
RCS 6080 Medical and Psychosocial Aspects of Rehabilitation Counseling Rheumatic Diseases.
42
Medical and Psychosocial Aspects of Rehabilitation Counseling Rheumatic Diseases
-
Upload
elijah-sydney-cobb -
Category
Documents
-
view
220 -
download
1
Transcript of RCS 6080 Medical and Psychosocial Aspects of Rehabilitation Counseling Rheumatic Diseases.
RCS 6080 Medical and Psychosocial Aspects of Rehabilitation
Counseling
Rheumatic Diseases

Rheumatoid Arthritis The prevalence of rheumatoid arthritis in most
Caucasian populations approaches 1% among adults 18 and over and increases with age, approaching 2% and 5% in men and women, respectively, by age 65
The incidence also increases with age, peaking between the 4th and 6th decades
The annual incidence for all adults has been estimated at 67 per 100,000

Rheumatoid Arthritis Both prevalence and incidence are 2-3 times
greater in women than in men
African Americans and native Japanese and Chinese have a lower prevalence than Caucasians
Several North American Native tribes have a high prevalence
Genetic factors have an important role in the susceptibility to rheumatoid arthritis

Rheumatoid Arthritis Rheumatoid arthritis is an autoimmune disease in
which the normal immune response is directed against an individual's own tissue, including the joints, tendons, and bones, resulting in inflammation and destruction of these tissues
The cause of rheumatoid arthritis is not known Investigating possibilities of a foreign antigen, such as a virus

Rheumatoid Arthritis Description
Morning stiffness Arthritis of 3 or more joints Arthritis of hand joints Symmetric arthritis Rheumatoid nodules Serum rheumatoid factor Radiographic changes
A person shall be said to have rheumatoid arthritis if he or she has satisfied 4 of 7 criteria, with criteria 1-4 present for at least 6 weeks

Rheumatoid Arthritis Rheumatoid arthritis usually has a slow, insidious
onset over weeks to months
About 15-20% of individuals have a more rapid onset that develops over days to weeks
About 8-15% actually have acute onset of symptoms that develop over days

Functional Presentation and Disability of RA In the initial stages of each joint
involvement, there is warmth, pain, and redness, with corresponding decrease of range of motion of the affected joint
Progression of the disease results in reducible and later fixed deformities
Muscle weakness and atrophy develop early in the course of the disease in many people

Complications of Rheumatoid Arthritis Complications include:
Carpal tunnel syndrome, Baker’s cyst, vasculitis, subcutaneous nodules, Sjögren’s syndrome, peripheral neuropathy, cardiac and pulmonary involvement, Felty’s syndrome, and anemia

Treatment and Prognosis Medications
NSAIDS - Usually, only one such NSAID should be given at a time. Can be titrated every two weeks until max dosage or response is obtained. Should try for at least 2 to 3 wk before assuming inefficacy.
Slow acting - Generally, if pain and swelling persist after 2 to 4 mo of disease despite treatment with aspirin or other NSAIDs, can add a slow-acting or potentially disease-modifying drug (eg, gold, hydroxychloroquine, sulfasalazine, penicillamine) Methotrexate, an immunosuppressive drug is now increasingly also used very early as one of the second-line potentially disease-modifying drugs.

Medications Corticosteroids – offer the most effective short-term relief
as an anti-inflammatory drugs. Long-term though improvement diminishes. Corticosteroids do not predictably prevent the progression of joint destruction, although a recent report suggested that they may slow erosions. Severe rebound follows the withdrawal of corticosteroids in active disease.
Immunosuppressive drugs These drugs (eg, methotrexate, azathioprine, cyclosporine) are increasingly used in management of severe, active RA. They can suppress inflammation and may allow reduction of corticosteroid doses. Major side effects can occur, including liver disease, pneumonitis, bone marrow suppression, and, after long-term use of azathioprine, malignancy.

Treatment Surgery: video
Removal of inflamed synovium
Arthroplasty
Physical therapy

Vocational Implications of Rheumatoid Arthritis Need to make frequent assessments of the person’s
functional ability as the disease progresses in order to provide realistic goals and support
Motor coordination, finger and hand dexterity, and eye-hand-foot coordination are adversely affected
Vocational goals dependent on fine, dexterous, or coordinated movement of the hand are not ideal

Vocational Implications of Rheumatoid Arthritis Most jobs requiring medium to heavy lifting are
not desirable
Activities such as climbing, balancing, stooping, kneeling, standing, or walking are hampered
Extremes of weather or abrupt changes in temperature should be avoided – indoor controlled climate better

Lupus Systemic lupus
erythematosus (also called SLE, or lupus) is an autoimmune disease of the body's connective tissues. Autoimmune means that the immune system attacks the tissues of the body. In SLE, the immune system primarily attacks parts of the cell nucleus.
SLE affects tissues throughout the body. Five times as many women as men get SLE. Most people develop the disease between the ages of 15 and 40, although it can show up at any age.

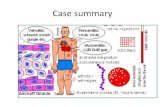
Lupus - Anatomy SLE causes tissue
inflammation and blood vessel problems pretty much anywhere in the body. SLE particularly affects the kidneys. The tissues of the kidneys, including the blood vessels and the surrounding membrane, become inflamed (swollen), and deposits of chemicals produced by the body form in the kidneys. These changes make it impossible for the kidneys to function normally.
Note the granular appearance of the cortex of these lupus affected kidneys – it’s across the entire surface of both kidneys suggesting a chronic condition.

Lupus Anatomy (cont). The inflammation of SLE can be seen in the
lining, covering, and muscles of the heart. The heart can be affected even if you are not feeling any heart symptoms. The most common problem is bumps and swelling of the endocardium, which is the lining membrane of the heart chambers and valves.
SLE also causes inflammation and breakdown in the skin. Rashes can appear anywhere, but the most common spot is across the cheeks and nose.
People with SLE are very sensitive to sunlight. Being in the sun for even a short time can cause a painful rash. Some people with SLE can even get a rash from fluorescent lights.
Rashes caused by SLE are red, itchy, and painful. The most typical SLE rash is called the butterfly rash, which appears on the face – particularly the cheeks and across the nose. SLE can also causes hair loss. The hair usually grows back once the disease is under control.

Lupus Anatomy (joints) Almost everyone with SLE has
joint pain or inflammation. Any joint can be affected, but the most common spots are the hands, wrists, and knees. Usually the same joints on both sides of the body are affected. The pain can come and go, or it can be long lasting. The soft tissues around the joints are often swollen, but there is usually no excess fluid in the joint. Many SLE patients describe muscle pain and weakness, and the muscle tissue can swell.

Lupus Anatomy Lupus can also affect the nervous system
causing headaches, seizures, and organic brain syndrome.
It can cause anemia due to blood loss or from the kidney disease (it does not directly effect the red blood cells).
Pregnancy: the chances of miscarriage, premature birth, and death of the baby in the uterus are high.

Seronegative Spondyloarthropathy
Consist of a group of related disorders that include Reiter's syndrome, ankylosing spondylitis, psoriatic arthritis, and arthritis in association with inflammatory bowel disease
Occurs more age at diagnosis in the third decade and a peak commonly among young men, with a mean incidence between ages 25 and 34
The prevalence appears to be about 1%
The male-to-female ratio approaches 4 to 1 among adult Caucasians
Genetic factors play an important role in the susceptibility to each disease

Seronegative Spondyloarthropathy
The cause is unclear, but there is strong evidence that the initial event involved interaction between genetic factors and environment factors, particularly bacterial infections
Reiter’s syndrome may follow a wide range of GI infections
Bowel inflammation has been implicated in the pathogenesis of endemic Reiter’s syndrome, psoriatic arthritis, and ankylosing spondylitis

Seronegative Spondyloarthropathy The spondyloarthropathies share certain common features,
including the absence of serum rheumatoid factor, an oligoarthritis commonly involving large joints in the lower extremities, frequent involvement of the axial skeleton, familial clustering, and linkage to HLA-B27
These disorders are characterized by inflammation at sites of attachment of ligament, tendon, fascia, or joint capsule to bone (enthesopathy)

Sacroiliitis Sacroiliitis is an
inflammation of the sacroiliac joint. Symptoms usually include a
fever and reduced range of motion.
Picture on the bottom right shows an individual with – sacroiliitis and Ankylosing Spondylitis. The arrows point to the inflamed and narrowed SI joints. They are white due to bony sclerosis around the joints

Ankylosing Spondylitis Chronic disease that primarily
affects the spine and may lead to stiffness of the back. The joints and ligaments that normally permit the back to move become inflamed. The joints and bones may grow (fuse) together.
The effects are inflammation and chronic pain and stiffness in the lower back that usually starts where the lower spine is joined to the pelvis or hip.
Diagnosis is made through: (a) medical history including symptoms, (b) X-rays, and possibly (c) blood tests for HLA-B27 gene

Ankylosing Spondylitis Treatment options:
With early diagnosis and treatment, pain and stiffness can be controlled and may reduce fusing. In women, AS is usually mild and hard to diagnose.
Exercise Medications: NSAIDs,
Sulfasalazine Posture management Self-help aids Surgery

Reiter's Syndrome Arthritis that produces pain, swelling, redness and
heat in the joints. It can affect the spine and commonly involves the joints of the spine and sacroiliac joints. It can also affect many other parts of the body such as arms and legs. Main characteristic features are inflammation of the joints, urinary tract, eyes, and ulceration of skin and mouth.
The symptoms are fever, weight loss, skin rash, inflammation, sores, and pain.

Reiter's Syndrome Reiter's often begins following
inflammation of the intestinal or urinary tract. It sets off a disease process involving the joints, eyes, urinary tract, and skin. Many people have periodic attacks that last from three to six months. Some people have repeated attacks, which are usually followed by symptom-free periods.
Diagnosis is made through a physical exam, skin lesions, and a test for the HLA-B27 gene

Reiter's Syndrome For different parts of the body,
different treatments are used: Medications: NSAIDs, antibiotics, topical skin
medications Eye drops Joint protection
Various symptoms are treated by healthcare specialists

Psoriatic Arthritis Causes pain and swelling in
some joints and scaly skin patches on some areas of the body.
The symptoms are: About 95% of those with psoriatic
arthritis have swelling in joints outside the spine, and more than 80% of people with psoriatic arthritis have nail lesions. The course of psoriatic arthritis varies, with most doing reasonably well.
Silver or grey scaly spots on the scalp, elbows, knees and/or lower end of the spine.
Pitting of fingernails/toenails Pain and swelling in one or more
joints Swelling of fingers/toes that gives
them a "sausage" appearance.
Psoriatic Arthritis Diagnosis may involve X-rays, blood
tests, and joint fluid tests. Treatment options:
Skin care Light treatment (UVB or PUVA) Corrective cosmetics Medications: glucocorticoids, NSAIDs, DMARDs
(disease-modifying anti-rheumatic drugs) Exercise Rest Heat and cold Splints Surgery (rarely)

Inflammatory Bowel Disease IBD consists of two
separate diseases that cause inflammation of the bowel and can cause arthritis or inflammation in joints:
Crohn's Disease involves inflammation of the colon or small intestines.
Ulcerative Colitis is characterized by ulcers and inflammation of the lining of the colon.

Inflammatory Bowel Disease The amount of the bowel disease usually
influences the severity of arthritis symptoms. Other areas of the body affected by inflammatory bowel disease include ankles, knees, bowel, liver, digestive tract, skin, eyes, spine, and hips.
Treatment options: Diet Exercise Medication: Corticosteroids, Immunosuppressants, NSAIDs,
Sulfasalazine Surgery

Functional Presentation and Disability of the Spondylarthropathies When the axial skeleton is involved,
the initial symptom is morning stiffness and lower back pain
As the disease worsens, there is progressive diminution of motion of the spine
Eventually, the sacroiliac joints, lumbar, thoracic, and cervical spine become fused
At this stage, the spine is no longer painful, but the person has lost all ability to flex or rotate the spine and generally develops a hunched-over posture with fused flexion of the cervical spine and flexion contracture of the hips to compensate for the loss of the lordosis curvature in the lumbar spine

Functional Presentation and Disability of the Spondylarthropathies The joints where the ribs attach to the
vertebrae are also affected, and chest expansion and lung volume are decreased
Frequently, peripheral joints are involved, and the pattern is usually asymmetric oligoarthritis involving primarily the large or medium joints, including the hips, knees, and ankles
Rarely are smaller joints or the joints in the upper extremities involved
Loss of motion of the spine or pain in the spine with motion generally affects a person's mobility

Functional Presentation and Disability of the Spondylarthropathies
Walking remains unimpaired unless the hips and knees are affected
Frequent stooping and bending become impossible
A person with ankylosing spondylitis typically is able to continue vocational activity despite progressive stiffness, unless it requires significant back mobility or physical labor

Vocational Implications of the Spondylarthropathies
The person should be considered for vocational or professional education as resources and interests dictate
A stiff back will limit the person’s rotation and flexion so that overall dexterity may be affected
Tasks that require reaching or bending will be difficult and lifting over 10-15 pounds may cause increased back pain
Climbing and balancing skills, stooping, and kneeling may be tolerated initially but become difficult as the disease worsens
Need time to stretch spine frequently

Degenerative Joint Disease(Osteoarthritis) Most common rheumatic
disease and is characterized by progressive loss of cartilage and reactive changes at the margins of the joint and in the subchondral bone
The disease usually begins in one’s 40s
Prevalence increases with age and the disease becomes almost universal in individuals aged 65 and older
Primarily affects weight-bearing joints such as the knees, hips, and lumbrosacral spine

Degenerative Joint Disease Cause is unclear Considered to be a “wear and tear” arthritis
and is thought to occur as a consequence of some earlier damage or overuse of the joint
Obesity is frequently associated with it Genetic factors play a role in the
development that is sex-influenced and dominant in females, resulting in an incidence 10 times greater than in men
The final outcome is full-thickness loss of cartilage down to bone

Degenerative Joint Disease In early disease, pain
occurs only after joint use and is relieved by rest
As the disease progresses, pain occurs with minimal motion or even at rest
Nocturnal pain is commonly associated with severe disease

Functional Limitations and Degenerative Joint Disease Limited use of the involved joint
Walking and transfer activities may be impaired
Generally, ADLs will not be significantly impaired

Treatment and Prognosis of Degenerative Joint Disease Meds Early PT/exercises Heat/cold therapy Joint protection Surgery
Osteoarthritis is a slowly progressive disease The eventual outcome is complete
destruction of the joint, and ultimately surgical intervention is required

Vocational Implications and Degenerative Joint Disease Can continue in present job unless it requires
dexterous or heavy use of the involved joint Heavy lifting should be avoided Light to medium work should be possible Climbing, balancing skills, stooping, and
kneeling may be impaired Returning to work after surgery requires
intensive postop rehab and continued exercise to maintain muscle strength
Most individuals are able to sustain gainful employment and a normal level of activity

Additional Resources and Information from the Web American College of Rheumatology (
www.rheumatology.org) National Institute of Arthritis and Musculoskeletal and
Skin Diseases (www.niams.nih.gov) Arthritis Foundation (www.arthritis.org) Arthritis National Research Foundation (
www.curearthritis.org) Info on Juvenile RA (
http://www.nlm.nih.gov/medlineplus/juvenilerheumatoidarthritis.html)
Spondylitis Association of America (www.spondylitis.org)
Arthritis.com: Latest Arthritis Information & Community (www.arthritis.com)











![Darby Free Library [6080]](https://static.fdocuments.net/doc/165x107/55a2bbd61a28ab3f5f8b47a2/darby-free-library-6080.jpg)



