight leg
raise

Increase SVR Vasopressors
• Noradrenaline = alpha
(beta 1)
• Phenylephrine pure alpha
agonist
• Metaraminol = alpha
(beta 1+2)
• Vasopressin V1
Iinocostrictors
• Adrenaline = alpha and
Beta 1 (beta2)
Alpha receptors = peripheral
vasoconstriction
Beta1 receptors =
chronotrophy and inotropy
Beta 2 receptors
vaso/bronchodilatation
MAP = CO (SV x HR) x SVR
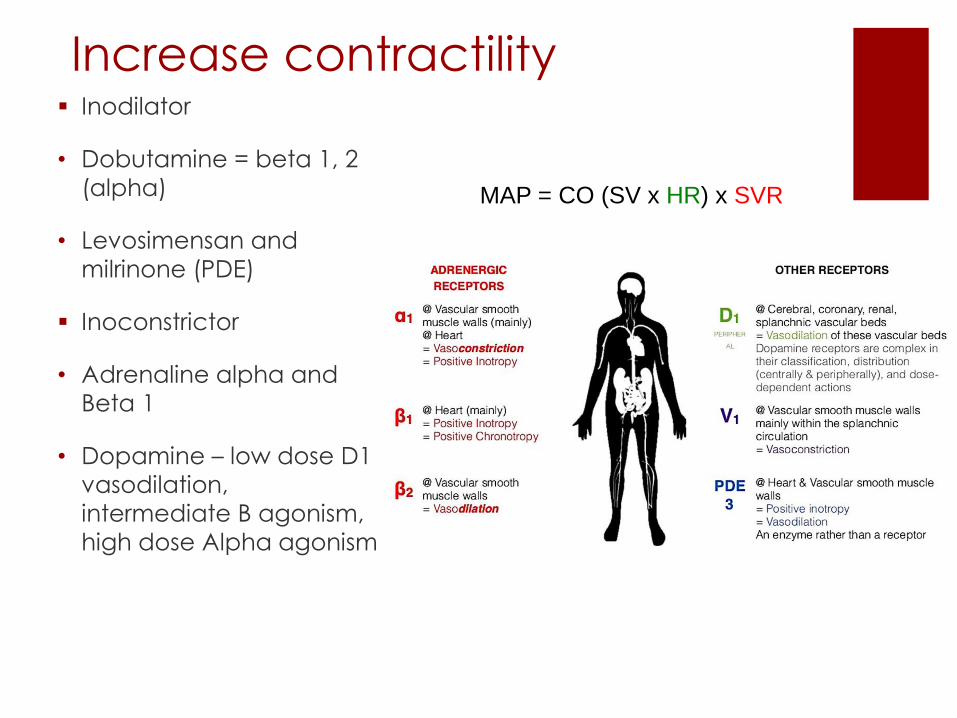
Increase contractility Inodilator
• Dobutamine = beta 1, 2
(alpha)
• Levosimensan and
milrinone (PDE)
Inoconstrictor
• Adrenaline alpha and
Beta 1
• Dopamine – low dose D1
vasodilation,
intermediate B agonism,
high dose Alpha agonism
MAP = CO (SV x HR) x SVR
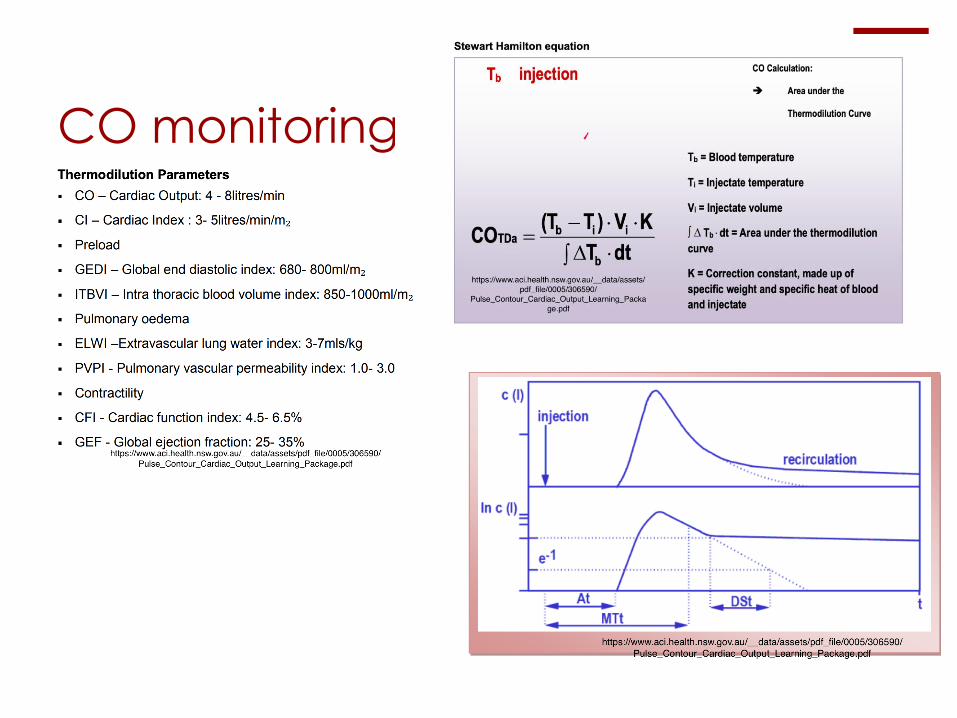
CO monitoring

Sepsis – life threatening organ dysfunction
due to dysregulated host response to infection
SOFA or qSOFA (SBP <100, RR>22 GCS <15) score >2 (mortality 10%)
Septic shock – MAP <65 + Lac>2 despite adequate fluid resuscitation (mortality
>40%)
Management – begin immediately
30ml/Kg crystalloid in 3hrs
Regular review of CO (dynamic over static variables) MAP>65 if req vasopressors
Fluid resus to normalise lactate
Cultures
Abx – broad- spectrum (within 1hr of recognition), rationalised once organism
identified. Not in inflammatory conditions, duration 7-10/7, short duration, PCT
Identification of source and source control
Noradrenaline (need art line), dobutamine
Hb>70, Plt>10 or >20 if risk of bleeding, >50 if bleeding or needing proceedure

Renal Replacement
Threapy
Indications
o Fluid overload (refractory to medical treatment)
o Refractory hyperkalaemia
o Uraemic pericarditis/ encephalopathy
o Refractory metabolic acidosis pH<7.3
o Raised Cr

Types CRRT, PIRRT, IHD
CRRT – haeamodynamic instability
Access
HD – dialysis via diffusion
HF – filtration
mix
Anticoagulant
Exchange rate L/min – Ur/Cr, K
Fluid removal / fluid balance
Questions ?


















