Recent Advances in the Treatment of Post Traumatic Stress ... · Borderline Personality Disorder...
49
Recent Advances in the Treatment of Post Traumatic Stress Disorder Jon Bisson School of Medicine Cardiff University
Transcript of Recent Advances in the Treatment of Post Traumatic Stress ... · Borderline Personality Disorder...

Recent Advances in the Treatment of
Post Traumatic Stress Disorder
Jon Bisson
School of Medicine
Cardiff University

Agenda
• What are we treating
• Psychological approaches
• Pharmacological approaches
• Treatment resistance

What Are We Treating?
• How is PTSD diagnosed?
• How does PTSD present?
• Are any symptoms more important to target than others?
• Does time of presentation matter?

Diagnosing PTSD
• DSM-IV (2000) replaced by DSM-5 in
2013
• ICD-10 (1992) to be replaced by ICD-11 in
2018
• Definition challenged by heterogeneity of
presentation and absence of diagnostic
tests

DSM-5 PTSD Criterion A
• Exposure to actual or threatened death, serious
injury, or sexual violence through:
– 1. Direct experience
– 2. Witnessing, in person
– 3. Learning of event happening to a close family
member or friend (actual or threatened death must be
violent or accidental)
– 4. Repeated or extreme exposure to aversive details
(e.g. Human remain collection, police and details of
child abuse. Not TV, etc. unless work related)

DSM-5 PTSD
• Trauma and Stressor Related Disorder
• Exposure to traumatic event
• Re-experiencing
• Avoidance
• Negative alterations in cognitions and mood
• Alterations in arousal and reactivity

ICD-11 PTSD
• 2 Re-experiencing
– Flashbacks/powerful
images & nightmares
• 2 Avoidance
– Thoughts & feelings
– Places, people, activities
• 2 Hyperarousal
– Startle & hypervigilance

ICD-11 Complex PTSD
• Emotion Regulation– Hyperactivation, de-
activation
• Negative Self-Concept– feeling diminished, defeated,
worthless,
– shame, guilt, despair
• Disturbed Relationships – difficulties in feeling close,
little interest in relationships or social engagement

Borderline Personality Disorder
• Pervasive pattern of instability of interpersonal relationships, self-image, and affects, beginning by early adulthood
• Frantic efforts to avoid real or imagined abandonment
• Extremes of idealization and devaluation
• Impulsivity• Recurrent suicidal
behaviour

Complex PTSD vs Borderline PD
• Focuses on the effects of trauma
• PTSD symptoms core element
• Trauma-focused treatment
• Stable negative self concept
• Avoidance of relationships
• High risk of suicide, suicide attempts and self-injurious behavior are salient features
• Diagnosis and effective treatment organized around these issues
• Lack of a stable self concept and fears of abandonment

PTSD Registry
• 300 and growing• NCMH participants • PTSD diagnosis or TSQ
+ve• CAPS-5, ICD-TI, ICD-TQ,
PHQ, AUDIT• Attachment, social
support, emotional regulation, coping skills, interpersonal functioning, post traumatic cognitions, MUS

PTSD Registry Participants
• Mean age 47.4 (12.3), range 16-76
• 49% female
• 95% white
• 50% married or cohabiting
• 34% in work
• Trauma characteristics– Mean age 25.4 (14.6)
– 19.1 (14.7) years since worst trauma• 14 (7.3%) MVA, 30 (15.6%) CSA, 27 (14.1%) combat
– 92 (49%) reported CPA or CSA

Diagnosis

ICD11 PTSD & Complex PTSD
0
10
20
30
40
50
60
70
Female Working Childhood Abuse
Complex PTSD
PTSD

DSM-5 & ICD-11
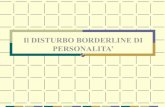
54%
10%
13%
24%

Borderline PD & ICD11 Complex PTSD

Borderline PD less age & ICD11
Complex PTSD

U.S. Prevalence
• US National Co-morbidity Survey
• > 5,500 15 to 54 year olds
• Trauma Exposure
– 60.7% M, 51.25% F
• Lifetime Prevalence
– 10.4% F, 5.0% M, 6.8%
• 12 Month Prevalence
– 3.5%
Kessler et al (1995 & 2005)

Adult Psychiatric Morbidity Survey 2014

Adult Psychiatric Morbidity Survey 2014

Co-morbidity
• Present in > 50% cases
• Commonest co-diagnoses
– Major depressive disorder
– Panic disorder
– Other anxiety disorder
– Substance abuse/dependence
• NB personality disorder

How can we prevent PTSD?

SingIe Session Early Intervention
• No certain clinical effects
for any intervention tested
in 12 RCTs
• Single session debriefing
may cause harm to some
individually debriefed
individuals
• No convincing evidence
emerging for group
debriefing
Rose et al, 2005

How can we treat PTSD?
• Psychological treatments

Psychological Treatments for PTSD
• Systematic review and meta-analysis
• Primary outcome reduction in clinician assessed severity of PTSD symptoms
• Wait list/usual care control
• 70 studies
• 4,761 participants
• Quality low overall

PsychoRx vs Waitlist
Bisson et al, 2013
Effect Size

PsychoRx vs Waitlist Dropout
0
1
2
3
4
5
6
7
TFCBT EMDR Non TFCBT GroupTFCBT
OtherTherapies
Exp TFCBT Cog TFCBT
Bisson et al, 2013

Guided Self Help

Pilot 2
• Acceptable
• Empowerment
• Refine diary

Spring


RAPID
• NIHR funded phase III RCT
• GSH vs TFCBTCT
• GSH developed through phase I & II studies
• Multi-centre
• 192 participants
• Oct 2016 – Jan 2020

How can we treat PTSD?
• Pharmacological treatments

Pharmacotherapy for PTSD
• Systematic review and meta-analysis
• Primary outcome reduction in clinician
assessed severity of PTSD symptoms
• Placebo control
• 70 studies, 5,300 participants
• Quality moderate overall

PharmacoRx vs Placebo
Hoskins et al, 2015

CAPS–SX Reductions in Means
-60
-50
-40
-30
-20
-10
0
12 week study 6 month study
Venlafaxine
Sertraline
Placebo
Davidson et al, 2006 x 2

How do we approach treatment resistant PTSD?
• Psychological
• Pharmacological
• Other

Evidence-based Practice
• Without clinical expertise, practice risks becoming tyrannised by evidence, for even excellent external evidence may be inapplicable to or inappropriate for an individual patient
• Without current best evidence, practice risks becoming rapidly out of date, to the detriment of patients
• Knowledge sources– Invention, research, innovation,
improvement, practice
Sackett et al, 1996
“Good healthcare professionals use
both individual clinical expertise and
the best available external evidence,
and neither alone is enough.”

Phased Approaches for Complex Presentations
• Phase one– Physical difficulties, accommodation, food, clothes,
money
– Emotional stabilisation• Social support
• Psychological input – stress management, skills training
• Pharmacological treatment
• Phase two– Trauma focused therapy
• Phase three– Integration to new situation

STAIR-MPE
• Phase I: Skills Training in Affective and Interpersonal Regulation (STAIR)
• Phase II: Modified Prolonged Exposure (MPE)
• 8 x one hour of each with handouts & homework
Cloitre et al, 2002

3MDR Study
• Motion-assisted, multi-modular memory desensitisation and reconsolidation
• FiMT funded Phase II RCT
• 42 participants
• Oct 2016 - Sept 2018

Background
• Urgent need to identify effective treatments for military veterans who do not respond to, or are unable to engage with, current first line treatments
• Based on therapeutic principles of virtual reality exposure therapy and EMDR
• Exposure by virtual reality, enhanced with walking, music and high affect pictures, eliminates cognitive avoidance during exposure and promotes presence

Background
• Working memory theory– Working memory has limited resources
– A dual task uses resources
– Less memory available for other processes
– Recollection of memories less vivid and less affect-laden
• Pilot research in the Netherlands– Decrease in PTSD symptoms
– No dropout or adverse effects
– Participants positive

Other Psychosocial Approaches
• Mindfulness
• Yoga
• Emotional Freedom Therapy
• Rewind Technique
• Surf Therapy

Hopwood and Schutte, 2017

Other Pharmacological Approaches
• Trazodone
• Quetiapine
• Prazosin (alpha 1 antagonist)
• Phenelzine
• Carbamazepine
• Cortisol
• Oxytocin
• D-cycloserine
• 3,4-methylenedioxy methamphetamine
Raskind et al (2013) – American Journal of Psychiatry

What would be an appropriate treatment pathway for PTSD?
• First line
• Second line
• Third line
• ? Fourth line
• When do you stop treatment?

Possible Treatment Pathway
• Full assessment• First line
– Individual TFCBT or EMDR
• Second line– Alternative TFPT, Non TFCBT, Group TFCBT,
pharmacotherapy (paroxetine, fluoxetine, sertraline or venlafaxine)
• Third line– Further pharmacotherapy (quetiapine, prazosin,
trazodone, carabmazepine)
• Other issues– To phase or not to phase
• Stabilisation
– Stepped/stratified/precision approach– Individual choice

Cardiff University Traumatic Stress
Research Group
• Kali Barawi
• Jon Bisson
• Sarah Cosgrove
• Tony Downes
• Mat Hoskins
• Neil Kitchiner
• Catrin Lewis
• Neil Roberts
• Ben Sessa
• Natalie Simon
• Rob Sinnerton
• Stan Zammitt