Rbc disorders-3
55
HEMOLYTIC ANEMIAS Dr.CSBR.Prasad, M.D.,
-
Upload
prasad-csbr -
Category
Health & Medicine
-
view
1.457 -
download
5
description
Target: UG students of medicine.
Transcript of Rbc disorders-3

HEMOLYTIC ANEMIAS
Dr.CSBR.Prasad, M.D.,

Clinical presentation
• Anemia
• Jaundice
• Organomegaly
• Delayed mile stones
• Dysmorphic facies
• Gall stones in young

Hemolytic anemias Common features:
• Premature destruction of red cells
• Elevated erythropoietin
• Accumulation of hemoglobin degradation products

Destruction of RBCs
• Physiologically takes place in mononuclear phagocytic system (Spleen,Liver, BM)
• Terms:
– Extravascular hemolysis
– Intravascular hemolysis

Extravascular hemolysis
• Caused by alterations that render the red cell less deformable
• Clinical features:
– Anemia
– Splenomegaly &
– Jaundice

Intravascular hemolysis
Causes: • Mechanical injury
– Prosthetic heart valves – Fibrin Thrombi in microcirculation or – Repetitive physical trauma
• Marathon running
• Complement fixation – Abs to RBCs
• Intracellular parasites – Malaria
• Exogenous toxic factors – Clostridial sepsis

Intravascular hemolysis
Manifested by:
• Anemia
• Hemoglobinemia
• Hemoglobinuria
• Hemosiderinuria, and
• Jaundice
• No splenomegaly

Intravascular hemolysis
• Low serum haptoglobin
• Methemoglobinemia
• Renal hemosiderosis
• Elevated serum bilirubin levels (UC)
• Gall stones
• Increased urobilinogen

Hemolytic Anemias - investigations
• Peripheral smear – Fragmented RBC, nucleated RBC, polychromatophilic cells,
• ↑ Reticulocytes • Bone marrow
– ↑ Cellularity, M:E ratio 1:1 (Erythroid hyperplasia) – ↑ Normoblasts
• Extramedullary hematopoiesis • ↑ Bilirubin – cholelithiasis • Hemosiderosis

Red cell sequestration in splenic sinusoids

There are numerous fragmented RBC's seen here. Some of the irregular shapes appear
as "helmet" cells. Such fragmented RBC's are known as "schistocytes" and they are
indicative of a microangiopathic hemolytic anemia (MAHA) or other cause for
intravascular hemolysis. This finding is typical for disseminated intravascular
coagulopathy (DIC).

Polychromatophilic cells

Reticulocyte

Fig. 1.24
Normal marrow fragments and cell trails.

Hereditary Spherocytosis (HS)

• Inheritance
– AD (75%)
– Compound heterozygosity
• Northern Europe (1 in 5000)
• Defective cell membrane skeleton
• Spherical & less deformable RBC
• Splenic sequestration % destruction

Pathogenesis
• Cytoskeletal defect
• The life span of the affected red cells 10 to 20 days

Hereditary Spherocytosis
• Spectrin – Major protein of membrane cytoskeleton
• Two polypeptide chains – α and β
• Spectrin is tethered to the inner surface of cell membrane by ankyrin, protein 4.2 to trans membrane transporter band 3



Hereditary Spherocytosis
• Gene mutation involving ankyrin, protein 4.2, spectrin or band 3 reduce membrane stability
• Spontaneous loss of cell membrane
• ↓ Cell surface to volume ratio – spheroidal shape
• Spherocytes are less deformable and vulnerable to splenic sequestration and destruction

Schematic representation of the red cell membrane cytoskeleton and alterations leading to spherocytosis and hemolysis

Red cell sequestration in splenic sinusoids

Hereditary Spherocytosis
• Clinical features – Anemia - varies
– Splenomegaly
– Jaundice
• Aplastic crisis – triggered by parvovirus infection of marrow precursor
• Hemolytic crisis

Hereditary Spherocytosis
• Hb – normal / decreased
• MCV – decreased
• MCHC – increased more than 36 gm/dl
• PBS – Spherocytes
– Reticulocytosis – more than 8%
– Nucleated RBC
• Osmotic fragility test

Osmotic fragility test

Osmotic fragility test

Hereditary Spherocytosis

Hereditory Spherocytosis

The size of many of these RBC's is quite small, with lack of the central zone of pallor.
These RBC's are spherocytes. In hereditary spherocytosis, there is a lack of spectrin, a
key RBC cytoskeletal membrane protein. This produces membrane instability that
forces the cell to the smallest volume--a sphere. In the laboratory, this is shown by
increased osmotic fragility. The spherocytes do not survive as long as normal RBC's.

Reticulin stain

Hereditary Spherocytosis
• Osmotic fragility test – Confirmatory test
• Spherocytes are vulnerable to osmotic lysis induced in vitro by hypotonic salt solution
• Hemolysis starts at 0.8 gm% and completes between 0.5 – 0.4 gm%

G6PD - deficiency

Name the two important products of HMP shunt
• NADPH
• Ribose-5-Phophate


G6PD - deficiency
• Erythrocytes are vulnerable to oxidant induced injury
• Intracellular reduced glutathione (GSH) inactivates oxidant
• G6PD is needed for maintaining adequate quantity of GSH

G6PD - deficiency
• Sulfhydral group of globin chain of Hb is oxidized.
• Hb precipitate to form Heinz bodies – damage the cell membrane
• Bite cells
• Intravascular hemolysis


Heinz bodies

G6PD - deficiency
Oxidant stress • Drugs
– Antimalaria – primaquine – Sulfonamide – Sulfones – Nitrofurans – Analgesic
• Infection – Viral hepatitis, pneumonia, typhoid fever • Food – fava beans (Favism)

G6PD - deficiency
• X – linked disorder • More than 350 G6PD genetic variants are recognised • G6PD A-
– 10% of American black – Normal enzyme activity in reticulocyte – Unstable enzyme – half time 13 days (62 days)
• G6PD Mediterranean – Severe ↓ enzyme activity – less than 10% – Severe hemolysis

G6PD - deficiency
• Asymptomatic
• Infectious disease / drug exposure
• Sudden onset of anemia
• Hemoglobinuria, Hemoglobinemia
• Abdominal / low back pain
• Self limited

G6PD - deficiency
• PBS
– Spherocytes, erythrocyte fragments, bite cells, Heinz bodies, polychromasia
• Measurement of enzyme activity
– Fluorescent spot test
– Dye reduction test

Polychromatophilic cells

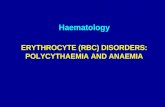
PNH Paroxysmal Nocturnal Hemoglobinuria

• Incidence of 2 to 5 per million

Acquired Membrane disorder
• Paroxysmal nocturnal hemoglobinuria (PNH) is a disease that results from acquired mutations in the phosphatidylinositol glycan complementation group A gene (PIGA), an enzyme that is essential for the synthesis of certain cell surface proteins

Attachment of proteins to cell membrane
• Transmembrane proteins
• GPI linked proteins: The others are attached to the cell membrane through a covalent linkage to a specialized phospholipid called glycosylphosphatidylinositol (GPI).
• In PNH, these GPI-linked proteins are deficient because of somatic mutations that inactivate PIGA

• PNH blood cells are deficient in three GPI-linked proteins that regulate complement activity:
1. decay–accelerating factor, or CD55
2. Membrane inhibitor of reactive lysis, or CD59
3. C8 binding protein.
• Of these factors, the most important is CD59, a potent inhibitor of C3 convertase that prevents the spontaneous activation of the alternative complement pathway.

• Red cells, platelets, and granulocytes deficient in these GPI-linked factors are abnormally susceptible to lysis or injury by complement
• In red cells this manifests as intravascular hemolysis
• The hemolysis is paroxysmal and nocturnal

Urine samples from a typical PNH patient

PNH is diagnosed by flow cytometry

Major vein thrombosis
• Thrombosis is the leading cause of disease-related death in individuals with PNH
• Other causes:
– Protein C / S deficiency
– Factor V Leiden
– Hyperfibrinogenemia

END

Dr.CSBR.Prasad, M.D.,
Associate Professor of Pathology,
Sri Devaraj Urs Medical College,
Kolar-563101,
Karnataka,
INDIA.