
RECENT ADVANCES IN MANAGEMENT OF HIE
26
RECENT ADVANCES IN TREATMENT OF HIE BY DR. TAUHID IQBALI MBBS(JIPMER) MD PED. (PMCH)
-
Upload
tauhid-iqbali -
Category
Health & Medicine
-
view
83 -
download
0
Transcript of RECENT ADVANCES IN MANAGEMENT OF HIE

RECENT ADVANCES IN TREATMENT OF HIE
BYDR. TAUHID IQBALIMBBS(JIPMER)MD PED. (PMCH)
DEFNITION OF HIE
NEONATAL ENCEPHALOPATHY
FOLLOWING SEVERE BIRTH ASPHYXIA OR PERINATAL HYPOXIA IS REFERED TO AS HIE

PATHOPHYSIOLOGY OF HIE
Pathogenesis of HIE involves cascades of events. And it consist of:
1. Primary energy failure 2. Latent phase 3. Reperfusion injury 4 .Secondary phase

PRIMARY ENERGY FAILURE SEVERE HYPOXIA
DEPLETON OF HIGH ENERGY PHOSPHATE COMPOUNDS
INCREASE RELEASE OF GLUTAMATE AT SYNAPTIC LEVEL
FAILURE OF Na+-k+ ATPase
DEPOLARIZATION OF CELL MEMBRANE
INFLUX OF Na+ INFLUX OF Ca++
OSMOTIC INFLUX OF WATER
CYTOTOXIC NEURONAL EDEMA
ACTIVATION OF INTRACELLULAR PROTEASES AND LIPASES
PRODUCTION OF:XANTHINE OXIDASENOPROSTAGLANDINS
FREE RADICAL GENERATION
NMDA RECEPTOR ACTIVATION
Ca ++ INFLUX
NEURONAL NOS ACTIVATION
INCREASE NO RELEASE
NO AND FREE RADICALS COMBINE TO FORM PEROXYNITRITE ( A HIGHLY TOXIC OXIDAND )
NECROTIC CELL DEATH OF NEURONS
LATENT PHASE
PHASE WHERE CEREBRAL METABOLISM TRANSIANTLY RECOVERS
REPERFUSION PHASE
1.ACTIVATION OF : Cyclooxygenase Xanthine oxidase Lipoxygenase
INCREASE PRODUCTION OF FREE RADICAL
2. ACCUMULATION OF NO

SECONDARY PHASE
IT INVOLVES CONTRIBUTIONS OF:
MITOCHONDRIAL DYSFUNCTION
CASPASE ACTIVATION
INFLAMATORY MEDIATORS
EXCITO TOXIC – OXIDATION CASCADES
APOPTOTIC CELL DEATH

PATHOPHYSIOLOGY OF HIE CONT. TIME LINE
SO NOW AS WE UNDERSTOOD THE CURRENT MECHANISM OF HIE !!

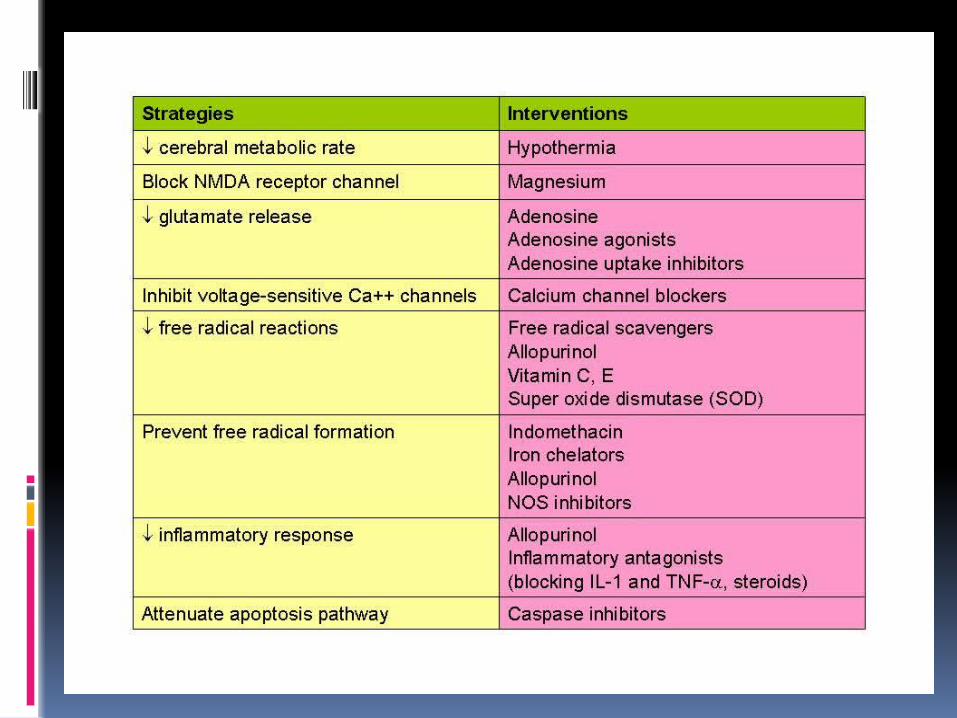
OUR STRATEGIES WOULD BE TO: DECREASE CEREBRAL METABOLIC RATE
BLOCK NMDA RECEPTOR CHANNEL
DECREASE GLUTAMATE RELEASE
INHIBIT VOLTAGE GATED Ca++ CHANNELS
DECREASE FREE RADICAL REACTIONS
PREVENT FREE RADICAL FORMATIONS
DECREASE INFLAMATORY RESPONSE
ATTENUATE APOPTOSIS CASCADES

THIS IS WHAT GIVES US HUNTING
GROUND FOR ADVANCED THERAPUTIC MODALITIES IN HIE
HYPOTHERMIA THERAPYMILD HYPOTHERMIA (3-4 degree below baseline temperature) IS
NEUROPROTECTIVE
MECHANISM OF ACTION:
1.DECREASE CEREBRAL METABOLICRATE AND ENERGY DEPLETION
2.DECREASE EXCITATORY NEUROTRANSMITTER RELEASE
3.DECREASE APOPTOSIS
4.DECREASE VASCULAR PERMEABILITY AND EDEMA
What is the optimal timing of initiation of hypothermia therapy?
Cooling must begin early, within 6 hours of injury. However, experimental evidence strongly suggest that the earlier the better.
What is the optimal duration of hypothermia therapy?
The greater the severity of the initial injury, the longer the duration of hypothermia needed.
But it should be at least used for 72 hours
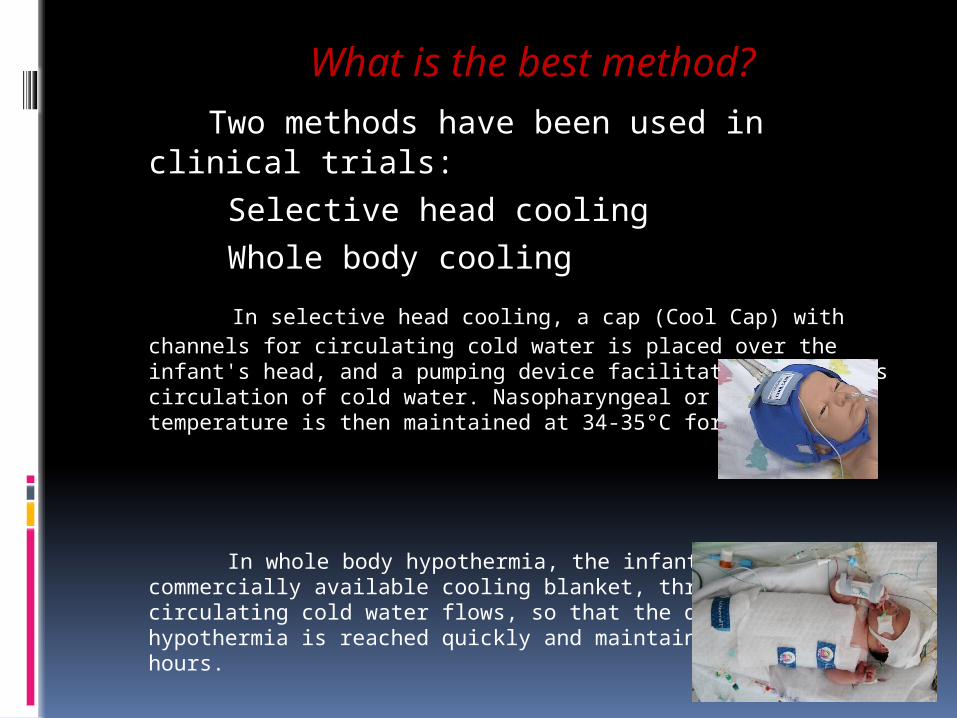
What is the best method? Two methods have been used in clinical trials:
Selective head cooling
Whole body cooling
In selective head cooling, a cap (Cool Cap) with channels for circulating cold water is placed over the infant's head, and a pumping device facilitates continuous circulation of cold water. Nasopharyngeal or rectal temperature is then maintained at 34-35°C for 72 hours
In whole body hypothermia, the infant is placed on a commercially available cooling blanket, through which circulating cold water flows, so that the desired level of hypothermia is reached quickly and maintained for 72 hours.
What is the optimal rewarming method?
Rewarming is a critical period. In
clinical trials, rewarming was carried out gradually, over 6-8 hours.

ADVERSE EFFECTS:THOUGH THEORETITAL IT INCLUDESCOAGULATION DEFECT
LEUKOCYTES MALFUNCTION
PULMONARY HYPERTENSION
WORSENING OF METABOLIC ACIDOSIS
ABNORMALITIES OF CARDIAC RHYTHM
2013 Cochrane review says
Significant adverse effect is limited to only SINUS BRADYCARDIA and THROMBOCYTOPENIA

LONG TERM OUTCOME:2012 NICHD trial Combined outcome of death and IQ score
below 70 occurred in62% of patient in control group47% of patient in hypothermia therapy group Death Control group 48%Hypothermia therapy group 28% Severe disabilityControl group 60%Hypothermia therapy group 41%
STUDIES ON THERAPUTIC HYPOTHERMIA IN HIE
A decrease in the combined outcomes of mortality/major neurodevelopmental disability at 18 months (8 studies)
A reduction in mortality (11 studies)
A reduction in neurodevelopmental disability in survivors (8 studies)
9 independent meta-analyses have confirmed a consistent and robust beneficial effect of therapeutic hypothermia for moderate-to-severe encephalopathy
OTHER NEW THERAPUTIC MODALITIESOXYGEN FREE RADICAL INHIBITOR AND SCAVENGERS
DIRECT INHIBITORS:SUPEROXIDE DISMUTASE
ENDOPEROXIDASE
CATALASE
SCAVENGERS:VITAMIN E
VITAMIN C
MANNITOL
INDIRECT INHIBITORS:INDOMETHACIN
ALLOPURINOL
CYCLOOXYGENASE
N-ACETYL CYSTEINE
MELATONIN
Study have shown promising results but their use will depend on the ability to develop appropriate delivery system that will allow action at the cellular and specific tissue site

CALCIUM CHANNEL BLOCKERSFLUNARIZINE
NIMODIPINE
These two drugs appears mot efficacious on animal study
Results of clinical trial is awaited
ERYTHROPOIETINIts neuroprotective mechanism is mediated
through:1.Direct neurotropic effect
2.Decrease susceptibility to glutamate toxicity
3. Release of antiapoptotic factors
4.Reduce inflamation
5. Decrease nitric oxide mediated injury
6.Direct antioxidant effect
Epo 5000 u/kg have shown to provide significant neuroprotection and improved outcome

EXCITATORY AMINO ACID ANTAGONISTINHIBITOR OF GLUTAMATE RELEASE:BACLOFEN
ADENOSINE
ADENOSINE AGONIST
NMDA RECEPTOR BLOCKER:MAGNESIUM
PHENCYCLIDINE
DEXTROMETHORPHAN
KETAMINE
MK- 801 EAA antagonist MK-801 , has shown promising results in experimental animals and in
a limited number of adult trials. However, this drug has serious cardiovascular adverse effects
HOWEVER
MAGNESIUM SULFATE IS A NATURAL ANTAGONIST OF NMDA WITH LESS SIDE EFFECTS SO ROLE OF MS AS A NEUROPROTECTIVE AGENT IN PREVENTION OF BRAIN DAMAGE IN HIE DESERVE ACTIVE CONSIDERATION AND EVALUATION IN FUTURE
PREVENTION OF EXCESS NITRIC OXIDE FORMATION
NOS INHIBITOR:NITROARGININE
Administration of nitroarginine in immature rats caused prolonged inhibition of NOS and thus reduction in the extent of brain injury
Agents decreasing inflamatory response:AllopurinolInflamatory antagonist IL1 blocker TNF alfa blocker

ATTENUATE APOPTOSIS PATHWAYCASPASE INHIBITORS
STEM CELL TRANSPLANTATION THERE IS EVIDENCE THAT SUGGEST NEONATE BRAIN IS
ENDOWED WITH THE CAPABILITY FOR ENDOGENOUS NEUROGENESIS FLOWING HIE
INFACT MANY EXPERIMENTAL EVIDENCES SUGGEST SCT MAY REPAIR THE DAMAGED NEURONSIN BRAIN
SEVERAL TYPES OF STEM CELLS HAVE BEEN USED IN RODENTS INCLUDING NEURONAL STEM CELLS MESNCHYMAL STEM CELLS AND HEMATOPOIETIC STEM CELLS
THERE IS EVIDENCE THAT SUGGEST THAT GENETICALLY MODIFIED STEM CELLS MAY BE MORE EFFECTIVE THAN UNMODIFIED STEM CELLS
THUS SCT HAS POTENTIAL TO BECOME A FUTURE NEUROPROTECTIVE AND REGENERATIVE THERAPY FOR HIE

THANK YOU


















