Yoga Ratnawali - Shri Kanth Shambhu _3274 , 3275_Alm_15_shlf_3_Devanagari - Ayurveda_Part1
Upload
ravi-kanthCategory
view
223download
0
8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 1/95
DR.RAVIKANTHDR.RAVIKANTH
PG[GEN. MED]PG[GEN. MED]

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 2/95
DEFINITIONDEFINITION
EPIDEMIOLOGYEPIDEMIOLOGY
CLASSIFICATIONCLASSIFICATION ETIOLOGYETIOLOGY
PATHOGENESISPATHOGENESIS
MANAGEMENTMANAGEMENT

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 3/95
DEFINITIONDEFINITION
Heart failure (HF) is a clinical syndromeHeart failure (HF) is a clinical syndrome
that occurs in pt¶s who because of that occurs in pt¶s who because of
inherited or acquired abnormality of inherited or acquired abnormality of cardiac structure or function, develop acardiac structure or function, develop a
constellation of clinical features that leadconstellation of clinical features that lead
to frequent hospitalizations, a poor qualityto frequent hospitalizations, a poor quality
of life, and a shortened life expectancyof life, and a shortened life expectancy

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 4/95
EPIDEMIOLOGYEPIDEMIOLOGY
HF prevalence rises with age.HF prevalence rises with age.
affects 6affects 6± ±10% of people over the age of 10% of people over the age of
65.65. relative incidence of HF is lower in womenrelative incidence of HF is lower in women
overall prevalence of HF is increasing, inoverall prevalence of HF is increasing, in
part because of advances in managementpart because of advances in managementof cardiac disorders, such as MI, valvular of cardiac disorders, such as MI, valvular
heart disease, and arrhythmias,heart disease, and arrhythmias,

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 5/95
Prevalence of CHF by Year 2030Prevalence of CHF by Year 2030Prevalence of CHF by Year 2030Prevalence of CHF by Year 2030
5.7
4.2
3
0
1
2
3
4
5
6
1990 Estimate 2010 Projection 2030 Projection
Cardiology Roundtable. 1998. Estimate based on expert interviews. Aging America: Trends and
Projections. 1991 ed. US Dept. of Health and Human Services, Washington, DC, 1991.

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 6/95
1
11
% OF
POPULATION
45 - 54 55 -64 65 - 74 75+
AGE [YRS]
PREVALENCE OF HF
MALES
FEMALES
Braunwald 8th edn
8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 7/95
classificationclassification
HF patients categorized into two groups:HF patients categorized into two groups:
Because these two conditions haveBecause these two conditions have
distinct pathophysiology & prognosis.distinct pathophysiology & prognosis.

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 8/95
CLASSIFICATION
OF
HEART FAILURE
HF with Depressed
EF[Systolic failure]
HF with Preserved
EF[Diastolic failure]

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 9/95
ETIOLOGYETIOLOGY
DEPRESSED EF
CAD
CHRONIC PRESSURE OVERLOAD
CHRONIC VOLUME OVERLOAD
NON ISCHAEMIC DILATED CARDIOMYOPATHY
DISORDERS OF RATE & RHYTHM

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 10/95
PRESERVED EF
PATHOLOGICAL HYPERTROPHY
AGING
RESTRICTIVE CARDIOMYOPATHY
FIBROSIS
ENDOMYOCARDIAL DISORDERS

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 11/95
ETOLOGIES OF HF
CAD
OTHERS
CAD -HTN
CAD
CAD -HTN
OTHERS

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 12/95
Pulmonary Heart DiseasePulmonary Heart Disease
Cor pulmonaleCor pulmonale
Pulmonary vascular disordersPulmonary vascular disorders
HighHigh--Output StatesOutput States
Metabolic disorders ;Thyrotoxicosis,Metabolic disorders ;Thyrotoxicosis,Nutritional disorders (beriberi)Nutritional disorders (beriberi)
Excessive bloodExcessive blood--flow requirements;flow requirements;--Systemic arteriovenous shuntingSystemic arteriovenous shunting
--Chronic anemiaChronic anemia

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 13/95
Pathogenesis of HFPathogenesis of HF
with depressed EFwith depressed EF
Progressive disorder Progressive disorder
initiated by index eventinitiated by index event
Initially asymptomatic due to activatinInitially asymptomatic due to activatinof compensatory mechanismsof compensatory mechanisms
Transition from asymptomatic toTransition from asymptomatic to
symptomatic HF occurs due tosymptomatic HF occurs due to
ventricular remodellingventricular remodelling..

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 14/95

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 15/95

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 16/95
Compensatory mechanisms areCompensatory mechanisms are--
Activation of RAA & adrenergic nervous Activation of RAA & adrenergic nervous
system.system. Inc. myocardial contractility.Inc. myocardial contractility.
Activation of vasodilatory agents like Activation of vasodilatory agents like
ANP/BNP/PGE2/PGI2/NO ANP/BNP/PGE2/PGI2/NO

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 17/95
NEURO HORMONAL ACTIVATION NEURO HORMONAL ACTIVATION ± ±
Facilitate perfusion of vital organs initially.Facilitate perfusion of vital organs initially.
But finally contribute to end organ changes inBut finally contribute to end organ changes inheart & excess salt & water retention inheart & excess salt & water retention in
advanced HFadvanced HF

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 18/95
Compensatory mechanisms of HF
8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 19/95
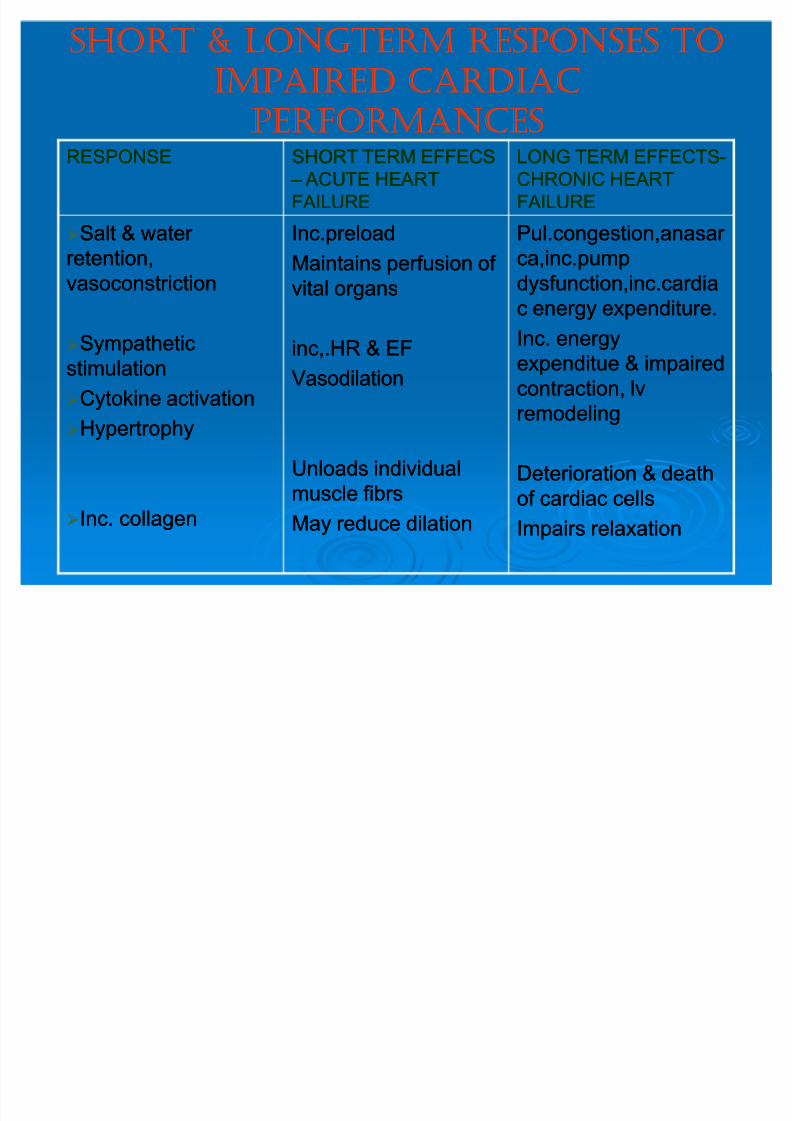
SHORT & LONGTERM RESPONSES TOSHORT & LONGTERM RESPONSES TO
IMPAIRED CARDIACIMPAIRED CARDIAC
PERFORMANCESPERFORMANCESRESPONSERESPONSE SHORT TERM EFFECSSHORT TERM EFFECS
± ± ACUTE HEART ACUTE HEART
FAILUREFAILURE
LONG TERM EFFECTSLONG TERM EFFECTS--
CHRONIC HEARTCHRONIC HEART
FAILUREFAILURE
Salt & water Salt & water
retention,retention,
vasoconstrictionvasoconstriction
SympatheticSympathetic
stimulationstimulation
Cytokine activationCytokine activation
HypertrophyHypertrophy
Inc. collagenInc. collagen
Inc.preloadInc.preload
Maintains perfusion of Maintains perfusion of
vital organsvital organs
inc,.HR & EFinc,.HR & EF
VasodilationVasodilation
Unloads individualUnloads individual
muscle fibrsmuscle fibrs
May reduce dilationMay reduce dilation
Pul.congestion,anasar Pul.congestion,anasar
ca,inc.pumpca,inc.pump
dysfunction,inc.cardiadysfunction,inc.cardiac energy expenditure.c energy expenditure.
Inc. energyInc. energy
expenditue & impairedexpenditue & impaired
contraction, lvcontraction, lv
remodelingremodeling
Deterioration & deathDeterioration & death
of cardiac cellsof cardiac cells
Impairs relaxationImpairs relaxation

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 20/95
LV RemodellingLV Remodelling
StimulusStimulus
Mechanical stretch of myocyteMechanical stretch of myocyte
Circulating neurohormonesCirculating neurohormones Inflammatory cytokinesInflammatory cytokines
Reactive oxygen speciesReactive oxygen species

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 21/95
Structural/functional changesStructural/functional changes
Myocyte hypertrophyMyocyte hypertrophy
Alterations in contractile properties of Alterations in contractile properties of myocytemyocyte
Progressive loss of myocyteProgressive loss of myocyte
Beta adrenergic desensitisationBeta adrenergic desensitisationReorganisation of extracellular matrixReorganisation of extracellular matrix
which doesn¶t provide supportwhich doesn¶t provide support

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 22/95
All these lead toAll these lead to
Decreased cardiac outputDecreased cardiac output
Inc lv dilationInc lv dilation Inc hemodynamic overloadigInc hemodynamic overloadig

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 23/95
8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 24/95
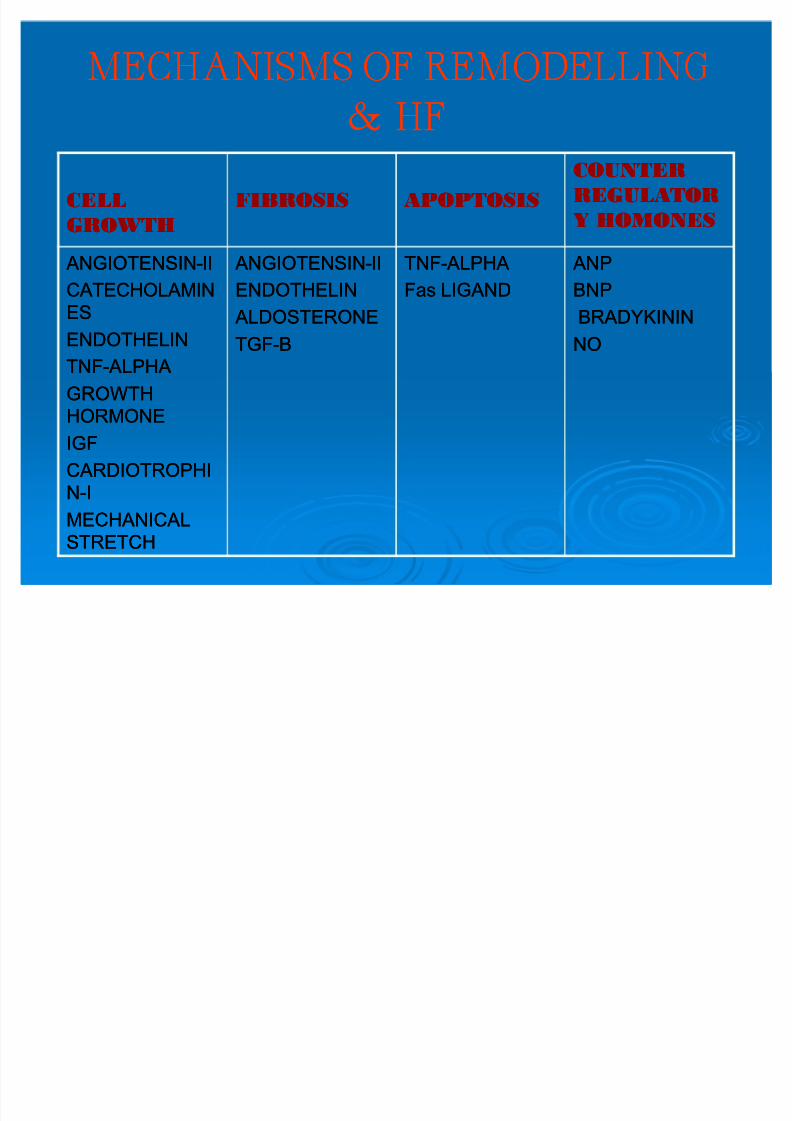
MECHANISMS OF REMODELLINGMECHANISMS OF REMODELLING
& HF& HF
CELL CELL
GROWTHGROWTH
FIBROSISFIBROSIS APOPTOSISAPOPTOSIS
COUNTERCOUNTER
REGULATORREGULATOR
Y HOMONESY HOMONES
ANGIOTENSIN ANGIOTENSIN--IIII
CATECHOLAMINCATECHOLAMIN
ESES
ENDOTHELINENDOTHELIN
TNFTNF--ALPHA ALPHA
GROWTHGROWTH
HORMONEHORMONEIGFIGF
CARDIOTROPHICARDIOTROPHI
NN--II
MECHANICALMECHANICAL
STRETCHSTRETCH
ANGIOTENSIN ANGIOTENSIN--IIII
ENDOTHELINENDOTHELIN
ALDOSTERONE ALDOSTERONE
TGFTGF--BB
TNFTNF--ALPHA ALPHA
Fas LIGANDFas LIGAND
ANP ANP
BNPBNP
BRADYKININBRADYKININ
NONO

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 25/95
Pathogenesis of HF
with normal EF

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 26/95
CRITERIA FOR DIASTOLIC HFCRITERIA FOR DIASTOLIC HF
Definitive evidence of CHFDefinitive evidence of CHF
Objective evidence of normal LV systolicObjective evidence of normal LV systolic
functionfunctionObjective evidence of LV diastolicObjective evidence of LV diastolic
dysfunctiondysfunction
MEDICINE UPDATE 2010

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 27/95
DIFFERENCESDIFFERENCES
DHFDHF SHFSHF
EFEF normalnormal decreaseddecreased
Regional wallRegional wall
thicknessthickness
increasedincreased decreaseddecreased
EDVEDV NormalNormal increasedincreased
MEDICINE UPDATE 2010
8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 28/95
SYMPTOMSSYMPTOMS
MAJORMAJOR
DysneaDysnea
OrthopneaOrthopnea
PndPnd Bil pedal edemaBil pedal edema
FatigueFatigue
Pulmonary edemaPulmonary edema
Exercise intoleranceExercise intolerance
cachexiacachexia
MINORMINOR
Wt.lossWt.loss
CoughCough
NocturiaNocturia
PalpitationsPalpitations
Peripheral cyanosisPeripheral cyanosis
depressiondepression

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 29/95
SIGNSSIGNS
MAJORMAJOR
TachycardiaTachycardia
Inc.venouspressureInc.venouspressure
Positive hepatojugular reflexPositive hepatojugular reflexRalesRales
TacypneaTacypnea
S3S3
HepatomegalyHepatomegaly
Ankle edema Ankle edema
Ascites Ascites
Pleural effusionPleural effusion
MINORMINOR
MRMR
CardiomegalyCardiomegaly
HypotensionHypotension
Pulsus alternansPulsus alternans
ExtrasystolesExtrasystoles
AF AF
Wt.lossWt.loss

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 30/95
FRAMINGHAM CRITERIAFRAMINGHAM CRITERIA
MAJOR CRITERIAMAJOR CRITERIA PND or orthopneaPND or orthopnea
neck vein distensionneck vein distension
RalesRales
CardiomegalyCardiomegaly
Acute pulmonary Acute pulmonary
edema,s3 gallopedema,s3 gallop
Hepatojugular Hepatojugular reflexreflex
IcreasedIcreased venous pressurevenous pressure
MINOR CRITERIAMINOR CRITERIA Ankle edema Ankle edema
ExertionalExertional dysneadysnea
HepatomegalyHepatomegaly
Pleural effusionPleural effusion
Decreased vital capacityDecreased vital capacity
Tachycardia[>120/min]Tachycardia[>120/min]

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 31/95
MAJOR OR MINOR CRITERIAMAJOR OR MINOR CRITERIA
Wt.loss > 4.5 kg in 5 days in response toWt.loss > 4.5 kg in 5 days in response to
treatmenttreatmentDIAGNOSISDIAGNOSIS
2 MAJOR2 MAJOR
1MAJOR + 2 MINOR1MAJOR + 2 MINOR
8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 32/95
DIFFERENTIAL DIAGNOSISDIFFERENTIAL DIAGNOSIS
Pulmonary diseasePulmonary disease
pneumonia,asthma,copdpneumonia,asthma,copd
Sleep disordered breathingSleep disordered breathing
ObesityObesity
Renal failureRenal failure
Hepatic failureHepatic failure
HypoalbuminemiaHypoalbuminemia
Venous stasisVenous stasis

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 33/95
EVALUATION OF PTÙS WITH HFEVALUATION OF PTÙS WITH HF
Routine lab testingRoutine lab testing Cbp,sr.cr,electrolytes,ck,troponin,LFT,Cbp,sr.cr,electrolytes,ck,troponin,LFT,
TSH,urine analysisTSH,urine analysis
ChestChest--xx--rayray yesyes
ecgecg yesyes
2d2d--echoecho yesyes
Holter monitoringHolter monitoring No,unless symptoms of arrythmiaNo,unless symptoms of arrythmia
Exercise testingExercise testing yesyes
Coronary angiographyCoronary angiography Selected pt¶s with CADSelected pt¶s with CAD
biomarkersbiomarkers YesYes
CTCT
MRIMRI
FOLLOWFOLLOW--UPUP ClinicalClinical
examination,electrolytes,bnp,ecg,2examination,electrolytes,bnp,ecg,2
dd--echo when indicatedecho when indicated
8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 34/95
ECGECG
Normal ecg excludes systolic dysfunction.Normal ecg excludes systolic dysfunction.
To asessTo asess
Rhythm abnormalitiesRhythm abnormalitiesHypertrophyHypertrophy
MIMI

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 35/95
CHEST XCHEST X--RAYRAY
Inc. calibre ul vesselsInc. calibre ul vessels
Septal linesSeptal lines
Small pl. effusionsSmall pl. effusions
Thickened interlobar Thickened interlobar
fissuresfissures
Bats wingBats wing
Vascular pedicle inc.Vascular pedicle inc. CardiomegalyCardiomegaly

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 36/95
KERLEYKERLEY--B LINESB LINES BasesBases
11--2 cm long2 cm long
Horizontal in directionHorizontal in direction
Perpendicular toPerpendicular topleural surfacepleural surface
KERLEYKERLEY--C LINESC LINES
Near hilumNear hilum Run obliquelyRun obliquely
Longer than BLonger than Blineslines

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 37/95
2d2d--echoecho
To assesTo asses
Lv functionLv function
Valvular abnormalitiesValvular abnormalitiesRegional wall motion abnormalitiesRegional wall motion abnormalities
Severity of lv remodellingSeverity of lv remodelling

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 38/95

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 39/95
BIOMARKERSBIOMARKERS
Provide diagnostic & prognosticProvide diagnostic & prognostic
information.information.
Predicts response to treatmentPredicts response to treatmentCommonly used are BNP & ProCommonly used are BNP & Pro--BNPBNP
Increased in both systolic & diastolicIncreased in both systolic & diastolic
dysfuction.dysfuction.Normal BNP excludesNormal BNP excludes HF.HF.

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 40/95
BNPBNP
32 AA polypeptide32 AA polypeptide
SourceSource ± ± ventricleventricle
Predictor of high LVPredictor of high LV
EDPEDP
Increases with ageIncreases with age
Women have highWomen have high
BNP than men[in nonBNP than men[in non--chf]chf]
Cut off point 80 pg/mlCut off point 80 pg/ml
1
81
55 -
64
65 -
74
75+
non - chf n
non- chf omen
CARDIOLOGY CLINICSCARDIOLOGY CLINICS--by JAMES B. YOUNGby JAMES B. YOUNG

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 41/95
THERAPEUTIC THERAPEUTIC
MONITORING MONITORING
U seful to evaluate longtermU seful to evaluate longterm
effects of short term Rx effects of short term Rx
ENDPOINTS ENDPOINTS-- death &death &
readmission ratesreadmission rates
Pt¶s with more BNP during Pt¶s with more BNP during
hosp & prehosp & pre-- discharge hasdischarge has
more end pointsmore end points
Final BNP < 430pg/ml is strong Final BNP < 430pg/ml is strong NPV for re admissionNPV for re admission 0
1600
END
N
N N
END
N
b f r Rx
ft r Rx
CARDIOLOGY CLINICSCARDIOLOGY CLINICS--by JAMES B. YOUNGby JAMES B. YOUNG
8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 42/95
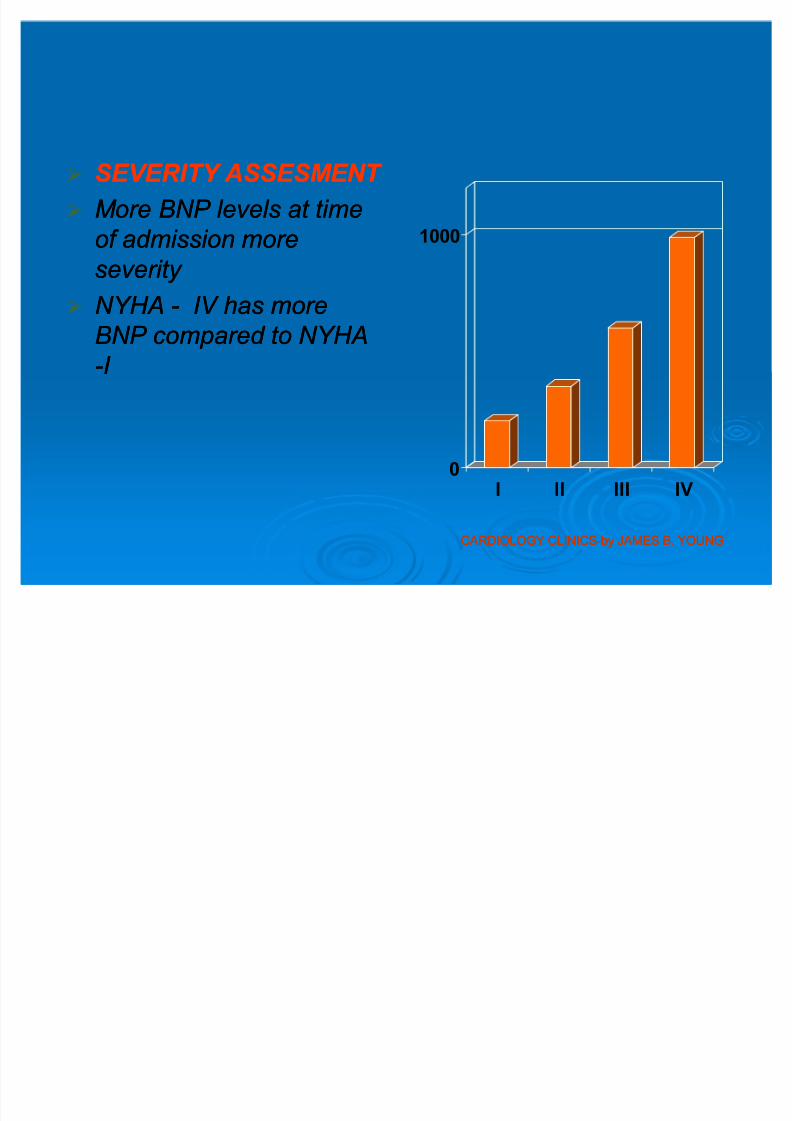
S EVERITY ASS E S MENT S EVERITY ASS E S MENT
M ore BNP levels at timeM ore BNP levels at time
of admission moreof admission more
severity severity NYHANYHA -- IV has moreIV has more
BNP compared to NYHABNP compared to NYHA
--I I
0
1000
I II III IV
CARDIOLOGY CLINICSCARDIOLOGY CLINICS--by JAMES B. YOUNGby JAMES B. YOUNG

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 43/95
ROLE IN ACUTE HF ROLE IN ACUTE HF
to differentiate acute hf to differentiate acute hf
from other causes of from other causes of
dyspneadyspnea
To predict outcomeTo predict outcome
M ore bnp levels indicateM ore bnp levels indicate
more symptomsmore symptoms
0
100
200
300
400
500
600700
800
900
1000
N N-
CH
V D CH
CARDIOLOGY CLINICSCARDIOLOGY CLINICS--by JAMES B. YOUNGby JAMES B. YOUNG

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 44/95
THERAPEUTIC THERAPEUTIC
MONITORING MONITORING
U seful to evaluate longtermU seful to evaluate longterm
effects of short term Rx effects of short term Rx
ENDPOINTS ENDPOINTS-- death &death &readmission ratesreadmission rates
Pt¶s with more BNP during Pt¶s with more BNP during
hosp & prehosp & pre-- discharge hasdischarge has
more end pointsmore end points
Final BNP < 430pg/ml is strong Final BNP < 430pg/ml is strong NPV for re admissionNPV for re admission 0
1600
END
IN
N N
END
IN
b f r Rx
ft r Rx
CARDIOLOGY CLINICSCARDIOLOGY CLINICS--by JAMES B. YOUNGby JAMES B. YOUNG

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 45/95
DIFFERNTIATION DIFFERNTIATION
Other conditionsOther conditions
Cor pulmonaleCor pulmonale
Pul.embolismPul.embolism
HTNHTN
LvhLvh
Acute or chronic Acute or chronic
ischemiaischemia0
10
20
30
40
50
60
H N D C D
CARDIOLOGY CLINICSCARDIOLOGY CLINICS--by JAMES B. YOUNGby JAMES B. YOUNG

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 46/95
Other biomarkersOther biomarkers
CRPCRP
TNFTNF--alphaalphaUric acid levelsUric acid levels
Surfectant proteinSurfectant protein--BB
Growth differentiating factor[gdf Growth differentiating factor[gdf--15]15]

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 47/95
MANAGEMENTMANAGEMENT
ACUTE HF ACUTE HF
CHRONIC HFCHRONIC HF
NEWER THERAPIESNEWER THERAPIES ACC GUIDELINES ACC GUIDELINES

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 48/95
ACUTE HF ACUTE HF

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 49/95
PRECIPITANTS OF HFPRECIPITANTS OF HF
POTENTIALLYPOTENTIALLYPRE ENTABLEPRE ENTABLE
NOTREADILYNOTREADILYPRE ENTABLEPRE ENTABLE
Poor dietary compliancePoor dietary compliance
Poormedical compliancePoormedical compliance
Use of drugs precipitatingUse of drugs precipitating
HFHF
inadequate HTN treatmentinadequate HTN treatment
Anemia Anemia
Excess alcohol consumptionExcess alcohol consumption
Acute MI Acute MI
Arrythmias Arrythmias
InfectionInfection
Acute valvular insufficiency Acute valvular insufficiency
Endocrine abnormalitiesEndocrine abnormalities

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 50/95
TREATMENT GOALSTREATMENT GOALS
Stabilize hemodynamic derangements thatStabilize hemodynamic derangements that
provoked symptomsprovoked symptoms
Identify & treat reversible factors thatIdentify & treat reversible factors thatprecipitated HFprecipitated HF
ReRe--establish effective OP regimen toestablish effective OP regimen to
prevent relapse & disease progressionprevent relapse & disease progression
Educate pt & familyEducate pt & family

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 51/95
CRITERIA FOR ADMISSIONCRITERIA FOR ADMISSION
E IDENCE OF SE ERELY E IDENCE OF SE ERELY DECOMPENSATED HFDECOMPENSATED HF
HypotensionHypotension
worsening renal functionworsening renal function
altered mentationaltered mentation
DYSPNEA AT RESTDYSPNEA AT REST
reflected by tachypnea at restreflected by tachypnea at rest
o2 sat < 90%o2 sat < 90% HEMODYNAMICALLY SIGNIFICANT HEMODYNAMICALLY SIGNIFICANT ARRYTHMIASARRYTHMIAS
including new onset AFincluding new onset AF
ACUTE CORONARY SYNDROMESACUTE CORONARY SYNDROMESHFSA GUIDE LINES

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 52/95
Immediate resuscitation
Pt distressed or in pain
Arterial o2 saturation>95%
Normal HR & Rhythm
Mean BP>70 mm hg
yes
no
no
yes
yes
yes
yes
No
no
no
Fluid challengeAdeqate preload
Inc.fio2,consider cpap,nippv
Pacing,antiarrythmics,etc
asodilators,consider diuresis
If volume overload
Analgesia or sedation
If moribund bls,als
Adeqate CO,reversal of metabolic
Acidosis ,svo2>65%,signs of Adeqate perfusion
no
yes
Consider inotropes or further
After load manipulation
Reasses freqently

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 53/95
HEMODYNAMIC PROFILES IN HEMODYNAMIC PROFILES IN
ACUTE HFACUTE HF
Elevated lv filling pressuresElevated lv filling pressures
PROFILE APROFILE A
Warm & dryWarm & dry
PROFILE BPROFILE B
Warm &wetWarm &wet
PROFILE LPROFILE L
Cold& dryCold& dry
PROFILE CPROFILE C
Cold&wetCold&wet

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 54/95
Hemodynamic classification provides useful guide for Hemodynamic classification provides useful guide for selecting initial optimal therapiesselecting initial optimal therapies
ProfileProfile--B[ to decrease lv filling pressures]B[ to decrease lv filling pressures]
DiureticsDiuretics
Vasodilators[ntg,nitropruside,nesiritide]Vasodilators[ntg,nitropruside,nesiritide]
ProfileProfile--c[to inc. CO & dec.lv filling press]c[to inc. CO & dec.lv filling press]
dobutaminedobutamine
dopaminedopamine
milrinonemilrinone ProfileProfile--LL
fluid therapy/dopaminefluid therapy/dopamine
TREATMENT STRATEGIES OF HFTREATMENT STRATEGIES OF HF

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 55/95
TREATMENT STRATEGIES OF HFTREATMENT STRATEGIES OF HF
olume Volume
over loadover load
Worsening Worsening
renal renal
functionfunction
SystolicSystolic
>100mm of >100mm of
hghg
Blood Blood
9090--100100
PressurePressure
<90<90
yesyes yesyes Vasodilator Vasodilator
diureticsdiuretics
vasodilator/invasodilator/in
otropeotrope
diureticsdiuretics
Inotrope/dopaInotrope/dopa
minemine
diureticdiuretic
yesyes nono Vasodilator Vasodilator diureticsdiuretics
Vasodilator/inVasodilator/inotropeotrope
Recheck vol.Recheck vol.statusstatus
Inotrope/dopaInotrope/dopa
minemine
diureticsdiuretics
nono yesyes Vasodilator for Vasodilator for
hyprtnsve HFhyprtnsve HF
Vasodilator/inVasodilator/in
otropeotrope
Rechck volRechck vol
statusstatus
Inotrope/dopInotrope/dop
Nor Nor--e/vpe/vp
nono nono vasodilator vasodilator treat astreat as
CardiogenicCardiogenic
shockshock
same assame as
aboveabove

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 56/95
INITIATING DOSEINITIATING DOSE MAXIMUM DOSEMAXIMUM DOSE
VASODILATORSVASODILATORS
NitroglycerinNitroglycerin
NitroprussideNitroprusside
NesiritideNesiritide
2020 mcg/minmcg/min
1010 mcg/minmcg/min
Bolus 2Bolus 2 mcg/kgmcg/kg
4040 ± ± 400400 mcg/minmcg/min
3535 ± ± 350350 mcg/minmcg/min
0.010.01 ± ± 0.030.03 mcg/kg/minmcg/kg/min
INOTROPESINOTROPES
DobutamineDobutamine
MilrinoneMilrinone
DopamineDopamine
levosimendanlevosimendan
11 ± ± 2 mcg/kg/min2 mcg/kg/min
Bolus 50 mcg/kgBolus 50 mcg/kg
11 ± ± 2 mcg/kg/min2 mcg/kg/min
Bolus 12 mcg/kgBolus 12 mcg/kg
22-- 10 mcg/kg/min10 mcg/kg/min
0.10.1 ± ± 0.75 mcg/kg/min0.75 mcg/kg/min
22 ± ± 4 mcg/kg/min4 mcg/kg/min
0.10.1 ± ± 0.2 mcg/kg/min0.2 mcg/kg/min
VASOCONSTRICTORVASOCONSTRICTOR
SS
DopamineDopamine
epinephrineepinephrine
5 mcg/kg/min5 mcg/kg/min
0.5 mcg/kg/min0.5 mcg/kg/min
55 ± ± 15 mcg/kg/min15 mcg/kg/min
50 mcg/kg/min50 mcg/kg/min
8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 57/95
CRITERIA FOR DISCHARGECRITERIA FOR DISCHARGE
At least 24 hr stable fluid status,BP,renal At least 24 hr stable fluid status,BP,renal
function on oral regimen planned for homefunction on oral regimen planned for home
Should be free of dyspnea,symptomaticShould be free of dyspnea,symptomatic
hypotension while at rest & walking smallhypotension while at rest & walking small
distancesdistances
HFSA GUIDE LINES

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 58/95
CHRONIC HFCHRONIC HF

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 59/95
High Risk: Hypertension, coronary artery disease, diabetes, family
history of cardiomyopathy
Asymptomatic LVD: Previous MI, LV systolic dysfunction,
asymptomatic valvular disease
Symptomatic HF: Known structural
heart disease, shortness of breath and
fatigue, reduced exercise tolerance
Refractory
End-Stage HF:
Marked symptoms
at rest despite maximalmedical therapy
AA
BB
CC
DD
Heart Failure Disease Progression:Heart Failure Disease Progression:
ACC/AHA Heart Failure StagesACC/AHA Heart Failure Stages
Heart Failure Disease Progression:Heart Failure Disease Progression:
ACC/AHA Heart Failure StagesACC/AHA Heart Failure Stages
ACC/AHA = American College of Cardiology/American Heart Association; LVD = left ventricular
dysfunction; MI = myocardial infarction. Adapted from Yancy CW et al. Prim Care Spec Ed. 2002;6:15-19.

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 60/95
STAGESTAGE--A A STAGESTAGE--BB STAGESTAGE--CC STAGESTAGE--DD
High risk for High risk for developmentdevelopment
of HF,noof HF,no
structuralstructural
abnormalityabnormality
HaveHavestructuralstructural
abnormality,abnormality,
no symptomsno symptoms
HaveHavestructuralstructural
abnormality,abnormality,
symptomssymptoms
RefractoryRefractoryHF requiringHF requiring
specialisedspecialised
interventionsinterventions
Pt¶s withPt¶s with
HTN,CAD,DHTN,CAD,D
M or usingM or using
cardiotoxinscardiotoxinswith familywith family
h/o CMh/o CM
Pt¶s withPt¶s with
Previous MI,Previous MI,
Lv systolicLv systolic
dysfunction,dysfunction,
Asymptomati Asymptomati
c valvular c valvular
diseasedisease
Pt¶s with str.Pt¶s with str.
HeartHeart
disease,withdisease,with
sob,fatigue,resob,fatigue,reducedduced
exerciseexercise
intoleranceintolerance
Have markedHave marked
symptoms atsymptoms at
rest &rest &
refractory torefractory tomedicalmedical
treatmenttreatment

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 61/95
TREATMENT OF CHRONIC HFTREATMENT OF CHRONIC HF
STAGESTAGE--A A STAGESTAGE--BB STAGESTAGE--CC STAGESTAGE--DD
Treat HTN,Treat HTN,
EncourageEncourage
smoking cessation,smoking cessation,
Treat lipidTreat lipid
disorders,disorders,
Discourage alcoholDiscourage alcoholintake,intake,
Control metabolicControl metabolic
syndrome,syndrome,
ACE ACE-- I in appr. Pt¶sI in appr. Pt¶s
All measures All measures
under stageunder stage--aa
DRUGSDRUGS--
ACE ACE--II
ARB¶S ARB¶S
BB-- blockersblockersDevices inDevices in
selected pt¶sselected pt¶s
ICD¶SICD¶S
All measures All measures
under stageunder stage--a,a,
stagestage--b.b.
Drugs routine useDrugs routine use
Diuretics for fluidDiuretics for fluid
retentionretention
ACE ACE--II
In selected pt¶sIn selected pt¶s
Aldosterone ant Aldosterone ant
agonistsagonists
ARB¶S ARB¶S
DigitalisDigitalisHydralazine/nitrateHydralazine/nitrate
DevicesDevices
Biventricular Biventricular
pacingpacing
ICD¶SICD¶S
All measures under All measures under
stagestage ± ±a,b,ca,b,c
DECCISIONDECCISION
REGARDINGREGARDING
HEARTHEART
TRANSPLACENTATTRANSPLACENTAT
ION,ION,
ChronicChronic
INOTROPES,INOTROPES,
PermanentPermanent
mechanical supportmechanical support
etcetc

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 62/95
STEPPED THERAPY OF HF

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 63/95
TREATMENT OF CHFTREATMENT OF CHF

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 64/95
TREATMENT OF CHFTREATMENT OF CHF
Asses for fluid retention
Fluid retention No fluid retention
diuretic ACE-I
B-BLOCKER
If persistent symptoms ARB¶S
ALDOSTERONE ANTAGONISTHYDRALAZINE + ISOSORBIDE/DIGOXIN
8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 65/95
DIURETIC S;DIURETIC S; Pt¶ s require chronic diuretic therapy often at lower dosesPt¶ s require chronic diuretic therapy often at lower doses
Decrease or discontinue if significant improvement in clinical status ocursDecrease or discontinue if significant improvement in clinical status ocurs
Consider following when congestion fails to improve with diuretic theraphyConsider following when congestion fails to improve with diuretic theraphy
--Na+ & fluid restrictionNa+ & fluid restriction--increase dose of loop diureticincrease dose of loop diuretic
--continuos infusioncontinuos infusion
--add orally[metalozone or spironolactone] or iv [chlorthiazide]add orally[metalozone or spironolactone] or iv [chlorthiazide]
--consider ultrafiltration finallyconsider ultrafiltration finally
Aldosterone antagonist¶s contraindication; Aldosterone antagonist¶s contraindication;--Sr.cr..>2.5mg/dlSr.cr..>2.5mg/dl
--sr.K+ >.5mmol/lsr.K+ >.5mmol/l
--in addition to othr K+ sparing diureticsin addition to othr K+ sparing diuretics
HFSA GUIDE LINES

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 66/95
Hydralazine/oral nitrate;Hydralazine/oral nitrate;
ConsiderationsConsiderations
in pt¶s intolerant to ACEin pt¶s intolerant to ACE--I/ARB¶S due toI/ARB¶S due tohyperkalemia ,renal insufficiencyhyperkalemia ,renal insufficiency
In pt¶s with LV dysfunction,remainIn pt¶s with LV dysfunction,remain
symptomatic despite standard therapysymptomatic despite standard therapy
8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 67/95
BB--BLOCKERS BLOCKERS -- RECOMMENDATIONSRECOMMENDATIONS
GeneralGeneral initiate lower dosesinitiate lower doses
UptitrateUptitrate gradually,nogradually,no sooner sooner than at 2 week intervalsthan at 2 week intervals
Maintain at max. dosesMaintain at max. doses
Consideration if symptom worse or Consideration if symptom worse or
side effects occur side effects occur
Adjust dose of diuretic Adjust dose of diuretic
Titrate to target dose onceTitrate to target dose once
symptoms resolvesymptoms resolve
If uptitration difficultIf uptitration difficult Prolong titration intervalProlong titration interval
Reduce target doseReduce target dose
Ref to HF specialistRef to HF specialist
Acute exacerbation of chronic HF Acute exacerbation of chronic HFoccursoccurs
Maintain therapy if possibleMaintain therapy if possible
Reduce dose if necessaryReduce dose if necessary
Avoid abrupt discontinuation Avoid abrupt discontinuation
If stoped/red restart graduallyIf stoped/red restart gradually
before dischargebefore discharge

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 68/95
DIGOXINDIGOXIN
RecommendationsRecommendations
Pt¶s with symptomatic LV dysfunction whoPt¶s with symptomatic LV dysfunction whohave AFhave AF
For pt¶s with symptoms & signs of HFFor pt¶s with symptoms & signs of HF
while receiving standard therapywhile receiving standard therapy
DOSE DOSE
0.1250.125-- 0.25mg/day0.25mg/day

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 69/95
ANTICOAGULATION ;[ANTICOAGULATION ;[WARFARINWARFARIN]]
RecommendationRecommendation Pt¶s with chronic or paroxysmal AFPt¶s with chronic or paroxysmal AF
With h/o systemic/pulmonary emboli [stroke/TIA]With h/o systemic/pulmonary emboli [stroke/TIA]
Recent large anterior MI or recent mi with LVRecent large anterior MI or recent mi with LV
thrombus[treated for initial 3 months]thrombus[treated for initial 3 months]
INRINR------22--33
ASPIRINASPIRIN
Used in low doses in HF with IHDUsed in low doses in HF with IHD

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 70/95
CARDIAC RESYNCHRONISATIONCARDIAC RESYNCHRONISATION
THERAPHY/BIVENTRICULAR PACINGTHERAPHY/BIVENTRICULAR PACING
RecommendationsRecommendations Pt¶s in sinus rhythm with EF < 35%,andPt¶s in sinus rhythm with EF < 35%,and
QRS>120msQRS>120ms
Who remain symptomatic despite medicalWho remain symptomatic despite medicaltherapytherapy

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 71/95
ICD¶SICD¶S
Used to reduce sudden cardiac deathUsed to reduce sudden cardiac death
Considered for pt¶s of classConsidered for pt¶s of class--II,III HF withII,III HF withEF <30EF <30--35% on optimal medical therapy35% on optimal medical therapy

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 72/95
ANEMIA ANEMIA
Look for reversible causes & treatLook for reversible causes & treat
Role of erythropoitin under investigationRole of erythropoitin under investigationRENAL DY S FUNCTION RENAL DY S FUNCTION
Poor prognosisPoor prognosis
Treated with standard medical therapyTreated with standard medical therapy
Fluid restrictionFluid restriction
Hemofiltration & CRRT consideredHemofiltration & CRRT considered
VITAMIN DEFICIENCY VITAMIN DEFICIENCY
Abstinence from alcohol Abstinence from alcohol
Rx thiamine deficiencyRx thiamine deficiency
COR PULMONALE COR PULMONALE
Rx underlying pulmonary disorder [bronchodilators,steroids,AB¶s,NIMV]Rx underlying pulmonary disorder [bronchodilators,steroids,AB¶s,NIMV]
DiureticsDiuretics
Digoxin has less roleDigoxin has less role

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 73/95

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 74/95
NEUTRAL ENDOPEPTIDASE INHIBITORSNEUTRAL ENDOPEPTIDASE INHIBITORS
Useful in chronic HFUseful in chronic HF
MOA; inhibition of NEP which degradeMOA; inhibition of NEP which degradenariuretic peptidesnariuretic peptides
Example;Example;candoxatril,ecadotril candoxatril,ecadotril
ISTAROXIMEISTAROXIME
MOA;inhibition of Na+/K+ ATPase &MOA;inhibition of Na+/K+ ATPase &stimulation of sarcolemmal ca+ pumpstimulation of sarcolemmal ca+ pumpwhich improves myocardial relaxationwhich improves myocardial relaxation

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 75/95
VASOPRESSIN ANTAGONISTSVASOPRESSIN ANTAGONISTS
MOA;MOA;V1aV1a--receptor receptor--mediate vasoconstrictionmediate vasoconstriction
V2V2--mediate water reabsorptionmediate water reabsorptionDrugs;Drugs;
conivaptanconivaptan--v1a & v2 receptor antagonistv1a & v2 receptor antagonist
tolvaptan &tolvaptan & lixivaptanlixivaptan--v2 antagonistsv2 antagonists

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 76/95
OTHER THERAPIESOTHER THERAPIES
Natriuretic peptidesNatriuretic peptides
Cardiac myosin activatorsCardiac myosin activators
Adenosine antagonists Adenosine antagonists
Cytokine targeting therapyCytokine targeting therapy
Immunomodulation therapyImmunomodulation therapy
Immunoglobulin or interferon therapyImmunoglobulin or interferon therapy
Matrix modulation therapyMatrix modulation therapy
8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 77/95
ACC 2009 GUIDE LINES ACC 2009 GUIDE LINES

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 78/95
ACCF/AHA practice guidelinesACCF/AHA practice guidelines are are intended tointended to
assist healthcare providers in clinicalassist healthcare providers in clinical
decision makingdecision making by describing a range of generallyby describing a range of generally
acceptable approachesacceptable approaches
for the diagnosis, management, andfor the diagnosis, management, andprevention of specific diseases or prevention of specific diseases or conditions.conditions.

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 79/95
Classification of RecommendationsClassification of Recommendations
CLASSCLASS--
11benifit >>> benifit >>>
riskrisk
CLASSCLASS--
2a 2a benefit>>riskbenefit>>risk
CLASSCLASS--
2b2b benefit > benefit >
risk risk
CLASSCLASS--
33Risk > Risk >
benifitbenifit
ProcedureProcedure
or or
treatmenttreatment
should beshould be
performedperformed
//
administer administer
eded
It isIt is
reasonablreasonabl
e toe to
performperform
ProcedureProcedure
/treatment/treatment
ProcedureProcedure
/treatment/treatment
may bemay be
considereconsidere
dd
ProcedureProcedure
/treatment/treatment
not to benot to be
performedperformed
,it may be,it may be
harmfulharmful
R OF HF WITH PRESERVED EFR OF HF WITH PRESERVED EF

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 80/95
Rx OF HF WITH PRE S ERVE D EF Rx OF HF WITH PRE S ERVE D EF STAGESTAGE--AA
ClassClass--11 Control of HTNControl of HTN
Treat lipid disordersTreat lipid disorders
Control blood sugar Control blood sugar
Avoid smoking,alcohol Avoid smoking,alcohol
Control rate or restore sinus rhythm in svt¶sControl rate or restore sinus rhythm in svt¶s
Treat thyroid disordersTreat thyroid disorders Perform periodic evaluation for signs &Perform periodic evaluation for signs &
symptoms of HFsymptoms of HF

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 81/95
ClassClass--22
ACE ACE--I or ARB¶S in pt¶s with h/oI or ARB¶S in pt¶s with h/o
atherosclerotic vascular atherosclerotic vascular disease,diabetes,or HTN with cvs riskdisease,diabetes,or HTN with cvs risk
factorsfactors

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 82/95
ClassClass--33
Nutritional supplements to preventNutritional supplements to prevent
development of structural heart disease.development of structural heart disease.

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 83/95
STAGESTAGE--BB
ClassClass--11 Apply All class Apply All class--1 recommendations as of stage1 recommendations as of stage--aa
BB--blocker&ACEblocker&ACE--I with h/o MI regardles of EF or I with h/o MI regardles of EF or
HF symptomsHF symptoms BB--blockr without h/o MI but with decreasd EF butblockr without h/o MI but with decreasd EF butno HF symptomsno HF symptoms
ACE ACE--I in all pt¶s with reducd EF with or withoutI in all pt¶s with reducd EF with or withouth/o MIh/o MI
Recommend coronary revascularisationRecommend coronary revascularisation Valvular replacement if hemodynamicalyValvular replacement if hemodynamicaly
significantsignificant

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 84/95
STAGESTAGE--BB
ClassClass--22
ACE ACE--I/ARB¶S for pt¶s with HTN & LVHI/ARB¶S for pt¶s with HTN & LVH
Placement of ICD in ischemic ³2a´/nonPlacement of ICD in ischemic ³2a´/nonischemic cardiomyopathy ³2b´ with EFischemic cardiomyopathy ³2b´ with EF
lessthan 30% &have reasonable lifelessthan 30% &have reasonable life
expectancy more than 1 yr expectancy more than 1 yr

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 85/95
ClassClass--33
Use of digoxin in pt¶s with lowUse of digoxin in pt¶s with low
EF,sinus rhythm,no h/o HF symptomsEF,sinus rhythm,no h/o HF symptomsUse of nutritional supplements to treatUse of nutritional supplements to treat
or prevent HFsymptomsor prevent HFsymptoms
Use of CCB¶S with negative inotropicUse of CCB¶S with negative inotropiceffect in asymptomatic pt¶s with loweffect in asymptomatic pt¶s with lowEF aftr MIEF aftr MI

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 86/95
STAGESTAGE--CC
ClassClass--11 Apply all clas Apply all clas--1 recommendations for stage1 recommendations for stage--aa
Diuretics&salt restriction in pt¶s of fluid retentionDiuretics&salt restriction in pt¶s of fluid retention ACE ACE--I in all unless contraindicatedI in all unless contraindicated
Avoid NSAID¶S,CCB¶S,anti Avoid NSAID¶S,CCB¶S,anti--arrythmicsarrythmics
exercise trainingexercise training
Placement of ICD in pt¶s with h/o cardiacPlacement of ICD in pt¶s with h/o cardiac
arrest,VF,VTarrest,VF,VT

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 87/95
ClassClass--2a2aDigitalis to decrease hospitalisationsDigitalis to decrease hospitalisations
Add combination of hydralazine & nitrate Add combination of hydralazine & nitratewith persistent symptoms inspite of takingwith persistent symptoms inspite of taking ACE ACE--I/BI/B--blockr blockr
ClassClass--2b2bUse of hydralazine/nitrate in pt¶s intolerantUse of hydralazine/nitrate in pt¶s intolerant
of ACEof ACE--I/ARB¶SI/ARB¶S

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 88/95
ICD therapy in pt¶s of IHD postICD therapy in pt¶s of IHD post--MI/non ischemicMI/non ischemic
cardiomyopathy with EF less than 30% withcardiomyopathy with EF less than 30% with
NYHA classNYHA class--2,3 symptoms to prolong survival2,3 symptoms to prolong survival
CRT in pt¶s of cardiac dyschrony,LVEF less thanCRT in pt¶s of cardiac dyschrony,LVEF less than30% in sinus rhythm,with NYHA class30% in sinus rhythm,with NYHA class--3,43,4
symptomssymptoms
Addition of aldosterone antagonist in selected Addition of aldosterone antagonist in selected
pt¶s if Sr.CR less than 2.5[men]/2 [women] &pt¶s if Sr.CR less than 2.5[men]/2 [women] &potassium less than 5mg/dlpotassium less than 5mg/dl

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 89/95
CLASSCLASS--33
Use of combination of ACEUse of combination of ACE--
I/ARB¶S/aldosterone antagonistsI/ARB¶S/aldosterone antagonistsUse of CCB¶SUse of CCB¶S
Longterm use of inotropic agentsLongterm use of inotropic agents

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 90/95
STAGESTAGE--DD
ClassClass--11
Meticulous identification &control of fluidMeticulous identification &control of fluid
retentionretentionRefer for cardiac transplantationRefer for cardiac transplantation
Offer pt¶s with implantable defibrillatorsOffer pt¶s with implantable defibrillators
8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 91/95
ClassClass--2a2a Consider left ventricular assist device in highlyConsider left ventricular assist device in highly
selected pt¶s with refractory end stage failureselected pt¶s with refractory end stage failure
classclass--2b2b
Pulmonary artery catheter placement to guidePulmonary artery catheter placement to guide
therapytherapy
Mitral valve repair/replacementMitral valve repair/replacement
Continuous infusion of inotropic agentsContinuous infusion of inotropic agents
8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 92/95
ClassClass--33
Partial left ventriculectomy not indicate inPartial left ventriculectomy not indicate in
pt¶s of non ischemic cardiomyopathypt¶s of non ischemic cardiomyopathyRoutine intermittent infusions of inotropicRoutine intermittent infusions of inotropic
agents not recommendedagents not recommended
8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 93/95
Treatment of HF with normal EFTreatment of HF with normal EF
ClassClass--11 Control HTNControl HTN
Control Ventricular rate in pt¶s of AFControl Ventricular rate in pt¶s of AF
Diuretics to control congestive symptomsDiuretics to control congestive symptomsClassClass--2a2a Coronary revascularisation in pt¶s of CADCoronary revascularisation in pt¶s of CAD
ClassClass--2b2b Restoration & maintanence of sinus rhythm in af Restoration & maintanence of sinus rhythm in af Use of bUse of b--bckr/acebckr/ace--i/arb¶s not wel establishedi/arb¶s not wel established
Use of digoxin not establishedUse of digoxin not established
8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 94/95
REFERENCESREFERENCES
HARRISON¶S 17HARRISON¶S 17 thth editionedition
BRAUNWALD¶S HEART DISEASE 8BRAUNWALD¶S HEART DISEASE 8 thth editionedition
HURST¶S Manual of cardiology 12HURST¶S Manual of cardiology 12thth editionedition
CARDIOLOGY CLINICSCARDIOLOGY CLINICS--by JAMES B. YOUNGby JAMES B. YOUNG
CARDIOLOGY UPDATE 2009CARDIOLOGY UPDATE 2009-- AMAL KUMAR AMAL KUMAR
BENERJEEBENERJEE
HEART FAILURE comprehensive guideHEART FAILURE comprehensive guide ± ± bybyG.WILLIAM DECG.WILLIAM DEC

8/4/2019 Ravi Kanth Heart Failure
http://slidepdf.com/reader/full/ravi-kanth-heart-failure 95/95