reCoA risk factors
9
369 Risk Factors for Recoarctation and Results of Reoperation: A 40-Year Review Ali Dodge-Khatami, M.D., Carl L. Backer, M.D., and Constantine Mavroudis, M.D. Division of Cardiovascular-ThoracicSurgery, The Children 's Memorial Hospital, Chicago, Illinois, and Department of Surgery, Northwestern University Medical School, Chicago, Illinois ABSTRACT Background: We analyzed a single institution 40-year experience with children that had coarctation repair to define risk factors for recoarctation and to evaluate the results of reoperation for recoarctation. Material and Methods: Between 1957 and 1998,271 patients had primary surgical repair of coarctation of the aorta. Techniques for primary repair included Gore-tex patch aortoplasty (PATCH; n = 1181, resection with extended end-to-end anasto- mosis (RXEEA; n = 691, subclavian flap aortoplasty (SFA; n = 611, resection with simple end- to-end anastomosis (ETE; n = 181, resection and interposition graft (n = 41, and extra- anatomic graft (n = 1 ). Techniques for recoarctation repair included PATCH, interposition graft, and extra-anatomic graft. Results: Median age at initial repair was 156 days. Major as- sociated cardiac anomalies were present in 96 patients (35%). A hypoplastic aortic arch was present in 37 patients (14%). There were three early deaths (1%) and six late deaths (2%). One patient had paraplegia (0.4%). Recoarctation occurred in 29 patients (11%) and was most frequent with ETE and SFA repairs (33% and 20%, respectively). Multiple logistic re- gression analysis revealed ETE repair (p = 0.0002), SFA repair (p = 0.0491, and aortic arch hypoplasia (p = 0.0001) to be risk factors for recoarctation. Using PATCH as the covariate, the odds ratio t o develop recoarctation was 3.5 for SFA, 17.2 for ETE, and 15.2 for hypoplastic aortic arch. There was no mortality or paraplegia after recoarctation repair (n = 23). Six pa- tients had seven balloon angioplasties; two of these patients later required reoperation. Three patients required a second reoperation for persistent coarctation. Conclusions: In our 40-year review, simple end-to-end anastomosis and subclavian flap repair had the highest incidence of recoarctation, especially when associated with aortic arch hypoplasia. We rec- ommend resection with extended end-to-end anastomosis for repair of neonates and infants and Gore-tex patch aortoplasty for children over the age of 1 year. Surgical repair of recur- rent coarctation is safe, effective, and has a low incidence of persistent coarctation. (J Card Surg 2000; 15:369-377) This material was presented at the 13th Annual Meeting of the European Association for Cardio-thoracic Surgery, Glasgow, Scotland, September 5-8, 1999 Address for correspondence: Carl L. Backer, M.D., Children's Memorial Hospital, 2300 Children's Plaza, m/c 22, Chicago, IL 6061 4. Fax: (773) 880-3054; e-mail: [email protected]
-
Upload
ali-dodge-khatami-md-phd -
Category
Documents
-
view
141 -
download
0
Transcript of reCoA risk factors

369
Risk Factors for Recoarctation and Results of Reoperation: A 40-Year Review Ali Dodge-Khatami, M.D., Carl L. Backer, M.D., and Constantine Mavroudis, M.D.
Division of Cardiovascular-Thoracic Surgery, The Children 's Memorial Hospital, Chicago, Illinois, and Department of Surgery, Northwestern University Medical School, Chicago, Illinois
ABSTRACT Background: We analyzed a single institution 40-year experience with children that had coarctation repair t o define risk factors for recoarctation and t o evaluate the results of reoperation for recoarctation. Material and Methods: Between 1957 and 1998,271 patients had primary surgical repair of coarctation of the aorta. Techniques for primary repair included Gore-tex patch aortoplasty (PATCH; n = 1181, resection with extended end-to-end anasto- mosis (RXEEA; n = 691, subclavian flap aortoplasty (SFA; n = 611, resection with simple end- to-end anastomosis (ETE; n = 181, resection and interposition graft (n = 41, and extra- anatomic graft (n = 1 ). Techniques for recoarctation repair included PATCH, interposition graft, and extra-anatomic graft. Results: Median age at init ial repair was 156 days. Major as- sociated cardiac anomalies were present in 96 patients (35%). A hypoplastic aortic arch was present in 37 patients (14%). There were three early deaths (1%) and six late deaths (2%). One patient had paraplegia (0.4%). Recoarctation occurred in 29 patients (11%) and was most frequent with ETE and SFA repairs (33% and 20%, respectively). Multiple logistic re- gression analysis revealed ETE repair (p = 0.0002), SFA repair (p = 0.0491, and aortic arch hypoplasia (p = 0.0001) t o be risk factors for recoarctation. Using PATCH as the covariate, the odds ratio t o develop recoarctation was 3.5 for SFA, 17.2 for ETE, and 15.2 for hypoplastic aortic arch. There was no mortality or paraplegia after recoarctation repair (n = 23). Six pa- tients had seven balloon angioplasties; t w o of these patients later required reoperation. Three patients required a second reoperation for persistent coarctation. Conclusions: In our 40-year review, simple end-to-end anastomosis and subclavian flap repair had the highest incidence of recoarctation, especially when associated with aortic arch hypoplasia. We rec- ommend resection with extended end-to-end anastomosis for repair of neonates and infants and Gore-tex patch aortoplasty for children over the age of 1 year. Surgical repair of recur- rent coarctation is safe, effective, and has a l o w incidence of persistent coarctation. (J Card Surg 2000; 15:369-377)
This material was presented at the 13th Annual Meeting of the European Association for Cardio-thoracic Surgery, Glasgow, Scotland, September 5-8, 1999 Address for correspondence: Carl L. Backer, M.D., Children's Memorial Hospital, 2300 Children's Plaza, m/c 22, Chicago, IL 6061 4. Fax: (773) 880-3054; e-mail: [email protected]
370 DODGE-KHATAMI. ET AL. RISK FACTORS FOR RECOARCTATION
J CARD SURG 2000;15:369-377
INTRODUCTION
Coarctation of the aorta was first successfully repaired by Crafoord in 1944.' Since that first pro- cedure there have been multiple different surgi- cal procedures described for coarctation, all of which have their individual advantages and disad- vantages. In most current reviews of coarctation repair operative mortality is almost exclusively secondary to associated cardiac anomalies, but recoarctation continues to be a problem. Re- coarctation has been reported to occur in a num- ber of children in surgical series despite many dif- ferent technique^.^,^ Close follow-up of these patients, with more widespread use of sophisti- cated noninvasive diagnostic methods (Doppler echocardiography, magnetic resonance imaging, exercise studies) have revealed a higher inci- dence of recoarctation than was often previously s ~ s p e c t e d . ~ The initial type of repair remains per- haps the single most important alterable part of an equation that includes the child's age, arch anatomy, and associated cardiac anomalies. The quest continues for the optimal first surgical re- pair that will provide the patient with the lowest operative mortality and freedom from recoarcta- tion or other complications of the repair. Although the reported results of reoperation for recoarcta- tion are good, 4-6 some centers use balloon an- gioplasty as the initial procedure of choice for re- c~arctat ion.~ We reviewed the various surgical techniques utilized at our hospital since 1957 and attempted to use this 40 year experience to de- fine risk factors associated with recoarctation. We also evaluated the risks and results of re- coarctation surgery in our patients.
MATERIAL AND METHODS
Between 1957 and 1998, 271 patients pre- senting with coarctation of the aorta underwent primary surgical repair at the Children's Memorial Hospital, Chicago, Illinois, U.S.A. Surgical tech- niques included Gore-tex (W.L. Gore and Associ- ates, Inc. Phoenix, AZ, USA) patch aortoplasty (PATCH, n = 1181, resection with extended end- to-end anastomosis (RXEEA, n = 691, subclavian flap aortoplasty (SFA, n = 611, resection with simple end-to-end anastomosis (ETE, n = 181, re- section and interposition graft (n = 41, and extra anatomic graft (n = 1). Some of the patients un- dergoing PATCH and RXEEA have been previ-
ously r e p ~ r t e d . ~ , ~ During this time period one pa- tient had percutaneous balloon angioplasty as the primary therapy for coarctation. The simple ETE repair was primarily used from 1957 to 1980, SFA from 1980 to 1990, PATCH with Dacron from 1970 to 1978, PATCH with Gore-tex from 1979 to the present and RXEEA from 1991 to the present. For the sake of statistical relevance, the four ma- jor surgical types (PATCH, RXEEA, SFA, and ETE) were used for the analysis that follows. Statistical analysis included Chi-square test, Fisher's Exact test, and survival analysis using the Kaplan-Meier method and Cox's proportional hazards model. Dr. Edwin H. Chen was our statistician. Recoarc- tation was considered as the endpoint for com- paring surgical types and Gore-tex patch aorto- plasty was the covariate. Long-term follow-up (> 1 year) was available for 142 patients (52% of the total surgical population) with a median follow-up of 5.2 years. The follow-up in general is much bet- ter in the more recent cohorts (PATCH, RXEEA) than for the earlier cohorts (SFA, ETE). We realize this is a weakness of our review, but this is in our opinion an inherent problem with a 40-year re- view. In many cases, with people moving, there are no forwarding phone numbers or addresses.
RESULTS
Median age at initial repair was 156 days (range 1 day-17.1 years). Major associated cardiac anom- alies were present in 96 cases (35%). Operative mortality occurred in 3 patients (1 YO). One 4 day old had transposition of the great arteries, ventric- ular septa1 defect, hypoplastic aortic arch, coarc- tation, and juxtaposed atrial appendages. That child underwent initial Gore-tex patch aortoplasty, had arterial switch 6 days after coarctation repair, and expired 6 days later. A 5-month-old child had Gore-tex patch aortoplasty through a left thoraco- tomy followed 2 days later by repair of a complete atrioventricular canal defect. The patient under- went mitral valve replacement on postoperative day 9 because of mitral stenosis, and died the next day of cardiac failure. A 7 day old had simul- taneous repair of coarctation with RXEEA and VSD closure. The child was taken to the operating room while on ECMO for meconium aspiration, and died of respiratory failure 26 days post-op.
There were five late cardiac deaths and one late noncardiac death (2%). Morbidity after initial repair occurred in 28 patients (10%). There was
J CARD SURG 2000;15:369-377
DODGE-KHATAMI, ET AL. 371 RISK FACTORS FOR RECOARCTATION
one instance of paraplegia (0.4%). That child was a 7 year old that had ETE repair in 1973. Initial clamp time was 30 minutes. There was major bleeding necessitating a second aortic clamp ap- plication (10 minutes). Because of a high gradient across the ETE repair (48 mm Hg), a Dacron patch was placed anteriorly during a third aortic clamp (25 minutes). The child was noted to be para- plegic immediately postop. Morbidity included temporary left vocal cord paralysis (n = 6; 2%), paradoxical hypertension requiring prolonged in- travenous antihypertensive agents (n = 9; 3%), chylothorax (n = 4;1.5%), seizures and/or intrac- erebral hemorrhage (n = 4; 1.5%), short left arm after subclavian flap (n = 2; 1 YO), necrotizing enterocolitis (n = 1 ; 0.4%) and supraventricular arrhythmia (n = 1; 0.4%). There were three in- stances of aortic aneurysm; two false aneurysms after Dacron patch and Gore-tex Patch, and one true aneurysm after SFA. All were noted as an en- largement of the mediastinum on follow-up CXR. They were successfully repaired through a left thoracotomy using partial cardiopulmonary by- pass (2) and through a median sternotomy using cardiopulmonary bypass with circulatory arrest (1 ) between 1 and 4 months postoperatively.
Aortic arch hypoplasia was defined as fol- I o w s . ~ ~ The aortic arch was divided into three parts: the proximal transverse arch, the distal transverse arch, and the aortic isthmus. The prox- imal transverse arch was hypoplastic when the di- ameter was 60% or less than the ascending aorta, the distal transverse arch and isthmus were hypoplastic when their diameter was less than 50% and 40% respectively of the ascending aorta. A hypoplastic aortic arch was present in 37 cases (14%). Almost half (14/30) of the patients with recoarctation initially presented with a hy- poplastic aortic arch. The highest percentage of hypoplastic aortic arch was found in the group un- dergoing RXEEA repair, which best addresses this coexisting obstructive lesion. Recurrent coarctation developed in 29 patients (1 1 Yo). This was defined as an arm-leg blood pressure gradi- ent > 20 mm Hg. Recoarctation occurred most frequently in patients having undergone ETE at initial repair (6 of 181, 33%. This was followed by SFA (12 of 611, 20%, RXEEA (5 of 69), 7%, and lastly by PATCH (6 of 118), 5%. Mean interval to reoperation for recurrent coarctation was 2.7 years (0.1-1 1.3 years). Redo surgical correction included PATCH (n = 131, extra-anatomic pros-
thetic graft (n = 41, RXEEA (n = 31, interposition graft (21, and SFA (n = 1). Six patients had seven balloon angioplasties. Two of these 6 patients later required surgical reintervention. One child had simultaneous VSD closure and resection of coarctation with end-to-end anastomosis at age 10 months, balloon angioplasty of a recurrent coarctation at age 6, and re-resection with hemashield graft interposition at age 17 years. The other child had coarctation resection and end- to-end anastomosis at age 5 years, balloon an- gioplasty of recurrent coarctation at age 6, and patch aortoplasty at age 7. There was no surgical mortality in reoperation for recurrent coarctation and no major morbidity (no paraplegia) was sus- tained. In 3 patients, a second reoperation was required for persistent recoarctation. Two pa- tients had SFA as their first operation, one a patch (ages 2, 10 and 15 days). The second operations were PATCH and left carotid to aorta conduit (2). The third operations were PATCH (2) and as- cending to descending aortic conduit. The mean interval to repeat reoperation surgery was 5.4 years. Using Fischer's Exact Test, univariate analysis revealed surgical repair type, hypoplastic aortic arch and young age at initial repair (< 30 days) to be risk factors for recoarctation (p < 0.001, p < 0.001 and p < 0.003, respectively). These 3 variables appear to be interdependent, as infants tend to have a higher incidence of aortic arch hypoplasia and more severe coarctation. To further delineate these factors, multiple logistic regression analysis isolated patch aortoplasty (which had the lowest incidence of recoA = 5.1 YO) as its reference point (covariate). The odds ratio to develop recoarctation relative to PATCH was 3.47 for subclavian flap aortoplasty (p = 0.0491, 17.2 for end-to-end anastomosis (p = 0.0002), and 15.2 for hypoplastic aortic arch (p = 0.0001). Young age (< 30 days) carried a risk ten- dency towards recoarctation with a 2.3 odds ra- tio, but was not statistically significant (p = 0.12).
To further analyze outcome between types of surgical repair and age, the 2 operations reserved mostly for infants and children < 1 year old, namely RXEEA and SFA were compared. This was done in view of the fact that 63/69 = 91% of all RXEEAs and 58/61 = 95% of all SFAs in our series were un- der 1 year of age. Freedom from reoperation for re- coarctation after RXEEA repair was superior to SFA (p = 0.04, log-rank test) with a 1 year reoperation probability of 12% (RXEEA) versus 23% (SFA).

372 DODGE-KHATAMI, ET AL. RISK FACTORS FOR RECOARCTATION
J CARD SURG 2000: 15:369-377
Similar results were found when hypoplastic arch was added as the covariate (p < 0.001). As ex- pected, very similar results emerged when only neonates (< 30 days old) in both RXEEA and SFA repair groups were considered. Neonates having SFA were at a 6.3 times higher risk of reoperation (95% confidence Interval [CII; 1.6-24.7) than neonates having RXEEA (adjusted for hypoplastic arch). Hypoplastic arch infants were at 7.3 times higher risk of reoperation (95% CI; 1.9-28.3) when adjusted for surgery type. No significant difference was found between RXEEA and PATCH (p = 0.64).
DISCUSSION
The goal of our historical review of patients un- dergoing coarctation repair at Children's Memor- ial Hospital (CMH) was to determine what the risk factors were for recoarctation -the single most specific postoperative complication still de- scribed. Our review of 271 patients having four major different types of repair revealed that the highest incidence of recoarctation was after ETE, the next highest after SFA. Recurrence was more common in infants < 30 days of age and in infants
with a hypoplastic aortic arch. The lowest inci- dence of recoarctation was after RXEEA (an op- eration for neonates and infants) and PATCH (an operation for older children). A possible weak- ness of our analysis is that long-term follow-up is only available for 52% of the total patient popula- tion. This weakness is balanced by the fact that the patients that had the highest number of re- coarctations are also those with the poorest fol- low-up. Most of the early patients in the series (with relatively poor long-term follow-up) had ETE or SFA, while the more recent cohort (with ex- cellent follow-up available) had the lowest re- coarctation rate. Hence, missing recoarctation in the earlier patients would only further condemn ETE and SFA, and we are confident we have not missed recoarctation in the PATCH and RXEEA patients. We also examined our results with re- coarctation surgery, which were good-no signif- icant morbidity, no mortality, and a 10% inci- dence of persistent coarctation.
The first surgical repair of coarctation as re- ported by Crafoord and Nylin in 1944 consisted of coarctation resection and end-to-end anastomo- sis (ETE)' (see Fig. 1). The high incidence of re-
Figure 1. Resection and simple end-to-end anastomosis. Dotted lines indicate area of coarctation which is to be re- sected. The ductus is ligated, the coarctation resected, and end-to-end anastomosis distal to the left subclavian artery is performed.

J CARD SURG 2000;15:369-377
DODGE-KHATAMI, ET AL. 373 RISK FACTORS FOR RECOARCTATION
TABLE 1 Meta-Analysis of Published Results of
Coarctation Repair Number
Procedure of Patients Mortality Recoarctation
Resection with 395 56 (1596) 72 (l8Y0) end-to-end anastomo- ~1~2.3.11-15
Patch aorto- 721 32 (5%) 43 (6%) plasn/2,8.17-21
flap2.13.2528 Subclavian 436 56 (130/0) 63 (15%)
Resection with 507 34 (7%) 37 (7%) extended end-to-end anastomo- ~1~3,9,15.31-33
coarctation noted on long term follow-up became a concern and a catalyst towards other tech- niques. The incidence of recoarctation after sim- ple ETE is reported to be between 6 and 86%.2.3.11-15 The meta-analysis shown in Table 1 demonstrates that in 395 patients that under-
went ETE, there was a mortality rate of 15% and a recurrence rate of 18%. Although we had no mortality after ETE, our recurrence rate was 33%. In our series the one instance of paraplegia oc- curred after ETE. This resulted from tension on the suture line which led to bleeding which re- quired a second clamp application. This resulted in stenosis at the anastomosis requiring a 3rd clamp application and patch placement. The total clamp time exceeded one hour and presumably was the etiology of the paraplegia. The high rate of recoarctation after simple ETE has been attrib- uted variously to inadequate resection of ductal tissue which later involutes, lack of growth at a circumferential suture line, and failure to address the often associated hypoplastic arch.
Vosschulte16 reported the patch aortoplasty technique in 1961 (see Fig. 2). The incidence of recoarctation reported after PATCH repair ranges from 2 to 21 %.2-8,17-21 In the meta-analysis sum- mary displayed in Table 1 (n = 7211, the overall mortality of PATCH was 5%, the recoarctation rate was 6%. There does appear to be a high in- cidence of ReCoA in neonates after PATCH, 21- 50% in several series2r8-22 making this technique
/
Figure 2. Patch aortoplasty. Dotted lines indicate where aorta is to be incised across the coarctation. The coarcta- tion ridge is not excised, collaterals are controlled, not divided. The Gore-tex patch is sutured in place as shown, up on to the left subclavian artery and distal to the collateral insertion.
374 DODGE-KHATAMI, ET AL. RISK FACTORS FOR RECOARCTATION
J CARD SURG 2000;15:369-377
a poor choice for neonates. Advantages of this approach in older children include avoiding exten- sive dissection and relatively short cross-clamp times. The technique allows for preservation of collaterals and a tension-free anastomosis. A po- tential complication of PATCH is the possibility of aneurysm formation on the side of the aorta op- posite of the patch. Resection of the coarctation “ridge” in early surgical series was implicated in weakening the aortic wall, making it more prone to develop an aneurysrn.l9,23 It is important to note a significant difference in aneurysm forma- tion according to the material used for the patch. Using a Dacron patch, the incidence of aneurysm formation is 5 - 1 3 ? 4 0 . ~ ~ , ~ ~ Using PTFE, there has been only one report of aneurysm formation in 326 patients.8 We have used PTFE for the patch material a t Children’s Memorial Hospital since 1979, and none of those patients has required re- operation for a true aneurysm. One patient re- quired reoperation for a false aneurysm related to a needle hole leak. The highest incidence of aneurysm formation after PATCH has been re- ported when this technique is used in adults with
a long-standing coarctation.18 We have used in- terposition grafts in adults for this very reason.
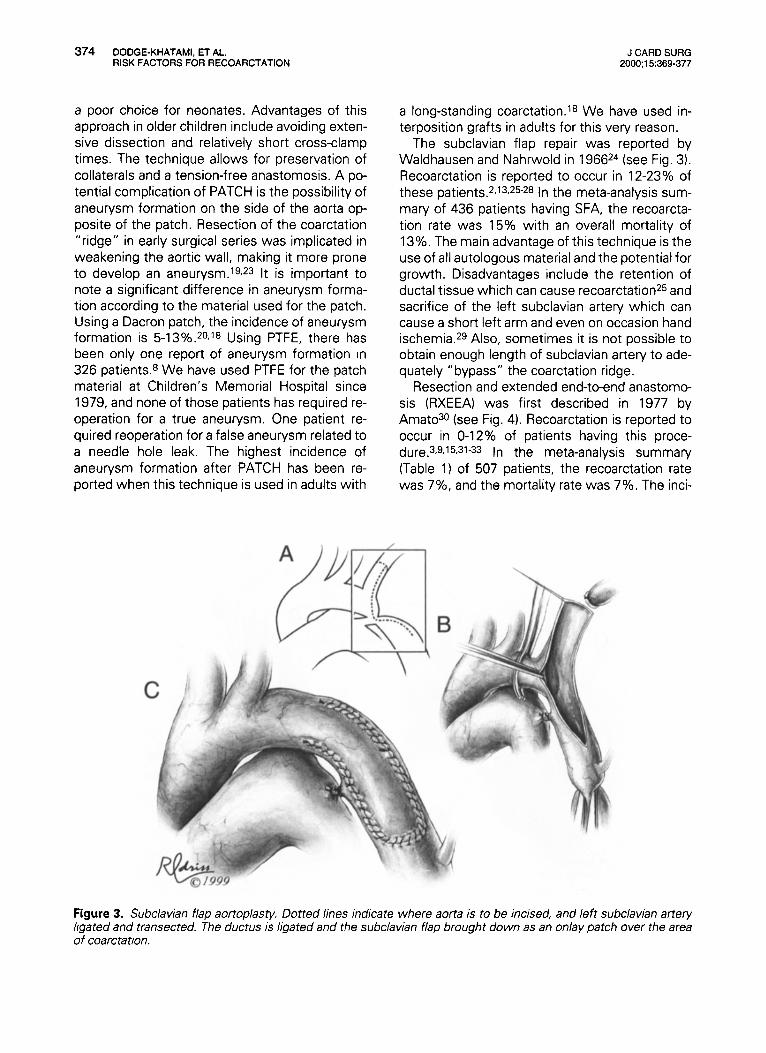
The subclavian flap repair was reported by Waldhausen and Nahrwold in 196624 (see Fig. 3). Recoarctation is reported to occur in 12-23% of these patients.2.13-25-28 In the meta-analysis sum- mary of 436 patients having SFA, the recoarcta- tion rate was 15% with an overall mortality of 13%. The main advantage of this technique is the use of all autologous material and the potential for growth. Disadvantages include the retention of ductal tissue which can cause rec~arc ta t ion~~ and sacrifice of the left subclavian artery which can cause a short left arm and even on occasion hand ischemia.29 Also, sometimes it is not possible to obtain enough length of subclavian artery to ade- quately ”bypass“ the coarctation ridge.
Resection and extended end-to-end anastomo- sis (RXEEA) was first described in 1977 by Amat030 (see Fig. 4). Recoarctation is reported to occur in 0-12% of patients having this proce- dure.3,9,15,31-33 In the meta-analysis summary (Table 1) of 507 patients, the recoarctation rate was 7%, and the mortality rate was 7%. The inci-
Figure 3. Subclavian flap aortoplasty. Dotred lines indicare where aorta is to be incised, and left subclavian artery ligated and transected. The ductus is ligated and the subclavian flap brought down as an onlay parch over the area of coarctation.

J CARD SURG 2000;15:369-377
DODGE-KHATAMI, ET AL. 375 RISK FACTORS FOR RECOARCTATION
Figure 4. Resection with extended end-to-end anastomosis. Dotted lines show area of coarctation resection and incisions in transverse arch and descending aorta. The ductus is ligated and a long oblique anastomosis is con- structed between the undersurface of the transverse arch and the descending thoracic aorta.
dence of recoarctation is higher in patients with more severe aortic arch hypoplasia (1 2% recoarc- tation hypoplastic arch vs. 2% recoarctation if nor- mal archl.32 Advantages of this repair include the resection of all ductal tissue, correction of arch hy- poplasia, the use of autologous tissue allowing growth, and the preservation of the subclavian artery. Disadvantages include possible tension on the suture lines with resultant bleeding and a po- tentially increased mortality due to a more exten- sive procedure. We have also noted that care must be taken in the orientation of the two orifices to prevent torsion on the transverse arch.
The results of reoperation for recurrent coarc- tation were quite good in our series. Technique of reoperation was most commonly PATCH or prosthetic graft (interposition or extra-anatomic). Twenty-nine patients underwent reoperation (n = 23) and/or balloon dilation (7 dilations in 6 pa- tients) with no mortality and no paraplegia. Two of the patients having balloon dilation eventually required surgical reintervention. Three patients required a second reoperation for persistent re-
coarctation. All 3 of these patients had their first operation in the first 2 weeks of life. These re- sults are similar to those reported in other recent series. Kron reported 23 patients having reinter- vention (1 7 operative procedures, 6 balloons) with one procedure related death and no para- ~ l e g i a . ~ Ralph-Edwards and colleagues reported reoperation on 43 patients with 86% managed with patch aortoplasty.5 Twenty-six percent of these patients required augmentation of the transverse arch (under circulatory arrest). Mortal- ity rate was 7%, and no ischemic spinal cord in- jury occurred with either simple proximal clamp- ing or cardiopulmonary bypass.5 Sakopoulos reported reoperations in 56 patients, most with a prosthetic patch, with no deaths or major com- plications and a 96% success rate.6 The other al- ternative to surgical intervention for recurrent coarctation is balloon angioplasty. We used this technique in 6 patients, two of whom required eventual surgical intervention. Yetman and col- leagues reported an extensive review of 90 pa- tients that had balloon angioplasty for recurrent

376 DODGE-KHATAMI, ET AL. RISK FACTORS FOR RECOARCTATION
J CARD SURG 2000;15:369-377
c~arctat ion.~ Mean systolic pressure gradients were reduced from 31 to 8 mm Hg, with one death and one aortic tear requiring urgent surgi- cal intervention. Seventy-two percent of patients remained free from reintervention after balloon angioplasty. In that series, transverse arch hy- poplasia (defined as a transverse arch z-score <-2) was the primary predictor of the need for reintervention. Our current policy is to recom- mend balloon angioplasty for most recoarcta- tions and if that is unsuccessful, proceed with PATCH repair or in more complex cases interpo- sition graft via median sternotomy with car- diopul mona ry bypass.
Our review identified the following risk factors for recoarctation: younger age at operation, ETE repair, SFA repair, and aortic arch hypoplasia. Young age is a factor difficult to sort out because it is the most critical coarctation and those with associated congenital heart disease that are PGE, dependant that require early intervention. In an early review article (1984) Foster described a 38% incidence of recoarctation if initial repair was before age 3 months as compared to only 1.5% if repair was done after 3 years of age.34 In a more recent analysis (1 991 1, Messmer and colleagues found no correlation with age but implicated baseline anatomy as the major determinant of re- coarctation.22 Our results agree with Messmer's analysis as young age failed to maintain statistical significance in multivariate analysis. What is im- portant is the type of operation for these neonate and infant patients. PATCH has an excessively high recoarctation rate in this group as does sim- ple ETE and SFA. It is our conclusion that in nearly all neonates the procedure of choice should be RXEEA. Although the transverse arch will grow after procedures such as SFA and ETE, a review of the outcome of patients with a hypoplastic aor- tic arch having SFA or ETE shows a higher inci- dence of recoarctation than after a procedure which directly addresses the hypoplastic arch such as RXEEA. In our series, those patients that had RXEEA had the highest incidence of associ- ated hypoplastic transverse arch, yet they had the lowest incidence of recoarctation. For older chil- dren (> l year of age) we continue to recommend PATCH aortoplasty with PTFE because of its very low morbidity and very low incidence of recoarc- tation. If recoarctation does occur, if balloon an- gioptasty is unsuccessful, surgical repair is safe and effective.
REFERENCES
1. Crafoord C, Nylin G: Congenital coarctation of the aorta and its surgical treatment. J Thorac Surg
2. Quaegebeur JM, Jonas RA, Weinberg AD, et al: Congenital Heart Surgeons Society: Outcomes in seriously ill neonates with coarctation of the aorta: a multiinstitutional study. J Thorac Cardiovasc Surg
3. Kappetein AP, Zwinderman AH, Bogers AJ, et al: More than thirty-five years of coarctation repair: An unexpected high relapse rate. J Thorac Cardiovasc Surg 1994; 107:87-95.
4. Kron IL, Flanagan TL, Rheuban KS, et al: Incidence and risk of reintervention after coarctation repair. Ann Thorac Surg 1990;49:920-926.
5 Ralph-Edwards AC, Williams WG, Coles JC, et al: Reoperation for recurrent aortic coarctation. Ann Thorac Surg 1995;60:1303-1307.
6. Sakopoulos AG, Hahn TL, Turrentine M, et al: Surgery for congenital heart disease: recurrent aor- tic coarctation: Is surgical repair still the gold stan- dard? J Thorac Cardiovas Surg 1998;116:560-565.
7. Yetman AT, Nykanen D, McCrindle BW, et al: Bal- loon angioplasty of recurrent coarctation: A 12- year review. J Am Coll Cardiol 1997;30:811-816.
8. Backer CL, Paape K, Zales VR, et al: Coarctation of the aorta: repair with polytetrafluoroethylene patch aortoplasty. Circulation 1995;92(Suppl. 11):Il- 132-11- 136.
9. Backer CL, Mavroudis C, Zias EA, et al: Repair of coarctation with resection and extended end-to-end anastomosis. Ann Thorac Surg 1998;66:1365-1371.
10. Moulaert AJ, Bruins CC, Oppenheimer-Dekker A: Anomalies of the aortic arch and ventricular septa1 defects. Circulation 1976;53:1011-1015.
11. Cobanoglu A, Teply JF, Grunkemeier GL, et al: Coarctation of the aorta in patients younger than three months: a critique of the subclavian flap op- eration. J Thorac Cardiovasc Surg 1985;89:128- 135.
12. Korfer R, Meyer H, Kleikamp G, et al: Early and late results after resection and end-to-end anastomo- sis of coarctation of the thoracic aorta in early in- fancy. J Thorac Cardiovasc Surg 1985;89:616-622.
13. Ziemer G, Jonas RA, Perry SB, et al: Surgery for coarctation of the aorta in the neonate. Circulation
14. Brouwer MHJ, Kuntze CEE, Ebels T, et al: Repair of aortic coarctation in infants. J Thorac Cardiovasc Surg 1991 ; 101 : 1093-1 098.
15. van Heurn LW, Wong CM, Spiegellhalter DJ, et al: Surgical treatment of coarctation of aorta in infants younger than 3 months, 1985-1 990. Success of ex- tended end-to-end arch aortoplasty. J Thorac Car- drovasc Surg 1994;107:74-86.
1945;14:347-361.
1 994; 108:841-854.
1986;74(Suppl. 1):25-31.

J CARD SURG 2000;15:369-377
DODGE-KHATAMI, ET AL. 377 RISK FACTORS FOR RECOARCTATION
16. Vosschulte K: Surgical correction of coarctation of the aorta by an "isthmusplastic" operation. Thorax
17. Yee ES, Soifer SJ, Turkey K, et al: Infant coarcta- tion: a spectrum in clinical presentation and treat- ment. Ann Thorac Surg 1986;42:488-493.
18. Clarkson PM, Brandt PWT, Barratt-Boyes BG, et al: Prosthetic repair of coarctation of the aorta with particular reference to Dacron onlay patch grafts and late aneurysm formation. Am J Cardiol 1985;
19. Hehrlein FW, Mulch J, Rautenberg HW, et al: Inci- dence and pathogenesis of late aneurysm after patch graft aortoplasty for coarctation. J Thorac Cardiovasc Surg 1986;92:226-230.
20. del Nido PJ, Williams WG, Wilson GJ, et al: Syn- thetic patch angioplasty for repair of coarctation of the aorta: Experience with aneurysm formation. Circulation 1986;74(Suppl. 1):32-36.
21. Ungerleider RM: Commentary: Is there a role for prosthetic patch aortoplasty in the repair of coarc- tation? Ann Thorac Surg 1991;52:601-602.
22. Messmer BJ, Minale C, Muhler E, et al: Surgical correction of coarctation in early infancy: Does sur- gical technique influence the result? Ann Thorac Surg 1991 ;52:594-603.
23. DeSanto A, Bills RG, King H, et al: Pathogenesis of aneurysm formation opposite prosthetic patches used for coarctation repair. J Thorac Cardiovasc Surg 1987; 94:720-723.
24. Waldhausen JA, Nahrwold DL: Repair of coarcta- tion of the aorta with a subclavian flap. J Thorac Cardiovasc Surg 1966;51.532-533.
1961 ;16:338-345.
561342-346.
25. Sanchez GR, Balsara RK, Dunn JM, et al: Recurrent obstruction after subclavian flap repair of coarcta- tion of the aorta in infants. J Thorac Cardiovasc Surg 1986;91:738-746.
26. Metzdorff MT, Cobanoglu A, Grunkemeier GL, et al: Influence of age at operation on late results with subclavian flap aortoplasty. J Thorac Cardiovasc Surg 1985;89:235-241.
27. Ehrhardt P, Walker DR: Coarctation of the aorta corrected during the first month of life. Arch Dis Child 1989;64:330-332.
28. Mililken JC, Brawn WJ, Mee RB: Neonatal coarc- tation: Clinical spectrum and improved results. J Am Coll Cardiol 1990;15:78A .
29. Geiss D, Williams WG, Lindsey WK, et al: Upper extremity gangrene. A complication of subclavian artery division. Ann Thorac Surg 1980;30:487-489.
30. Amato JJ, Rheinlander HF, Cleveland RJ. A method of enlarging the distal transverse arch in infants with hypoplasia and coarctation of the aorta. Ann Thorac Surg 1977;23:261-263.
31. Lansman S, Shapiro AJ, Schiller MS, et al: Ex- tended aortic arch anastomoses for repair of coarc- tation in infancy. Circulation 1986;74(Suppl. 1):37- 41.
32. Conte S, Lacour-Gayet F, Serraf A, et al: Surgical management of neonatal coarctation. J Thorac Cardiovasc Surg 1995;109:663-675.
33. Van Son JAM, Falk V, Schneider P, et al: Repair of coarctation of the aorta in neonates and young in- fants. J Card Surg 1997;12:139-146.
34. Foster ED: Reoperation for aortic coarctation. Ann Thorac Surg 1984;38:81-89.