
Readmission Rate for Congestive Heart Failure Patients … · Objective Measure/Indicator Target...
10
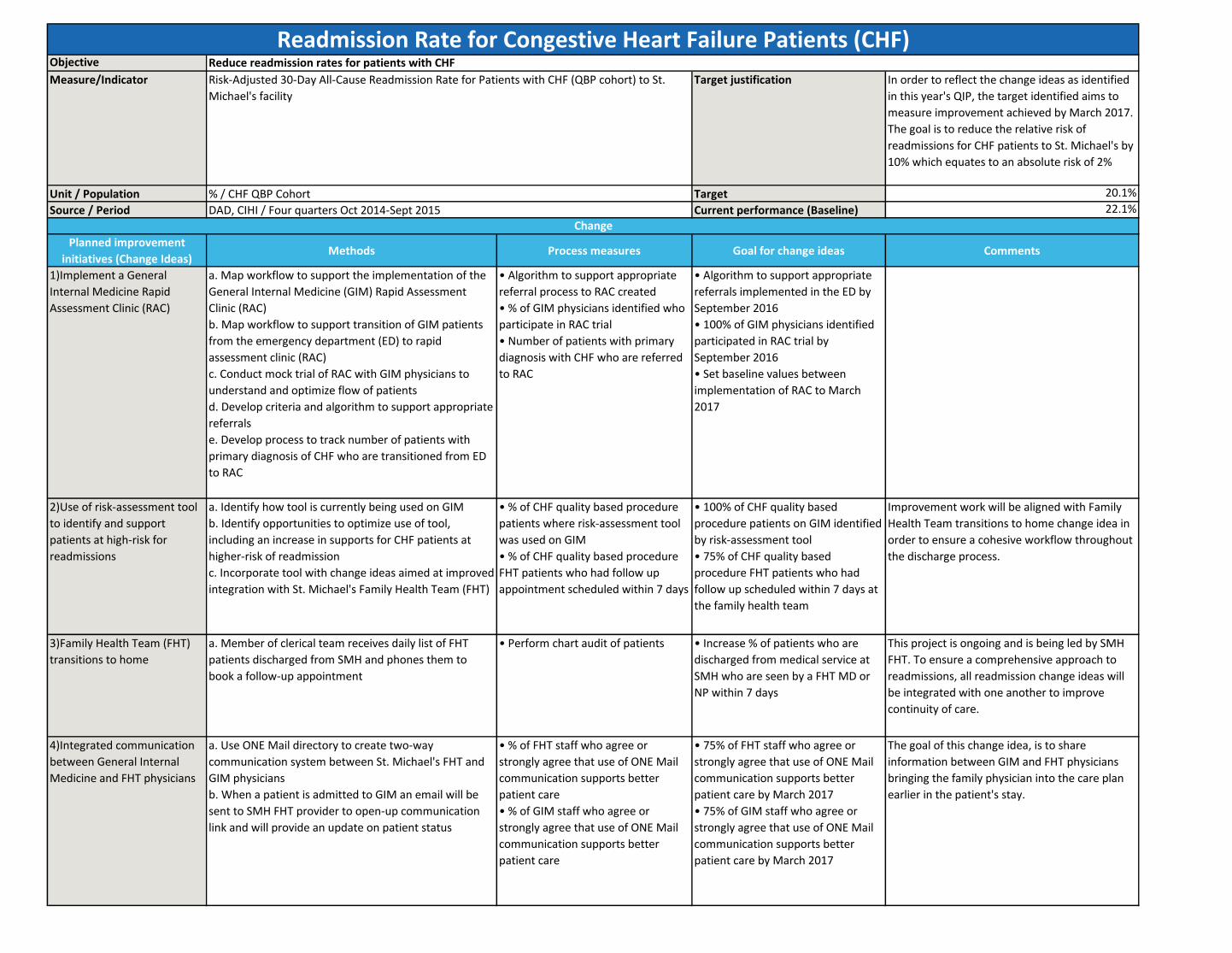
Objective Measure/Indicator Target justification In order to reflect the change ideas as identified in this year's QIP, the target identified aims to measure improvement achieved by March 2017. The goal is to reduce the relative risk of readmissions for CHF patients to St. Michael's by 10% which equates to an absolute risk of 2% Unit / Population Target 20.1% Source / Period Current performance (Baseline) 22.1% Planned improvement initiatives (Change Ideas) Methods Process measures Goal for change ideas Comments 1)Implement a General Internal Medicine Rapid Assessment Clinic (RAC) a. Map workflow to support the implementation of the General Internal Medicine (GIM) Rapid Assessment Clinic (RAC) b. Map workflow to support transition of GIM patients from the emergency department (ED) to rapid assessment clinic (RAC) c. Conduct mock trial of RAC with GIM physicians to understand and optimize flow of patients d. Develop criteria and algorithm to support appropriate referrals e. Develop process to track number of patients with primary diagnosis of CHF who are transitioned from ED to RAC • Algorithm to support appropriate referral process to RAC created • % of GIM physicians identified who participate in RAC trial • Number of patients with primary diagnosis with CHF who are referred to RAC • Algorithm to support appropriate referrals implemented in the ED by September 2016 • 100% of GIM physicians identified participated in RAC trial by September 2016 • Set baseline values between implementation of RAC to March 2017 2)Use of risk-assessment tool to identify and support patients at high-risk for readmissions a. Identify how tool is currently being used on GIM b. Identify opportunities to optimize use of tool, including an increase in supports for CHF patients at higher-risk of readmission c. Incorporate tool with change ideas aimed at improved integration with St. Michael's Family Health Team (FHT) • % of CHF quality based procedure patients where risk-assessment tool was used on GIM • % of CHF quality based procedure FHT patients who had follow up appointment scheduled within 7 days • 100% of CHF quality based procedure patients on GIM identified by risk-assessment tool • 75% of CHF quality based procedure FHT patients who had follow up scheduled within 7 days at the family health team Improvement work will be aligned with Family Health Team transitions to home change idea in order to ensure a cohesive workflow throughout the discharge process. 3)Family Health Team (FHT) transitions to home a. Member of clerical team receives daily list of FHT patients discharged from SMH and phones them to book a follow-up appointment • Perform chart audit of patients • Increase % of patients who are discharged from medical service at SMH who are seen by a FHT MD or NP within 7 days This project is ongoing and is being led by SMH FHT. To ensure a comprehensive approach to readmissions, all readmission change ideas will be integrated with one another to improve continuity of care. 4)Integrated communication between General Internal Medicine and FHT physicians a. Use ONE Mail directory to create two-way communication system between St. Michael's FHT and GIM physicians b. When a patient is admitted to GIM an email will be sent to SMH FHT provider to open-up communication link and will provide an update on patient status • % of FHT staff who agree or strongly agree that use of ONE Mail communication supports better patient care • % of GIM staff who agree or strongly agree that use of ONE Mail communication supports better patient care • 75% of FHT staff who agree or strongly agree that use of ONE Mail communication supports better patient care by March 2017 • 75% of GIM staff who agree or strongly agree that use of ONE Mail communication supports better patient care by March 2017 The goal of this change idea, is to share information between GIM and FHT physicians bringing the family physician into the care plan earlier in the patient's stay. Change Readmission Rate for Congestive Heart Failure Patients (CHF) Reduce readmission rates for patients with CHF Risk-Adjusted 30-Day All-Cause Readmission Rate for Patients with CHF (QBP cohort) to St. Michael's facility % / CHF QBP Cohort DAD, CIHI / Four quarters Oct 2014-Sept 2015
Transcript of Readmission Rate for Congestive Heart Failure Patients … · Objective Measure/Indicator Target...
Objective
Measure/Indicator Target justification In order to reflect the change ideas as identified
in this year's QIP, the target identified aims to
measure improvement achieved by March 2017.
The goal is to reduce the relative risk of
readmissions for CHF patients to St. Michael's by
10% which equates to an absolute risk of 2%
Unit / Population Target 20.1%
Source / Period Current performance (Baseline) 22.1%
Planned improvement
initiatives (Change Ideas)Methods Process measures Goal for change ideas Comments
1)Implement a General
Internal Medicine Rapid
Assessment Clinic (RAC)
a. Map workflow to support the implementation of the
General Internal Medicine (GIM) Rapid Assessment
Clinic (RAC)
b. Map workflow to support transition of GIM patients
from the emergency department (ED) to rapid
assessment clinic (RAC)
c. Conduct mock trial of RAC with GIM physicians to
understand and optimize flow of patients
d. Develop criteria and algorithm to support appropriate
referrals
e. Develop process to track number of patients with
primary diagnosis of CHF who are transitioned from ED
to RAC
• Algorithm to support appropriate
referral process to RAC created
• % of GIM physicians identified who
participate in RAC trial
• Number of patients with primary
diagnosis with CHF who are referred
to RAC
• Algorithm to support appropriate
referrals implemented in the ED by
September 2016
• 100% of GIM physicians identified
participated in RAC trial by
September 2016
• Set baseline values between
implementation of RAC to March
2017
2)Use of risk-assessment tool
to identify and support
patients at high-risk for
readmissions
a. Identify how tool is currently being used on GIM
b. Identify opportunities to optimize use of tool,
including an increase in supports for CHF patients at
higher-risk of readmission
c. Incorporate tool with change ideas aimed at improved
integration with St. Michael's Family Health Team (FHT)
• % of CHF quality based procedure
patients where risk-assessment tool
was used on GIM
• % of CHF quality based procedure
FHT patients who had follow up
appointment scheduled within 7 days
• 100% of CHF quality based
procedure patients on GIM identified
by risk-assessment tool
• 75% of CHF quality based
procedure FHT patients who had
follow up scheduled within 7 days at
the family health team
Improvement work will be aligned with Family
Health Team transitions to home change idea in
order to ensure a cohesive workflow throughout
the discharge process.
3)Family Health Team (FHT)
transitions to home
a. Member of clerical team receives daily list of FHT
patients discharged from SMH and phones them to
book a follow-up appointment
• Perform chart audit of patients • Increase % of patients who are
discharged from medical service at
SMH who are seen by a FHT MD or
NP within 7 days
This project is ongoing and is being led by SMH
FHT. To ensure a comprehensive approach to
readmissions, all readmission change ideas will
be integrated with one another to improve
continuity of care.
4)Integrated communication
between General Internal
Medicine and FHT physicians
a. Use ONE Mail directory to create two-way
communication system between St. Michael's FHT and
GIM physicians
b. When a patient is admitted to GIM an email will be
sent to SMH FHT provider to open-up communication
link and will provide an update on patient status
• % of FHT staff who agree or
strongly agree that use of ONE Mail
communication supports better
patient care
• % of GIM staff who agree or
strongly agree that use of ONE Mail
communication supports better
patient care
• 75% of FHT staff who agree or
strongly agree that use of ONE Mail
communication supports better
patient care by March 2017
• 75% of GIM staff who agree or
strongly agree that use of ONE Mail
communication supports better
patient care by March 2017
The goal of this change idea, is to share
information between GIM and FHT physicians
bringing the family physician into the care plan
earlier in the patient's stay.
Change
Readmission Rate for Congestive Heart Failure Patients (CHF)Reduce readmission rates for patients with CHF
Risk-Adjusted 30-Day All-Cause Readmission Rate for Patients with CHF (QBP cohort) to St.
Michael's facility
% / CHF QBP Cohort
DAD, CIHI / Four quarters Oct 2014-Sept 2015

Objective
Measure/Indicator Target justification In order to reflect the change ideas as identified in this
year's QIP, the target identified aims to measure
improvement achieved by March 2017. The goal is to
reduce the relative risk of readmissions for COPD
patients to St. Michael's by 10% which equates to an
absolute risk of 2%
Unit / Population Target 24.4%
Source / Period Current performance (Baseline) 26.4%
Planned improvement
initiatives (Change Ideas)Methods Process measures Goal for change ideas Comments
1)Implement a General
Internal Medicine Rapid
Assessment Clinic (RAC)
a. Map workflow to support the implementation of the
General Internal Medicine (GIM) Rapid Assessment Clinic
(RAC)
b. Map workflow to support transition of GIM patients
from the emergency department (ED) to rapid
assessment clinic (RAC)
c. Conduct mock trial of RAC with GIM physicians to
understand and optimize flow of patients
d. Develop criteria and algorithm to support appropriate
referrals
e. Develop process to track number of patients with
primary diagnosis of COPD who are transitioned from ED
to RAC
• Algorithm to support appropriate
referral process to RAC created
• % of GIM physicians identified who
participate in RAC trial
• Number of patients with primary
diagnosis with COPD who are
referred to RAC
• Algorithm to support appropriate
referrals implemented in the ED by
September 2016
• 100% of GIM physicians identified
participated in RAC trial by
September 2016
• Set baseline values between
implementation of RAC to March
2017
2)Use of risk-assessment tool
to identify and support
patients at high-risk for
readmissions
a. Identify how tool is currently being used on GIM
b. Identify opportunities to optimize use of tool,
including an increase in supports for COPD patients at
higher-risk of readmission
c. Incorporate tool with change ideas aimed at improved
integration with St. Michael's Family Health Team (FHT)
• % of COPD quality based procedure
patients where risk-assessment tool
was used on GIM
• % of COPD quality based procedure
FHT patients who had follow up
appointment scheduled within 7 days
• 100% of COPD quality based
procedure patients on GIM identified
by risk-assessment tool
• 75% of COPD quality based
procedure FHT patients who had
follow up scheduled within 7 days at
the family health team
Improvement work will be aligned with Family Health
Team transitions to home change idea in order to ensure
a cohesive workflow throughout the discharge process.
3)Family Health Team (FHT)
transitions to home
a. Member of clerical team receives daily list of FHT
patients discharged from SMH and phones them to book
a follow-up appointment
• Perform chart audit of patients • Increase % of patients who are
discharged from medical service at
SMH who are seen by a FHT MD or
NP within 7 days
This project is ongoing and is being led by SMH FHT. To
ensure a comprehensive approach to readmissions, all
readmission change ideas will be integrated with one
another to improve continuity of care.
4)Integrated communication
between General Internal
Medicine and FHT physicians
a. Use ONE Mail directory to create two-way
communication system between St. Michael's FHT and
GIM physicians
b. When a patient is admitted to GIM an email will be
sent to SMH FHT provider to open-up communication
link and will provide an update on patient status
• % of FHT staff who agree or
strongly agree that use of ONE Mail
communication supports better
patient care
• % of GIM staff who agree or
strongly agree that use of ONE Mail
communication supports better
patient care
• 75% of FHT staff who agree or
strongly agree that use of ONE Mail
communication supports better
patient care by March 2017
• 75% of GIM staff who agree or
strongly agree that use of ONE Mail
communication supports better
patient care by March 2017
The goal of this change idea, is to share information
between GIM and FHT physicians bringing the family
physician into the care plan earlier in the patient's stay.
Readmission Rate for Chronic Obstructive Pulmonary Disease (COPD)Reduce readmission rates for patients with COPD
Risk-Adjusted 30-Day All-Cause Readmission Rate for Patients with COPD (QBP cohort) to St.
Michael's facility
% / COPD QBP Cohort
DAD, CIHI / Four quarters Oct 2014-Sept 2015
Objective
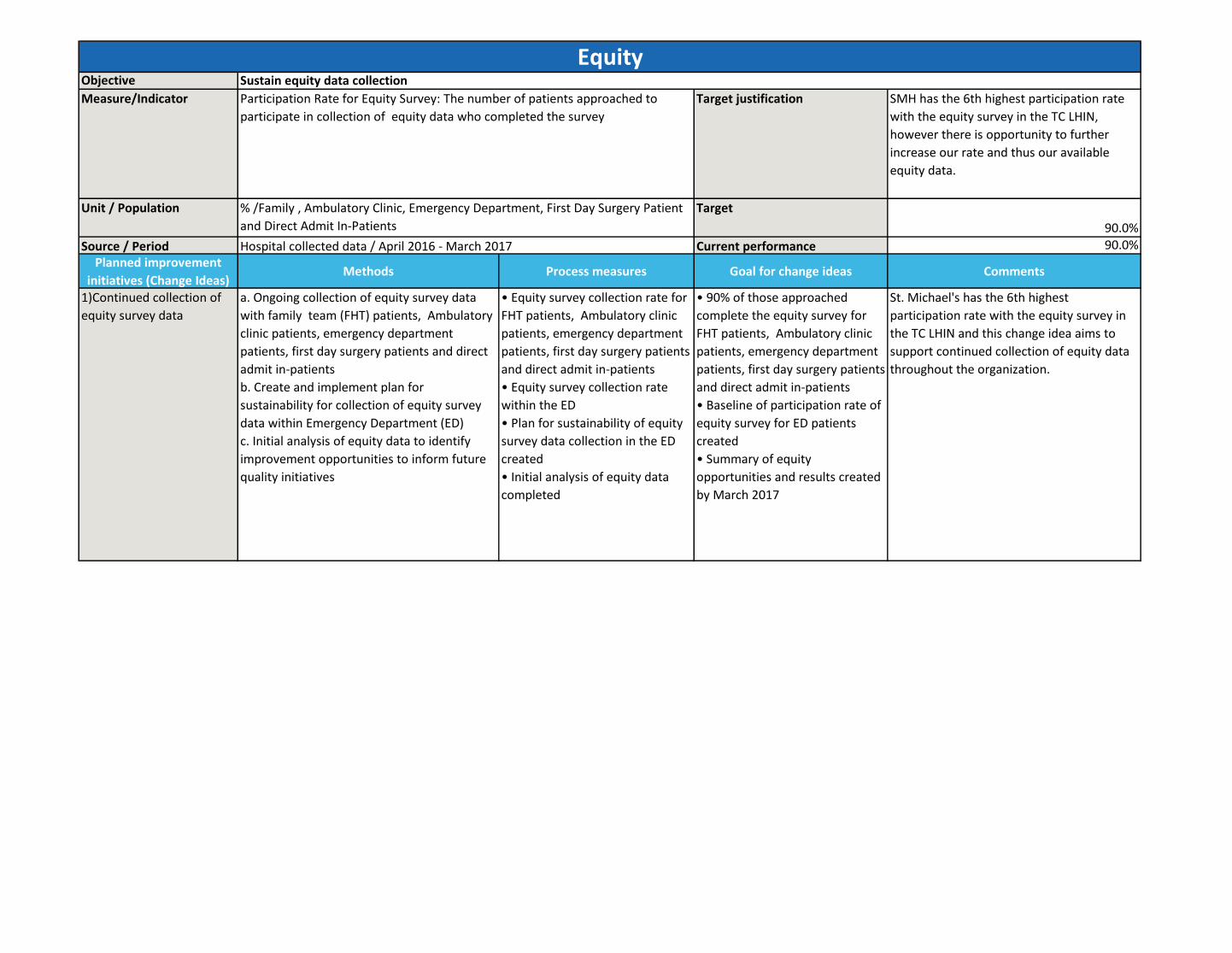
Measure/Indicator Target justification SMH has the 6th highest participation rate
with the equity survey in the TC LHIN,
however there is opportunity to further
increase our rate and thus our available
equity data.
Unit / Population Target
90.0%
Source / Period Current performance 90.0%
Planned improvement
initiatives (Change Ideas)Methods Process measures Goal for change ideas Comments
1)Continued collection of
equity survey data
a. Ongoing collection of equity survey data
with family team (FHT) patients, Ambulatory
clinic patients, emergency department
patients, first day surgery patients and direct
admit in-patients
b. Create and implement plan for
sustainability for collection of equity survey
data within Emergency Department (ED)
c. Initial analysis of equity data to identify
improvement opportunities to inform future
quality initiatives
• Equity survey collection rate for
FHT patients, Ambulatory clinic
patients, emergency department
patients, first day surgery patients
and direct admit in-patients
• Equity survey collection rate
within the ED
• Plan for sustainability of equity
survey data collection in the ED
created
• Initial analysis of equity data
completed
• 90% of those approached
complete the equity survey for
FHT patients, Ambulatory clinic
patients, emergency department
patients, first day surgery patients
and direct admit in-patients
• Baseline of participation rate of
equity survey for ED patients
created
• Summary of equity
opportunities and results created
by March 2017
St. Michael's has the 6th highest
participation rate with the equity survey in
the TC LHIN and this change idea aims to
support continued collection of equity data
throughout the organization.
EquitySustain equity data collection
Participation Rate for Equity Survey: The number of patients approached to
participate in collection of equity data who completed the survey
% /Family , Ambulatory Clinic, Emergency Department, First Day Surgery Patient
and Direct Admit In-Patients
Hospital collected data / April 2016 - March 2017

Objective
Measure/Indicator Target justification As a new survey is being implemented to capture
patient feedback (NRCC), we will be unable to
compare results between the two sources. This
year will be used to understand our current
state, develop a baseline and internal discharge
satisfaction measures.
Unit / Population TargetDeveloping Baseline
Source / Period Current performance Developing Baseline
Planned improvement
initiatives (Change Ideas)Methods Process measures Goal for change ideas Comments
1)Optimize the use of
discharge toolkit components
on Orthopaedic and Trauma
Neurosurgery Units
a. Assemble improvement working group
b. Identify gaps and opportunities to improve both
on unit processes and off unit processes related to
discharge planning
c. Plan and test improvements to discharge
planning, including improved communication tools
d. Monitor impact using performance data
• % of patients with an Estimated Date of
Discharge(EDD) entered within 24hrs of
admission
• % of patients who agree or strongly
agree they feel more prepared for
discharge after the implementation of
the discharge toolkit
• % of patients who received
preadmission EDD information
• 80% of patients have a Estimated Date
of Discharge entered within 24hrs of
admission
• 75% of patients who agree or strongly
agree they feel more prepared for
discharge after the implementation of
the discharge toolkit
• 75% of patients received
preadmission EDD information
Improvement work will be aligned with Patient
Oriented Discharge Summary(PODS) to ensure a
cohesive workflow throughout the discharge
process.
2)Implementation of Patient
Oriented Discharge
Summary(PODS) on
Orthopedic and Trauma
Neurosurgery Units
a. Work with multidisciplinary team to create
standardized PODS content for Orthopedics and
Trauma Neurosurgery units
b. Develop service specific content in the
electronic discharge system
c. Build teaching capacity in Orthopedic and
Trauma Neurosurgery staff through "Teach back"
training to enhance use of the PODS tool
d. Implement PODS tool for patients discharged
from the Orthopedic and Trauma Neurosurgery
Services
• % patient satisfaction scores related to
discharge questions on new NRC survey
• % of patients discharged that received a
Patient Oriented Discharge Summary on
Orthopedic and Trauma Neurosurgery
Units
• % of full and part time nurses on
Orthopedic and Trauma Neurosurgery
Units to receive "Teach back" patient
education training
• Develop baseline for patient discharge
satisfaction utilizing the new NRC tool
between April 2016 - March 2017
• 80% of patients discharged received a
Patient Oriented Discharge Summary on
Orthopedic and Trauma Neurosurgery
Units
• 70% of full and part time nurses on
Orthopedic and Trauma Neurosurgery
Units receive "Teach back" patient
education training
3)Develop method to collect
timely discharge satisfaction
data to inform the creation of
internal discharge satisfaction
measures
a. Conduct an internal and external review for best
practice
b. Identify question and delivery options for
patient discharge satisfaction surveys
c. Plan and test patient discharge satisfaction
collection on a small scale
d. Evaluate and improve new method for timely
discharge satisfaction data
e. Analyze data to determine best internal
measures for discharge satisfaction
• Identify method for collecting patient
discharge satisfaction feedback
• Develop content of patient discharge
satisfaction collection tool
• Create a plan to implement collection
of timely discharge satisfaction data
• Develop internal measures for
discharge satisfaction
• Identify method for collecting patient
discharge satisfaction feedback by July
2016
• Develop content of patient discharge
satisfaction collection tool by July 2016
• Implement collection of timely
discharge satisfaction data by
September 2016
• Internal measures for discharge
satisfaction developed by September
2016
In order to understand the patient's perspective
of improvement initiatives, a more timely
feedback mechanism is required. Therefore we
are committed to finding a new solution and also
developing our own internal measures for
discharge satisfaction.
Discharge Patient SatisfactionImprove patient discharge satisfaction
Discharge Patient Satisfaction: Patient satisfaction related to continuity & transition
% / All acute patients
NRC Picker / To be established

4)Develop a robust reporting
processes across discharge
continuum
a. Review of current patient flow and discharge
process indicators
b. Develop recommendations for refined
indicators and illicit feedback from staff
c. Develop mechanism and timeframes for
providing performance data
d. Explore structure to best support data sharing,
including implementing performance boards
e. Implement changes
• Refined patient flow and discharge
process indicators and targets identified
• New performance reports created and
disseminated to units
• Units with Performance Boards
implemented
• Refined patient flow and discharge
process indicators and targets identified
by July 2016
• New performance reports created and
disseminated to units by August 2016
• Performance Boards implemented
and updated according to a standard
process on Orthopaedic and Trauma
Neurosurgery Units by May 2016
In order to provide the units with more
insightful, timely feedback on the tests of
change, Performance Boards will be
implemented across all the units involved in a
2016/17 QIP project.

Objective
Measure/Indicator Target justification This target is an internal benchmark. We have
based this on the improvement our previous
change ideas have led to in other clinical areas. A
10% improvement is expected based on this
year's work.
Unit / Population Target 7.19
Source / Period Current performance 8.00
Planned improvement
initiatives (Change Ideas)Methods Process measures Goal for change ideas Comments
1)Implement post fall debrief
tool and process on Trauma
Neurosurgery Unit (9CC)
a. Assemble improvement working group
b. Agree on a standard process/ timelines for
use of Standard Review Template following a
fall with harm
c. Devise evaluation plan to review efficacy of
template
• Determine baseline completion
rate for Standard Review process
• Set target for completion of
Standard Review process
• Baseline completion rate of
Standard Review process identified
by November 2016 • Target for
Standard Review completion, set by
December 2016
The 2016/17 Falls improvement work will focus
on Trauma Neurosurgery Unit (9CC) and General
Internal Medicine Unit (14CC) as two units with
the highest in-patient falls rates. The goal is to
refine the process for using a Standard Review
Tool on the pilot units before spreading it to the
rest of the hospital.
2)Improve identification of
patients at risk for falling
a. Ensure falls risk assessment is completed
upon admission for all patients
• % of patients screened within
24hrs of admission to all inpatient
units
• 95% of patients screened within
24hrs of admission to all inpatient
units
3)Implement strategies to
reduce falls for at risk
patients
a. Implement intentional hourly overnight
rounding on Trauma Neurosurgery Unit (9CC)
b. Implement individualized care plans for
patients screened at risk for falls on Trauma
Neurosurgery Unit (9CC) & General Internal
Medicine Unit (14CC)
c. Explore technology options (e.g. lowered
beds, bed alarms) for patients screened at risk
for falls
• Number of falls per 1000 patient
days
• Number of falls per 1000 patient
days for patient who have been
screened as at risk for falls
• Completion of care plans for
patients identified at risk for falls
on Trauma Neurosurgery Unit
(9CC) & General Internal Medicine
Unit (14CC)
• Reduce falls by 10% on Trauma
Neurosurgery Unit (9CC) by March
2017
• Reduce falls by 10% on General
Internal Medicine Unit (14CC) by
March 2017
• 75% of patients identified at risk,
have a completed care plan for
Trauma Neurosurgery Unit (9CC) &
General Internal Medicine Unit
(14CC), by March 2017
After successfully testing the practice of
intentional rounding for General Internal
Medicine Unit (14CC) over the past year, the
initiative will be extended to Trauma
Neurosurgery Unit (9CC) to examine if similar
results can be achieved.
4)Provide key performance
data to General Internal
Medicine (14CC) and Trauma
Neurosurgery (9CC) Units
a. Design performance board template
b. Implement Performance Boards on Trauma
Neurosurgery Unit (9CC) & General Internal
Medicine Unit (14CC)
c. Design standardized process for updating
the performance board
• Units with Performance Boards
implemented
• % of staff who agree, or strongly
agree that the performance board
supports improved
communication of performance
data
• Performance Boards implemented
and updated according to a standard
process on Trauma Neurosurgery
Unit (9CC) & General Internal
Medicine Unit (14CC) by May 2016
• 75% of staff who agree, or strongly
agree that the performance board
supports improved communication
of performance data, by January
2017
In order to provide the units with more insightful,
timely feedback on the tests of change,
Performance Boards will be implemented across
all the units involved in a 2016/17 QIP project.
FallsAvoid patient falls
Falls rate: Number of falls in General Internal Medicine and Trauma
Neurosurgery per 1,000 patient days in General Internal Medicine and Trauma
Neurosurgery Units
% / General Internal Medicine and Trauma Neurosurgery inpatients
Hospital collected data / January - December 2015

Objective
Measure/Indicator Target justification Focused improvement efforts on the intensive
care units (ICUs) aim to shift the culture. This
is expected to provide some overall
improvement (5% for each ICU) this year, but
support creation of foundational change
culture for future improvements.
Unit / Population Target67.0%
Source / Period Current performance63.6%
Planned improvement
initiatives (Change Ideas)Methods Process measures Goal for change ideas Comments
1)Focused efforts in the
intensive care units (ICUs)
aimed at improving
appropriate glove use
a. Assemble improvement working group with
representation from four ICU's
b. Conduct current state analysis with focus on culture and
common reasons for hand hygiene moment 1 misses
c. Plan and test strategies for improving processes around
glove use and providing peer feedback
d. Conduct staff education and training to support culture
change
e. Monitor hand hygiene opportunities and compliance
data
• Development of multi-disciplinary
working group including: nursing,
health disciplines, management and
medical staff
• Moment 1 hand hygiene compliance
in the four ICUs
• Rate of moment 1 hand hygiene miss
related to glove use
• Working group assembled,
monthly meetings booked by April,
2016
• 5% point improvement in hand
hygiene compliance in each ICU by
March 2017
• 10% reduction in misses related to
glove use by March 2017
The goal is to create a forum for discussion about
changes made on each unit and their perceived and
real impacts on hand hygiene compliance. This
should support dissemination of key change ideas to
support a culture shift.
2)Implement a Peer Auditor
Program
a. Develop a program for formal training and certification
of front line staff and managers as "Hand Hygiene
Ambassadors"
b. Garner feedback from frontline and leadership staff
c. Embed best practice with a focus on proficiency using
the HandyAudit tool and providing feedback to peers/staff
• Peer auditing curriculum developed
• # of units with one front-line staff
certified as a peer auditor
• # of peer auditors completing at least
one audit per month
• Curriculum developed by April
2016
• 80% of units have at least one
certified peer auditor by December
2016
• 75% of certified auditors perform
at least one audit per month by
March 2017
Following the positive reception of the On-the-spot
feedback trial, the peer auditing program aims to
provide front line staff with information regarding
when, where, how and why they are missing hand
hygiene. It will also encourage front line
participation in hand hygiene improvements efforts,
which could positively influence culture change.
3)Explore opportunities to trial
an electronic solution for real-
time feedback
a. Assess and compare available electronic solutions for
real-time feedback
b. Select and implement an electronic solution to provide
real-time hand hygiene compliance data
• Develop pilot implementation plan
to support introduction of real-time
feedback
• Develop plan to evaluate pilot of real-
time feedback solution
• Pilot of real-time feedback
solution implemented by October
2016
• Complete evaluation of real-time
feedback solution by March 2017
This solution aims to provide information to units in
real-time as to their current rate of hand hygiene.
This is valuable information that can be actioned
immediately should a reduction in compliance be
identified.4)Provide key information to
units regarding their Hand
Hygiene performance for
moment 1
a. Meet with inpatient units to review data, set targets and
action plans for 2016/17
b. Disseminate monthly performance reports reflecting
unit specific targets, challenges/barriers and common
misses to units
c. Collect and share hand hygiene misses information for
intensive care units as part of monthly reporting
d. Performance Boards implemented with a standard
process to update, on four ICUs
• # of units with moment 1 compliance
target selected
• # of units receiving monthly
compliance reports
• # ICU's receiving moment 1 misses
data
•# of units with Performance Boards
implemented
• 100% of inpatients units with
moment 1 compliance target
selected by April 2016
• 100% of units receiving monthly
reports by April 2016
• 100% of ICUs receiving monthly
details regarding moment 1 misses
by April 2016
• Four ICUs with Performance
Boards implemented and updated
according to a standard process by
May 2016
In order to provide the units with more insightful,
timely feedback on the tests of change, Performance
Boards will be implemented across all the units
involved in a 2016/17 QIP project.
Hand HygieneReduce hospital acquired infection rates
Number of times that hand hygiene was performed before initial patient contact
during the reporting period, divided by the number of observed hand hygiene
opportunities before initial patient contact per reporting period, multiplied by 100.
% / Health providers in the entire facility
Publicly Reported, MOH / Jan 2015 - Dec 2015

Objective
Measure/Indicator Target justification The average BPMH completion for the last 4
quarters has been 72.7%. The focus this year
is not to actively improve performance but
to maintain the current rate.
Unit / Population Target 73.0%
Source / Period Current performance 73.0%
Planned improvement
initiatives (Change Ideas)Methods Process measures Goal for change ideas Comments
1)Build an electronic
Medication Reconciliation
(eMedRec) solution
a. Assemble working group to inform
electronic medication reconciliation tool
b. Identify current state workflow and data
requirements to support implementation of
electronic medication reconciliation tool
c. Design and test electronic medication
reconciliation tool with frontline users
d. Modify based on user feedback
e. Implement tool and plan for spread
• Process maps of relevant
medication reconciliation
workflows
• # of identified staff for
participation in user testing
• New electronic medication
reconciliation tool created
• Process maps of relevant
medication reconciliation
workflows completed by
September 2016
• 100% of identified staff
participated in user testing
• New electronic medication
reconciliation tool implemented
by March 2017
This work will be led by the IT department
and Quality & Performance team will
provide support as needed for
implementation of the eMedRec solution.
2)Support ongoing
completion of BPMH on
admission (Inpatient Units)
a. Modify performance reports to:
i) reflect BPMH completion (vs. medication
reconciliation)
ii) categorize elective surgical patients who
had their BPMH completed in the pre-
admission facility (PAF)
b. Develop engagement and communication
strategy with the surgical areas with high
numbers of elective PAF patients
c. Introduce manual chart audits to assess for
quality of BPMH and medication
reconciliation
• % of admitted patients with
BPMH completed
• Baseline for quality assessment
collected through audit process
• Performance reports adjusted
to contain revised metrics
• 73% of admitted patients with
BPMH completed by March 2017
• Baseline quality assessments
for BPMH and medication
reconciliation completed for each
unit by December 2016
• Revised performance reports in
place by September 2016
The new methodology will categorize the
results based on the area that completed
the BPMH. For elective surgical patients, the
BPMH is completed in PAF and not on the
unit by the admitting service. The
performance reports and rates for each
service will now reflect this differentiation
and will be a more accurate reflection of the
BPMH and medication reconciliation
processes that occur on surgical services.
3)Support Medication
Reconciliation process on
Mental Health Unit
a. Continue to monitor monthly BPMH and
medication reconciliation completion rates on
Mental Health
b. Disseminate monthly performance rates to
the Mental Health Quality Committee
• % of admitted patients with
BPMH completed
• 80% of patients admitted to
Mental Health with BPMH
completed achieved by March
2017
The Quality & Performance team will
continue to maintain and support the
improvement efforts made by the Mental
Health program with BPMH completion and
medication reconciliation processes for
admitted patients.
Medication ReconciliationMaintain the current rate of best possible medication history completion on admission
Best possible medication history(BPMH) completion: The total number of
patients with a best possible medication history completed as a proportion of
patients admitted (excluding Labour & Delivery and NICU)
% / All inpatients (excluding L&D and NICU)Salumatics / October - December 2015
Objective
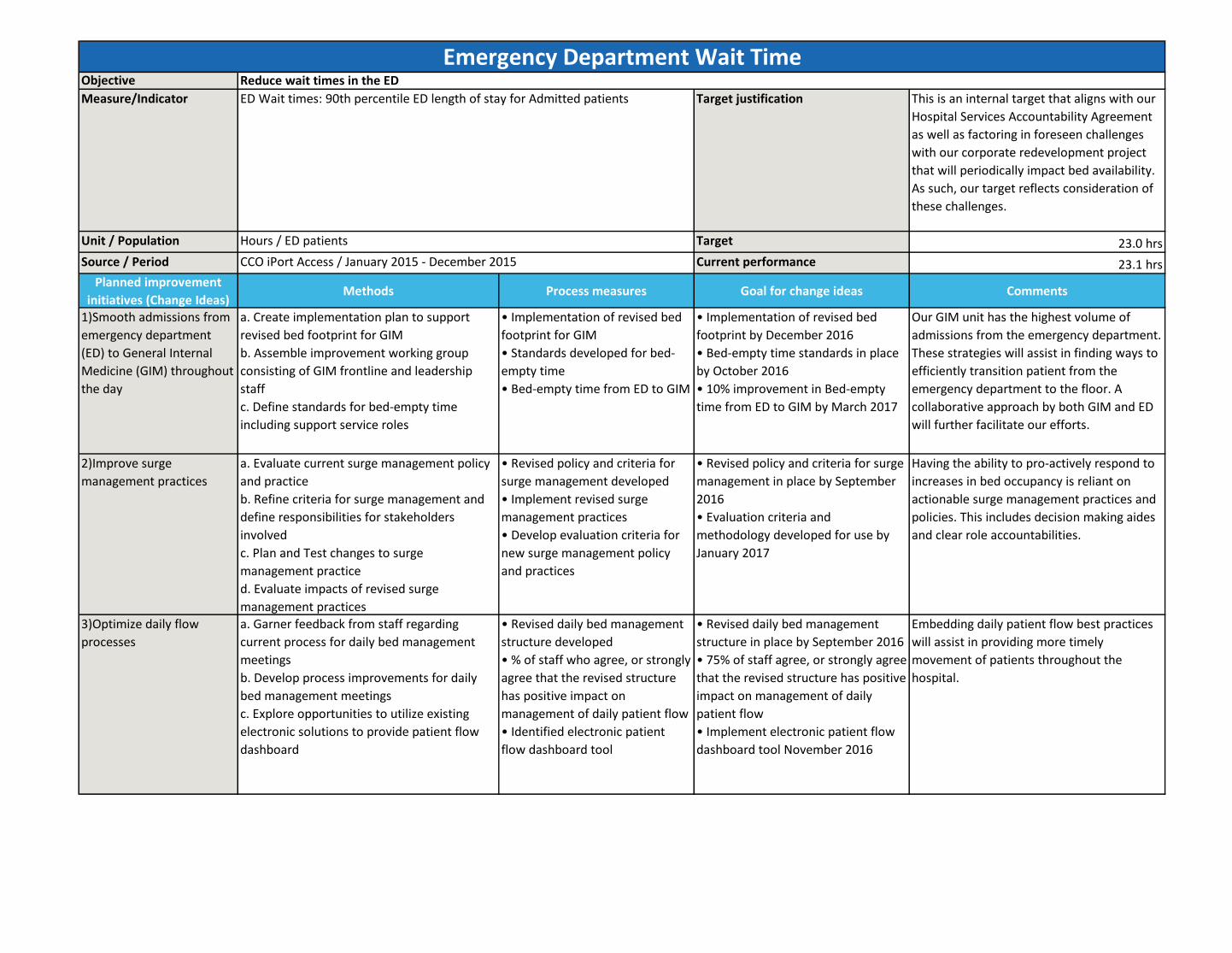
Measure/Indicator Target justification This is an internal target that aligns with our
Hospital Services Accountability Agreement
as well as factoring in foreseen challenges
with our corporate redevelopment project
that will periodically impact bed availability.
As such, our target reflects consideration of
these challenges.
Unit / Population Target 23.0 hrs
Source / Period Current performance 23.1 hrs
Planned improvement
initiatives (Change Ideas)Methods Process measures Goal for change ideas Comments
1)Smooth admissions from
emergency department
(ED) to General Internal
Medicine (GIM) throughout
the day
a. Create implementation plan to support
revised bed footprint for GIM
b. Assemble improvement working group
consisting of GIM frontline and leadership
staff
c. Define standards for bed-empty time
including support service roles
• Implementation of revised bed
footprint for GIM
• Standards developed for bed-
empty time
• Bed-empty time from ED to GIM
• Implementation of revised bed
footprint by December 2016
• Bed-empty time standards in place
by October 2016
• 10% improvement in Bed-empty
time from ED to GIM by March 2017
Our GIM unit has the highest volume of
admissions from the emergency department.
These strategies will assist in finding ways to
efficiently transition patient from the
emergency department to the floor. A
collaborative approach by both GIM and ED
will further facilitate our efforts.
2)Improve surge
management practices
a. Evaluate current surge management policy
and practice
b. Refine criteria for surge management and
define responsibilities for stakeholders
involved
c. Plan and Test changes to surge
management practice
d. Evaluate impacts of revised surge
management practices
• Revised policy and criteria for
surge management developed
• Implement revised surge
management practices
• Develop evaluation criteria for
new surge management policy
and practices
• Revised policy and criteria for surge
management in place by September
2016
• Evaluation criteria and
methodology developed for use by
January 2017
Having the ability to pro-actively respond to
increases in bed occupancy is reliant on
actionable surge management practices and
policies. This includes decision making aides
and clear role accountabilities.
3)Optimize daily flow
processes
a. Garner feedback from staff regarding
current process for daily bed management
meetings
b. Develop process improvements for daily
bed management meetings
c. Explore opportunities to utilize existing
electronic solutions to provide patient flow
dashboard
• Revised daily bed management
structure developed
• % of staff who agree, or strongly
agree that the revised structure
has positive impact on
management of daily patient flow
• Identified electronic patient
flow dashboard tool
• Revised daily bed management
structure in place by September 2016
• 75% of staff agree, or strongly agree
that the revised structure has positive
impact on management of daily
patient flow
• Implement electronic patient flow
dashboard tool November 2016
Embedding daily patient flow best practices
will assist in providing more timely
movement of patients throughout the
hospital.
Emergency Department Wait TimeReduce wait times in the ED
ED Wait times: 90th percentile ED length of stay for Admitted patients
Hours / ED patients
CCO iPort Access / January 2015 - December 2015

4)Refine existing daily
management practices
related to Alternate Level
of Care (ALC) on General
Internal Medicine (GIM)
a. Develop process for regular review of ALC
patients
b. Develop method to promote early
engagement of patients and families
c. Design and test ALC escalation algorithm
• Regular review process for ALC
developed
• % of ALC days compared to
patient care days on GIM
• ALC escalation algorithm
created and tested
• Regular review process for ALC in
place by August 2016
• 10% improvement in ALC days
compared to patient care days on
GIM
• ALC escalation algorithm created
and tested by October 2016
These strategies are focused on reducing the
highest proportion of ALC patients within the
organization.


















