
Recognising agents in health systems…and complexity
37
Recognising agents in health systems …. and complexity ICHS 5 www.hpsa- africa.org @hpsa_africa www.slideshare.net/ hpsa_africa Introduction to Complex Health Systems
-
Upload
consortium-for-health-policy-systems-analysis-in-africa-chepsaa -
Category
Health & Medicine
-
view
68 -
download
0
Transcript of Recognising agents in health systems…and complexity

Recognising agents in health systems ….
and complexity
ICHS 5
www.hpsa-africa.org
@hpsa_africa
www.slideshare.net/hpsa_africa
Introduction to Complex Health Systems

Recognising agents in health systems ….
and complexity
• Who are they?• What influences their behaviour?• What power do agents have? • What implications for system
functioning?

Going back to the people & software of health systems

Who are the system agents?

Categories of people & organisations
• Patients & citizens• Health providers &
managers at various levels, & other health ‘organisations’
• Public, NGO, & private-for profit organisations
• Various levels/groups/units in ‘collective mediator’
• Other sectors• Professional
associations• Trade Unions• Research groups
• Who else??

In public service organisations, who ...
• controls resources?• has political influence (including media,
pressure groups)?• has involvement in the service delivery
process?• has impact on wider environment of
organisation (e.g. regulatory bodies, local authorities)?

Agents in Systems
May play several system roles,• have relationships with other individuals• be part of groups, and/or work within
organisations, with their own histories of experience – which are part of bigger systems e.g. the
District Health System• be located in specific ‘settings’, with their
own histories

What influences agents’ behaviour?
1. Mindsets, assumptions, beliefs
How many fs?
two of the most powerful and effective of all human fears are the
fear of failure and the fear of success

http://www.theinvisiblegorilla.com/videos.html
Use ‘the Monkey business illusion’

Observable data and experiences
I select data from what I observe
I adopt beliefs, draw a map
I make assumptions based on these meanings
I add cultural and personal meanings
Reflexive loop our beliefs influence our selection
I take actions based on my beliefsThe Ladder of Inference
Conclusion: opinion
reached
Interpretation: meanings &
assumptions added
Selected data:
what you choose
Observable data:
what people actually said
and did
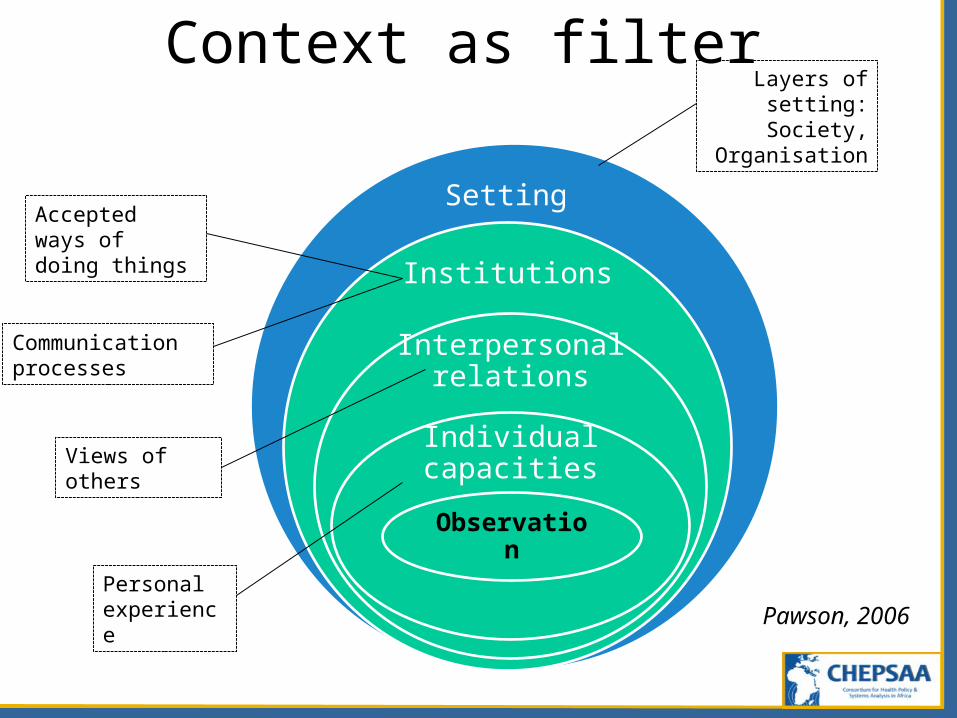
Setting
Institutions
Interpersonal relations
Individual capacities
Observation
Pawson, 2006Personal experience
Views of others
Accepted ways of doing things
Communication processes
Layers of setting: Society,
Organisation
Context as filter

Organisational influencesVisible: the formal organisation
Vision, Mission, Structure, Job descriptions, Goals, Strategies, Operating policies
complicated
Invisible: the informal organisation
Power and influence patterns\Group dynamicsImpulsivenessFeelingsInterpersonal relationsOrganisational cultureIndividual needs
complex
Adapted from Kusek et al.
2013
Personal & cultural meanings
• Discuss examples from papers

Sensemaking
‘the process individuals undertake as they try to understand what is going on around them, as they try to make sense of events and experiences’
(Balogun 2003)

2. Interests
Interests
• Thing for/about which one has concerne.g. power or status or financial gain, fear of
loss• Interests shaped by:
– personal values & factors– memories of similar policy experiences– group loyalty– organisational factors– socio-political, socio-economic factors
• Influence responses to change

Reflection point
• What is your primary position in the health system?
• In that position, what are your interests?– Personally and/or Professionally
3. What power do agents have?

Reflection point
• What is your primary position in the health system?
• In that position, what is your power?– To do what?– Over whom?
• What impact does the exercise of your power have on others around you?

Power in HS: the view from the bottom
National & Provincial Programme & Support Managers
Front Line Manager & Provider
multiple & sometimes conflicting TOP-DOWN demands
Mid- Level Managers
hierarchy
Local Government and Health Consortium, 2004
Politicians
Power in health systems
From top to bottom
From bottom to top

Discretionary power in organisations exists
‘whenever the effective limits on [the public officer’s] power leave him free to make a choice among possible courses of action and inaction’ (Davis 1969, p.4).
Everyday discretionary power
Overt:• Issuing instructions
to others• Publicly refusing to
follow instructions• Being rude to
patients
Covert:• Taking unnecessary
sick days• Taking
unnecessarily long tea breaks
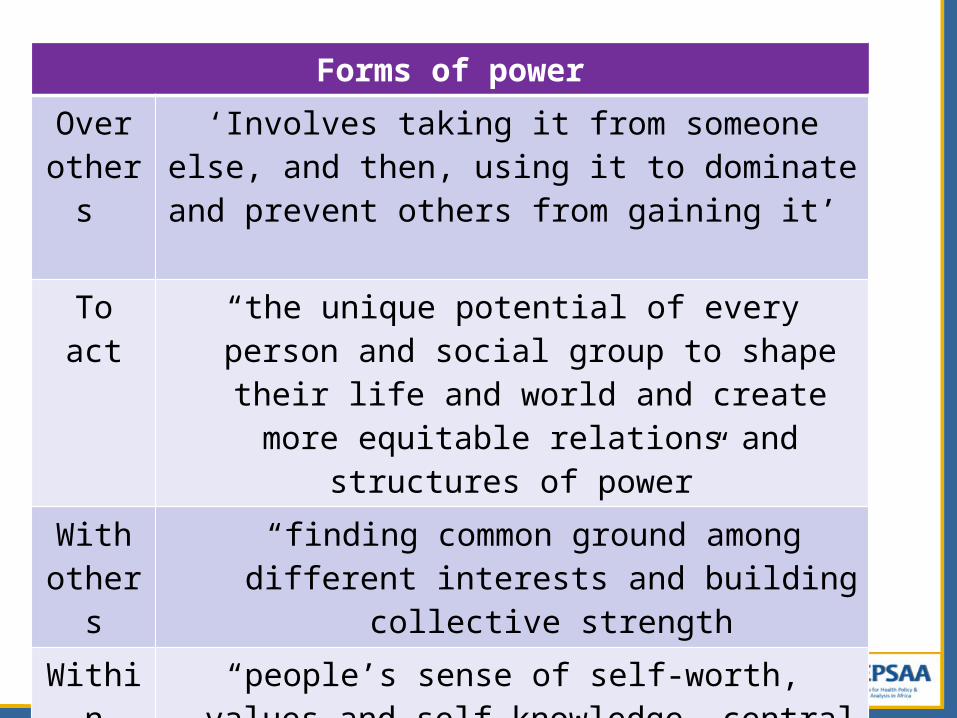
Forms of power
Over others
‘Involves taking it from someone else, and then, using it to dominate and prevent others from
gaining it’
To act “the unique potential of every person and social group to shape their life and world and create
more equitable relations and structures of power”
With others
“finding common ground among different interests and building collective strength
Within “people’s sense of self-worth, values and self-knowledge, central to individual and group
understanding of being citizens with rights and responsibilities”

Sources of power
Personal Organisational
Context:Personal, Group, Organisational, Societal
Implications for systems functioning?

Agents influence system change
The Dynamic Responses Model
Health worker
dynamic responses
De-jure system
De-facto system
Formal health system
Health system as experienced
by patients
Ssengooba et al. 2007

The software matters, in interaction with hardware
Hardware:
Tangible software:
Intangible software:capabilities to commit and engage; adapt & self-renew; balance diversity and coherence
Organ-isational hierarchy
HR estab-
lishment
Technology
Finance
Management knowledge
and skills
Formal management
processesValues &norms
Informal rules
Relation-ships
Comm-unicatio
n
Adapted from Aragon, 2010

Pathways of change are unpredictable
Health system
Intervention

Virtuous or Vicious feeedback loops?
SUPERVISOR PROVIDERS PATIENTS
Acceptability & Trust
Abusive patient-provider
interactions

Example: South African rural allowance
(Ditlopo et al, 2011)Rural allowance introduced 2004, payments awarded retrospectively to July 2003, intended to support rural HR motivation & retention• Impacts?
– Some positive impacts on recruitment BUT– Junior nurses felt undervalued and dissatisfied– Impact of financial incentives short-lived &
inadequate by selvesWhy?
Low relative to total salary & remoteness not considered; perceived as divisive & not poorly
communicated

Change in complex systems
• Change is emergent within organisations – influenced by context; unpredictable, dynamic, non-linear; with unintended consequences that can reinforce or counteract change interventions (Balogun 2006)
Wrap up: All system agents
• Have power to take decisions that influence change in system – are not just robots; have minds of their own!
• Operate within contexts that – influence their mindsets – shape their interests & power relative to
others
• So, organisational change is emergent & unpredictable

Copyright
Funding
You are free:To Share – to copy, distribute and transmit the work
To Remix – to adapt the work
Under the following conditions:Attribution You must attribute the work in the manner specified by the author or licensor (but not in any way that suggests that they endorse you or your use of the work).
Non-commercial You may not use this work for commercial purposes.
Share Alike If you alter, transform, or build upon this work, you may distribute the resulting work but only under the same or similar license to this one.
Other conditionsFor any reuse or distribution, you must make clear to others the license terms of this work.
Nothing in this license impairs or restricts the authors’ moral rights.
Nothing in this license impairs or restricts the rights of authors whose work is referenced in this document.
Cited works used in this document must be cited following usual academic conventions.
Citation of this work must follow normal academic conventions. Suggested citation:
Introduction to Complex Health Systems, Presentation 5. Copyright CHEPSAA (Consortium for Health Policy & Systems Analysis in Africa) 2014, www.hpsa-africa.org www.slideshare.net/hpsa_africa
This document is an output from a project funded by the European Commission (EC) FP7-Africa (Grant no. 265482). The views expressed are not necessarily those of the EC.

The CHEPSAA partners
University of Dar Es SalaamInstitute of Development Studies
University of the WitwatersrandCentre for Health Policy
University of GhanaSchool of Public Health, Department of Health Policy, Planning and Management
University of LeedsNuffield Centre for International Health and Development
University of Nigeria Enugu Health Policy Research Group & the Department of Health Administration and Management
London School of Hygiene and Tropical MedicineHealth Economics and Systems Analysis Group, Depart of Global Health & Dev.
Great Lakes University of KisumuTropical Institute of Community Health and Development
Karolinska InstitutetHealth Systems and Policy Group, Department of Public Health Sciences
University of Cape TownHealth Policy and Systems Programme, Health Economics Unit
Swiss Tropical and Public Health InstituteHealth Systems Research Group
University of the Western CapeSchool of Public Health


















