Radiotherapy Utilisation Rates - Girogiro-rt.org/.../2018/04/Radiotherapy-Utilisation-Rates.pdf ·...
33
Radiotherapy Utilisation Rates M Barton, G Delaney J Shafiq, S Jacob, S Thompson, K Wong T Hanna Funded by Department of Health and Ageing, Government of Australia
Transcript of Radiotherapy Utilisation Rates - Girogiro-rt.org/.../2018/04/Radiotherapy-Utilisation-Rates.pdf ·...

Radiotherapy Utilisation Rates
M Barton, G Delaney
J Shafiq, S Jacob, S Thompson, K Wong
T Hanna Funded by Department of Health and
Ageing, Government of Australia

Indications for radiotherapy
• Superior clinical outcome
– survival
– local control
– toxicity profile
• and the patient is suitable
– performance status
– co-morbidities.

Tree design
RT
Good PS
No RT
Poor PS
Localised disease
RT
symptoms for RT
Good PS
NO RT
Poor PS
Metastatic disease
Example cancer
• Type/site
• Stage
• Performance status
• Relapse

0.56
RT
Good PS (0.70)
No RT
Poor PS (0.30)
Localised disease (0.80)
0.06
RT
symptoms for RT (0.50)
Good PS (0.60)
NO RT
Poor PS (0.40)
Metastatic disease (0.20)
Example cancer

• 1000+ Pieces of evidence examined
• Constructed RTU trees on 23/23 cancers
• Comprises 98% of all cancer by incidence
• 52% of all cancers need RT
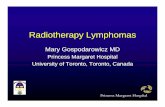
RTU 2003

Zimbabwe
Zambia
Yemen Vietnam
Venezuela
Uzbekistan
Uruguay
United States
United Kingdom
United Arab Emirates
Ukraine
Uganda
Turkey
Tunisia
Thailand
Tanzania
Tajikistan
Syria
Sudan
Sri Lanka
Spain
South Africa
Slovenia
Slovakia
Singapore
Sierra Leone
Serbia
Senegal
Saudi Arabia
Russia
Romania
Qatar
Portugal
Poland
Philippines
Peru
Paraguay
Panama
Pakistan
Nigeria
Niger
Nicaragua
Namibia
Myanmar
Morocco
MongoliaMoldova
Mexico
Mauritius
Malta
Mali
Malaysia
Malawi
Madagascar
Macedonia
Lithuania
Libya
Liberia
Lebanon
Latvia
Kyrgyzstan
Kuwait
Korea Rep.
Korea DPR
Kenya
Kazakhstan
Jordan
Japan
Jamaica
Ireland
Iraq
Indonesia
India
Iceland
Hungary
Honduras
Haiti
Guatemala
Greece
Ghana
Germany
Georgia
Gabon
France
Ethiopia
Estonia
EritreaEl Salvador
Egypt
Ecuador
Dominican Republic
Democratic Republic of the Congo
Czech Republic
Cyprus
Cuba
Croatia
Cote D'Ivoire
Costa Rica
China
Chile
Chad
Central African Republic
Cape Verde
Canada
Cameroon
Burkina Faso
Bulgaria
Brazil
Botswana
Bosnia and Herzegovina
Bolivia
Benin
Belarus
Bangladesh
Azerbaijan
Australia
Armenia
Argentina
Angola
Algeria
Albania
Afghanistan
% of cases requiring RT
0 - 0.39
0.39 - 0.43
0.43 - 0.47
0.47 - 0.51
0.51 - 0.55
0.55 - 0.59
0.59 - 1 N. Taylor, IAEA 2005

Other studies
Published
• Chemotherapy
• Brachytherapy
• Genetic services
• Screen-detected breast cancer
• Survival benefit breast
• Adaption to LMI countries
• Palliative RT
• Fractionation
On going
• Travel distance
• Survival and local control – RT
– Chemotherapy
• Integration with economics

Peer-reviewed publications 1. G Delaney, MB Barton, S Jacob, B Jalaludin. A model for decision making for the use of
radiotherapy in lung cancer. Lancet Oncology 2003; 4 : 120 – 128 2. G Delaney, MB Barton. S Jacob. Estimation of an optimal radiotherapy utilization rate for breast
cancer: A review of the evidence. Cancer 2003 Oct; 98;1977-1986. 3. MB Barton, S Jacob, V Gebski. Utility-adjusted analysis of the cost of palliative radiotherapy for
bone metastasis. Australas Radiol. 2003 Sep;47(3):274-8. 4. G Delaney, MB Barton. S Jacob. Estimation of an optimal radiotherapy utilization rate for
melanoma: A review of the evidence. Cancer. 2004 Mar 15;100(6):1293-301. 5. G Delaney, MB Barton. S Jacob. Estimation of an optimal radiotherapy utilization rate for
gynaecological cancers Part I: Malignancies of the Cervix, Ovary, Vagina, and Vulva. A review of the evidence. Cancer. 2004;101:671–81
6. G Delaney, S Jacob, MB Barton. Estimation of an optimal radiotherapy utilization rate for gynaecological cancers Part II: Carcinoma of the endometrium. A review of the evidence. Cancer. 2004;101:682–92
7. G Delaney, S Jacob, MB Barton. Estimation of an optimal radiotherapy utilization rate for gastro-intestinal cancers: A review of the evidence. Cancer. 2004;101:657–70
8. C Featherstone. G Delaney, S Jacob, MB Barton. Estimation of an optimal radiotherapy utilization rate for haematological malignancies (Part I): A review of the evidence. Cancer 2005 Jan 15; 103(2):383-92.
9. C Featherstone. G Delaney, S Jacob, MB Barton. Estimation of an optimal radiotherapy utilization rate for haematological malignancies (Part II): A review of the evidence. Cancer 2005 Jan 15;103(2):393-401.
10. G Delaney, S Jacob, MB Barton. Estimating the optimal external-beam radiotherapy utilization rate for genito-urinary cancers: A review of the evidence. Cancer. 2005 Feb 1;103(3):462-473
11. G Delaney, S Jacob, MB Barton. Estimating the optimal external-beam radiotherapy utilization rate for head and neck cancers: A review of the evidence. Cancer. 2005 Jun 1;103(11):2216-27.
12. G Delaney, S Jacob, C Featherstone and MB Barton. The Role of Radiotherapy in the Treatment of Cancer: Estimating the optimal utilization from a review of evidence-based clinical guidelines. Cancer 2005 Sep 15; 104(6): 1129-37
13. G Delaney, S Jacob, MB Barton. Estimating the optimal radiotherapy utilization for cancer of the central nervous system, thyroid cancer and cancer of unknown primary origin from evidence-based clinical guidelines. Cancer 2006 Jan 15;106(2):453-65.
14. MB Barton, M Frommer, RJ Shafiq. The role of radiotherapy in cancer control in low and middle income countries. Lancet Oncology 2006, 7 (7): 584-595.
15. Jacob S, Ng W, Delaney GP, Barton MB. Estimation of an optimal chemotherapy utilisation rate for primary malignant brain tumours: an evidence-based benchmark for cancer care. Clin Oncol (R Coll Radiol). 2011 Feb;23(1):48-54. S Vinod, MB Barton. Actual versus optimal utilisation of radiotherapy in lung cancer – Where is the shortfall? Asia Pacific Journal of Clinical Oncology.2007; 3: 1- 7.
17. C Featherstone, A Colley, K Tucker, J Kirk, MB Barton. Estimating the referral rate for cancer genetic assessment from a systematic review of the evidence. Br. J. Cancer 2007: 96:391-398.
18. J Shafiq, GP Delaney, MB Barton. An evidence-based estimation of local control and survival benefit of radiotherapy for breast cancer. Radiother Oncol. 2007 Jul;84(1):11-7.
16. 19. F Hegi-Johnson, GS Gabriel, A Kneebone, S.K C Wong, B Jalaludin, S Behan, and MB Barton. Utilisation of Radiotherapy for Rectal Cancer in Greater Western Sydney 1994-2001. ANZ J Surg. 2007;3:134-142
20. M Alam, G Gabriel, M Barton, R Eek. Discriminating factors in treatment decisions for chemotherapy in elderly patients with colorectal cancer. Cancer Forum, 2008, 32 (1): 22-26.
21. G Delaney, J Shafiq, G Chappell and M Barton. Establishing treatment benchmarks for mammography-screened breast cancer population based on a review of evidence-based clinical guidelines. Cancer. 2008 May 1;112(9):1912-22
22. S Thompson, G Delaney, GS Gabriel, S Jacob, P Das, MB Barton. Estimation of the Optimal Brachytherapy Utilization Rate in the Treatment of Malignancies of the Uterine Corpus by a Review of Clinical Practice Guidelines and Primary Evidence. Int. J. Radiation Oncology Biol. Phys., Vol. 72, No. 3, pp. 849–858, 2008.
23. S Jacob, W Ng, R Ashgari, G Delaney, M Barton. Estimation of an optimal chemotherapy utilisation rate for colon cancer: an evidence-based benchmark for cancer care. Eur J Cancer 45 (2009) 2503 - 2509.
24. W Ng, S Jacob, G Delaney, M Barton. Estimation of an optimal chemotherapy utilisation rate for head and neck carcinoma: setting an evidence-based benchmark for the best-quality cancer care. Eur. J Cancer 2009 Aug;45(12):2150-9
25. S Jacob, K Wong, P Adams, GP Delaney, MB Barton. Estimation of an Optimal Utilisation Rate for Palliative Radiotherapy in Newly Diagnosed Cancer Patients. Clinical Oncology 22 (2010) 56–64.
26. W Ng, G Delaney, S Jacob, M Barton. Estimation of an optimal chemotherapy utilisation rate for breast cancer: Setting an evidence-based benchmark for the best-quality cancer care. Eur J Cancer. (2010) Mar;46(4):703-12.
27. S Jacob, E Hovey, W Ng, S Vinod, GP Delaney and MB Barton. Estimation of an optimal chemotherapy utilisation rate for lung cancer: An evidence-based benchmark for cancer care. Lung Cancer 69 (2010) 307–314.
28. A Fong, W Ng, MB Barton, G Delaney. Estimation of an evidence-based benchmark for the optimal endocrine therapy utilization rate in breast cancer. Breast. 2010 Oct; 19(5):345-9.
29. Jacob S, Ng W, Delaney GP, Barton MB. Estimation of an optimal chemotherapy utilisation rate for primary malignant brain tumours: an evidence-based benchmark for cancer care. Clin Oncol (R Coll Radiol). 2011 Feb;23(1):48-54.
30. MB Barton, GP Delaney. A decade of investment in radiotherapy in NSW; why does the gap between optimal and actual service delivery persist? Journal of Medical Imaging and Radiation Oncology 55 (2011) 433–441
31. PL Blinman, P Grimison, MB Barton, S Crossing, E Walpole, N Wong, K Francis, B Koczwara. The shortage of medical oncologists in Australia: the Australian Medical Oncology Workforce Study. MJA 2012; 196: 58–61
32. Thompson SR, Delaney GP, Gabriel GS, Jacob S, Barton MB. Estimation of the optimal brachytherapy utilisation rate in the treatment of vaginal cancer and comparison with patterns of care. J Med Imaging Radiat Oncol. 2012 Aug;56(4):483-9.
33. A Fong, J Shafiq, C Saunders, A Thompson, S Tyldesley, IA Olivotto, MB Barton, JA Dewar, S Jacob, W Ng, C Speers. A comparison of systemic breast cancer therapy utilization in British Columbia, Scotland, and Western Australia with models of “optimal” therapy. The Breast 2012 Aug;21(4):562-9.
34. Fong A, Shafiq J, Saunders C, Thompson AM, Tyldesley S, Olivotto IA, Barton MB, Dewar JA, Jacob S, Ng W, Speers C, Delaney GP. A comparison of surgical and radiotherapy breast cancer therapy utilization in Canada (British Columbia), Scotland (Dundee), and Australia (Western Australia) with models of "optimal" therapy. Breast. 2012 Aug;21(4):570-7.
35. S Thompson, GP Delaney, GS Gabriel, S Jacob, P Das and MB Barton. Estimation of the Optimal Brachytherapy Utilization Rate in the Treatment of Gynaecological Cancers and Comparison with Patterns of Care. Int J Radiation Oncol Biol Phys, Vol. 85, No. 2, pp. 400-405, 2013

RTU revision 2012
• External beam radiotherapy
• Synchronous chemotherapy
• Brachytherapy
• Patient preference

RTU revision 2012 Site Old RTU New RTU Changed indications
Bladder 58% 47% 0
Brain 92% 80% Tree changed
Breast 83% 87% 0
Cervix 58% 71% Tree changed
Colon 14% 4% -1
Gall bladder 13% 17% 0
Head and Neck 74% 74% Tree changed
Kidney 28% 15% -1
Leukaemia 4% 4% 0
Liver 0% 0% N/A
Lung 76% 77% 0
Lymphoma 65% 73% 4
Melanoma 23% 21% 3
Myeloma 38% 45% 3

Site Old RTU New RTU Changed indications
Oesophagus 80% 71% 1
Other 50% 19% Tree changed
Ovary 4% 4% 0
Pancreas 57% 49% Tree changed
Prostate 60% 58% Tree changed
Rectum 65% 60% 0
Stomach 68% 27% 1
Testis 49% 7% Tree changed
Thyroid 10% 4% Tree changed
Unknown Primary 61% 61% 0
Uterus 46% 38% Tree changed
Vagina 100% 94% Tree changed
Vulva 34% 39% Tree changed
TOTAL 52.3% 48.3%

Indications
Added • Lymphoma
• Melanoma
• Myeloma
• Oesophagus
• Stomach
Removed • Colon
• Kidney

Radiotherapy utilisation rates
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Old RTU New RTU

Absolute Percent Change to RTU for all Cancers by Site
2012 versus 2003 Model
-5% -4% -3% -2% -1% 0% 1% 2% 3% 4% 5%
TOTAL (all cancer)
Unknown Primary
Colon
Stomach
Bladder
Rectum
Brain
Lung
Head and Neck
Kidney
Melanoma
Testis
Breast
Uterus
Pancreas
Other
Gall bladder
Thyroid
Leukaemia
Ovary
Vagina
Liver
Vulva
Oesophagus
Cervix
Myeloma
Lymphoma
Prostate
Only change in AIHW data AIHW changes plus other changes

Synchronous Chemoradiotherapy
Tumour Site
Proportion of Notifiable Cancers
Optimal CT-RT Utilization Rate
Proportion of cancers with CT-RT indication
Bladder 2.0% 9% 0.2%
Brain 1.4% 53% 0.7%
Cervix 1.0% 51% 0.5%
Gall bladder 0.6% 17% 0.1%
Head and Neck 3.3% 26% 0.8%
Lung 9.0% 26% 2.3%
Oesophagus 1.2% 33% 0.4%
Pancreas 2.1% 35% 0.7%
Rectum 4.2% 55% 1.9%
Stomach 1.8% 20% 0.3%
Vagina 0.1% 78% 0.08%
Other 5.0% 5% 0.3%
Total 31.7% 28% 8.9%

Optimal Brachytherapy Utilization
Tumour Site Proportion of Notifiable Cancers %
Optimal BT Utilization
Rate %
Optimal BT Utilization Rate for all Cancers %
Cervix 1 53 0.5
Melanoma 10 2 0.2
Prostate 18 10 1.8
Uterine Corpus 2 39 0.7
Vagina 0.1 85 0.1
Total 31 11% 3.3%
Stephen Thompson

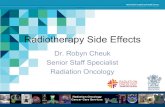
Sensitivity analysis
• Univaritate
– 150 variables
• Multivariate
– Monte Carlo simulation
Utilisation rate Range
RT 48.3% 47.9% 48.7%
CT RT 8.9% 8.5% 9.3%
Brachytherapy 3.3% 3.0% 3.3%
Tornado Diagram at
Cancer
Expected Value
0.48 0.48 0.48 0.48 0.48 0.48 0.48 0.48 0.49 0.49 0.49 0.49 0.49 0.49 0.49 0.49 0.49 0.50 0.50 0.50
pPref er_EBRTv sRP: 0.25 to 0.75
pPref er_RTv sRP: 0.25 to 0.75
pPref er_BTv sEBRT: 0.25 to 0.75
p_stomach_adjCRT_indicated: 0. to 1.
p_my eloma_bonepain_bispohphonate: 0.11 to 0.42
p_kidney _distant_mets: 0.23 to 0.58
pSBTM_indicatedGoodIR: 0. to 1.
p_pancreas_stageI_II_inop_CRT: 0. to 1.
p_unknown_primary_node_mets: 0.37 to 0.52
p_breast_stageI_II_1_3nodes: 0. to 1.
p_unknown_primary_bone_mets: 0.17 to 0.33
p_pancreas_adjuv ant_radiotherapy : 0. to 1.
p_colon_M1_unresectable: 0. to 0.11
p_gallbladder_unresectable_RT: 0. to 1.
p_melanoma_node_brain_bone_mets: 0.21 to 0.50
p_oesophagus_preop_RT: 0. to 1.
p_pancreas_stageIII_y oung: 0. to 1.
p_lip_adverse_f eatures: 0.07 to 0.34
p_v ulv al_stageI_II_no_surgery _CRT: 0. to 1.
Proportion of stage IV bladder cancer with bone metastases: 0.17 to 0.43
p_melanoma_RT_large_node: 0. to 1.
Proportion of patients getting surgery f or Stage II-III bladder cancer: 0.30 to 0.60
pLRDx_BT_Phy sically CI: 0.33 to 0.62
p_seminoma_st_I_radiotherapy : 0. to 0.445
p_melanoma_RT_ENS: 0. to 1.
p_lip_surgery : 0.81 to 0.99
pBone_metsbreast: 0.42 to 0.71
p_oroph_HPVpositiv eRRT: 0.24 to 0.84
p_ov arian_stageIV_metastasis: 0.12 to 0.18
p_unknown_primary_brain_mets: 0.03 to 0.09
p_lary nx_laser: 0. to 0.23
p_NSCLC_early __distant_relapse: 0.16 to 0.34
p_oesophagus_neoadjuv ant: 0.31 to 0.76
pSurgery ForStageI_VaginalCancer: 0.11 to 0.32
p_colon_T4_RT: 0. to 0.055
p_NHL_low_grade_CR: 0.38 to 0.66
p_oroph_HPVnegativ eRRT: 0.24 to 0.84
Proportion of stage IV bladder cancer with brain metastases: 0.01 to 0.12
p_NSCLC_lr_stageIIIa_updated: 0.09 to 0.38
p_oral_cav ity _surgery _StI_II: 0.76 to 0.90
p_cerv ix_Medically Inoperable: 0.04 to 0.19
p_NSCLC_surgery_margins_updated: 0.01 to 0.05
p_relapse_ALL_child: 0.12 to 0.46
p_gallbladder_resectable: 0.45 to 0.59
p_oral_cav ity _III_IVB_no_adjuv RT: 0. to 0.08
p_kidney _M1_sy mptomatic_primary : 0. to 0.06
p_thy roid_papillary_distant_recur: 0.04 to 0.11
p_oesophagus_bone_mets: 0.16 to 0.33
VRwithoutDM: 0. to 0.29
p_SCLC_brain_mets: 0.16 to 0.26
p_gallbladder_metastatic: 0.38 to 0.47
pSurgery ForStageII_VaginalCancer: 0.07 to 0.20
p_v ulv al_stageIII_IVA_no_surgery _CRT: 0. to 1.
p_NSCLC_StageIIIA_distant: 0.32 to 0.59
p_oesophagus_resectable: 0.53 to 0.80
p_cerv ix_LN: 0.73 to 0.80
p_adult_AML_complete_remission: 0.55 to 0.75
p_AML_adult_relapse: 0.43 to 0.60
p_v ulv al_local_recurrence: 0.15 to 0.33
p_v ulv al_node_positiv e: 0.57 to 0.76
p_v ulv al_recurrent_RT: 0.23 to 0.38
p_oesophagus_lc: 0.21 to 0.68
p_lary nx_sg_conserv ativ e_surgery : 0. to 0.23
p_CNS_ALL_child: 0.03 to 0.07
p_thy roid_papillary_bone_mets: 0.19 to 0.30
p_headandneck_N1_2a_disease: 0.09 to 0.22
p_adult_ALL_complete_remission: 0.78 to 0.93
p_NHL_low_MALT_CR_to_HP: 0.56 to 0.81
p_thy roid_papill_local_recur: 0.03 to 0.15
p_oesophagus_postop_recurrence: 0.40 to 0.50
p_seminoma_st_III_resid_disease: 0. to 0.15
p_oroph_HPVpositiv e: 0.66 to 0.80
p_testicular_ca_brain_mets_RT: 0. to 1.
p_seminoma_st_II_resid_disease: 0. to 0.07
pIRDx_BT_Phy sically CI: 0.20 to 0.52
pHRDx_BT_Phy sically CI: 0.29 to 0.61
p_rectum_resectable_CRTindicated: 0. to 1.
p_oesoph_distant_mets: 0.18 to 0.30
p_melanoma_node_positiv e: 0.22 to 0.55
p_melanoma_H_N: 0.16 to 0.20
p_unknown_primary_CRT: 0. to 1.
p_paranasal_operableRRT: 0. to 0.62
p_oroph_HPVpositiv e_adjRT: 0.31 to 0.36
p_oroph_HPVnegativ e_adjRT: 0.56 to 0.63
p_hy pophary nx_CRTrate: 0.50 to 0.81
p_cerv ix_Margin: 0.10 to 0.60
p_breast_v ary _node_inv olv ement: 0.18 to 0.34

Factors that affect Patient choice
• Treatment
– Benefits, toxicity, previous experience
• Socio-demographic
– Age, sex, marriage, dependents
• Clinical
– Type, stage, LN, recurrence
• Methodology
– Framing, order of questions, starting point
• Time
• Cognitive/affective
– Belief in tmt benefits, need to act, regret
• Provider

Actual utilisation
Journal of Medical Imaging and Radiation Oncology 55 (2011) 433–441

Actual utilisation
Raw data RT 34,442
32% New cancers 108,064
Data linkage 2004 -2006
RT 25,917 24%
New cancers 108,064
Data Linkage + GIS
RT 24,952 26%
New cancers 96,803
NSW
ACT
QLD
SA
NSW
VIC
ACT
• NSW 2004 - 2006 • Optimal RTU at
diagnosis = 44%

21
P < 0.001
0%
5%
10%
15%
20%
25%
30%
0- km 50- km 75- km 100-km
125-km
150-km
200-km
250-km
300-km
350-km
400+km
Effect of travel distance on RTU in NSW & ACT (2004-06)
P<0.001

Appropriateness
-2000 -1000 0 1000 2000 3000 4000
Radiotherapy
Chemotherapy
Hormone therapy
Screen-detected breast cancer
Recommended &received
Not recommended ¬ received
Not recommended butreceived
Recommended butnot received
CANCER May 1, 2008, 112 (9): 1912 - 1922

Conclusions
Optimal utilisation
• 48.3% RT
• 8.9% CTRT
• 3.3% BT
Actual utilisation
• Discrepancies between methods
• Appropriateness

Estimating cost and benefit Melanoma
Mucosal
0.0100.01 0.0083
Ocular
0.0200.02
Surgery
0.9300.07
No surgery /inadequate m argin
0.0700.01 0.0980
Lentigo Maligna Melanom a
0.0800.069 / 0.7
Desm oplastic
0.0200.02 0.0455
No recurrence
0.9800.44
Nodal recurrence
0.9000.01 0.0000
Brain mets
0.0800.00 0.0000
Bone m ets
0.0200.00 0.0000
Nodal/brain/bone recurrence
0.0200.000 / 18.4
Stage I
0.5600.000 / 0.4
Nodal recurrence
0.9000.00 0.0000
Brain mets
0.0800.00 0.0000
Bone m ets
0.0200.00 0.0000
Nodal/ brain/ bone recurrence
0.2500.000 / 18.4
No bone/ brain/ nodal recurrence
0.7500.01
No ENS
0.5000.000 / 4.6
Extra-nodal spread (ENS)
0.5000.01 0.0070
Node size <=4cm
0.6100.070 / 12.3
Node size >4cm
0.3900.01 0.0070
Single node involved
0.4500.097 / 15.3
Multiple nodes involved
0.5500.05 0.0070
Node positive
0.2400.121 / 17.9
No recurrence
0.9200.04
Nodal recurrence
0.9000.00 0.0000
Brain mets
0.0800.00 0.0000
Bone m ets
0.0200.00 0.0000
Nodal/ brain/ bone recurrence
0.5100.000 / 18.4
No bone/ brain/ nodal recurrence
0.4900.00
Nodal /sy stemic recurrence
0.0800.000 / 9.4
pT1-3
0.8400.000 / 0.8
pT4
0.1600.01 0.0090
Head and neck
0.2100.029 / 3.8
No recurrence
0.8000.17
Nodal recurrence
0.9000.04 0.0000
Brain mets
0.0800.00 0.0000
Bone m ets
0.0200.00 0.0000
Nodal/brain/bone recurrence
0.2000.000 / 18.4
Non head and neck
0.7900.000 / 3.7
Node negative
0.7600.006 / 3.7
Stage II-III
0.4400.034 / 7.1
Non desm oplastic
0.9800.015 / 3.3
Stage I-III
0.8500.033 / 3.7
Nodal recurrence
0.9000.03 0.0000
Brain mets
0.0800.00 0.0000
Bone m ets
0.0200.00 0.0000
Sy mptomatic brain/bone/node metastases
0.5100.000 / 13.9
No sy mptom atic brain/bone/node m etastases
0.4900.03
Stage IV
0.0700.000 / 7.1
Cutaneous
0.9700.033 / 3.7
Melanom a 0.035 / 3.9
Total Proportion 5-yr benefi t proportion

Indication Number of Fractions
Local control
Local control/fractions
Proportion of all cases
Mucosal Melanoma
30 25% 0.83% 1%
Lentigo 10 98% 9.8% 1%
Desmoplastic 20 91% 4.55 2%
LN +ve 20 14% 0.7% 7%
H&N pT4 20 18% 0.9% 1%
All cases 3.9 3.5% 0.90% 100%
Estimating cost and benefit Melanoma

GTFRCC

Adapting model to other jurisdictiosn
• Cancer data
• Stage data
• Available models
– RTU
– Survival
• Cost data

Effect of tumour distribution
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
East
Africa
Central
Africa
Northern
Africa
Southern
Africa
Western
Africa
all Africa
Liver
Ovary etc.
Leukaemia
Thyroid
Testis
Multiple myeloma
Melanoma of skin
Kidney etc.
Corpus uteri
Other Pharynx
Pancreas
Hodgkin's disease
Colon/Rectum
Brain, nervous system
Nasopharynx
Larynx
Oral cavity
Lung
Stomach
Bladder
Non-Hodgkin lymphoma
Oesophagus
Prostate
Cervix uteri
Breast
0%
10%
20%
30%
40%
50%
60%
70%
Central Africa WesternAfrica
East Africa SouthernAfrica
NorthernAfrica
RTU

Globocan data sources
High quality national or
regional (coverage >50%)
7%
High quality regional
(coverage 10% to 50%) 11% High quality
regional (coverage <10%)
42%
National data 5%
Regional data 16%
Frequency data 8%
No data 11%

Data quality and GNI/person
$0
$5,000
$10,000
$15,000
$20,000
$25,000
$30,000
$35,000
$40,000
A B C D E F G
Ave
rage
GN
I/p
ers
on
Data Quality
A. High quality national or
regional (coverage
>50%) 7%
B. High quality regional
(coverage 10% to 50%)
11%
C. High quality regional
(coverage <10%) 42%
D. National data 5%
E. Regional data 16%
F. Frequency data 8%
G. No data 11%

Top 10 cancers
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
Pro
po
rtio
n o
f al
l can
cers
Less developed
Medium development
High development
Very High development

Individual country variation
0%
5%
10%
15%
20%
25%
30%
35%
Swit
zerl
and
New
Zea
lan
d
Egyp
t
Au
stri
a
Luxe
mb
ou
rg
Gre
ece
Spai
n
Sau
di A
rab
ia
Ko
rea,
Rep
ub
lic o
f
Cze
ch R
epu
blic
Pu
erto
Ric
o
Arm
enia
No
rth
ern
Afr
ica
Po
lyn
esia
Cu
ba
Geo
rgia
Bo
snia
He
rzeg
ovi
na
Aze
rbai
jan
Asi
a
Tim
or-
Lest
e
Turk
men
ista
n
Mal
div
es
Trin
idad
an
d T
ob
ago
Ph
ilip
pin
es
Uzb
eki
stan
El S
alva
do
r
Nam
ibia
Ch
ad
Kyr
gyzs
tan
Eth
iop
ia
Me
lan
esia
Som
alia
Uga
nd
a
Fiji
Be
nin
Rw
and
a
Lib
eria
Mal
i
Tan
zan
ia
Swaz
ilan
d
Pro
po
rtio
n o
f al
l can
cers
Cervix

Available models
RTU Stage data Survival model
Lung 77% y y Breast 87% y y Stomach 27% y y Liver 0% n/a y Colorectum 22% ? y Haematology 40% Y y Cervix uteri 71% y y Oesophagus 71% y Head and Neck 74% y y Prostate 58% y n