
CASE REPORT A Rare Case of Broad Ligament Fibroid: A Case ...
Upload
apollo-hospitalsCategory
view
105download
0
Rare c
case pictuures and p
presentatiion

ww.sciencedirect.com
a p o l l o m e d i c i n e 1 0 ( 2 0 1 3 ) 3 3 7e3 3 8
Available online at w
ScienceDirect
journal homepage: www.elsevier .com/locate/apme
Rare case pictures and presentation
Sundeep Upadhyaya a, Bhowmik Meghnathi b,*a Senior Consultant, Department of Rheumatology, Indraprastha Apollo Hospitals, Sarita Vihar, New Delhi, IndiabDNB Resident, Department of Rheumatology, Indraprastha Apollo Hospitals, Sarita Vihar, New Delhi, India
Keywords:
Tendon xanthomas
Arthritis
Familial hypercholesterolemia
Musculoskeletal system
Joint pains
* Corresponding author.E-mail address: [email protected]
0976-0016/$ e see front matter Copyright ªhttp://dx.doi.org/10.1016/j.apme.2013.11.006
1. A patient with arthralgias and nodularswelling over the knuckles and right Achillestendon
1.1. History and background
A 37-year-old male, non-smoker, non-diabetic patient, pre-
sented to the OPD at Indraprastha Apollo Hospital in 2005with
a history of progressive nodular swellings over the knuckles
(metacarpophalangeal joints), right Achilles tendon and both
elbows which were associated with joint pains (Fig. 3). There
was a swelling around the right ankle (medial aspect) (Fig. 4).
The patient had a mildly elevated ESR (30) and came with a
presenting diagnosis of sero-negative rheumatoid arthritis
and was on methotrexate and NSAID treatment, but to no
avail. His family history was unremarkable except for the
presence of cardiovascular disease. On further detailed
questioning it emerged that the patient’s father died at the age
of 33 years due tomyocardial infarction. Also his elder brother
has had an episode of coronary artery disease-myocardial
infarction at the age of 42 years. Although the patient himself
had no angina, chest pain, breathlessness, palpitation or
(B. Meghnathi).2013, Indraprastha Medic
edema to implicate any cardiac disease, he had never been
evaluated for possible cardiac ailment including ECG, 2D-
Echo, Serum lipid profile, etc.1
2. Discussion
The patient did not have any gross synovitis of hand joints or
knees, but there was a synovial thickening/tenosynovitis of
the right ankle. The patient also had multiple tendon
xanthomas over the MCP joints and elbows2 giving the
appearance of polyarthritis-synovitis (rheumatoid arthritis
mimic) to the casual observer. His evaluation at our center
revealed the possibility of a metabolic disorder and this was
confirmed by the presence of a severely deranged lipid pro-
file2 (Total cholesterol > 800) and a strong family history. The
absence of 1) polyarthritis, 2) raised inflammatory markers
(on repeat testing at our center) and 3) the Rheumatoid Fac-
tor, ANA confirmed the diagnosis in this patient. Based on
the clinical and laboratory findings, a diagnosis of Familial
hypercholesterolemia was made and the patient was treated
accordingly.
al Corporation Ltd. All rights reserved.
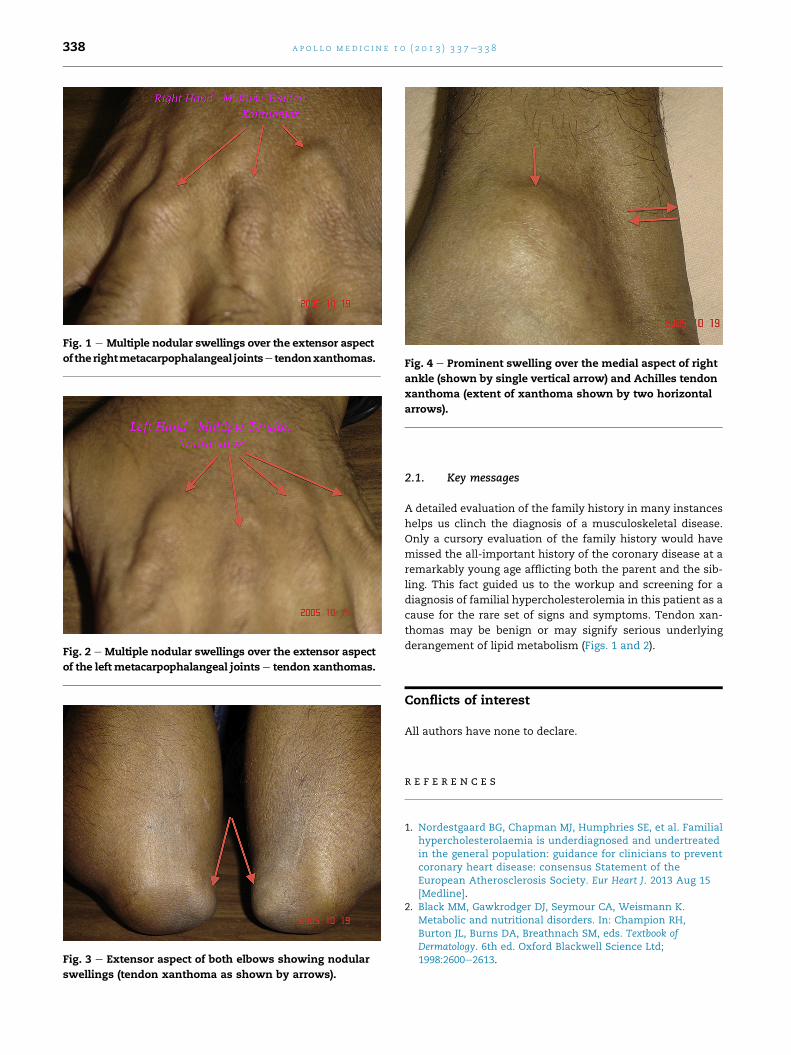
Fig. 1 e Multiple nodular swellings over the extensor aspect
of therightmetacarpophalangeal jointse tendonxanthomas.
Fig. 2 e Multiple nodular swellings over the extensor aspect
of the left metacarpophalangeal jointse tendon xanthomas.
Fig. 3 e Extensor aspect of both elbows showing nodular
swellings (tendon xanthoma as shown by arrows).
Fig. 4 e Prominent swelling over the medial aspect of right
ankle (shown by single vertical arrow) and Achilles tendon
xanthoma (extent of xanthoma shown by two horizontal
arrows).
a p o l l o m e d i c i n e 1 0 ( 2 0 1 3 ) 3 3 7e3 3 8338
2.1. Key messages
A detailed evaluation of the family history in many instances
helps us clinch the diagnosis of a musculoskeletal disease.
Only a cursory evaluation of the family history would have
missed the all-important history of the coronary disease at a
remarkably young age afflicting both the parent and the sib-
ling. This fact guided us to the workup and screening for a
diagnosis of familial hypercholesterolemia in this patient as a
cause for the rare set of signs and symptoms. Tendon xan-
thomas may be benign or may signify serious underlying
derangement of lipid metabolism (Figs. 1 and 2).
Conflicts of interest
All authors have none to declare.
r e f e r e n c e s
1. Nordestgaard BG, Chapman MJ, Humphries SE, et al. Familialhypercholesterolaemia is underdiagnosed and undertreatedin the general population: guidance for clinicians to preventcoronary heart disease: consensus Statement of theEuropean Atherosclerosis Society. Eur Heart J. 2013 Aug 15[Medline].
2. Black MM, Gawkrodger DJ, Seymour CA, Weismann K.Metabolic and nutritional disorders. In: Champion RH,Burton JL, Burns DA, Breathnach SM, eds. Textbook ofDermatology. 6th ed. Oxford Blackwell Science Ltd;1998:2600e2613.

Apollo hospitals: http://www.apollohospitals.com/Twitter: https://twitter.com/HospitalsApolloYoutube: http://www.youtube.com/apollohospitalsindiaFacebook: http://www.facebook.com/TheApolloHospitalsSlideshare: http://www.slideshare.net/Apollo_HospitalsLinkedin: http://www.linkedin.com/company/apollo-hospitalsBlog:Blog: http://www.letstalkhealth.in/


















