
Radiological quiz. Sudden sensorineural hearing loss due ...
4
Case report/Kazuistyka Radiological quiz. Sudden sensorineural hearing loss due to multiple sclerosis Cavid Cabbarzade 1, *, Burçe Özgen 2 , Levent Sennaroglu 1 1 Otorhinolaryngology, Hacettepe University, School of Medicine, Ankara, Turkey 2 Radiology Hacettepe University, School of Medicine, Ankara, Turkey Introduction Sudden sensorineural hearing loss (SSNHL) has more than 100 possible etiologies, apart from the most common ones such as microvascular alterations and viral infections [1, 2]. Multiple sclerosis (MS) is a recurrent neurological disorder with extensive multiple plaque formation consis- ting of chronic inflammation, demyelinization and gliozis [3]. Peripheral nervous system involvement is not so common in MS [4]. SSNHL owing to multiple sclerosis (MS) is seen more common than expected. Although 6% of MS patients have several complaints about hearing loss, 80% of them have been found to have objective hearing distortions [5, 6]. SSNHL has been detected in 1% of MS patients [7]. A case with SSNHL owing to MS who had clinical and dramatic radiological improvement just after medical therapy was reported in this article, with the help of updated literature. Case A 22-year-old young female patient was admitted to our clinic with a 2-week hearing loss and fullness complaint in right ear. She had been followed up by a neurologist with the diagnosis of MS for 7 years. The patient did not have tinnitus or vertigo and there was no sign of any viral otolaryngologia polska 68 (2014) 264–267 article info Article history: Otrzymano: 20.08.2013 Zaakceptowano: 20.09.2013 Dostępne online: 26.09.2013 Keywords: Multiple sclerosis Sudden sensorineural hearing loss abstract Objective: A case with sudden sensorineural hearing loss (SSNHL) owing to multiple sclerosis (MS) who had clinical and dramatic radiological improvement just after medical therapy was reported in this article. Method: Case report and review of related literature. Results: A 22-year-old female patient with MS related SSNHL was presented in this article. Magnetic resonance imaging (MRI) revealed an MS plaque localized at pons exten- ding from right cochlear nucleus to proximal part of the right cochlear nerve. Most dra- matic recovery was present in the 5th day control MRI, where the plaque located on pons disappeared completely. On the 10th day control audiogram hearing recovery was obser- ved and pure tone audiogram levels were almost normal. Conclusion: Sudden sensori- neural hearing loss owing to MS is seen more common than expected. It has good prog- nosis. Magnetic resonance imaging is also thought to have an important role in diagnosis and treatment efficacy of SSNHL owing to MS. Published by Elsevier Urban & Partner Sp. z o.o. on behalf of Polish Otorhinolaryngology – Head and Neck Surgery Society. * Corresponding author at: Hacettepe University, School of Medicine, Department of Otorhinolaryngology, 06100 Sıhhiye, Ankara, Turkey. Tel.: +90 312 305 1785; fax: +90 312 311 3500. E-mail address: [email protected] (C. Cabbarzade). Available online at www.sciencedirect.com ScienceDirect journal homepage: www.elsevier.com/locate/otpol 0030-6657/$ – see front matter . Published by Elsevier Urban & Partner Sp. z o.o. on behalf of Polish Otorhinolaryngology – Head and Neck Surgery Society. http://dx.doi.org/10.1016/j.otpol.2013.09.004
Transcript of Radiological quiz. Sudden sensorineural hearing loss due ...
o t o l a r yn go l o g i a p o l s k a 6 8 ( 2 0 1 4 ) 2 6 4 – 2 6 7
Available online at www.sciencedirect.com
ScienceDirect
journal homepage: www.elsevier.com/locate/otpol
Case report/Kazuistyka
Radiological quiz. Sudden sensorineural hearing
loss due to multiple sclerosisCavid Cabbarzade 1,*, Burçe Özgen 2, Levent Sennaroglu 1
1Otorhinolaryngology, Hacettepe University, School of Medicine, Ankara, Turkey2Radiology Hacettepe University, School of Medicine, Ankara, Turkey
a r t i c l e i n f o
Article history:
Otrzymano: 20.08.2013
Zaakceptowano: 20.09.2013
Dostępne online: 26.09.2013
Keywords:� Multiple sclerosis� Sudden sensorineural hearing loss
a b s t r a c t
Objective: A case with sudden sensorineural hearing loss (SSNHL) owing to multiple
sclerosis (MS) who had clinical and dramatic radiological improvement just after medical
therapy was reported in this article. Method: Case report and review of related literature.
Results: A 22-year-old female patient with MS related SSNHL was presented in this
article. Magnetic resonance imaging (MRI) revealed an MS plaque localized at pons exten-
ding from right cochlear nucleus to proximal part of the right cochlear nerve. Most dra-
matic recovery was present in the 5th day control MRI, where the plaque located on pons
disappeared completely. On the 10th day control audiogram hearing recovery was obser-
ved and pure tone audiogram levels were almost normal. Conclusion: Sudden sensori-
neural hearing loss owing to MS is seen more common than expected. It has good prog-
nosis. Magnetic resonance imaging is also thought to have an important role in diagnosis
and treatment efficacy of SSNHL owing to MS.
Published by Elsevier Urban & Partner Sp. z o.o. on behalf of Polish
Otorhinolaryngology – Head and Neck Surgery Society.
Introduction
Sudden sensorineural hearing loss (SSNHL) has more than100 possible etiologies, apart from the most common onessuch as microvascular alterations and viral infections [1,2]. Multiple sclerosis (MS) is a recurrent neurologicaldisorder with extensive multiple plaque formation consis-ting of chronic inflammation, demyelinization and gliozis[3]. Peripheral nervous system involvement is not socommon in MS [4]. SSNHL owing to multiple sclerosis(MS) is seen more common than expected. Although 6% ofMS patients have several complaints about hearing loss,80% of them have been found to have objective hearing
* Corresponding author at: Hacettepe University, School of MedicinTurkey. Tel.: +90 312 305 1785; fax: +90 312 311 3500.
E-mail address: [email protected] (C. Cabbarzade).0030-6657/$ – see front matter . Published by Elsevier Urban & Partner Sp. z o.o.
http://dx.doi.org/10.1016/j.otpol.2013.09.004
distortions [5, 6]. SSNHL has been detected in 1% of MSpatients [7]. A case with SSNHL owing to MS who hadclinical and dramatic radiological improvement just aftermedical therapy was reported in this article, with the helpof updated literature.
Case
A 22-year-old young female patient was admitted to ourclinic with a 2-week hearing loss and fullness complaint inright ear. She had been followed up by a neurologist withthe diagnosis of MS for 7 years. The patient did not havetinnitus or vertigo and there was no sign of any viral
e, Department of Otorhinolaryngology, 06100 Sıhhiye, Ankara,
on behalf of Polish Otorhinolaryngology – Head and Neck Surgery Society.
[(Fig._1)TD$FIG]
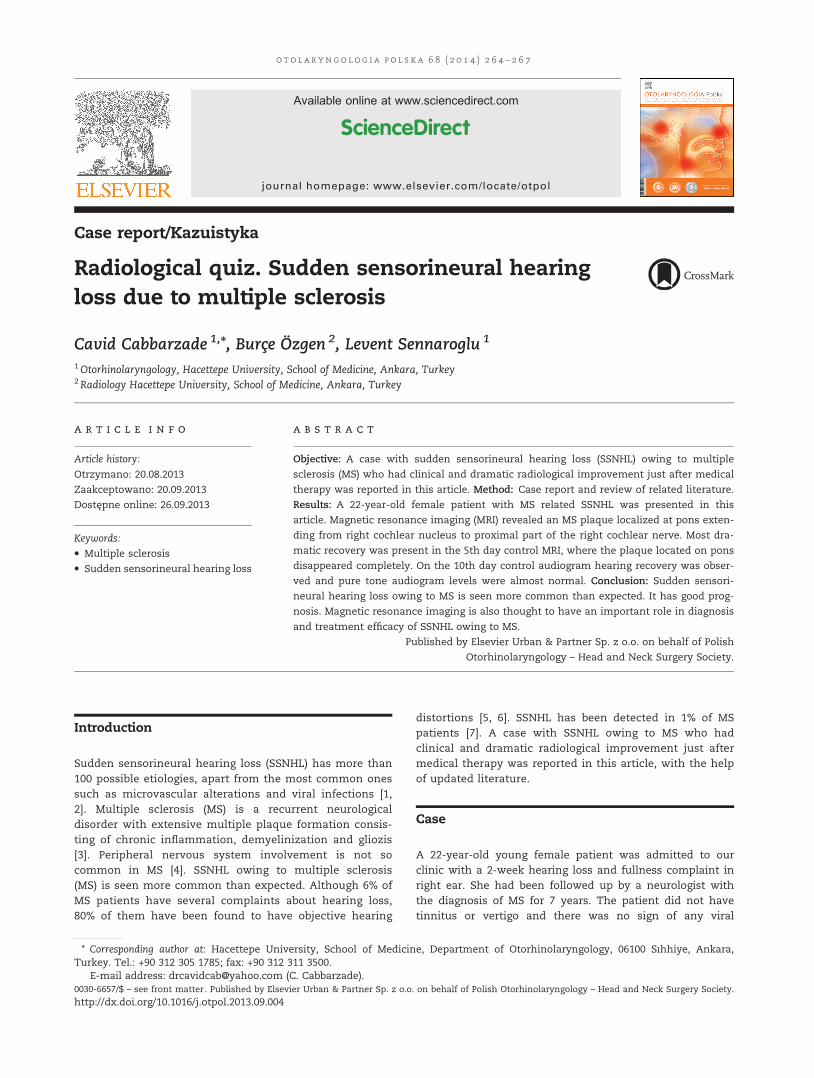
Fig. 1 – Pure tone audiograms of the patient on the first (A), fifth (B) and tenth (C) days
o t o l a r yn g o l o g i a p o l s k a 6 8 ( 2 0 1 4 ) 2 6 4 – 2 6 7 265
infection. She did not have any head trauma or acoustictrauma prior to hearing loss. On pure tone audiogram (PTA)there was mild to moderate SSNHL after 500 Hz (Fig. 1A).On the brainstem auditory evoked response (BAER) testshortening of right ear's IV and V waves and left ear'sV wave was detected. Magnetic resonance imaging (MRI)revealed an MS plaque localized at pons extending fromright cochlear nucleus to proximal part of the right cochlearnerve (Fig. 2A–C). The plaque had peripheral contrastenhancement which was compatible with active demyelini-zation. Treatment protocol which was composed of lowmolecular weight dextrane (5 mg/kg), betahistine (24 mgtwice in a day) and asetozolamide (250 mg once in a day)was started. Also methylprednisolone (1000 mg once a day)for 7 days was added to therapy by Neurology Department.On the 5th day control PTA, there was hearing improve-ment (Fig. 1B). Most dramatic recovery was present in thecontrol MRI, where the plaque located on pons disappearedcompletely (Fig. 3A and B). On the 10th day controlaudiogram hearing recovery was observed and PTA levelswere almost normal (Fig. 1C).
Discussion
MS is an acquired neurological disorder which is characteri-zed by demyelinization of central nervous system and mightcause multiple neurologic deficits. Patients with MS generallyare admitted to hospital with paresthesis, neurological weak-ness, ocular or cerebellar deficits [8]. Our case was admittedto our clinic with hearing loss and fullness in the right ear.
Eighty percent of the MS patients have audiovestibulardisorders [2]. Vertigo is seen relatively more common inpatients with MS and it is the initial symptom in 10% of cases[3]. SSNHL is detected in about 1% of MS patients in differentseries [2, 3]. Due to active attacks of MS demyelinization couldbe seen in cochlear nerve and appears as SSNHL [6]. AlsoSSNHL might be the initial symptom of MS [1]. Recurrentattacks of bilaterally SSNHL can be a warning sign of MS [3].
SSNHL owing to MS is seen due to demyelinization atcranial nerve or auditory brainstem. In most cases in theliterature demyelinization plaque is detected at root of thecochlear nerve, besides lesions through the nerve were also
[(Fig._2)TD$FIG]
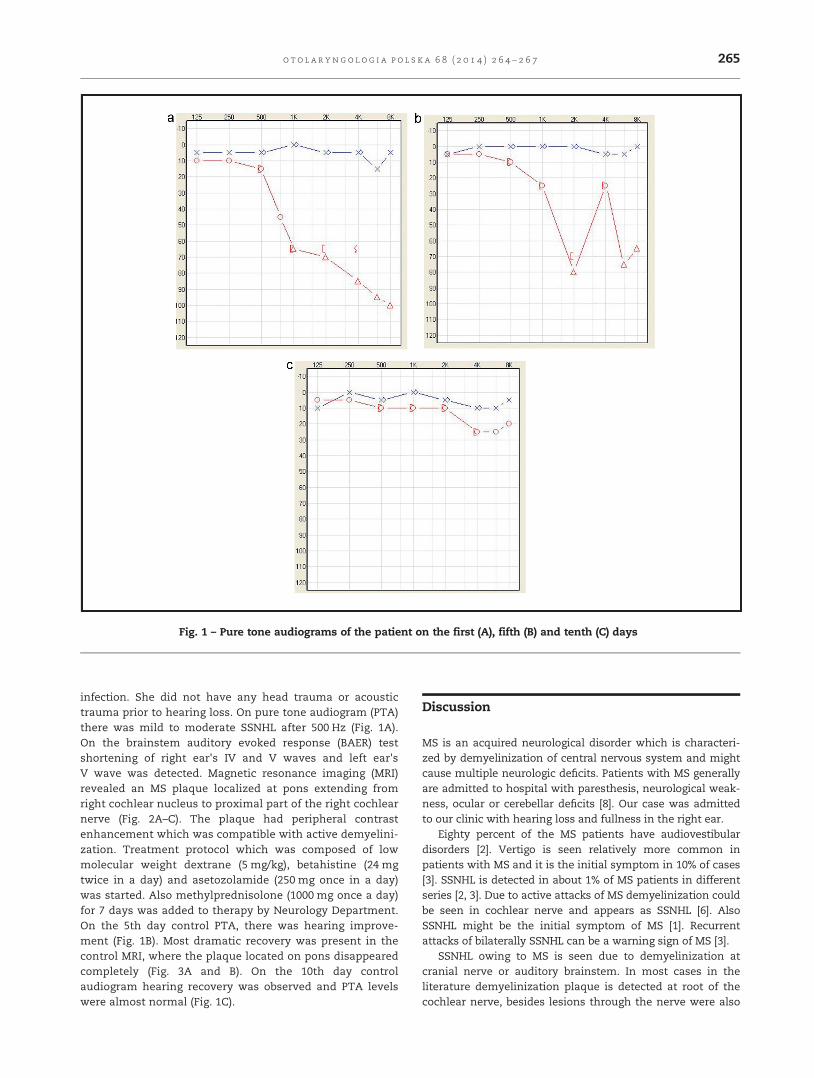
Fig. 2 – Axial T2 weighted (A) and post-contrast T1 weighted (B) images demonstrate an ovoid T2 hyperintense lesion (arrow)located at the anterior aspect of the right middle cerebellar peduncle with ring like enhancement on the post-contrastimages. Several other demyelinating plaques are also seen at the pons and the left cerebellum. Axial T2 weighted image (C)from the supratentorial brain reveals multiple demyelinating lesions in the white matter
[(Fig._3)TD$FIG]
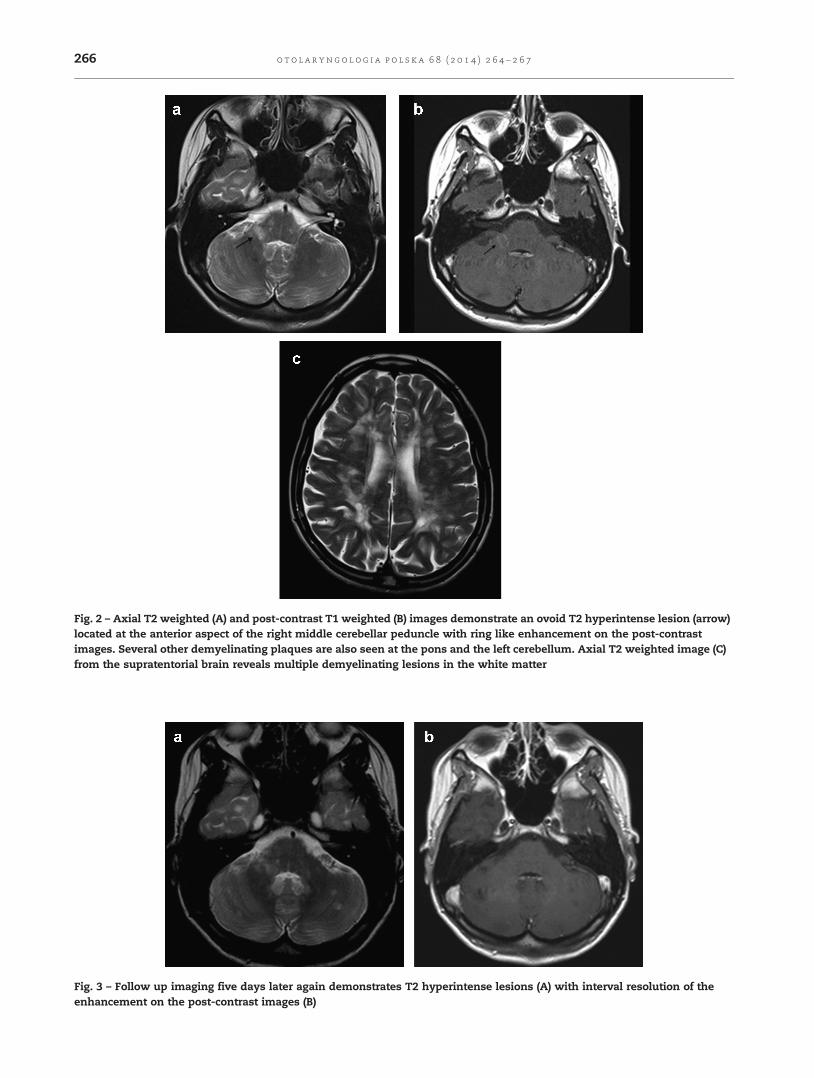
Fig. 3 – Follow up imaging five days later again demonstrates T2 hyperintense lesions (A) with interval resolution of theenhancement on the post-contrast images (B)
o t o l a r yn go l o g i a p o l s k a 6 8 ( 2 0 1 4 ) 2 6 4 – 2 6 7266

o t o l a r yn g o l o g i a p o l s k a 6 8 ( 2 0 1 4 ) 2 6 4 – 2 6 7 267
reported [4, 7, 9]. In the present case a large demyelinizationplaque was detected on the proximal part of the rightcochlear nerve and cochlear nucleus which disappeared onthe 5th day of the medical therapy and hearing gain wasalso observed.
Hearing loss pattern depends on the localization of thedemyelinization plaque. If demyelinization occurs on the rootof cochlear nerve, high frequency hearing loss is observedlike in cochlear nerve masses. Low frequency hearing loss isdetected in cases with demyelinization in auditory brainstem. Edema around the demyelinization area may mimicthe cochlear type SSNHL [2]. In our case rapid hearingimprovement may be seen due to regression of demyeliniza-tion area and absorption of the edema in auditory tract.
In MS cases with SSNHL PTA, BAER, caloric test and MRIshould be performed besides the clinical assessment. Dec-rease in neural velocity in MS patients might cause latencyand amplitude changes in BAER which can be observed asabsence or latency of the waves and latency between waves[2]. Even in patient with MS who do not have audiologicaldysfunction symptoms, latency, shortening of the amplitudeand absence of the wave V is commonly seen [6]. In ourpatient's BAER test there were low amplitudes of wave IVand V at the affected ear and also at the opposite clinicallyunaffected ear.
MRI has superiority to computerized tomography indetecting demyelinization lesions in MS [8]. MRI has a veryimportant role in diagnosis, following up and detectingtherapy efficacy in MS patients. Modern MRI techniquessuch as diffusion tensor imaging (DTI), magnetic transferimaging (MTI), magnetic resonance spectroscopy (MRS) andrelaxometry have higher sensitivity and specificity in dis-tinguishing normal and affected brain tissue in MS [10].
SSNHL in MS patients is generally short termed and hasgood prognosis [4]. In these cases, central nervous systemdemyelinization occurs at intra-axial part above thecochlear nerve bifurcation which supports the prognosis [4].In our case on the 5th day of the therapy completeradiologic improvement and on the 10th day full clinicrecovery was observed.
Conclusion
Both ENT specialists and neurologists should be alerted toMS in patients with SSNHL. SSNHL owing to MS has goodprognosis. Also MRI has very important role in diagnosis aswell as following up treatment efficacy in patients withSSNHL owing to MS.
Authors' contributions/Wkład autorów
CC – study design, data interpretation, acceptance offinal manuscript version, literature search. BÖ, LS – study
design, data interpretation, acceptance of final manuscriptversion.
Conflict of interest/Konflikt interesu
None declared.
Financial support/Finansowanie
None declared.
Ethics/Etyka
The work described in this article has been carried out inaccordance with The Code of Ethics of the World MedicalAssociation (Declaration of Helsinki) for experiments invol-ving humans; EU Directive 2010/63/EU for animal experi-ments; Uniform Requirements for manuscripts submitted toBiomedical journals.
r e f e r e n c e s / p i �s m i e n n i c t w o
[1] Drulovic B, Ribarić-Jankes K, Kostić V, Sternić N. Multiplesclerosis as the cause of sudden 'pontine' deafness.Audiology 1994;33(4):195–201.
[2] Ozunlu A, Mus N, Gulhan M. Multiple sclerosis:a cause of sudden hearing loss. Audiology 1998;37(1):52–58.
[3] Oh YM, Oh DH, Jeong SH, Koo JW, Kim JS. Sequentialbilateral hearing loss in multiple sclerosis. Ann Otol RhinolLaryngol 2008;117(3):186–191.
[4] Hellmann MA, Steiner I, Mosberg-Galili R. Suddensensorineural hearing loss in multiple sclerosis: clinicalcourse and possible pathogenesis. Acta Neurol Scand2011;124(4):245–249.
[5] Schweitzer VG, Shepard N. Sudden hearing loss: anuncommon manifestation of multiple sclerosis.Otolaryngol Head Neck Surg 1989;100(4):327–332.
[6] Yamasoba T, Sakai K, Sakurai M. Role of acute cochlearneuritis in sudden hearing loss in multiple sclerosis. JNeurol Sci 1997;146(2):179–181.
[7] Bergamaschi R, Romani A, Zappoli F, Versino M, Cosi V. MRIand brainstem auditory evoked potential evidence of eighthcranial nerve involvement in multiple sclerosis. Neurology1997;48(1):270–272.
[8] Franklin DJ, Coker NJ, Jenkins HA. Sudden sensorineuralhearing loss as a presentation of multiple sclerosis. ArchOtolaryngol Head Neck Surg 1989;115(1):41–45.
[9] Furman JM, Durrant JD, Hirsch WL. Eighth nerve signs in acase of multiple sclerosis. Am J Otolaryngol 1989;10(6):376–381.
[10] Ceccarelli A, Bakshi R, Neema M. MRI in multiple sclerosis:a review of the current literature. Curr Opin Neurol 2012;25(4):402–409.


















