Re-visioning the Delivery of Health Care Services to Uninsured Patients in Harris County Final...
118
Re-visioning the Delivery of Health Care Services to Uninsured Patients in Harris County Final Report Prepared for Save Our ERs July 20, 2004
-
Upload
halle-morcom -
Category
Documents
-
view
218 -
download
2
Transcript of Re-visioning the Delivery of Health Care Services to Uninsured Patients in Harris County Final...

Re-visioning the Delivery of Health Care Services to Uninsured Patients in Harris County
Final Report
Prepared for Save Our ERs
July 20, 2004

2
Table of Contents
Introduction Study Approach Drivers of Inappropriate Harris County ED Use
Key Findings Conclusions
Models of Care in Other Communities Components of a Care Re-visioning Framework Strategic Options for Harris County Study Conclusion and Recommendation

3
Introduction
In recent years, Harris Counties emergency care system has become increasingly overburdened by growing emergency department (ED) volume, particularly among uninsured non-emergent patients to whom ED’s are substitutes for more appropriate, yet frequently unavailable, community-based primary care.
Since 2001, conditions have worsened to the point that a study commissioned by the “Save our ER’s” coalition (the Coalition) concluded that the already overburdened emergency system is likely to continue to decay to the point of collapse without corrective action in the near term.1
This conclusion has helped create support among Harris Counties health care and business communities that a substantive restructuring of health care services is needed to reduce inappropriate ED use and fragmentation of care.
1. Houston Trauma Economic Assessment and System Survey, Bishop+ Associates, prepared for Save our ERs, 2002.

4
Introduction (cont.)
The Lewin Group, Inc. (Lewin) was commissioned by the Coalition to assist them in creating a framework for re-visioning the organization and delivery of health care services in Harris County by developing and examining three conceptually distinct and credible options for reconfiguring care to safety-net populations in Harris County.
Each option is arrayed by the degree of system re-organization and resources required to undertake. Expanding appropriate ambulatory care capacity. Improving coordination of care. Exploring options for restructuring city and county
public health functions. Building effective governance.

5
Study Approach
Key study questions and issues are complex, requiring input from many data sources and informants.
Lewin’s methodology was multi-tiered. Key elements included:
Collecting and analyzing survey data from Harris County providers and secondary quantitative data sources.
Conducting 20 on-site key informant interviews.
Conducting over 40 telephone interviews. Conducting an environmental scan of promising
practices in five other communities that have
reorganized care for safety net populations. Interacting with key Harris Co. and other state
stakeholders on important study issues. Findings were synthesized to develop three
credible options for reducing inappropriate ED use.
Qualitative
Quantitative
Observational

6
Study Approach (cont.)
Our approach to support development of three system reconfiguration options is organized around an assessment of several key study questions, including: What are the magnitude and drivers of ED overcrowding in Harris County
and what are the implications of continuing the status quo? What approaches for reducing in-appropriate ED use, building capacity and
better coordinating care have been successfully implemented in other communities? What are the potential benefits and challenges of these models for Harris County?
What are the objectives, major components and expected outcomes of three alternative options for reducing inappropriate ED use and improving access to care for the uninsured in Harris County?
The remainder of this study presents: Our findings regarding the questions outlined above; and The key features, benefits and challenges of three distinct and
progressively more comprehensive options to reduce in-appropriate ED use and improve access to care for safety-net populations in Harris County.

Magnitude and Drivers of Inappropriate ED Use in Harris County

8
Magnitude of ED Use in Harris County
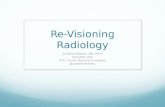
If current trends continue, Harris County ED use is projected to grow 38% between 2002 and 2015, after increasing 48% between 1991 and 2002.
Trends in Total Harris County ED Visits 1991-2015
Sources: AHA and the Draft HCHD Strategic Plan
1,742,000
1,261,317
853,968
-
200,000
400,000
600,000
800,000
1,000,000
1,200,000
1,400,000
1,600,000
1,800,000
2,000,000
FY 1991 FY 2002 FY 2015 (Projected)
To
tal V
isit
s

9
Magnitude of ED Use in Harris County:ED Use Is Concentrated Among Houston Safety Net Hospitals
Source: Begley, Charles, et al. Houston Safety Net Hospitals Emergency Department Use Study: January 1, 2002 through December 31, 2002 Final Report November 18, 2003.

10
Magnitude of ED Use in Harris County: Age Distribution of Harris County ED Users
Overall, most Harris County ED users are adults somewhat older than the general population.
Sources: Lewin Survey of Harris County Providers, 2000 Census data
n=17 hospitals
65+ Years26%
19-64 Years47%
0-18 Years27%
65+ Years7%
19-64 Years64%
0-18 Years29%
Overall Harris Co. Population

11
Magnitude of ED Use in Harris County: Income and Status of Harris County Hospital District ED Users
The income of most HCHD ED users is above 250% of poverty and most are US citizens.
Other1%
Undocumented Immigrants
16%
Documented Immigrants
9%
U.S. Citizens74%
201%-250% of FPL1%
101%-200% of FPL9%
250%+ of FPL55%
Other21%
0%-100% of FPL14%
Source: Lewin Survey of Harris County Providers
n=2 hospitals

12
Magnitude of ED Use in Harris County: Payer Mix of Harris County ED Users
CHIP2%
OTHER15%
SELF-PAY 24%
MEDICARE 13%
MEDICAID 20%
COMMERCIAL26%
MEDICARE 7%
MEDICAID 14%
COMMERCIAL11%
SELF-PAY 65%
OTHER3%
CHIP0%
Other Hospitals Reporting ED Data. (n=15)
While HCHD’s share of county-wide ED visits is only 14%, two-thirds are uninsured. Others have a more balanced payer mix.
Source: Lewin 2003 Survey of Harris County Providers
HCHD (n=2)

13
Magnitude of Inappropriate ED Use in Harris County
Over half of all ED visits are inappropriate.
By 2015, if current trends continue and no action is taken: Inappropriate ED use will
likely grow 38%, to about 950,000 visits.
Medicaid and the uninsured will comprise half of all inappropriate use.
Sources:1. Total County-Wide ED Visits from the AHA 2002 Annual Hospital Survey2. Percent of Inappropriate ED Visits from the "Houston Safety Net Hospitals Emergency Department Use Study" Final Report 3. Uninsured/Medicaid share of Inappropriate ED Visits from 17 hospitals responding to the Save Our ER's data request, representing
68% of county-wide ED use4. Source for FY 2015 estimated ED visits is the HCHD strategic plan.
Estimate of County-Wide Inappropriate Uninsured and Medicaid Emergency
Department Visits, FY 2002 Compared to FY 2015 Estimate Assuming No
System Change
FY 2002FY 2015
(Projected)
Total County-Wide ED Visits1 1,261,317 1,742,000
Percent of Inappropriate ED Visits 54.5% 54.50%
Estimated Number of Inappropriate ED Visits 687,418 949,390
Uninsured and Medicaid Share of Inappropriate ED Visits 51.70% 51.70%
Uninsured/Medicaid Inappropriate ED Visits 355,395 490,835

14
Drivers of Inappropriate ED Use in Harris County
Drivers of growth in Harris County inappropriate ED use include the downstream impacts of: Projected population growth Employment and healthcare coverage trends Lack of effective physician capacity Inadequate ambulatory care capacity Gaps in coordination of non-emergent care Cultural predisposition towards use of EDs

15
Drivers of Inappropriate ED Use: Projected Population Growth in Harris County
Source: 2000 U.S. Census, ESRI/CACI Demographics
Near-term growth will be concentrated among Hispanic and Asian populations.
Projected CMSA Population Growth Trends in Harris County, 2000-20015
2.5
3
3.5
4
4.5
2000Census
2003 2006 2008 2015
Po
pu
lati
on
(m
illio
ns)
Projected CMSA Population Growth Trends in Harris County, by Race and Ethnicity
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
1997 2000 2003 2006
Ch
an
ge
in P
op
ula
tio
n M
ix
White
Black
Hispanic
Asian/Pacific Is.
Harris County’s population is expected to grow 26% between 2000 and 2015.

16
Drivers of Inappropriate ED Use: Employer Health Care Coverage Trends
Between 1990 and 2000, Harris County enjoyed employment growth averaging 2.1 percent annually.2
The Houston-Galveston Area Council projects similar employment gains through 2025.
Much of the future growth is expected to be among small businesses, many of whom historically have provided limited or no health care coverage.
These trends threaten to increase the number of uninsured and place additional pressure on Harris Counties already strained emergency care system.
2. Houston-Galveston Area Council 2025 Regional Growth Forecast, May, 2003.

17
Drivers of Inappropriate ED Use:Lack Of Effective Primary Care Physician Capacity
Harris County has enough primary care physicians to meet population need.
However, inadequate reimbursement is a serious barrier to care for the uninsured and many Medicaid recipients.
Source: TX State Board of Medical Examiners, ESRI/CACI DemographicsNote: The shorter bars represent more physicians per person.
- 1,000 2,000 3,000
Persons/Primary Care Physicians
2001
2003
Ratio of Persons/Primary Care Physicans in Harris and Surrounding Counties
Ft. Bend Co.
Montgomery Co.
Harris Co.

18
Source: HCHD “Service Delivery Throughout Harris County” Presentation prepared by Gateway to Care 2003.
Inadequate Ambulatory Care Capacity: Current HC Clinic Locations Are Appropriate, But More Capacity is Needed
Harris County clinics appear well sited to meet the needs of safety-net populations.
But more capacity is needed to meet demand and care is fragmented.

19
Inadequate Ambulatory Care Capacity: Primary Care Demand Exceeds Supply
Available capacity addresses less than half of primary care demand among Harris County’s low income uninsured.
Therefore, there are no alternative access points to redirect inappropriate ED use.
Total Demand = 1.45 million visits
Total Estimated Capacity,
53%
Estimated Unmet Need, 47%
0
200000
400000
600000
800000
1000000
1200000
1400000
1600000

20
Inadequate Ambulatory Care Capacity: Demand For Primary Care By Low Income Uninsured Is High
A current estimate of primary care demand by uninsured Harris County residents under 200% poverty is over 1.4 million visits annually.
Estimated Number of Uninsured
830,000
Number of Uninsured Under 200% Poverty1
413,423
Average Primary Care Visits per Year Nationally
3.5
Estimated Primary Care Demand by Uninsured Under 200% Poverty
1,446,981 visits
Note: Uninsured under 200% FPL defined as Safety Net populations per AHRQ.
Sources: HCHD Strategic Plan, AHRQ

21
Inadequate Ambulatory Care Capacity: Primary Care Demand Exceeds Capacity
Available data suggests that demand among the uninsured for primary care exceeds current capacity .Clinic Type Number of
SitesTotal Primary
Care VisitsEstimated
Uninsured Visits
HCHD: Current and Approved
11 882,713 496,085
City/County DOH 12 184,460 99,846
Major non-profit 7+TCPA sites 1,015,983 84,682
School-Based 13 50,000 28,100
Teen 6 16,614 9,337
FQHC 2 19,513 10,942
Other (planned parenthood, mobile vans, etc.)
27 66,169 35,489
Total Estimated Capacity
2,235,452 764,481
Estimated Need 1,446,981
Estimated Unmet Need 682,500Sources: HCHD Office of Strategic Planning, Gateway to Care Health Home survey, Lewin Survey of Harris County providers, Dr. Chuck Begley and Lewin Group analysis

22
Inadequate Ambulatory Care Capacity: Demand for Behavioral Health is Also High
Demand for behavioral health services also exceeds available capacity in Harris County.
According to the Harris County Mental Health Needs Council, an estimated 120-130,000 people in Harris County have severe mental illness. About 60% are reportedly uninsured. In 2003, the public sector, including HCHD (7,305) and
MHMRA (186,567) together reported seeing about 194,000 visits.
Private sector capacity in Harris County was unavailable for this study.

23
Conclusions Regarding Inappropriate ED Use in Harris County
Analysis of available data led to a number of conclusions regarding inappropriate ED use in Harris County. These include:
Inappropriate ED use is significant and, absent effective intervention, will continue to grow due in part to factors outside the health sector’s control.
Continuing the status quo is risky, as future trends are likely to exacerbate stresses on the local health care delivery system and further compromise the ability of many Harris County residents to access needed care on a timely basis.
Strategies focused solely on re-directing inappropriate ED use are likely to fail due to lack of adequate alternative capacity.
Any adopted strategy must seek to better balance the local health care system through building new capacity and improving coordination of care.

Environmental Scan of Models of Care Adopted in Other Communities

25
Approaches Adopted In Other Communities May Be Useful
Lewin conducted an environmental scan to identify promising practices and administrative and governance models successfully tested elsewhere to reduce inappropriate ED use and system fragmentation.
Following are examples of models to: Build effective organization and governance. Expand healthcare coverage for small businesses. Increase physician capacity. Expand ambulatory care capacity. Improve coordination of ambulatory care. Consolidate public health services.

Organization and Governance

27

28
Denver Health - History
Prior to the creation of Denver Health, the City of Denver operated the Health and Hospital Department. The Department was in charge of all public health services, the city public hospital and clinics, as well as the Rocky Mountain Poison Control Center. The manager of the Department and all of the members of the board were appointed by the Mayor. The Department’s board acted mainly in an advisory capacity.
In the 1990s, Denver was subject to aggressive movement by managed care into the market. Many of the new HMOs began cherry-picking patients from the Department (e.g., patients with private insurance), threatening the department’s financial base. To combat this problem, the Department tried different strategies such as creating an HMO for city employees, among other activities.
In the mid-1990s, Denver’s mayor appointed a blue-ribbon task force to look at the organization of the department and develop recommendations for change and looked at several different options. However, the Mayor stipulated that the department could not become a private, free-standing non-profit entity.
The final recommendation was to develop an authority structure. While the authority remains public (a subdivision of the State of Colorado), it is able to operate independently as its own authority. In order to transition the Department into an authority, it was necessary to obtain authorization from the Colorado State Legislature.

29
Denver Health: Governance
Denver Health has a contractual relationship with the City of Denver to provide health care and public health services. When Denver Health became an authority, the contract included three agreements:
Transfer Agreement: All assets were transferred from the City to Denver Health.
Operating Agreement: Denver Health will serve the City of Denver in perpetuity. This insures that the city will not bid out for services.
Personnel Agreement: Employees from DHH are allowed to remain city employees or become employees of Denver Health. In the former case, they are leased to Denver Health.

30
Denver Health: Governance – Board Structure
Denver Health is governed by a nine-member board, appointed by the Mayor and confirmed by the City Council for a five-year term. Individual board members terms may be renewed for one additional term.
There are no stipulations regarding who may serve on the board of directors. When seats on the board are vacant, the CEO and remaining board members provide the Mayor with a list of possible replacements. Denver Health’s CEO serves as an invited member of the Mayor’s cabinet.
The City of Denver contracts with Denver Health for services. As a result, the Mayor and City Council have no direct authority over Denver Health beyond board appointments. The Board has complete authority over Denver Health.
Denver Health operates eight FQHCs. Each FQHC in the system has its own board to remain compliant with Section 330 requirements. Two members of the Denver Health Board are members of each FQHC board.

31
Denver Health: Organization and Structure
Denver Health is directed by a Chief Executive Officer, who also acts as Medical Director for the hospital.
Denver Health is divided into a number of Divisions, including: Hospital Division: The division runs the city hospital, as well as the city
911 system. Public Health Division: The division provides the majority of public
health services in the city, including infectious disease clinic, communicable disease control, TB clinic, STD clinic, immunization clinic, public health laboratories, and vital records.
Community Health Center Division: The division operates Denver Health’s 8 FQHCs and 13 school-based clinics.
General Council and Risk Management Division Human Resources Finance Quality Review and Office of the Assistant Medical Director Director of Managed Care Rocky Mountain Poison Control Center

32
Denver Health – Organizational Chart
Denver Health Board of Directors(Nine Members)
CEO & Medical Director
Chief Operating Officer Director of Public HealthDirector of
Community Health CentersDirector - Rocky Mountain
Poison Control CenterGeneral Counsel
Risk ManagementChief Financial Officer
• Hospital• 911
Public Health
InfectiousDisease
PH Labs
Vital Records
TB Clinic
8 FQHCs
11 School-basedClinics
Director of Managed Care
Director of Quality Reviewand Associate Medical Director
Director of Human Resources

33
Marion County, IN – Health and Hospital Corporation (HHC): Overview
Program Description: Beginning in 1954, Marion County, Indiana consolidated public health and health care functions into a single authority, the Health and Hospital Corporation (HHC).
Program Purpose: HHC provides medical health care, environmental health, and population health services to Marion County and the City of Indianapolis, Indiana.
Key Features: HHC operates both the Wishard Memorial Hospital System and the
County Health Department Physicians who work for HHC clinics all come from the Indiana
University Medical Group Primary Care (IUMGPC) HHC established a program called “Advantage,” a managed care-like
program for low-income, uninsured residents of Marion County, Indiana. The program is jointly owned by Wishard Hospital and Indiana University School of Medicine.

34
Marion County, IN – Health and Hospital Corporation (HHC): Governance
HHC is governed by a seven-member Board of Trustees, three appointed by the Mayor, two by the City-County Council, and two by the Board of County Commissioners. Historically, the board has included representation from the community, as well as legal and financial expertise.
HHC has few limitations on its own authority. While the Mayor may make requests, the board is free to turn them down. HHC’s annual budget must be approved by the county council. However, modifications made by the council can be appealed to the state.
As a consolidated taxing authority, HHC must work with the State Board of Accounts, which must approve all levies made by HHC. The State Board of Accounts must verify that levies do not exceed the state-mandated annual limits.
HHC also works closely with the State Board of Health and State Medicaid agency.

35
HHC: Organization and Structure
HHC operations are overseen by an Executive Division, including the President/Executive Director. The Executive Division is able to move assets, leverage funding from various sources, and coordinate activities to maximize efficiency.
The Marion County Health Department is divided into two bureaus:
Bureau of Environmental Health: Services include Food Safety, Housing and Neighborhood Health, Childhood Lead Poisoning Prevention, Indoor Air Quality, and Occupational Health.
Bureau of Population Health: Services include Communicable Disease Control, Chronic Disease Control, Dental Health, Immunizations, Maternal and Child Health, Nutrition Services, Public Health Laboratory Services, and Vital Records.

36
HHC: Organization and Structure
HHC’s Hospital Division operates Wishard Memorial Hospital and its health services. In the late 1990s, authority for all seven clinics within HHC was given over to the Hospital Division (previously the Hospital Division was in charge of only 2 of the clinics). This has brought about increased reimbursement and better integration with the Wishard Memorial Hospital for specialty care.
The seven clinics affiliated with HHC are currently under review for FQHC look-alike status. This will be a co-applicant arrangement between HHC and a single community board (51% community/49% other – of which 2 seats are for HHC). HHC will maintain budgetary control, while other issues will be handled jointly. This will likely provide greater oversight of the clinics and the benefits of look-alike status. HRSA is expected to approve this arrangement.
The Indiana University Medical Group – Primary Care (IUMGPC) provides staff for all of the clinics directly under HHC (i.e., Wishard clinics). IUMGPC also selects the medical director for the clinics.

37
Health and Hospital Corporation – Marion County
Health and Hospital Corporation
Hospital Division Health Department
Executive Division
Bureau ofEnvironmental Health
Bureau ofPopulation Health
Wishard MemorialHospital
Clinics

38
Cook County, Illinois - Bureau of Health Services
Program Description: In 1991, Cook County, Illinois formerly established the Bureau of Health Services (CCBHS) to provide health, hospital, public health, and health education services to throughout Chicago and its suburbs.
Program Purpose: CCBHS was designed to create a better-coordinated and more integrated system of health care delivery within Cook County.
Key Features: CCBHS includes a referral network that allows integration of
specialty care, in both affiliate and non-affiliate clinic, with the County Hospital.
CCBHS operates over 30 community-based clinics. Provides care to specific patient populations, including HIV/AIDS,
chronic care, and detainees in the correction system.

39
Cook County, IllinoisBureau of Health Services - Governance
Cook County Bureau of Health Services (CCBHS) is an executive agency of Cook County, under the President of the County. The Cook County Board of Commissioners acts as the governing board for the Bureau’s operating entities.
CCBHS is run by a the Bureau Chief. The chief operating officer of each operating division reports to the Bureau Chief. CCBHS includes seven separate divisions.
The Bureau Chief is appointed by the President of the County with the consent of the Board of Commissioners.

40
Cook County, IllinoisBureau of Health Services - Structure
CCBHS includes seven separate divisions:
Ambulatory & Community Health Network: The Network coordinates primary and specialty outpatient care in community, school-based and hospital outpatient settings.
Cermak Health Services: Cermak provides health services to roughly 10,000 detainees at the Cook County Department of Corrections and the Department of Community Supervision and Intervention
Department of Public Health (DPH): DPH provides public health services in all of Cook County, except for Chicago and four other cities/towns in the County.
Ruth H. Rohnstein CORE Center: The CORE Center provides outpatient care to those with HIV/AIDS and other infectious diseases.
John H. Stroger, Jr. Hospital: Cook County’s main hospital has 464 beds and a Level 1 Trauma Center.
Oak Forest Hospital: Oak Forest provides long-term, chronic disease, and rehabilitation services, and includes over 600 staffed beds.
Provident Hospital: Provident is a full-service hospital serving more than 50,000 patients annually.

41
Cook County, IllinoisBureau of Health Services - Org. Chart
Cook CountyBoard of Commissioners
Bureau ofHealth Services
Ambulatory and CommunityHealth Network
Cermak Health Services
Department ofPublic Health
Ruth H. Rohnstein CORE Center
John H. Stroger, Jr. Hospital Oak Forest Hospital
Provident Hospital

Models for Expanding Insurance Coverage

43
Health Access – Muskegon County, Michigan
Program Description: “Health Access,” a subsidized health care program for uninsured employees of small businesses and their dependents in Muskegon County, Michigan, established by the county with an initial grant from the Kellogg Foundation.
Program Purpose: To provide a basic health insurance-like product for low income workers who do not have access to health insurance, either on their own or through their employer.
Funding Source: Employers and employees each pay for 30 percent of product’s costs, while the community picks-up the rest utilizing DHS funds.
Key Features: Businesses that have not offered insurance for the past 12 months and have a median employee salary of no more than $11.50 are able to enroll in the program. Employees receive a basic benefits package and have their care managed by a primary care physician. The program only covers care given by providers located in Muskegon County and pays them on a fee-for-service basis. High-cost specialty care is covered by Medicaid by employing spend-down strategies.

44
Muskegon County, Michigan
Pros for Harris County The program could provide access to health care for many working
uninsured in Harris County. The product is not insurance, so reserve requirements do not take
effect.Cons for Harris County Because DSH funds are being maximized by Harris County, an
alternative source of funding would have to be found. Dedicated providers would have to be found to act as primary care
physicians for program beneficiaries. A current or new entity would have to take responsibility for managing
claims and administration.Recommendations SOER should consider this option if a dedicated funding source can be
found to subsidize the program. Business and provider buy-in is also critical for such a program.

45
Advantage – Marion County, Indiana
Program Description: “Advantage,” a managed care-like program for low-income, uninsured residents of Marion County, Indiana, established in 1997 by the Marion County Health and Hospitals Corporation and jointly owned by Wishard Hospital and Indiana University School of Medicine.
Program Purpose: To reduce inappropriate Emergency Department use and unnecessary hospital admissions, and to better track and monitor quality care.
Funding Source: Local taxes and redirected hospital federal disproportionate share funding.
Key Features: Uninsured residents are enrolled and assigned to a primary care provider who coordinates their care. The program includes an urgent visit center to complement Wishard’s Level I trauma center, a 24-hour call center that can redirect emergency calls to primary care providers and a focus on referring patients back from specialist to the primary care provider of record.

46
Advantage – Marion County, Indiana
History: When Advantage began, only clinics under the purview of HHC were utilized. Clinics outside the network were not integrated. As a result, a number of problems developed. The outside clinics wanted to offload their non-paying patients
to the HHC system. However, they could not make referrals to specialty care at Wishard Hospital. So, the clinic physicians would make a diagnosis and then refer their patients to the Wishard ED where they would be re-diagnosed and admitted for specialty care.
Outside clinics did not have access to the integrated data network of HHC. As a result, they could not maintain continuity of care for patients who were using both systems.

47
Advantage – Marion County, Indiana
History (cont’): As a result of these problems, HHC decided to expand the network for Advantage to include a number of outside clinics. As a result: the outside clinics have referral privileges to Wishard Hospital; the Advantage system can make sure that these clinics adhere
to protocols for referring specialty care (e.g., certain tests must be conducted before a referral can be made);
an electronic medical record can now be used for all Advantage patients throughout the entire system. This helps to maintain continuity of care. EDs also have access to this integrated data network; and
Advantage members, in some cases, may also access specialty care from hospitals outside of HHC through the outside clinics.

48
Advantage – Marion County, Indiana
Pros for Harris County Physicians are under a capitated arrangement, so they are
encouraged to have patients using the most appropriate care. This type of program utilizes the current health care system and
does not necessitate major functional changes.Cons for Harris County This type of a program requires total subsidization. The
population served does not qualify for other programs like Medicaid.
Recommendations Although the capitated arrangement with participating physicians
is attractive, SOER should be cautioned from replicating this model without first finding multiple sources of funding.

Increased Ambulatory Care Capacity and Coordination

50
Federal New Access Point Initiative
Program Description: The “New Access Point Initiative” was developed by the Bush Administration in August 2001 to expand current FQHCs and add new FQHCs around the country.
Program Purpose: To expand health coverage to the uninsured. Funding Source: Federal appropriations distributed by the
Bureau of Primary Health Care within the Health Resources and Services Administration (HRSA)
Key Features: The five-year program calls for $1.2 billion to fund 1,200 new or expanded FQHCs. Of the 1,200 sites, 570 will be expansions of current FQHCs. Of the 630 remaining sites, 420 will be expansions of existing health centers and 210 will be new start community health centers. New sites will receive a maximum grant of $650,000 per year and expansion sites will receive a maximum grant of $550,000.

51
Federal New Access Point Initiative
Pros for Harris County This program makes available funds for additional sites and
expansions of current sites. The Texas Legislature created an FQHC Incubator Program to facilitate
existing clinics in their attempt to obtain FQHC status. Obtaining FQHC “look-alike” status would still be beneficial in the
interim.Cons for Harris County The process for obtaining FQHC status is very competitive and a great
deal of effort can be expended without receiving approval. The governance requirements for FQHCs are strict, with 51 percent of
the board coming from the community.Recommendations FQHC expansion should be continued as part of a broader capacity
building strategy.

52
Chicago’s Access Community Health Network
Program Description: “Access Community Health Network,” a large FQHC system serving residents located on the South and West sides of Chicago.
Program Purpose: To provide underserved areas with high-quality health care in a clinic setting.
Funding Source: The program receives Section 330 funds for the clinics with FQHC status. The program also receives federal grant money for infant mortality, state grants for breast and cervical cancer, and foundation and individual philanthropic support. The most significant amount of funding comes from Medicaid, Medicaid HMO wrap-around, and Medicare.
Key Features: The Network operates 42 clinics under single corporate structure. Federal funds for FQHCs are passed through the Network to those clinics. The Network itself enjoys some of the benefits of the FQHC status, including medical malpractice coverage. The Network has relationships with a number of hospitals, allowing patients to be seen in a number of different places for specialty care.

53
Chicago’s Access Community Health Network
Pros for Harris County Having FQHCs and other clinics in an integrated network helps to
reduce administrative costs and provides economies of scale. The network structure allows funding and contracting to be leveraged
throughout the system. An integrated Network can more easily facilitate continual growth,
particularly with regard to adding additional FQHCs.Cons for Harris County An integrated Network approach requires substantial upfront
coordination and a willingness of various entities to work together. The board for such a Network would have to have diversity so as to
prevent overrepresentation by a single entity.Recommendations If SOER proceeds with efforts to bring additional FQHCs to Harris
County, this model should be considered as a method to coordinate the effort. However, buy-in among all participants is critical for it to work.

54
FQHC Look-Alike Initiative – Marion County, IN
Program Description: The Health and Hospital Corporation (HHC) of Marion County is currently seeking FQHC Look-alike status for each of its seven clinics.
Program Purpose: To obtain the benefits of FQHC look-alike status for clinics serving the HHC.
Key Features: The seven clinics affiliated with HHC are currently under
review for FQHC look-alike status. This will be a co-applicant arrangement between HHC and a single community board (51% community/49% other – of which 2 seats are for HHC). HHC will maintain budgetary control, while other issues will be handled jointly. This will likely provide greater oversight of the clinics and the benefits of look-alike status. HRSA is expected to approve this arrangement.

55
FQHC Look-Alike Initiative – Marion County, IN
Pros for Harris County FQHC Look-alike status is not competitive, yet still provides a number
of FQHC benefits, including enhanced revenue due to Prospective Payment System reimbursement, PHS Drug Pricing Discounts, access to DHHS outstationed eligibility workers, and “first dollar” Medicare reimbursement.
Cons for Harris County While the FQHC Look-alike status is not competitive, all of the Section
330 requirements must be met, including board requirements. HHC has a co-applicant arrangement with the FQHC Look-alike boards.
It may be difficult to isolate a single entity in Harris County to assume this responsibility.
Recommendations SOER may want consider finding CHCs that are near FCHC Look-alike
status to sponsor. Various entities could take on the responsibility of incubator.

56
Referral Network: Cook County, Illinois
Program Description: Since 1985, Cook County has maintained a referral system for non-affiliate clinics, allowing patients to receive specialty care through the County Hospital.
Program Purpose: To allow uninsured and indigent patients access to specialty care through referrals from primary care physicians.
Key Features: This network allows both clinics in Cook County’s Ambulatory &
Community Health Network (~30) and non-affiliated clinics (~60) to refer patients to Cook County Hospital for specialty care, as well as allowing Cook County’s ED the ability to re-direct patients to clinics for more appropriate care.
Clinics also have access to the hospitals labs and pharmacy (although pharmacy is now being scaled back to some degree).
Clinics in the network now use a Web-based referral system for their patients.
Primary Care Physicians must abide by referral rules detailed in the Web-based system. Approximately 10,000 patients per month are being referred through this system. The hospital uses the Web-based system as well to help patients locate clinics near their homes for primary care.

57
Referral Network: Cook County, Illinois
Pros for Harris County This system would allow clinics not affiliated with Ben Taub or LBJ
Hospitals to utilize a systematized method of referral. A Web-based system would provide efficiencies to the referral
process. Hospitals would have a means to find primary care homes for non-
emergent patients.Cons for Harris County While Cook County has one dominant health body, Harris County
has many. It may be difficult to coordinate among the different stakeholders in Harris County.
A Web-based system might require infrastructure improvements from already cash-strapped clinics.
Recommendations SOER should consider an integrated system for referrals. At the
same time, careful planning should occur to make insure that no one hospital system or clinic is overrun.

58
Project Access – Buncombe County, North Carolina
Program Description: “Project Access,” a volunteer physicians program for uninsured and indigent residents in Buncombe County, North Carolina, established in late 1995 in collaboration with the Buncombe County Medical Society.
Program Purpose: To match uninsured and indigent patients in need of specialty care with physicians willing to provide care for free
Funding Source: All services are donated by physicians and hospitals to which they are affiliated
Key Features: Physicians who participate in the program agree to see approximately 20 patients for free each year. Participating physicians are then put on a list available at local clinics and at the health department. Those who are in need of specialty care and do not have a means to pay for such care are referred to the appropriate and available doctor on the list. The physician is responsible for the needed care for that patient for three months, when the patient is re-evaluated to assess whether further specialty care is needed. The program currently has an average enrollment of 900-1,000 patients.

59
Issues to Consider Project Access – Buncombe County, North Carolina
Pros for Harris County The program could reduce the number of indigent patients who receive
specialty care from Ben Taub and LBJ Hospitals. Costs are limited to program administration and physician recruitment. Physicians are able to limit the number of patients they see under this
arrangement to prevent being overrun. Cons for Harris County This type of program involves significant buy-in from the physician
community, as well as hospitals for testing and labs. An administrative system would have to be established that could be
used in the many clinics and hospitals around the county.Recommendations SOER should consider this option in order to include private physicians
as part of the solution. To maintain continuity of care, physicians should be required to commit to at least one-year of service for each patient.

Health Services Consolidation

61
Health Services Consolidation – Marion County, IN
Program Description: Beginning in 1954, Marion County consolidated public health and health care functions into a single authority, the Health and Hospital Corporation (HHC)
Program Purpose: To improve coordination of care and gain operating efficiencies.
Funding Source: Local tax levies approved by the State Board of Accounts. Key Features:
HHC is a consolidated taxing authority. HHC’s Executive Division oversees the corporation, with the heads of the Hospital Division and Department of Health Division reporting to the Executive Director of HHC. HHC also acts as the board of health for the county.
HHC maintains a seven-member board (3 appointed by the Mayor, 2 appointed by the City-County Council, and 2 appointed by the Board of Commissioners).
Eight years ago, the hospital division assumed control over all seven clinics under the jurisdiction of HHC in order to maximize reimbursement from patients and other payers, and better integrate care with the Hospital.

62
Health Services Consolidation – Marion County, IN
Key Features (cont’): The Indiana University Medical Group – Primary Care (IUMGPC)
provides staff for all of the clinics directly under HHC (i.e., Wishard clinics). IUMGPC also selects the medical director for the clinics.
The medical director of Wishard Hospital (i.e., public hospital for Marion County) is a faculty member from Indiana University. However, the University’s contract with Wishard is up soon and changes are likely to occur, including finding a new medical director. The change is due to the current and other recent medical directors’ difficulties with hospital management.

63
Health Services Consolidation – Marion County, IN
Pros for Harris County Consolidating clinics and hospitals into an integrated delivery model would
allow for better patient management (e.g., specialty care) and data collection. This could help alleviate fragmentation in Harris County.
As a consolidated entity, public medical care and public health activities could be coordinated to maximize their benefit and eliminate duplicity.
Cons for Harris County HHC’s role as a consolidated taxing authority would be difficult to replicate
in Harris County due to the multiple jurisdictions involved. While HHC oversees one hospital system and one department of health,
consolidation in Harris County would include numerous entities in both medical care and public health.
Recommendations Harris County should examine the legal feasibility of any consolidation
efforts before proceeding. Harris County may want to consider a step approach, with consolidation happening in stages over time.

64
Summary Of Lessons Learned From Examining Other Communities
After examining other communities, several common success factors emerged that are relevant for Harris County as it considers options for strengthening service delivery and coordination of care. These include:
Strong leadership is essential for success. Consensus may be difficult to achieve but it is important to
keep stakeholders engaged in the process. It is important to anticipate and flexibly plan for potential
future policy, economic and other environmental developments.
Sound financial analysis and planning are critical to ensure the long term financial viability of alternative models and to make the “business case” for investment.
The need to establish transition planning, including leadership succession planning, as implementing meaningful change takes time.

Components of a Framework for Re-visioning Care in Harris County

66
Framework for Re-visioning Care
Lewin created a framework around which to develop, compare and assess three actionable strategic options for Harris County. The framework evolved from: Analysis of the magnitude and drivers of in-appropriate ED
use. Feedback from Harris County stakeholders. Approaches adopted by other communities.
The framework is grounded in a conclusion that the problem calls for a multi-faceted and well coordinated approach.
This chapter describes the framework’s components and summarizes stakeholder feedback regarding current status and future opportunities.

67
Options to Address the Problem in Harris County Feature Five Coordinated Components
Improve Coordination
of Care
Restructure Public
Health Functions
Assure Adequate Financing
Expand Ambulatory Care Capacity
Establish Effective
Governance

68
Expanding Ambulatory Care Capacity: Harris County Stakeholder Feedback
Most stakeholders believe new capacity is needed to relieve pressure on EDs, but approaches differ.
Many agree that a public/private solution includes a mix of: New specialty clinics. Expanded hours at HCHD and City and County public health
clinics. Development of new public and private FQHC and FQHC
look-alike capacity. Additional urgent care centers adjacent to private hospitals. More school-based health services. More physician capacity. Potential sources include
volunteers, medical schools, and National Health Service Corps.

69
Expanding Ambulatory Care Capacity (Cont.)
Progress is being made in many areas. Specialty Care: Two new HCHD clinics providing
106,000 annual visits received conceptual County approval.
Expanded Hours: HCHD clinics will expand hours in 2004, growing capacity by 160,000 visits annually.
FQHCs: HCA converted a clinic to an FQHC in 2003 and several other clinics are planning to apply in 2004.
Urgent Care Centers: Several private providers are exploring opening urgent care centers to redirect inappropriate ED use.
School-Based Care: Houston school district is working to expand the number of clinics.

70
Improving Coordination of Care: Stakeholder Feedback
Many Harris County stakeholders believe any growth in capacity must be accompanied by improved care coordination.
Components of a public-private solution cited include. Establish contractually-based patient referral guidelines a la the
Chicago model to reduce fragmentation. Hire additional full time community “Navigators”* to assist in
overcoming barriers to care. More effectively advertise and expand the number and hours of
telephone nurse triage services to help persons find alternatives to ED use.
Integrate patient medical records to follow patients across sites of care. Expand educational tools and outreach strategies to promote
appropriate use of health care services and improve access to insurance.
Develop a coordinated patient transportation strategy.
* Defined as individuals who can help direct care towards appropriate sites within the community.

71
Assuring Adequate Financing: Opportunities and Challenges
Funding will be needed to develop and operate new ambulatory care capacity.
Stakeholders noted opportunities, including: Support for change by the Mayor, Commissioners Court and
the business community. Conceptual county approval of funding for new ambulatory
care capacity called for by the HCHD strategic plan. Active efforts by coalitions such as Gateway to Care to plan
and coordinate FQHC expansion and other capacity building. Interest by private providers in new FQHCs and urgent care
centers to redirect inappropriate ED use. Foundation support. Efforts by The Houston Independent School District’s to
expand school-based health programs.

72
Assuring Adequate Financing: Opportunities and Challenges (cont.)
Challenges to overcome are significant, including: Limited potential for additional federal DSH funding
due to cutbacks and stricter oversight. Limited availability of federal funding for FQHC
expansion. HRSA received about 1,280 applications in FY 2002-2003, but only 418 were funded.
State cutbacks in Medicaid and CHIP eligibility. Little likelihood that the Texas legislature will
increase Medicaid outpatient and physician payment rates.
Passage of the Governor’s tax cap proposal would limit property tax revenue growth and county funding available for healthcare.

73
Restructuring Public Health Functions
Most Harris County stakeholders favor consolidation of City and County public health departments. Reasons cited include: Opportunities for improved integration of services. Opportunities for cost efficiencies by eliminating and
consolidating redundant services and functions. Opportunities to maximize use of underutilized
capacity. Opportunity to establish a centralized point of
accountability. Opportunity to provide a county-wide unified
response to public health emergencies.

74
Restructuring Public Health Functions
Those opposed cite: Concern that public health priorities and funding would
be diminished if merged with larger HCHD. Little real potential for cost efficiencies, as both
departments have independently achieved economies of scale.
Cost of standardizing information and other systems and potential for disrupting implementation of the HCHD IS strategic plan if merged with HCHD.
Cost of upgrading public health sites providing primary care services to JCAHO standards if merged with HCHD.
The strongest opposition centers around merging with HCHD.

Strategic Options for Harris County

76
We created a framework around which to develop and compare three actionable strategic options after assessing: The extent of inappropriate ED use and other
stresses on Harris County’s delivery system. Feedback from key Harris County and other
stakeholders. Models developed in other communities.
The framework for each option includes five key components.
Overview

77
Overview
Improve Coordination
of Care
Restructure Public
Health Functions
Assure Adequate Financing
Expand Ambulatory Care Capacity
Establish Effective
Governance
Each option features a different mix of five key components:

78
In developing three conceptually distinct strategic options, two categories emerged:
A minimalist or reactive option, which seeks to improve system efficiency while minimizing new funding commitments.
Two more proactive responses, which seek to expand health system capacity through multiple access points and improve system efficiency and coordination.
The following slide illustrates our framework for revisioning the delivery of health care services in Harris County.
Overview

79
CurrentSystemCurrentSystem
CurrentCapacity/
Coordination
HeightenedSystem
Efficiency
New Capacityand
Coordination
FullyRebalanced
System
1
2
3
Least Comprehensive
MostComprehensive
CoordinatedCommunity
Health System Option
CoordinatedCommunity
Health System Option
Strategic Realignment
Option
Strategic Realignment
Option
ReactiveOption
ReactiveOption
Ran
ge o
f C
on
fig
ura
tion
O
pti
on
s
Framework for RevisioningHealth Care in Harris County

80
The following describes key features and projected outcomes of three options for re-visioning organization and delivery of health care services in Harris County.
These options are arrayed by the magnitude of system change required.
Options are designed to be additive, with each more complex option building upon the components of less ambitious options.
This approach acknowledges variation in the scope of change required and provides stakeholders flexibility to move up or down the continuum of change.
Framework for RevisioningHealth Care in Harris County

81
CurrentSystemCurrentSystem
CurrentCapacity/
Coordination
HeightenedSystem
Efficiency
1
2
3
Least Comprehensive
MostComprehensive
ReactiveOption
ReactiveOption
Ran
ge o
f C
on
fig
ura
tion
O
pti
on
s
Strategic Options for Harris County:A Reactive Option

82
Under this option, Harris County would move incrementally and opportunistically toward its revisioning goals.
The focus of this “small fix” approach would center around maximizing the efficiency of the current system.
County providers would minimize new investment and maximize reimbursement through the selective conversion of existing community-based ambulatory care capacity to better reimbursed FQHCs and FQHC look-alikes and modest expansion of urgent care centers.
Reactive Reconfiguration Option:Objectives and Key Features

83
Major components of this “closed system” reactive option include: Several new urgent care centers built by private hospitals near
EDs to redirect nonemergent care and reduce financial losses. Opportunistically converting selected community clinics to
FQHCs or FQHC look-alikes to maximize reimbursement, but little investment in new capacity or referral linkages to other providers.
Maximizing revenue and reducing inappropriate ED use through improved billing and collections, along the lines of HCHD’s “Everyone Pays” initiative.
No change in the organization of city and county public health departments.
No new organizing or governance structure.
Reactive Reconfiguration Option:Objectives and Key Features

84
We examined the dimensions of such a system, including benefits and risks for Harris County, and compared its outcomes with the status quo.
We concluded that, despite some improved system efficiencies and financial performance, this option will not: Infuse enough new capacity to meaningfully improve
access to care reduce inappropriate ED use. Will not build needed coordination linkages across
provider sites and levels of care to reduce system fragmentation.
Reactive Reconfiguration Option:Summary Assessment

85
In contrast to the reactive option, proactive options seek to build a system with greater capacity and coordination that is maximally efficient and effective.
Both proactive options developed present more ambitious scenarios to improve access and reduce fragmentation of care, but differ with respect to such factors as: Community orientation.
Expansion of linkages between public and private not-for-profit health systems.
Scale of commitment to investment in new ambulatory care access points.
Creating new coordinating entities that consolidate currently fragmented efforts.
Framework for Revisioning Health Carein Harris County: Proactive Options

86
We developed two proactive options: Strategic Realignment; and
The Coordinated Community Health System
We then assessed their expected outcomes and recommended a preferred option for Harris County
Framework for Revisioning Health Carein Harris County: Proactive Options

87
CurrentSystemCurrentSystem
CurrentCapacity/
Coordination
HeightenedSystem
Efficiency
New Capacityand
Coordination
FullyRebalanced
System
1
2
3
Least Comprehensive
MostComprehensive
Strategic Realignment
Option
Strategic Realignment
Option
ReactiveOption
ReactiveOption
Ran
ge o
f C
on
fig
ura
tion
O
pti
on
s
Strategic Realignment Reconfiguration Option

88
This proactive option assumes that investment in new capacity and coordination is imperative to offer appropriate lower cost alternatives to non-emergent ED use and reduce system fragmentation.
The proposed new capacity, scheduled to phase-in by 2015, is diverse, featuring a variety of access points to care. It is grounded, however, on a pragmatic assumption that funding and commitment may not be available to support the full complement of new capacity needed to address current unmet need among safety net populations in Harris County.
Strategic Realignment Reconfiguration Option:Objectives and Key Features

89
This option also calls for establishing a limited referral network for redirecting inappropriate ED visits to clinics, FQHCs, FQHC look-alikes and urgent and specialty care centers and transferring selected patient care services from the city and county public health departments to the Harris County Hospital District (HCHD).
Strategic Realignment Reconfiguration Option:Objectives and Key Features

90
System components include new capacity and ambulatory care access points, including: A network of seven new FQHC and FQHC look-
alikes sufficient to treat 175,000 annual visits, or about 25% of current unmet need for primary care by the uninsured in Harris County.
New outpatient specialty clinics and urgent care centers to accommodate referrals from new ambulatory care access points and other community providers.
Strategic Realignment Reconfiguration Option:New Capacity

91
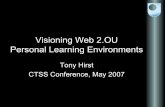
The new FQHC/FQHC look-alike network will require support of annual operating deficits. Financing of about $31 million will be required to
meet operating deficits that are projected to occur between 2005-2014 as new capacity is phased in.
Annual operating losses are projected to peak at about $4.6 million between 2007-2010 and then fall.
Caveat: Converting HCHD clinics to FQHCs requires careful legal assessment, due to possible adverse impacts on federal disproportionate share payments to HCHD.
Strategic Realignment Reconfiguration Option:Financing New Capacity

92
Notes: Assumes each site has 25,000 visit capacity and a $4.5 million annual operating budget;analysis excludes capital costs; assumes initial annual operating deficits of $1.5 millionfor FQHCs and $2.0 million for look-alikes; assumes sites are phased-in between 2005-2011;assumes deficits are eliminated in 3 years for FQHCs and 4 years for look-alikes throughrevenue diversification.
$2.25
$3.44
$4.55 $4.60 $4.57
$4.07
$0.61
$0.02
$2.33
$4.60
$-
$1
$1
$2
$2
$3
$3
$4
$4
$5
$5
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
Year
An
nu
al
Do
llar
Lo
sses
(m
illio
ns
)
Strategic Realignment Reconfiguration Option
Estimated Annual Operating Lossesof Seven New FQHCs and FQHC Look-alikes
2005-2014

93
Selective new initiatives for better coordinating care include: Establishing a limited referral network between
hospitals and ambulatory care centers to refer non-emergent patients from EDs to appropriate ambulatory care sites and refer patients from those sites to hospitals for specialty and diagnostic services.
Expanding the current county telephone nurse triage system and current community health education efforts. – Potential funding sources might include Greater Houston
provider organizations and grants.
Strategic Realignment Reconfiguration Option:Coordination of Care

94
Formation of a coordinating board to provide oversight and a unified planning structure for the FQHC and FQHC look-alike network. Board representation should reflect the diversity of
Harris County and include community, government and private and public health sector representation.
The Board would be authorized and funded to plan and begin implementing network expansion.
Strategic Realignment Reconfiguration Option:Coordination of Care

95
City City County County HCHD HCHD Patient Care Services
Patient Care Services
CollaborateCollaborate
Strategic Realignment Reconfiguration Option:Continued City/County Public Health Autonomy
Maintain each agency’s autonomy, but transfer selected women’s and children’s primary health care services to HCHC and explore greater collaboration between city and county health departments.

96
The pragmatic approach of meeting a pre-defined scope of need limits the risks of implementation failure, and: This option carefully phases-in meaningful capacity in a manner
that limits annual deficit funding and other financial risk.
This option builds some coordination between hospitals and ambulatory care sites to improve coordination of care and reduce inappropriate ED use.
This option may lower system-wide costs to the extent non-emergent care can be appropriately redirected to lower cost alternatives.
Transfer of selected patient care services to HCHD improves care coordination and facilitates “one stop shopping” for consumers.
This option may prove a useful fallback if the implementation risks of the option described below prove too daunting.
Strategic Realignment Reconfiguration Option:Summary Assessment

97
After examining the dimensions of the Strategic Realignment option in the context of its likely effectiveness in addressing issues of concern, we concluded that this approach is superior to the Reactive option.
In return for some investment, it partially rebalances the system by adding valuable primary care and other capacity, builds some system coordination infrastructure and creates a foundation for future expansion.
Strategic Realignment Reconfiguration Option:Summary Assessment Conclusion
However, we believe implementing this option will,at best, buy time, as significant unmet need and
fragmentation of care will remain and ED overcrowding,and its effects, will likely continue.

98
CurrentSystemCurrentSystem
CurrentCapacity/
Coordination
HeightenedSystem
Efficiency
New Capacityand
Coordination
FullyRebalanced
System
1
2
3
Least Comprehensive
MostComprehensive
CoordinatedCommunity
Health System Option
CoordinatedCommunity
Health System Option
Strategic Realignment
Option
Strategic Realignment
Option
ReactiveOption
ReactiveOption
Ran
ge o
f C
on
fig
ura
tion
O
pti
on
s
The Coordinated CommunityHealth System (CCHS) Option

99
Efficient and effective health care requires a balanced and integrated system of services designed to move patients rapidly to the most appropriate treatment setting.
The framework of this second proactive option is designed to help put in place the infrastructure to help achieve this in Harris County.
It encompasses the elements of both previous options, but is bolder and more far-reaching and is the strategy of choice.
The cornerstone of such a system for meeting the needs of Harris County residents is a strong, well coordinated ambulatory care network.
The CCHS Option: Overview

100
By 2015, CCHS calls for: Substantial investment in new capacity sufficient to meet
current demand for primary care by the uninsured. Significant improvements in system-wide coordination
through a county-wide patient referral network similar to Chicago’s.
Expanded and coordinated medical and behavioral health patient call center and community health education center capacity.
Consolidation of city and county public health functions. Establishing a high level public/private governance
structure to maintain the oversight and coordination required for effective system functioning.
The CCHS Option: Summary

101
EDs
Hospitals
Call Center
FQHCsBehavioral
Health
FQHC Look-Alikes
Urgent Care
Centers
Specialty Clinics
Health Education
Public Health
HarrisCounty CCHC
EDs
Hospitals
Call Center
FQHCsBehavioral
Health
FQHC Look-Alikes
Urgent Care
Centers
Specialty Clinics
Health Education
Public Health
HarrisCounty CCHC
The Recommended Option:Coordinated Community Health System

102
CCHS calls for a county-wide coordinated network of new ambulatory care access points, including: Five new FQHCs and nine FQHC look-alikes, each
able to see 50,000 visits annually, to address unmet need for primary care by the uninsured.
Additional outpatient specialty clinics and urgent care centers as called for by the HCHD strategic plan to accommodate referrals from new ambulatory care access points and other community providers.
Additional school-based health services and education.
The CCHS Option:Investment in New Capacity

103
The FQHC/FQHC look-alike network meets primary care demand with less financial risk than other clinic models: FQHCs/FQHC look-alikes are eligible for enhanced
Medicare and Medicaid funding and discounted drug pricing.
FQHCs also may receive malpractice coverage and federal Section 330 grant funding up to $650,000 annually.
Sites are required to provide primary, preventive and behavioral health services directly or by arrangement.
The CCHS Option:Investment in New Capacity

104
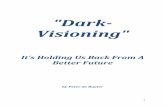
The new FQHC/FQHC look-alike network will require financing substantial operating deficits during the network phase-in period. Total estimated operating losses of about $158
million are projected between 2005-2017 as new capacity is phased in.
The CCHS Option:Investment in New Capacity

105
Notes: Assumes each site has 50,000 visit capacity and $9 million operating budget; excludes capitalcosts; assumes initial annual operating deficits of $3.4 million for 5 FQHCs and $4.0 millionfor 9 look-alikes; assumes sites are phased-in between 2005-2015; assumes deficits areeliminated in 3 years for FQHCs and 4 years for look-alikes through revenue diversification.
$16.56
$14.28
$12.28
$9.28
$7.40
$1.00
$2.00
$5.16
$8.28$8.56
$10.56
$15.56
$13.28
$-
$2
$4
$6
$8
$10
$12
$14
$16
$18
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
Year
An
nu
al D
olla
r L
oss
es (
mil
lion
s)
Harris County CCHS Option
Estimated Annual Operating Lossesfor 14 New FQHCs and FQHC Look-alikes
2005-2017

106
Improving care coordination will require community-wide involvement and linkages.
At the provider level, these include: Establishing county-wide, contractually-based patient referral
linkages between hospital EDs, clinics and urgent care centers a la the Chicago model, to reduce fragmentation of care.
Use of a Web-based system to coordinate patient referrals. Use of common IT and data reporting systems and integrating
patient medical records to follow patients across sites of care. Integrating behavioral health and primary care services in
FQHC/FQHC look-alikes.
The CCHS Option:Improving Care Coordination

107
At the community level, these include: Expanding the telephone nurse triage system to add a 24/7
mental health and substance abuse call center to provide counseling and referral services county-wide.
Developing a health education center and establishing linkagesto the telephone nurse triage system.
– The health education center would teach consumers how and when to access both providers and insurers.
– The education and telephone triage and counseling centers coordinate in sharing information to better target educational strategies, message development and consumer outreach.
The CCHS Option:Improving Care Coordination
Goal:To improve coordination of behavioral and physical health services and reduce inappropriate ED use.

108
Proposed call center and health education linkages.
Call CenterCall Center Health EducationHealth EducationLiaison/CollaborateLiaison/Collaborate
Analyze call volume to identify issues and
trends.
Tailor health education topicsand outreach strategies to address major issues and
trends.
The CCHS Option:Improving Care Coordination

109
Under CCHS, City and County population health functions are consolidated and selected women and children’s patient care services are transferred to HCHD.
City and CountyCity and County HCHD HCHD Patient Care Services
Patient Care Services
The CCHS Option:Restructuring Public Health Functions

110
Consolidating public health departments, as proposed in the past, would provide county-wide centralized administration of public health functions and provide a consistent level of services across city and county.
The CCHS Option:Restructuring Public Health Functions

111
This reorganization would also establish a focal point for public health accountability and allow for a county-wide unified response to public health emergencies. Other expected benefits of consolidating public health departments include: Flexibility to deploy resources county-wide where needed. Maintains autonomy of the local public health sector, while
streamlining and rationalizing services. Improves care coordination through “one stop shopping ” for
consumers. Serves as a useful transition for possible future consolidation
with HCHD and possibly MHMRA.
The CCHS Option:Restructuring Public Health Functions

112
Consolidation of public health departments could be conducted under the guidance of a transition plan that describes: The transfer of selected patient services to HCHD. The merger of city and county health departments. The establishment of county-wide administrative
and governance structures. The development of a sustainable funding
mechanism.
The CCHS Option:Restructuring Public Health Functions

113
An independent governance structure with representation and strong leadership by senior community leaders is an important element of the CCHS option.
The Board would provide oversight and coordination.
The CCHS Option:Create a High Level Governance Structure

114
Board membership should reflect the diversity of Harris County and should have sufficient credibility to enjoy the strong support of elected officials. To help achieve these goals, board membership might include: Senior city and county political leadership. Senior leaders with acknowledged credentials from
the medical community. Representation from business community leaders. Representation from not-for-profit sector leaders.
The CCHS Option:High Level Governance Structure

115
Essential principles of a framework to guide effective board operation should include: Sufficient independence from day-to-day political
pressure to operate effectively, but remain accountable for results.
An independent and reliable funding base. A leadership succession strategy to ensure
continuity of commitment. Ongoing Board training and education.
The CCHS Option:High Level Governance Structure

116
Implementing CCHS offers Harris County residents many benefits, including: A much better balanced network of health care providers and
services. Significantly reduced inappropriate ED use. Greatly strengthened system coordination and linkages across levels
of care. Improved public health efficiency and effectiveness. Expanded community access to appropriate care, emphasizing lower
cost primary and preventive services. Better integration of behavioral health with community-based primary
care. More appropriate and cost efficient use of health care by consumers
through expanded and coordinated health education and call center capacity.
The CCHS Option:Assessment of Benefits

117
The relative boldness of this option also carries with it a number of implementation challenges. These include: The need for significant investment in new capacity in the face
of possible funding constraints, including:– Stiff nation-wide competition for and limited availability of federal
funding for future FQHC expansion. – State cutbacks in Medicaid and CHIP eligibility.– Little likelihood that the Texas legislature will increase Medicaid
outpatient and physician payment rates.
Maintaining continuity of strong and committed leadership over time.
Clinical staff recruitment for the expanded network may be challenging in the face of nation-wide work force shortages.
The CCHS Option:Assessment of Challenges

118
On balance, CCHS appears to be the best strategic option for Harris County. While challenging to implement, we believe CCHS will, more than the other two options examined: Reduce inappropriate ED use and fragmentation of care in the
most efficient and effective manner. Assure optimal use of public and private financial resources. Proactively position Harris County for the future.
Implementing this approach may also heighten Harris County’s health care leadership profile nationally and enhance its ability to attract new businesses to spur continued regional economic growth.
The CCHS Option:Conclusion and Recommendation