
Radiographic Evaluation of Blunt Ankle Trauma
39
Jack Casey, HMS III Gillian Lieberman, MD Page 1 Jack Casey, HMS IV Gillian Lieberman, MD Radiographic Evaluation of Blunt Ankle Trauma
Transcript of Radiographic Evaluation of Blunt Ankle Trauma
Jack Casey, HMS III Gillian Lieberman, MD
Page 1
Jack Casey, HMS IVGillian Lieberman, MD
Radiographic Evaluation of Blunt Ankle Trauma

Jack Casey, HMS III Gillian Lieberman, MD
Page 2
Overview
• Importance of ankle injuries• Imaging– when, how, and what to look for• Anatomy review• Common ankle injuries
– Patient cases to illustrate mechanisms of injury and radiologic classification
Focus on radiology

Jack Casey, HMS III Gillian Lieberman, MD
Page 3
Historical Context

Jack Casey, HMS III Gillian Lieberman, MD
Page 4
Blunt Ankle Trauma – Still A Major Problem
• Most common MSK injury• Less that 15% of patients have clinically
significant fractures• Ankle films are 3rd most common radiologic study
ordered in many hospitals• > $500 million spent annually on ankle
radiographs in North America• Clinical guidelines can help guide management
Steill et al. JAMA, 1993.

Jack Casey, HMS III Gillian Lieberman, MD
Page 5
Indications for Imaging The Ottawa Ankle Rules
• Set of clinical guidelines, designed to have sensitivity of 100% for detecting fractures s/p blunt ankle trauma.– willing to accept trade-off of lower specificity
• Expected benefits: Limit radiation exposure, health care costs, ED waiting time.
• Designed to be easy to use
Jack Casey, HMS III Gillian Lieberman, MD
Page 6
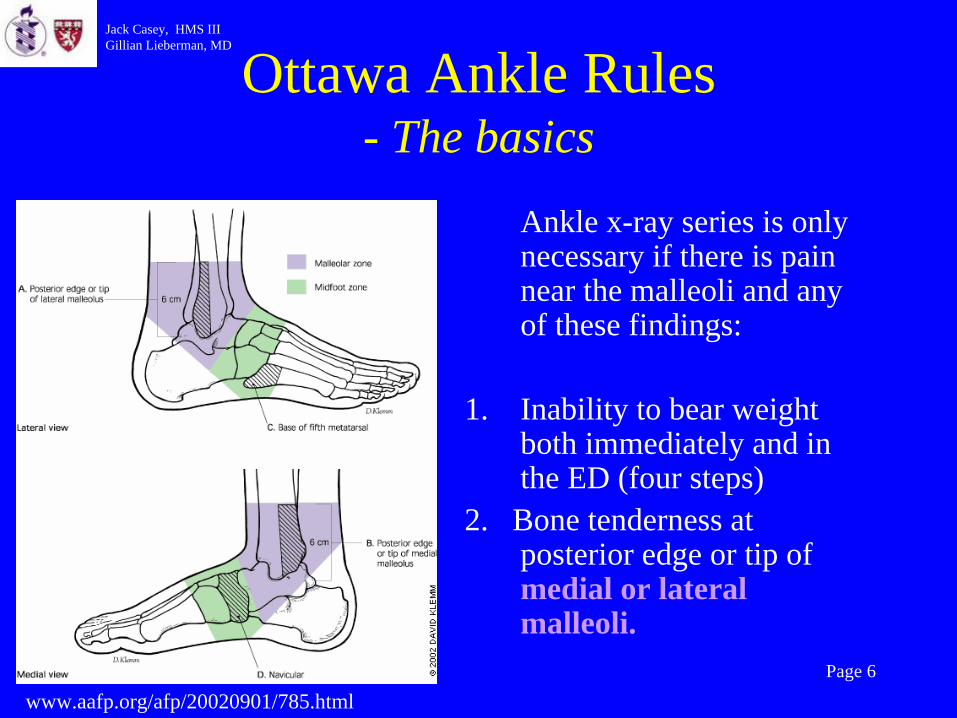
Ottawa Ankle Rules - The basics
Ankle x-ray series is only necessary if there is pain near the malleoli and any of these findings:
1. Inability to bear weight both immediately and in the ED (four steps)
2. Bone tenderness at posterior edge or tip of medial or lateral malleoli.
www.aafp.org/afp/20020901/785.html
Jack Casey, HMS III Gillian Lieberman, MD
Page 7
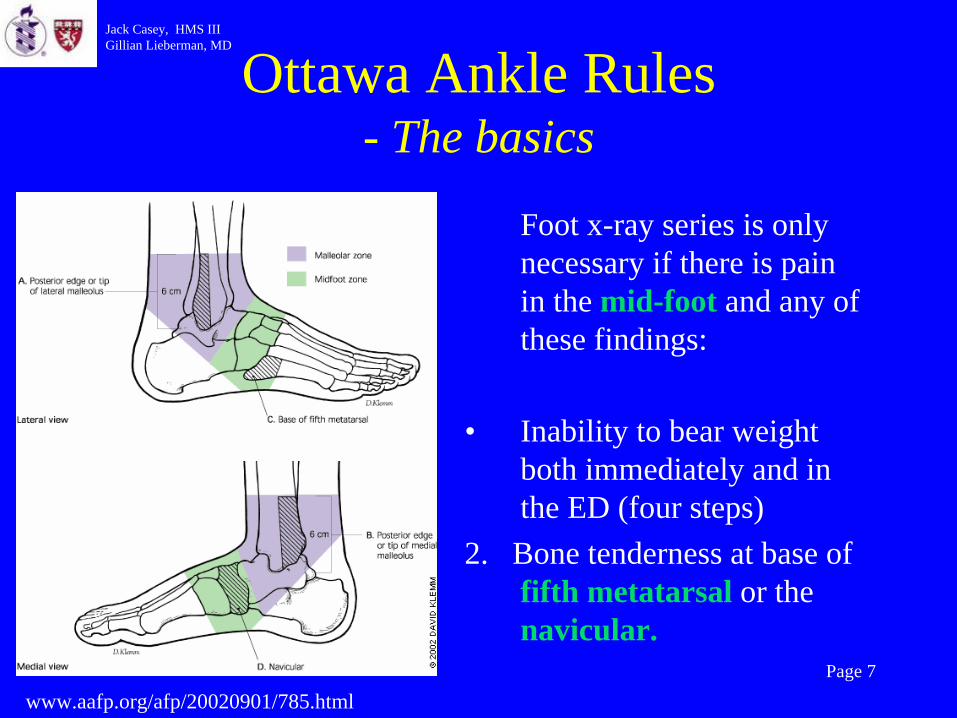
Ottawa Ankle Rules - The basics
Foot x-ray series is only necessary if there is pain in the mid-foot and any of these findings:
• Inability to bear weight both immediately and in the ED (four steps)
2. Bone tenderness at base of fifth metatarsal or the navicular.
www.aafp.org/afp/20020901/785.html

Jack Casey, HMS III Gillian Lieberman, MD
Page 8
Ottawa Ankle Rules - How good are they?
• Systemic review of 27 studies (15,581 patients) – Sensitivity 96.4 - 99.6 %– Specificity varied widely (10-79%)– Less than 2% of patients who were negative for fx according to
ankle rules actually had a fracture.– Missed fractures were almost always minor, did not affect long
term outcomes.
• 28% reduction in use of ankle radiography• No decrease in patient satisfaction
Bachmann et al. BMJ, 2003.Steill et al. JAMA, 1993.
Jack Casey, HMS III Gillian Lieberman, MD
Page 9
Ottawa Ankle Rules - A few limitations
• Not applicable to:– <18 y/o– Altered mental status– Multi-system trauma– Chronic/ subacute injuries
• Always trust clinical judgment

Jack Casey, HMS III Gillian Lieberman, MD
Page 10
Implementing the OAR
• Thorough (but brief) H+PEvaluate skin/ soft tissue. Assess for open fx.Check and document neurovascular statusPalpate entire distal 6 cm of both malleoli before asking patient to bear weightPalpate over 5th metatarsal and navicular for tendernessPalpate for tenderness over proximal fibula to exclude potential Maisonneuve fracture
• Think about underlying anatomy and mechanism of injury

Jack Casey, HMS III Gillian Lieberman, MD
Page 11
Basic Anatomy 1- Bones
Interactive Foot and Ankle. Primal Pictures, Ltc.
Anterior Process of Calcaneus
Jack Casey, HMS III Gillian Lieberman, MD
Page 12
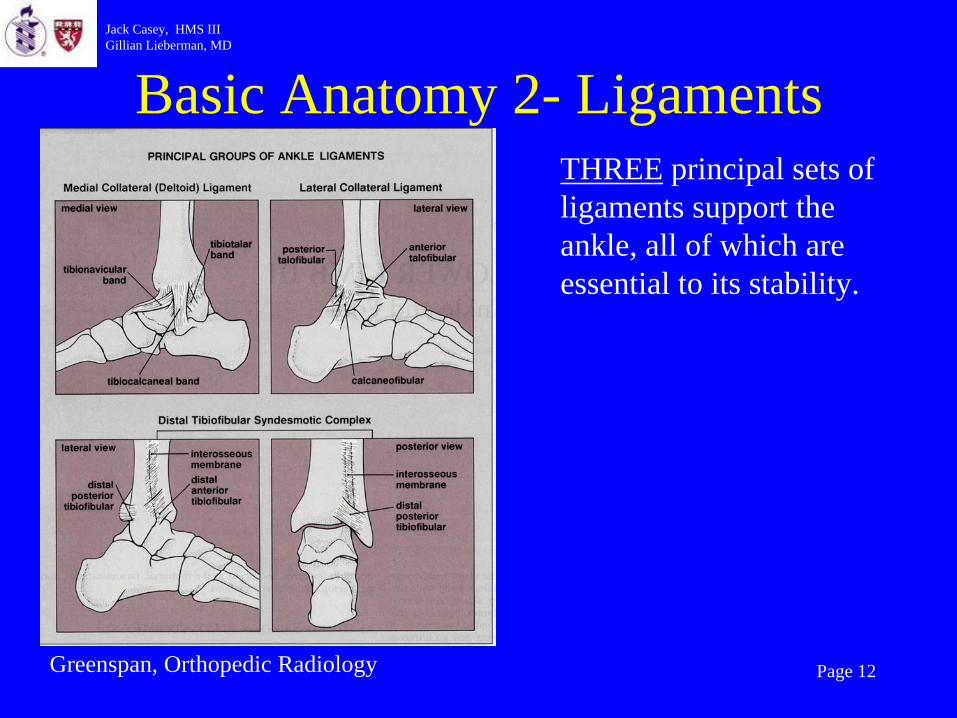
Basic Anatomy 2- Ligaments
Greenspan, Orthopedic Radiology
THREE principal sets of ligaments support the ankle, all of which are essential to its stability.

Jack Casey, HMS III Gillian Lieberman, MD
Page 13
Basic Anatomy 3- Tendons
Greenspan, OrthopedicRadiology

Jack Casey, HMS III Gillian Lieberman, MD
Page 14
Anatomy- Putting it All Together
Bones and connective tissue give rise to ring- like structure surrounding the talus.
Rosen’s Emergency Medicine: Concepts and Clinical Practice.

Jack Casey, HMS III Gillian Lieberman, MD
Page 15
Ankle Injuries-Inversion
Greenspan, Orthopedic Radiology
Remember Ring- Like Structure in Conceptualizing Injury.
www.emedicinehealth.com

Jack Casey, HMS III Gillian Lieberman, MD
Page 16
Ankle Injuries- Eversion
Greenspan, Orthopedic Radiology
Remember Ring- Like Structure in Conceptualizing Injury.
www.x-strap.com

Jack Casey, HMS III Gillian Lieberman, MD
Page 17
Appropriate Views
• Must always include:1) AP2) Mortise (ankle in 10 - 25 degrees of internal rotation)3) Lateral
• May add additional views in questionable cases (i.e. stress views, comparison views with uninjured ankle)

Jack Casey, HMS III Gillian Lieberman, MD
Page 18
Regions of Interest
• Bones of ankle joint• The fifth metatarsal tuberosity should be
seen in at least one projection. • Important to visualize anterior process of
the calcaneus.

Jack Casey, HMS III Gillian Lieberman, MD
Page 19
Normal AP Radiograph
www.rad.washington.edu

Jack Casey, HMS III Gillian Lieberman, MD
Page 20
Normal Mortise Radiograph
www.rad.washington.edu
Foot internally rotated 10- 35 degrees to allow for improved visualization of the mortise.

Jack Casey, HMS III Gillian Lieberman, MD
Page 21
AP vs. Mortise Views
AP Mortise
Images from Greenspan, Orthopedic Radiology

Jack Casey, HMS III Gillian Lieberman, MD
Page 22
Normal Lateral Radiograph
Note: ROI not fully included (5th
metatarsal absent)
www.rad.washington.edu

Jack Casey, HMS III Gillian Lieberman, MD
Page 23
Classifying Fractures
• Anatomic• Weber (AO)• Other

Jack Casey, HMS III Gillian Lieberman, MD
Page 24
Anatomic Classification of Fx
Identifying additional sites of fracture is not just an academic exercise– as bi/tri malleolar fx usually require othopedics eval, surgical management.
Greenspan,Orthopedic Radiology

Jack Casey, HMS III Gillian Lieberman, MD
Page 25
Unimalleolar Fx
Patient 1–s/p eversioninjury, fallfrom 10 feet
Small fx, medial malleolus
Also note dislocation talus
Image from BIDMC PACS
Jack Casey, HMS III Gillian Lieberman, MD
Page 26
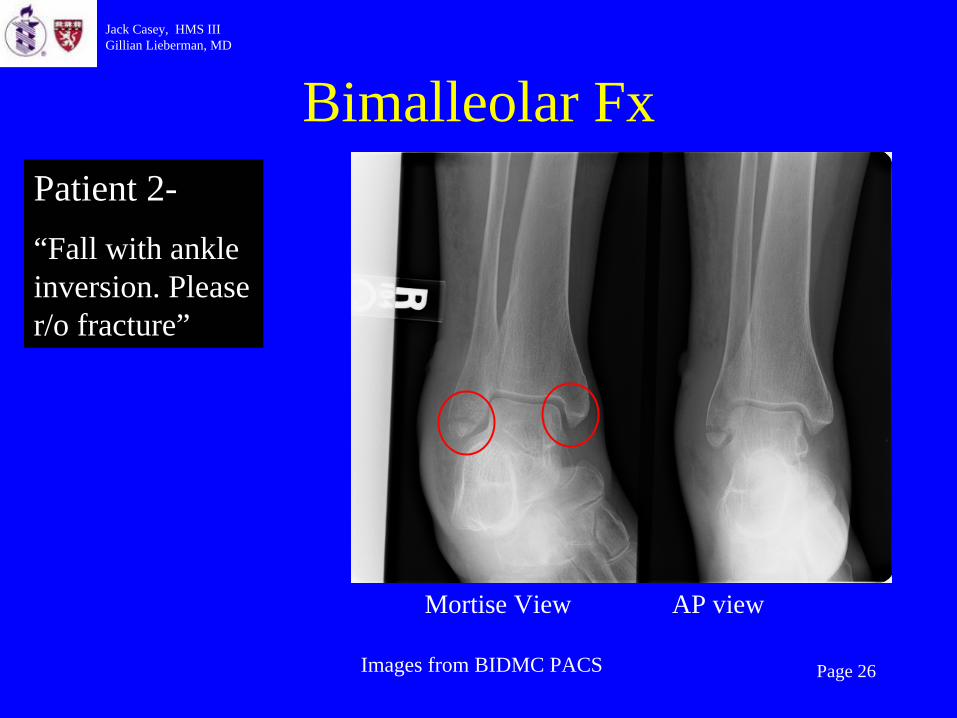
Bimalleolar FxPatient 2-“Fall with ankle inversion. Please r/o fracture”
Images from BIDMC PACS
Mortise View AP view

Jack Casey, HMS III Gillian Lieberman, MD
Page 27
Trimalleolar FxPatient 3-“Eversion injury. r/o fx” (ED films)
Images from BIDMC PACS

Jack Casey, HMS III Gillian Lieberman, MD
Page 28
Trimalleolar Fx ORIF
Images from BIDMC PACS
Patient 3 (Intra-op)
Jack Casey, HMS III Gillian Lieberman, MD
Page 29
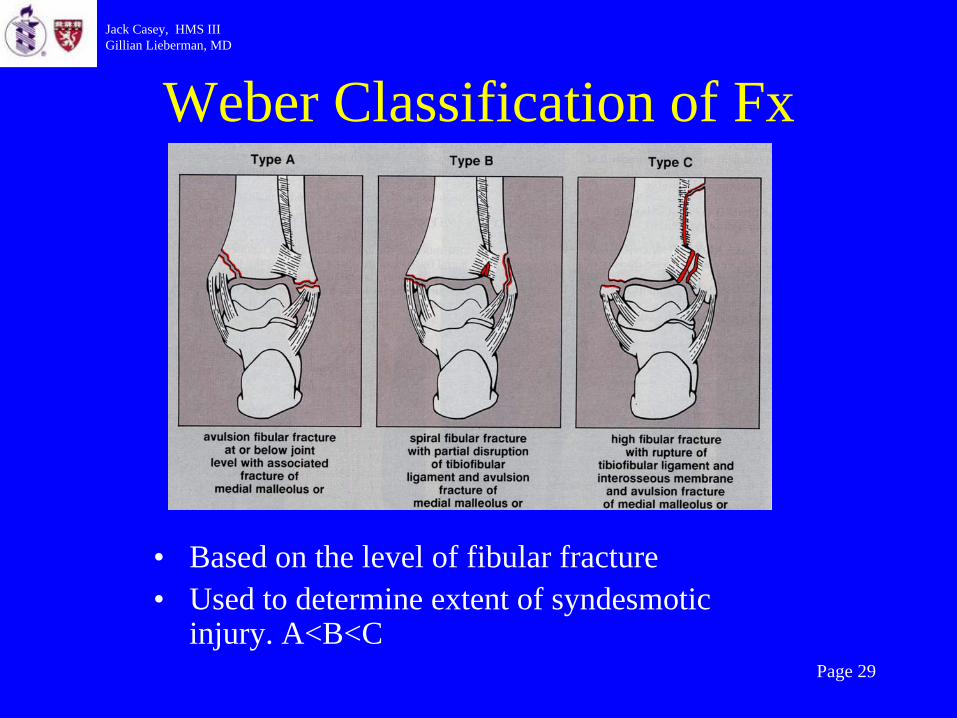
Weber Classification of Fx
• Based on the level of fibular fracture• Used to determine extent of syndesmotic
injury. A<B<C
Jack Casey, HMS III Gillian Lieberman, MD
Page 30
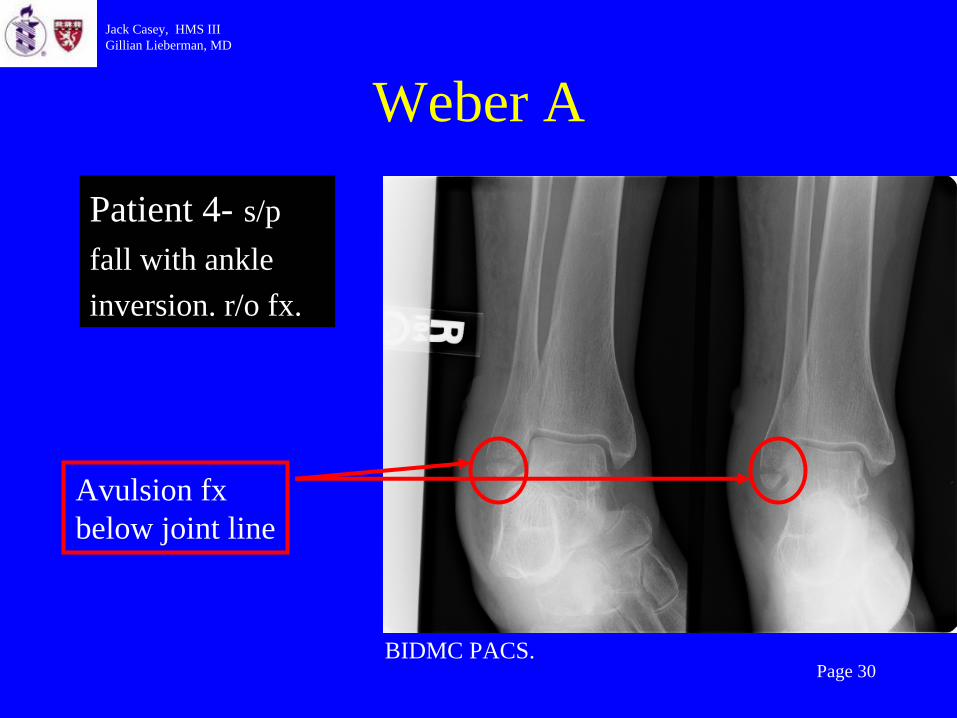
Weber A
Patient 4- s/pfall with ankleinversion. r/o fx.
BIDMC PACS.
Avulsion fx below joint line
Jack Casey, HMS III Gillian Lieberman, MD
Page 31
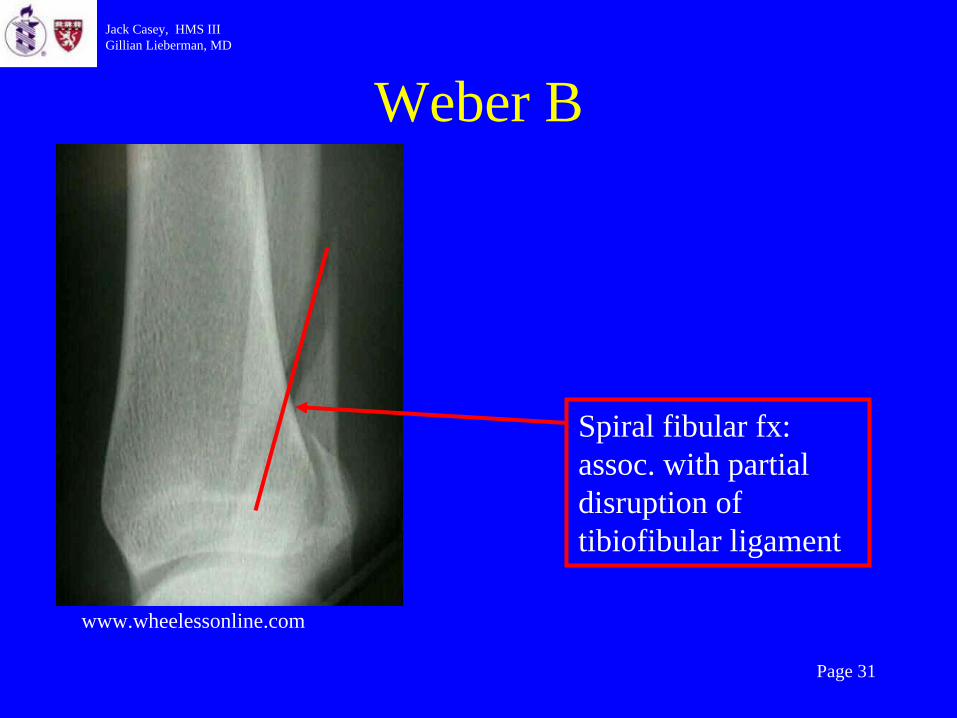
Weber B
www.wheelessonline.com
Spiral fibular fx: assoc. with partial disruption of tibiofibular ligament

Jack Casey, HMS III Gillian Lieberman, MD
Page 32
Weber C
How would you classify anatomically?
Patient 6—“s/p ankle trauma r/o fx”
Bimalleolar (comminuted)
BIDMC PACS.

Jack Casey, HMS III Gillian Lieberman, MD
Page 33
Recap of Classifications
• Anatomic- Uni/ Bi/ Tri Malleolar
• Weber- A/ B/ C

Jack Casey, HMS III Gillian Lieberman, MD
Page 34
Fracture 5th Metatarsal
BIDMC PACS
Patient 7—“s/p ankle inversion injury. r/o fx”

Jack Casey, HMS III Gillian Lieberman, MD
Page 35
Fracture 5th Metatarsal
Mechanism of Injury

Jack Casey, HMS III Gillian Lieberman, MD
Page 36
Beyond Simple Radiographs
If pain persists in 6-8 weeks, consider otherimaging modalities:
- MRI (for evaluation of ligaments/ tendons)- CT
Jack Casey, HMS III Gillian Lieberman, MD
Page 37
Summary
• Indications for RadiographsOttawa Ankle Rules:
o 4 sites for bony tenderness, 4 stepso Save time, money, and avoid radiation exposure, without
sacrificing quality
• Appropriate views, ROI• Think about anatomy• Always look for additional fx

Jack Casey, HMS III Gillian Lieberman, MD
Page 38
Acknowledgements
• Gillian Lieberman, MD• Pamela Lepkowski• Mary Hochman, MD• Larry Barbaras

Jack Casey, HMS III Gillian Lieberman, MD
Page 39
References• American College of Radiology. ACR appropriateness criteria. Imaging evaluation of
suspected ankle fractures. www.acr.org• Anis AH et al. Cost-effectiveness analysis of the Ottawa Ankle Rules. Annals of
emergency medicine. 1995.; 26:422-428.• Bachmann, LM et al. Accuracy of Ottawa ankle rules to exlude fractures of the ankle
and the mid-foot: systematic review. BMJ 2003; 326: 417.• Greenspan, A. Orthopedic radiology. A practical approach. Lipincott, Williams and
Williams. Philadelphia, PA. 2000. • Marx: Rosen’s Emergency Medicine. Concepts and clinical practice. Fifth ed. 2002,
Mosby, Inc. • Steill IG et al. Implementation of the Ottawa ankle rules. JAMA 1994; 271: 827-832.• Steill IG et al. Decision rules for the use of radiography in acute ankle injuries.
Refinement and prospective validation. JAMA 1993; 269:1127.• www.aafp.org/afp/20020901/785.html• www.rad.washington.edu• www.x-strap.com/pix/eversion.jpg


















