
Radiology signs
56
Aunt Minnie signs Aunt Minnie signs Dr Nitin Jain Dr Nitin Jain Senior Resident Senior Resident PGIMS PGIMS Rohtak Rohtak
-
Upload
nitin-jain -
Category
Health & Medicine
-
view
1.282 -
download
6
Transcript of Radiology signs
Aunt Minnie signsAunt Minnie signs
Dr Nitin JainDr Nitin JainSenior ResidentSenior Resident
PGIMSPGIMSRohtakRohtak
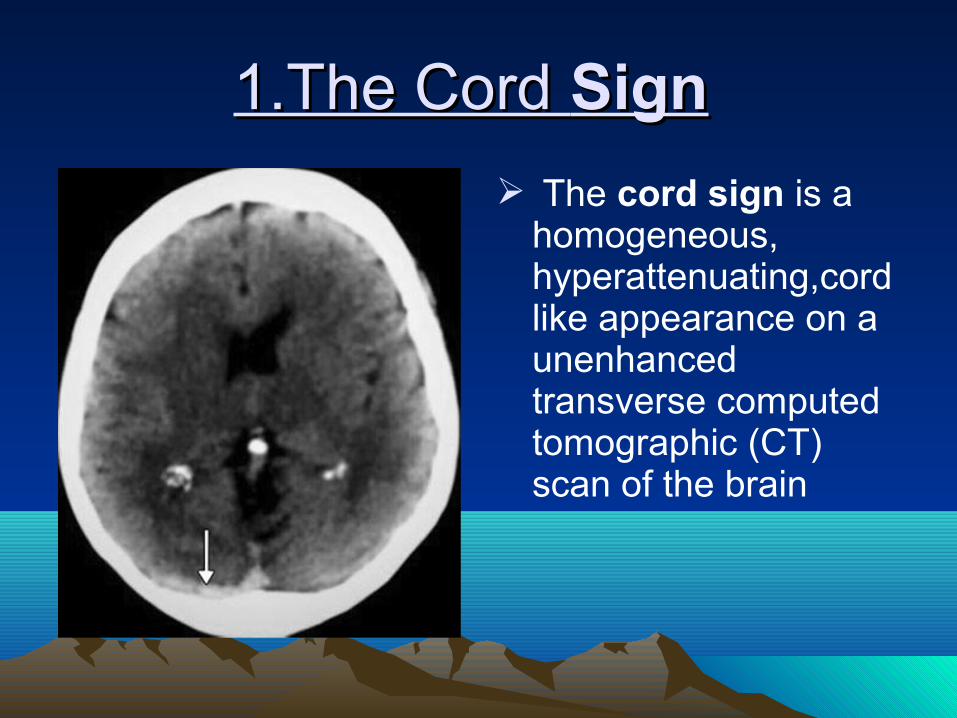
1.The Cord 1.The Cord SignSign
The cord sign is a homogeneous, hyperattenuating,cordlike appearance on a unenhanced transverse computed tomographic (CT) scan of the brain
The cord sign is one of the important clues in the diagnosis of CVTCVT on an unenhanced CT scan.
The cord sign demonstrates a newly formed thrombus.
Appearance of a strongly hyperintense triangle in the area of the sinus on nonenhanced CT images (dense triangle sign).
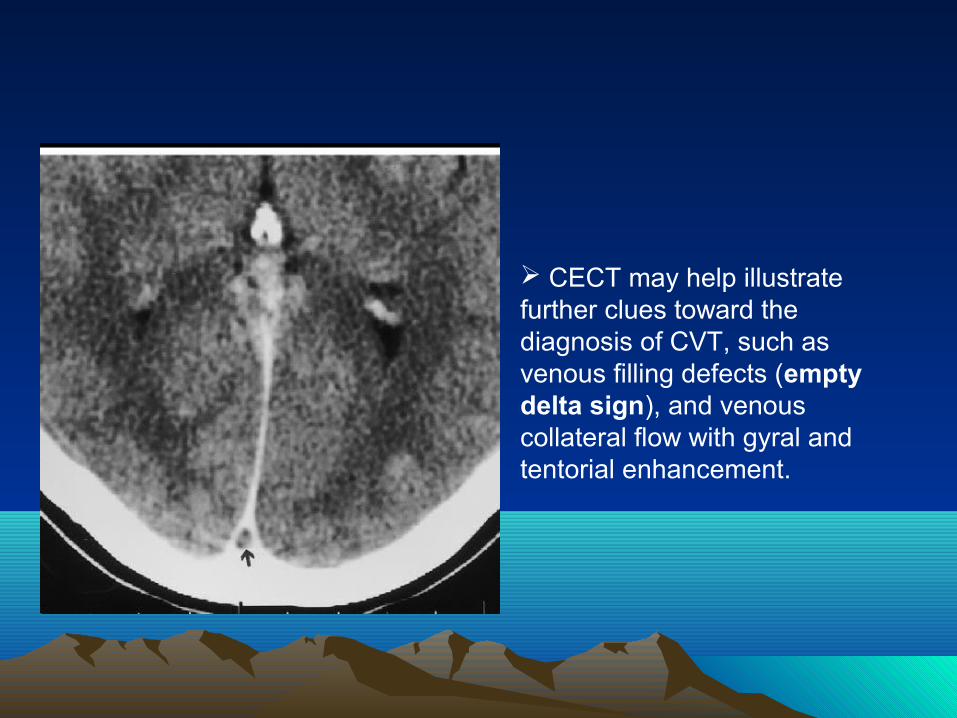
CECT may help illustrate further clues toward the diagnosis of CVT, such as venous filling defects (empty delta sign), and venous collateral flow with gyral and tentorial enhancement.

2.The Fat Halo Sign
The fat halo sign is seen on CT scans of the abdomen and appears as a thickened bowel wall demonstrating three layers: an inner and an outer layer of soft-tissue attenuation, between which lies a third layer of fatty attenuation.
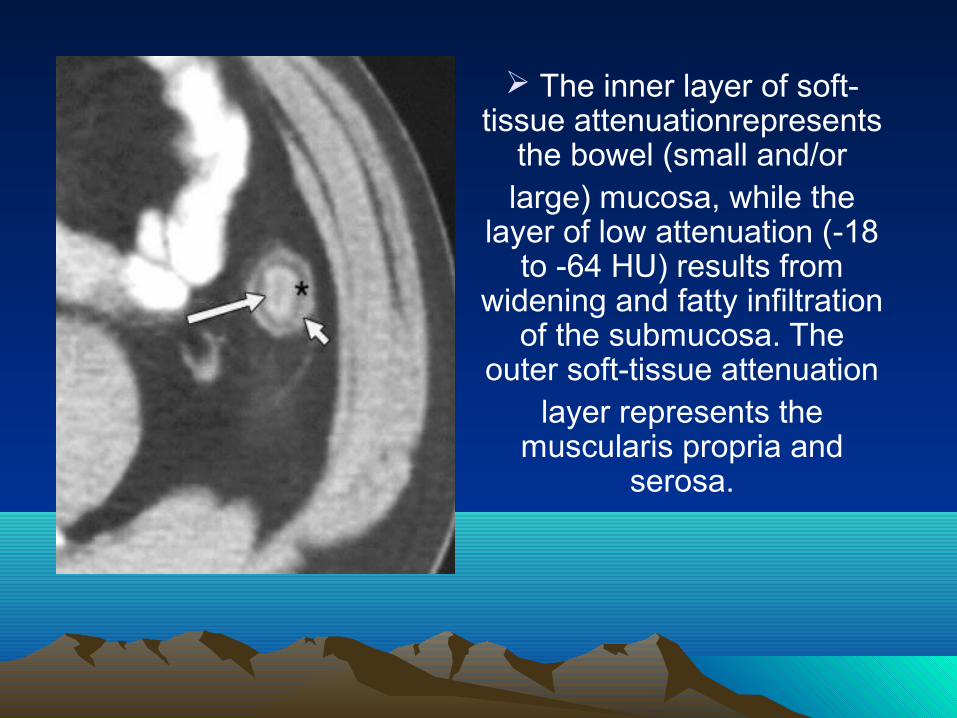
The inner layer of soft-tissue attenuationrepresents
the bowel (small and/orlarge) mucosa, while the
layer of low attenuation (-18 to -64 HU) results from
widening and fatty infiltration of the submucosa. The
outer soft-tissue attenuationlayer represents the
muscularis propria and serosa.
The fat halo sign is seen in various diseases of the bowel in which fatty infiltration of the submucosa is present . The sign has been described as typically appearing in patients with chronic inflammatory bowel disease (Crohn disease and ulcerative colitis).
3.The Cupola Sign
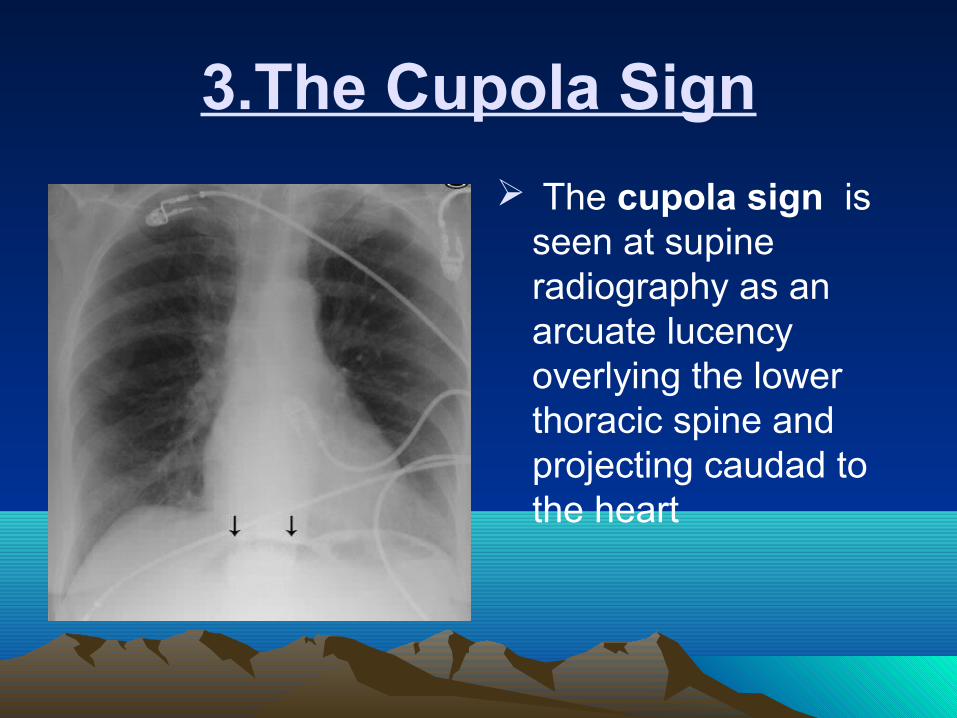
The cupola sign is seen at supine radiography as an arcuate lucency overlying the lower thoracic spine and projecting caudad to the heart

When the patient is in the supine position,air within the peritoneal cavity (pneumoperitoneum) will preferentially accumulate in the anterior portion of the cavity, beneath the central tendon of the diaphragm and within the median subphrenic space
4.The Split Pleura Sign
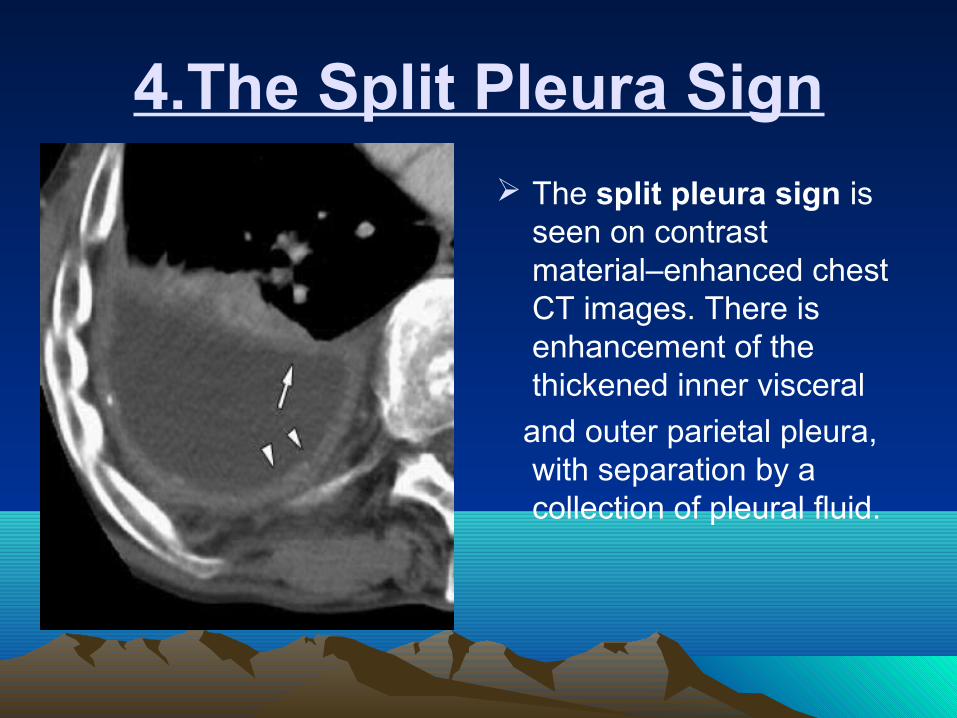
The split pleura sign is seen on contrast material–enhanced chest CT images. There is enhancement of the thickened inner visceral
and outer parietal pleura, with separation by a collection of pleural fluid.
The split pleura sign refers to thickening and increased contrast enhancement of the visceral and the parietal pleura separated by empyema or an exudative effusion.

5.The Reversal Sign
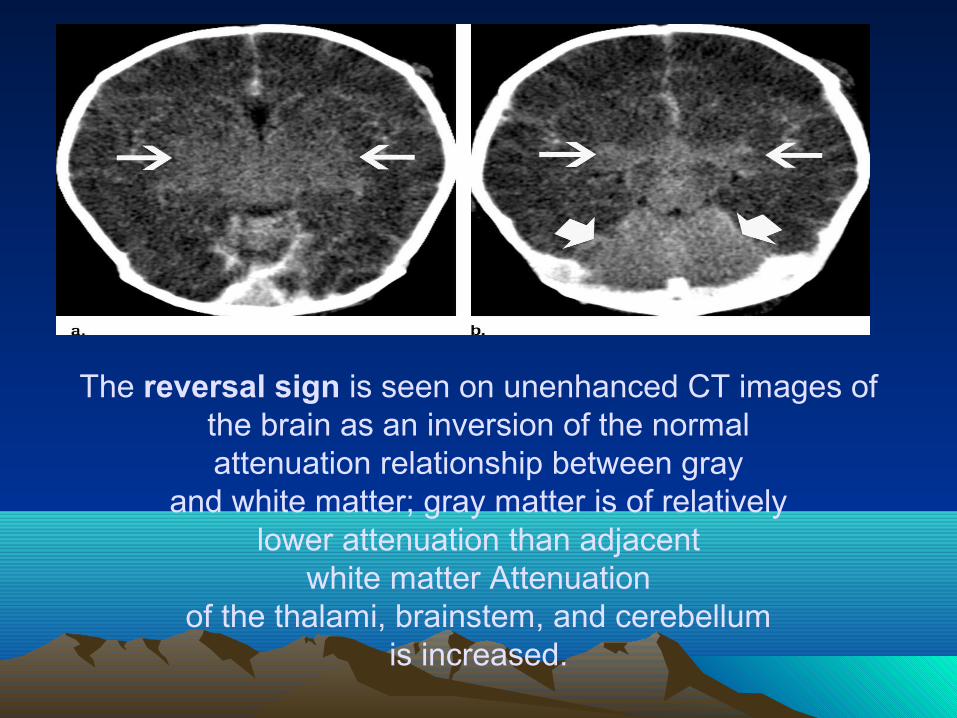
The reversal sign is seen on unenhanced CT images ofthe brain as an inversion of the normalattenuation relationship between gray
and white matter; gray matter is of relativelylower attenuation than adjacent
white matter Attenuationof the thalami, brainstem, and cerebellum
is increased.
The reversal sign indicates diffuse cerebral injury in a patient who has suffered an anoxic insult
Causes of the reversal sign include head trauma, hypoxia, birth asphyxia, drowning, status epilepticus, hypothermia, bacterial meningitis, strangulation, nonaccidental trauma, and other causes of global cerebral ischemia
Pathogenesis of the reversal sign is complex and not yet fully understood
The reversal sign is associated with a poor prognosis and indicates irreversible brain damage
6.The Polka-Dot Sign
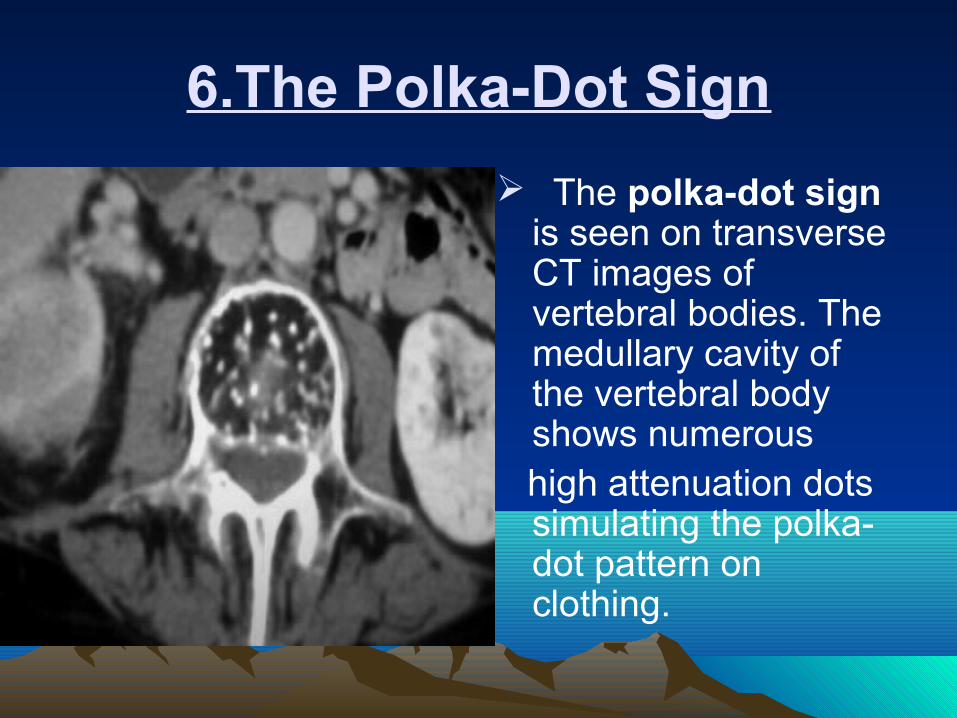
The polka-dot sign is seen on transverse CT images of vertebral bodies. The medullary cavity of the vertebral body shows numerous
high attenuation dots simulating the polka-dot pattern on clothing.
The polka-dot sign on CT images is produced by thickened trabeculae in a vertebral body hemangioma, seen in cross section as small punctate areas of high attenuation
The trabecular thickening occurs due to reinforcement of the osseousnetwork adjacent to the vascular channels of the lesion that have causedbone resorption. This process occurs within the fatty marrow
D/D-chondrosarcoma and intraosseousmeningioma
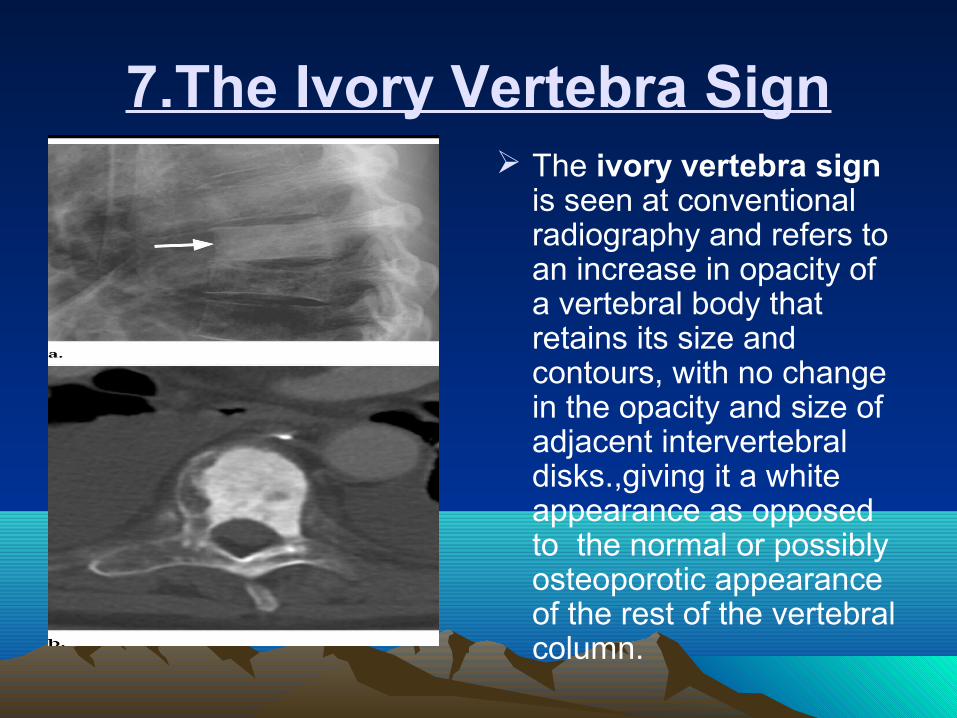
7.The Ivory Vertebra Sign The ivory vertebra sign
is seen at conventional radiography and refers to an increase in opacity of a vertebral body that retains its size and contours, with no change in the opacity and size of adjacent intervertebral disks.,giving it a white appearance as opposed to the normal or possibly osteoporotic appearance of the rest of the vertebral column.
The ivory vertebra sign can be seen in both adults and children.
In children, typically the result of lymphoma, usually Hodgkin lymphoma
In adults, the ivory vertebra sign has been associated with metastatic disease, especially carcinoma of the prostate or breast, and occasionally with osteosarcoma, carcinoid, Paget disease, and lymphoma, particularly Hodgkin lymphoma.
Paget disease can give the appearance of an ivory vertebral body, but, more often, the disease is characterized by the “picture frame” vertebral body
Lymphoma is particularly characteristic when there is an accompanying paraspinal soft-tissue mass.
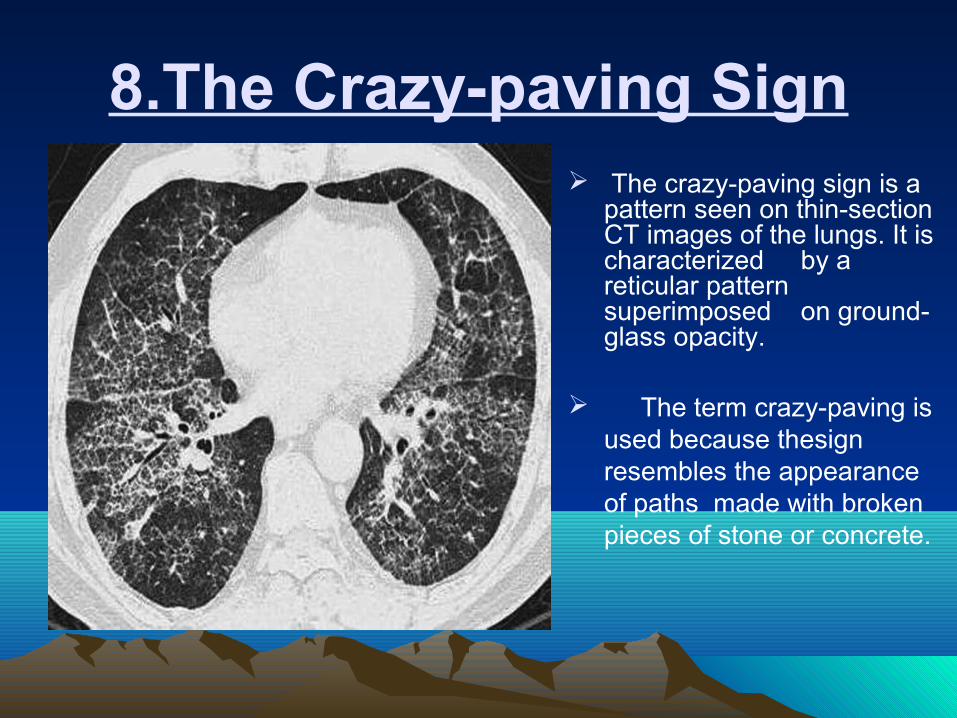
8.The Crazy-paving Sign The crazy-paving sign is a
pattern seen on thin-section CT images of the lungs. It is characterized by a reticular pattern superimposed on ground-glass opacity.
The term crazy-paving is used because thesign resembles the appearance of paths made with broken pieces of stone or concrete.

In the crazy-paving sign, ground-glass opacity may reflect the presence of airspace or interstitial abnormalities.
The lines of reticular opacities may represent interlobular septal thickening, thickening of the intralobular interstitium.
The crazy-paving sign was initially recognized in patients who had pulmonary alveolar proteinosis.
The differential diagnosis of crazy-paving sign includes Pneumocystis carinii pneumonia, mucinous bronchioloalveolar carcinoma , sarcoidosis, lipoid pneumonia , adult respiratory distress syndrome , and pulmonary hemorrhage syndromes.
The highest prevalence of crazy-paving sign in this study was seen in pulmonary alveolar proteinosis (100%), diffuse alveolar damage (67%), acute interstitial pneumonia (31%), and adult respiratory distress syndrome (21%).
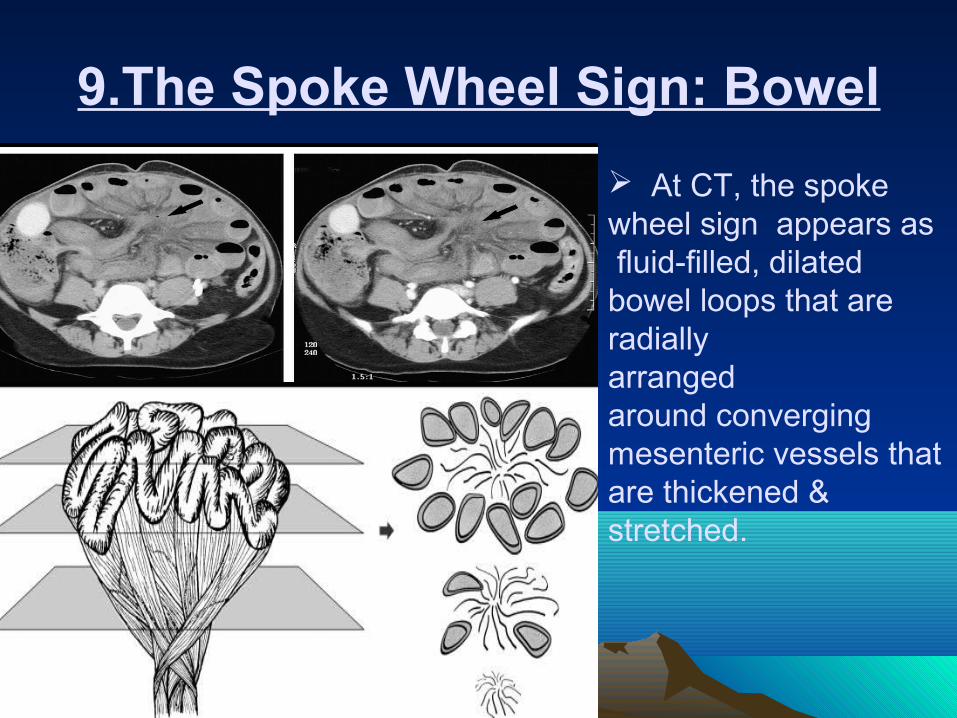
9.The Spoke Wheel Sign: Bowel
At CT, the spoke wheel sign appears as fluid-filled, dilated bowel loops that are radiallyarranged around converging mesenteric vessels that are thickened & stretched.
In small-bowel volvulus ,the shortening and tightening of the mesentery causes the fluid-filled, dilated bowel loops that are attached to the twisted mesentery to lie in a concentric, moreperipheral location, with the engorged and thickened mesentericvascular structures occupying the center.
The most common causes of small-bowel volvulus (ie, theso-called secondary small-bowel volvulus) are adhesive bands and internal and external hernias.
The most valuable CT finding for the detection of strangulating small-bowel obstruction is poor or no enhancement of the bowel wall after intravenous contrast material injection.
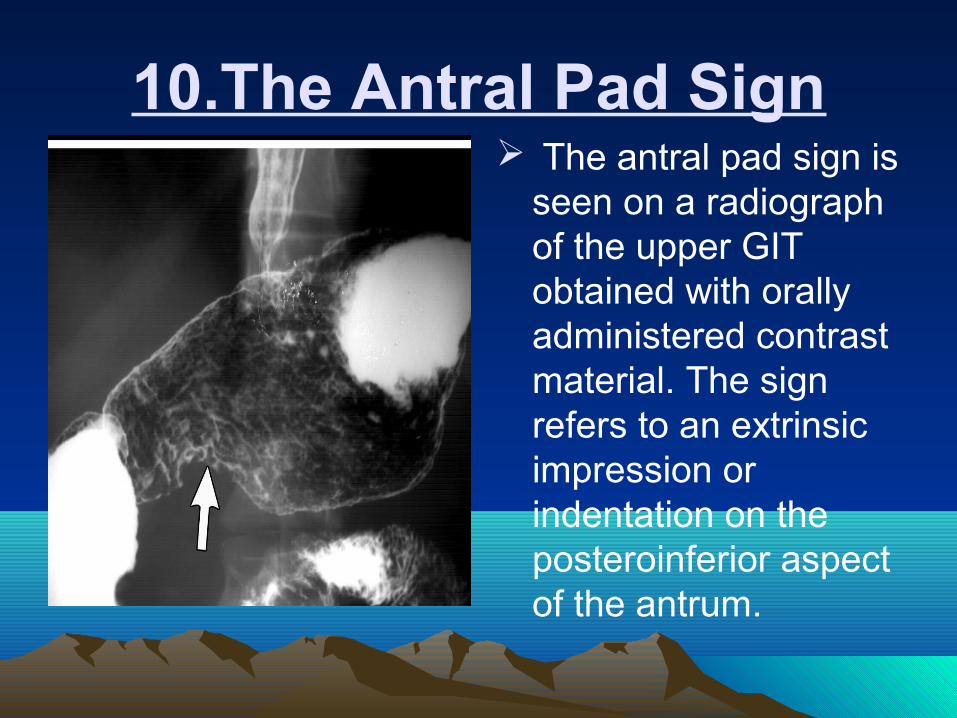
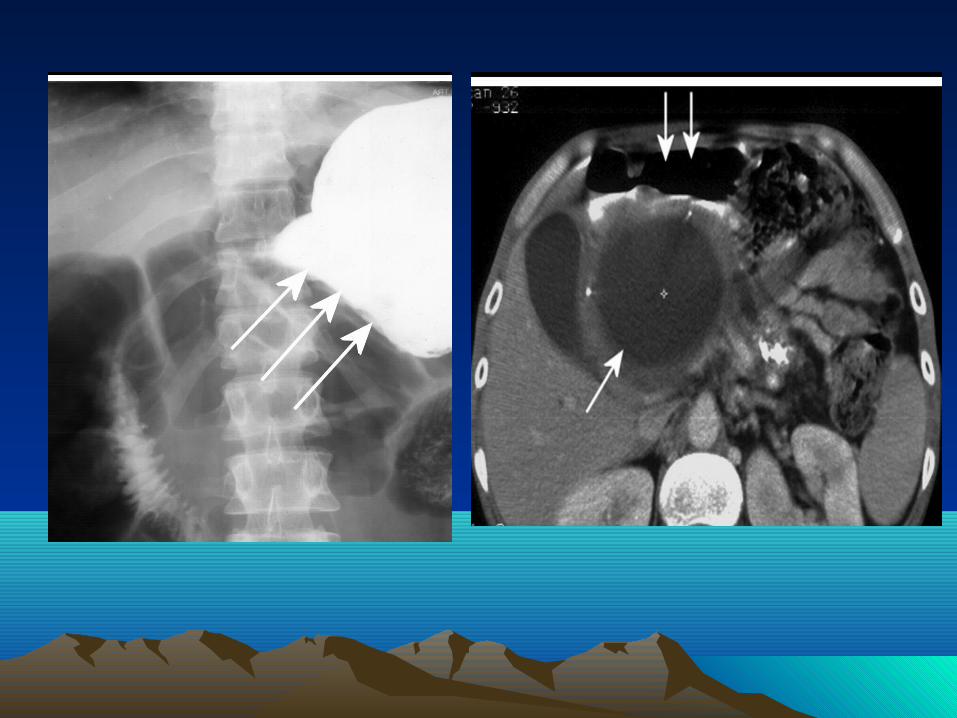
10.The Antral Pad Sign The antral pad sign is
seen on a radiograph of the upper GIT obtained with orally administered contrast material. The sign refers to an extrinsic impression or indentation on the posteroinferior aspect of the antrum.

The impression is typically caused by a lesion in the region of the head or body of the pancreas.
However, it has been shown that the antral pad sign can be caused by a normal gallbladder or by pancreatitis, pseudocyst of the pancreas, or neoplasms of the head and body of the pancreas.
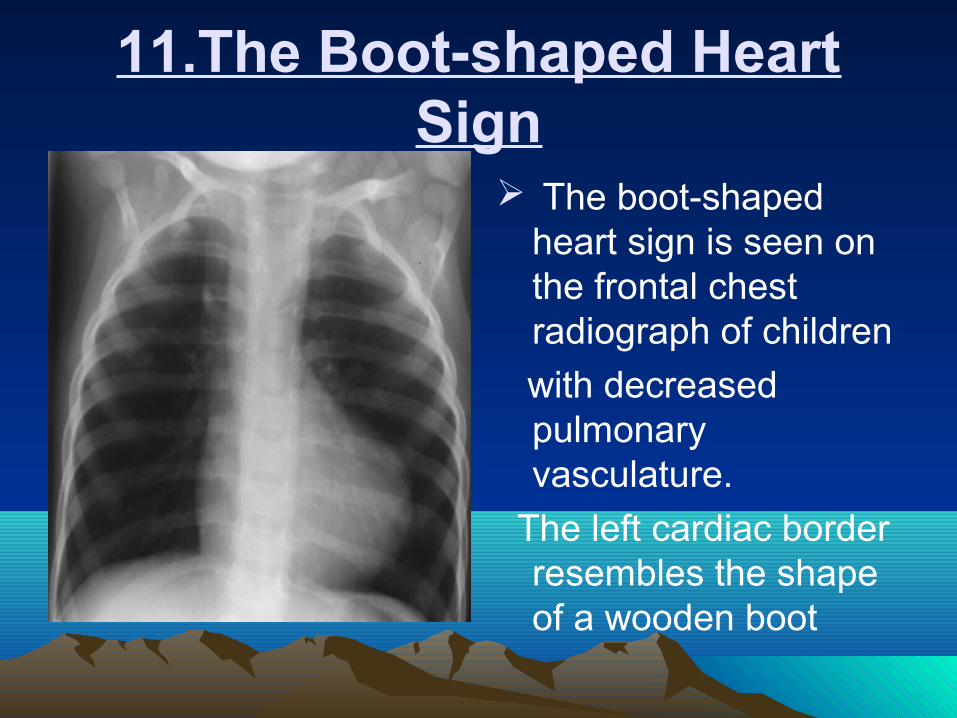
11.The Boot-shaped Heart Sign
The boot-shaped heart sign is seen on the frontal chest radiograph of children
with decreased pulmonary vasculature.
The left cardiac border resembles the shape of a wooden boot
The boot-shaped heart or coeur en sabot is often seen in patients with TOF, which is the most common cause (75%) of cyanotic heart disease.
The toe of the boot is formed by the upward pointing cardiac apex, which makes an acute angle with the diaphragm. The upturned cardiac apex is ascribed to right ventricular hypertrophy.
The narrower upper part of the boot results from a small or absent main pulmonary artery.
When TOF is also associated with an atrial septal defect,it is called the pentalogy of Fallot.
Right aortic arch occurs in 20%–30% of patients withcyanotic TOF.
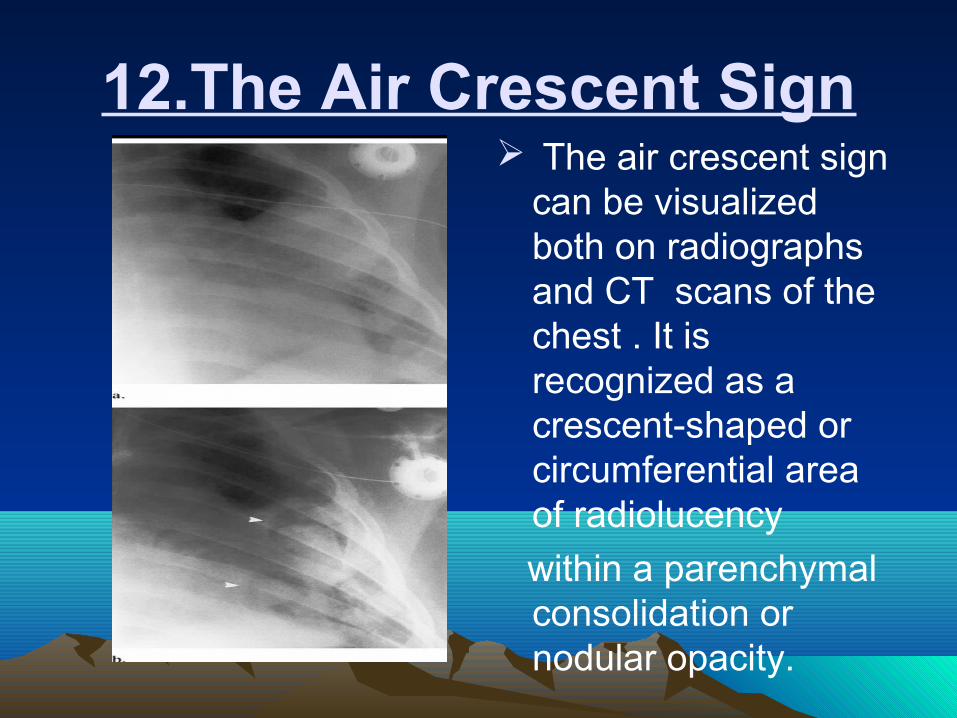
12.The Air Crescent Sign The air crescent sign
can be visualized both on radiographs and CT scans of the chest . It is recognized as a crescent-shaped or circumferential area of radiolucency
within a parenchymal consolidation or nodular opacity.
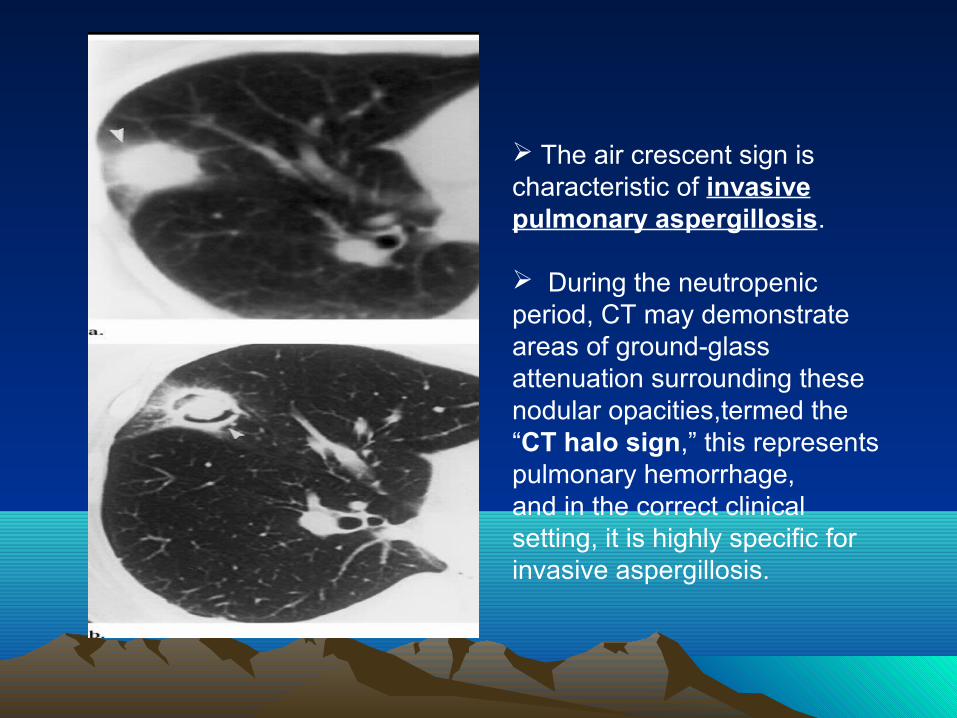
The air crescent sign ischaracteristic of invasive pulmonary aspergillosis.
During the neutropenicperiod, CT may demonstrate areas of ground-glassattenuation surrounding these nodular opacities,termed the “CT halo sign,” this represents pulmonary hemorrhage,and in the correct clinical setting, it is highly specific forinvasive aspergillosis.

Patients with neutropenia do not develop cavitary lesions.Visualization of the air crescent sign is an indicator that marksthe recovery phase of the infection.
A cavitating neoplasm,infections such as tuberculosis, nocardiosis, or a bacterial lung abscess may also give rise to an air crescent sign.
Not to mistake the Monad sign of aspergilloma withthe air crescent sign of invasive aspergillosis. The former developsin immunologically competent patients with structural lung disease. The radiographic appearance is that of a gravity dependentmass within a preexisting cavity.
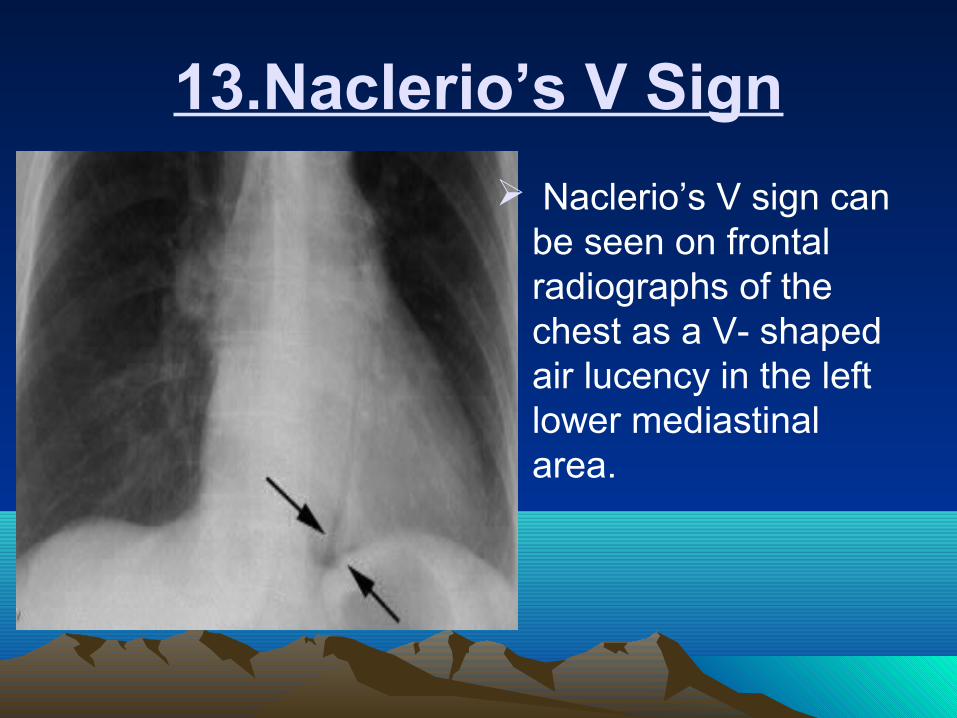
13.Naclerio’s V Sign
Naclerio’s V sign can be seen on frontal radiographs of the chest as a V- shaped air lucency in the left lower mediastinal area.
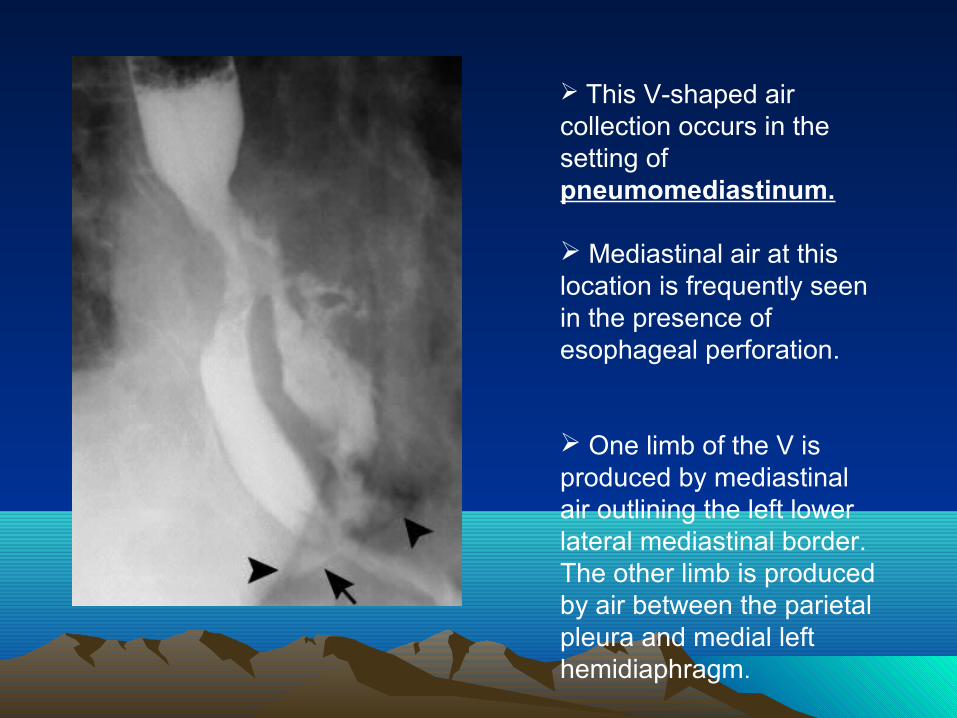
This V-shaped air collection occurs in the setting of pneumomediastinum.
Mediastinal air at this location is frequently seen in the presence of esophageal perforation.
One limb of the V is produced by mediastinal air outlining the left lower lateral mediastinal border. The other limb is produced by air between the parietal pleura and medial left hemidiaphragm.

14.The Deep Sulcus Sign
The deep sulcus sign is seen on chest radiographs obtained with the patient in the supine position. It represents lucency of the lateral costophrenic angle extending toward the hypochondrium.
It is important that the lateral costophrenic angles are included on the radiograph, as failure to diagnose pneumothorax may be life-threatening because of the risk of tension.
False-positive cases of the deep sulcus sign have beendescribed in patients with chronic obstructive pulmonary disease,in which hyperaeration of the lungs deepens the lateralcostophrenic angle.
Further evaluation with lateral decubitus radiography maybe helpful, but computed tomography is more sensitive forconfirming the presence of a pneumothorax in supine patients.

15.The Dependent Viscera Sign
The dependent viscera sign is seen at supine computed tomography (CT) in the thoracoabdominal area. The viscera (ie, the bowel or solid organs) are positioned against the posterior ribs, with obliteration of the posterior costophrenic recess
The dependent viscera sign is seen with diaphragmatic rupture.
The absence of posterior support by the diaphragm allows viscera to “fall” against the posterior ribs to a dependent position.
The dependent viscera sign is up to 100% sensitive as a sign of diaphragmatic rupture and 83% sensitive for right-sided injury.
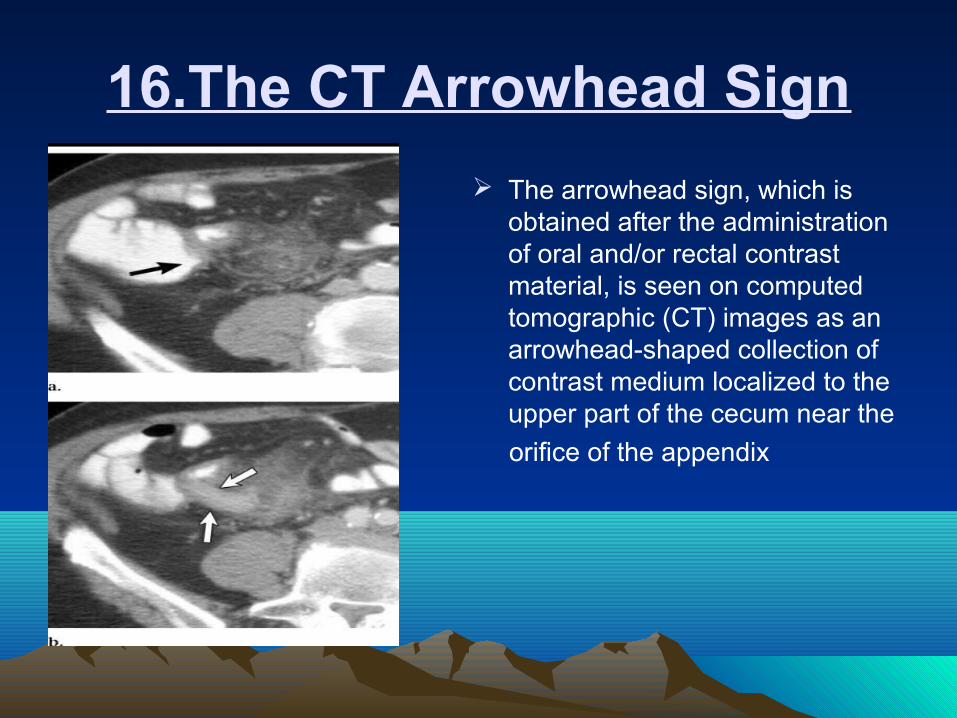
16.The CT Arrowhead Sign
The arrowhead sign, which is obtained after the administration of oral and/or rectal contrast material, is seen on computed tomographic (CT) images as an arrowhead-shaped collection of contrast medium localized to the upper part of the cecum near the
orifice of the appendix
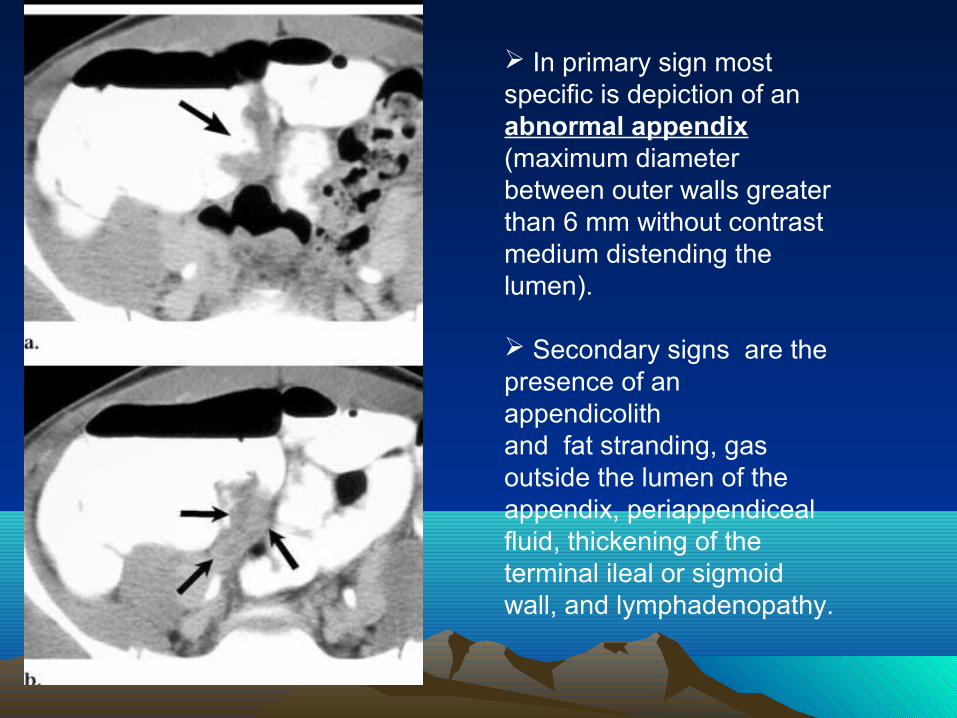
In primary sign most specific is depiction of an abnormal appendix(maximum diameter between outer walls greater than 6 mm without contrast medium distending the lumen).
Secondary signs are the presence of an appendicolithand fat stranding, gas outside the lumen of theappendix, periappendiceal fluid, thickening of the terminal ileal or sigmoid wall, and lymphadenopathy.
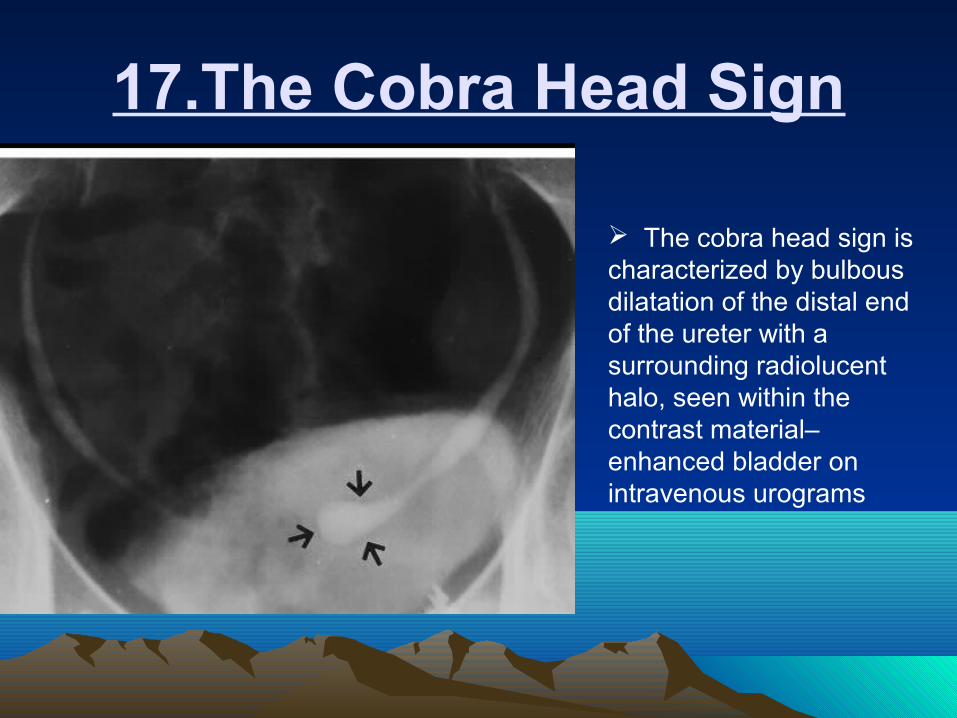
17.The Cobra Head Sign
The cobra head sign is characterized by bulbous dilatation of the distal end of the ureter with a surrounding radiolucenthalo, seen within the contrast material–enhanced bladder onintravenous urograms

The cobra head sign is classically seen with an intravesical ureterocele.
The term ureterocele denotes a cystic ballooning of the distal end of the ureter.
This type of ureterocele is also termed orthotopic, since it arises from a ureter with a normal insertion into the Trigone.
Most intravesical ureteroceles are incidental findings in asymptomatic adult patients. When large, ureteroceles can cause obstruction of the bladder neck, along with obstruction of the ipsilateral ureter. This results in an increased frequency of calculus formation, as well as infection.
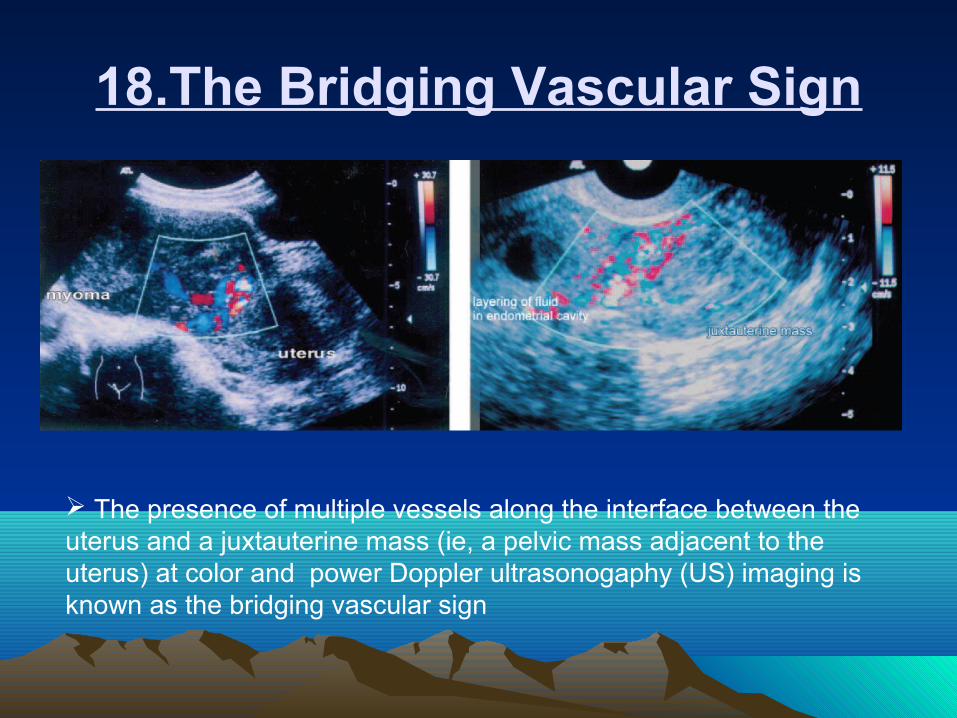
18.The Bridging Vascular Sign
The presence of multiple vessels along the interface between the uterus and a juxtauterine mass (ie, a pelvic mass adjacent to the uterus) at color and power Doppler ultrasonogaphy (US) imaging is known as the bridging vascular sign
Juxtauterine masses include subserosal myomas, adnexal masses, bowel masses, and other pelvic lesions.
The bridging vascular sign indicates the uterine origin of a juxtauterine mass.
Solid ovarian masses, such as fibromas, granulosa cell tumors, germ cell tumors (dysgerminomas, mixed germ cell tumors, or terato-sarcomas), metastatic tumors, and lymphomas, may be confused with subserous myomas owing to their similar imaging findings.
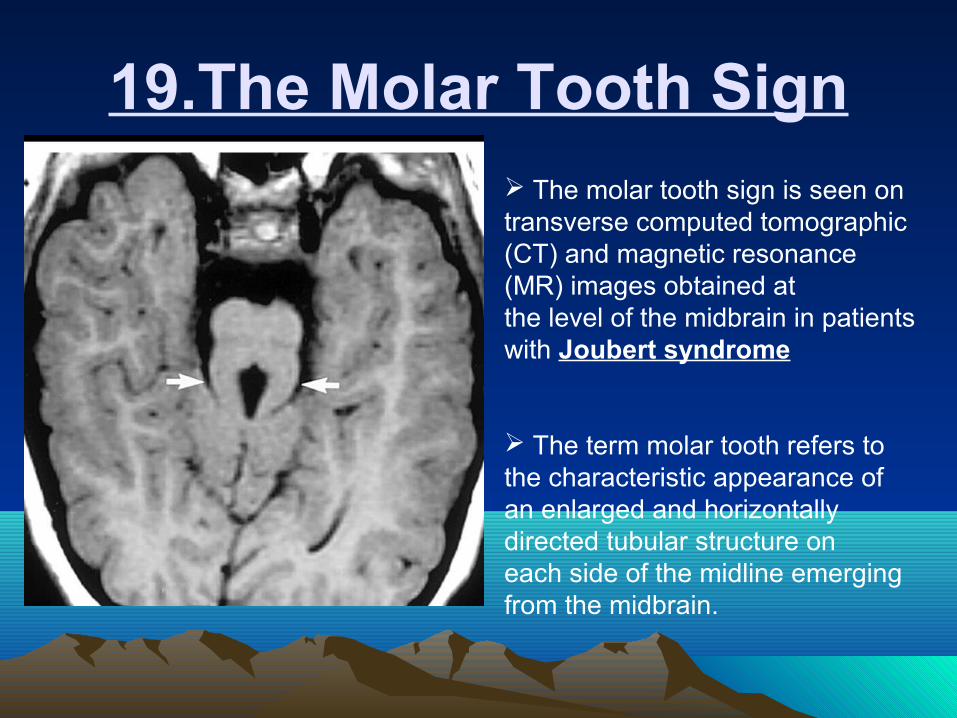
19.The Molar Tooth Sign The molar tooth sign is seen on transverse computed tomographic(CT) and magnetic resonance (MR) images obtained atthe level of the midbrain in patients with Joubert syndrome
The term molar tooth refers to the characteristic appearance ofan enlarged and horizontally directed tubular structure oneach side of the midline emerging from the midbrain.
The sign is caused by a lack of normal decussation of superiorcerebellar peduncular fiber tracts in patients with Joubert syndrome.
Joubert syndrome is an autosomal recessive disorder with characteristic pathologic findings of cerebellar vermian hypoplasia with a midline cleft.
Joubert syndrome has also been associated with a constellation of other findings, including microcephaly, dysmorphic facies, retinal dystrophy, tongue protrusion, multicystic kidney disease, congenital heart disease, unsegmented midbrain tectum, and agenesis of the corpus callosum.

20.The Mount Fuji Sign
The Mount Fuji sign is a finding that can be observed on computed tomographic (CT) scans of the brain in which bilateral subdural hypoattenuating collections cause compression and separation of the frontal lobes.
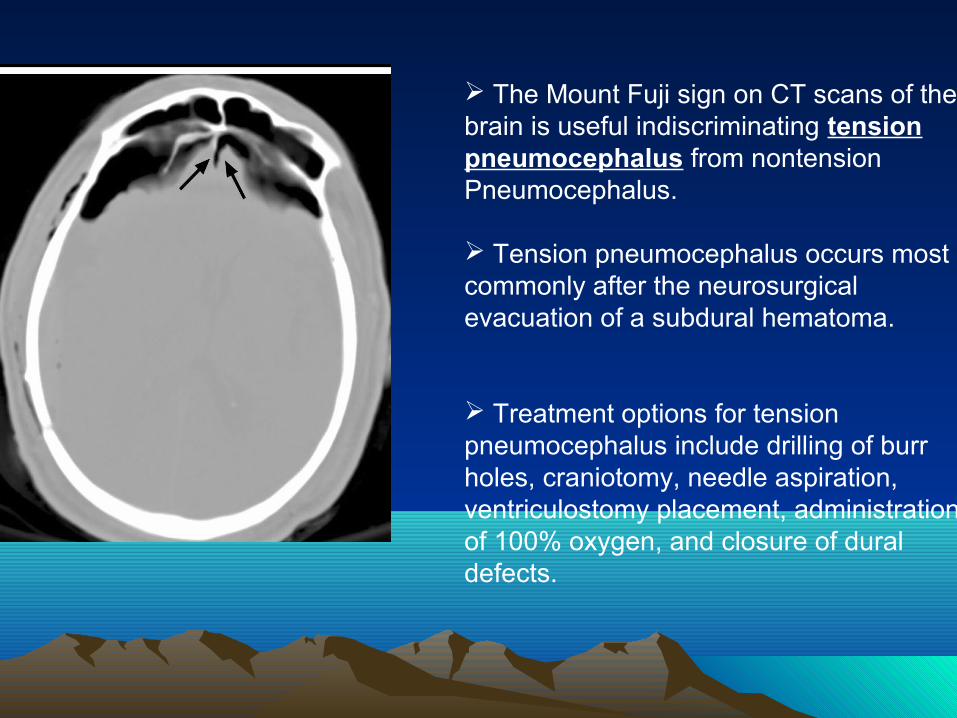
The Mount Fuji sign on CT scans of the brain is useful indiscriminating tension pneumocephalus from nontensionPneumocephalus.
Tension pneumocephalus occurs most commonly after the neurosurgicalevacuation of a subdural hematoma.
Treatment options for tension pneumocephalus include drilling of burr holes, craniotomy, needle aspiration, ventriculostomy placement, administrationof 100% oxygen, and closure of dural defects.

21.The Rigler Sign In the Rigler sign, which is also known as the double-wall signor the bas-relief sign , both sides of the bowel wall can be visualized on a radiograph of the abdomen obtained with the patient in the supine position.
The Rigler sign is the second most common sign ofpneumoperitoneum on supine radiographs, with a prevalenceof 32% in the studied cases of pneumoperitoneum.
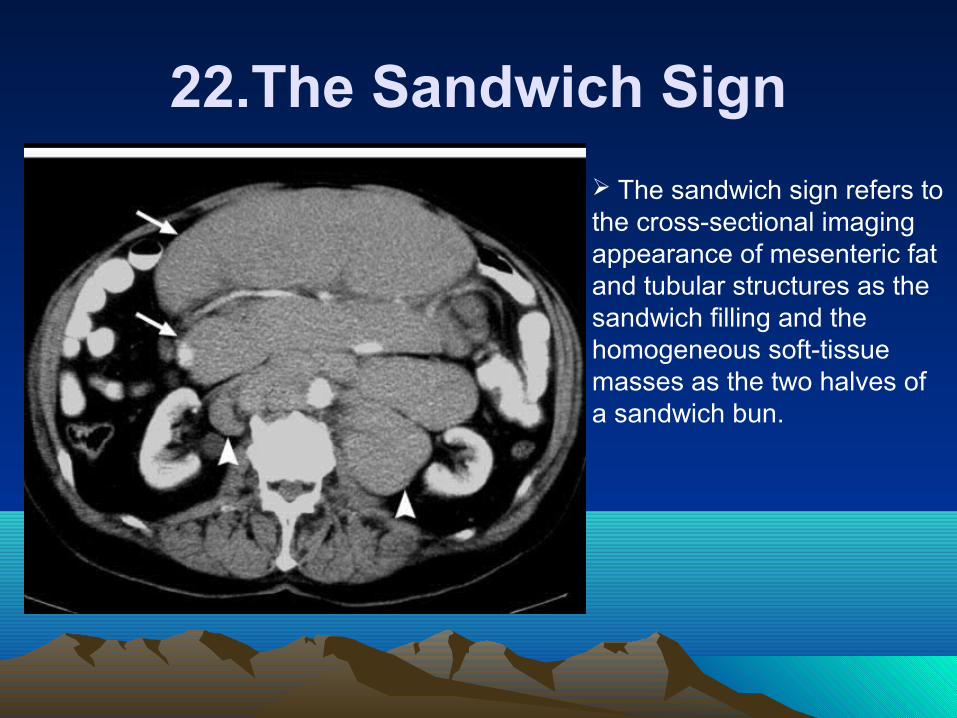
22.The Sandwich Sign
The sandwich sign refers to the cross-sectional imaging appearance of mesenteric fat and tubular structures as the sandwich filling and the homogeneous soft-tissue masses as the two halves of a sandwich bun.

The CT appearance of the mesenteric fat and vessels resemblessandwich filling, while the soft-tissue adenopathy representsthe bun.
There are numerous causes of mesenteric denopathy.,carcinoma,, carcinoid tumor, lymphadenopathy syndrome associated with acquired immunodeficiency syndrome (AIDS), tuberculosis, Whipple disease, and inflammatory bowel disease are among the most common causes. These diseases, however, do not produce the large bulky adenopathy that results in the sandwich sign.
This sign is specific to mesenteric lymphomas, most mesenteric lymphomas are NHLs.
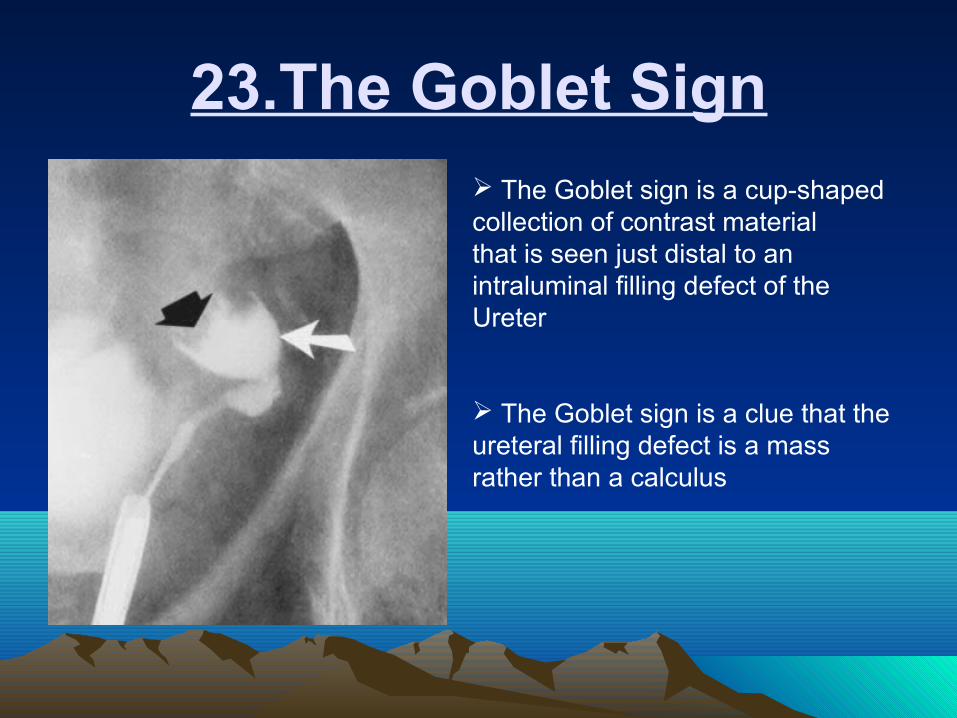
23.The Goblet Sign The Goblet sign is a cup-shaped collection of contrast materialthat is seen just distal to an intraluminal filling defect of theUreter
The Goblet sign is a clue that the ureteral filling defect is a massrather than a calculus
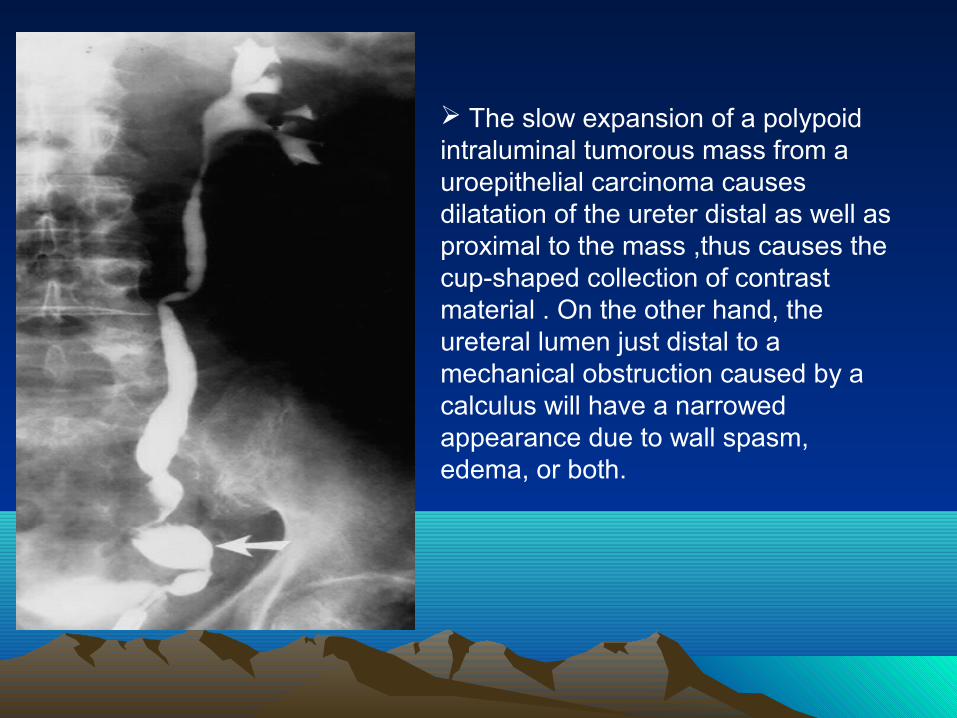
The slow expansion of a polypoidintraluminal tumorous mass from a uroepithelial carcinoma causes dilatation of the ureter distal as well as proximal to the mass ,thus causes the cup-shaped collection of contrast material . On the other hand, the ureteral lumen just distal to a mechanical obstruction caused by acalculus will have a narrowed appearance due to wall spasm,edema, or both.

24.The Golf Ball– on-Tee Sign
The golf ball– on-tee sign is seen during excretory urography and appears as a contrast agent–filled cavity (the golf ball) that lies adjacent to a blunted calyx (the tee).
The golf ball– on-tee sign is part of the spectrum of papillary necrosis and is distinguished by a papillary cavity that lies adjacent to a blunted Calyx.
The common etiology of papillary necrosis can be conveniently remembered with mnemonic NSAID: nonsteroidal anti-inflammatory medications, sickle cell hemoglobinopathies, analgesic nephropathy (specifically aspirin and phenacetin), infection (specifically tuberculosis), and diabetes.
Papillary necrosis can be bilateral or unilateral. Bilateral disease usually indicates a systemic or disseminated cause and often results from analgesic nephropathy, diabetes, and sickle cell trait or disease. Unilateral disease is associated with severe unilateral acute pyelonephritis, obstruction, and renal vein thrombosis.
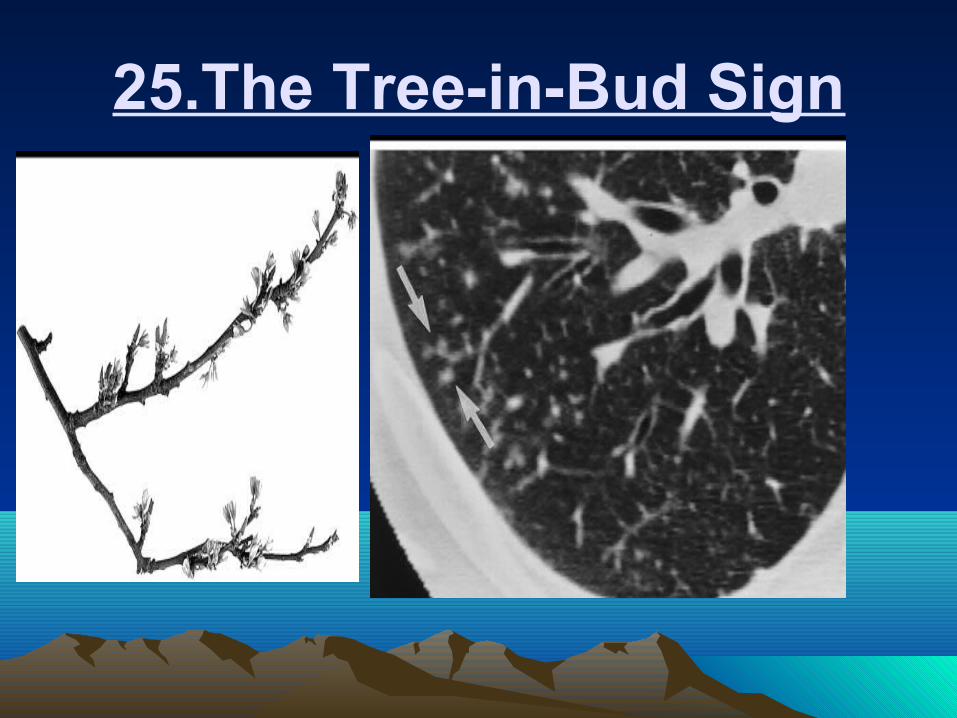
25.The Tree-in-Bud Sign

The tree-in-bud sign is a finding seen on thin-section CT images of the lung . Peripheral (within approximately 3–5 mm of the pleural surface), small (2–4 mm in diameter), centrilobular, and well-defined nodules of soft-tissue attenuation are connected to linear, branching opacities that have more than one contiguous branching site, thus resembling a tree in bud.
The tree-in-bud pattern represents bronchiolar luminal impaction with mucus, pus, or fluid, which demarcates the normally invisible branching course of the peripheral airways
The tree-in-bud sign has primarily been used as a descriptive term for abnormalities found on CT scans of the lung in patients with endobronchial spread of Mycobacterium tuberculosis.

THANKSTHANKS


















