Radio Logical Reasoning Congenital Sensorineural
4
WS1 AJR:194, March 2010 AJR Integrative Imaging LIFELONG LEARNING FOR RADIOLOGY Radiological Reasoning: Congenital Sensorineural Hearing Loss Nadja Kadom 1 , Raymond W. Sze Keywords: cochlear implant, CT, dysplasia, sensorineural hearing loss DOI:10.2214/AJR.07.7120 Received August 18, 2008 accepted ater revision March 14, 2009 . 1 Both authors: Department o Radiology, Children’s National Medical Center, 111 Michigan Ave., Washington, DC 20010. Address correspondence to N. Kadom ([email protected]). AJR 2010;194:WSXX–WSXX 0361–803X/10/1943–WS1 © American Roentgen Ray Society OBJECTIVE A 12-year-old girl with an outs ide diagnosis of bilateral profound to severe sensorineural hearing loss came to the pediatric hearing and speech center for cochlear implant evaluation. CT evaluation showed bilateral marked vestibu- lar aqueduct enlargement along with bilateral hypoplasia of the cochlea, minor dysplasia of the v estibule s, and bilater- ally underdeveloped lateral semicircular canals. The patient receiv ed a left cochlear implant and is doing well. CONCLUSION CT of the temporal bones is a v aluable tool in the diagnosis and treatment of pediatric congenital sensorineural hearing loss. Ke y functions of the radiolo gist are design of optimal imaging studies for children and in-depth anatomic–patho- logic knowledge for pre- and postsurgical anatomy . Case History A 12-year-old girl presented to the pediatric hearing and speech center for cochlear implant evaluation. The patient had an outside diagnosis of bil ateral profound sensorineural hearing loss. The patient was adopted from China, and no family history was av ailable. The patient was referred for CT of the temporal bones to evaluate the inner ear anatomy . CT CT of the temporal bones showed bilate ral hypoplasia of the cochlea (Fig. 1A) along with bilateral marked vestibular aqueduct enlargements (Fig . 1B), minor dysplasia of the vestibule s (Fig. 1B), and bilaterally underdev eloped lateral semicircular canals (Fig. 1B). Expert Discussion Temporal bone CT is a well-established technique for eval- uation of pediatric hearing loss, generally best suited f or evaluation of trauma and nonacute congenital dysplasias of the otic capsule. For patients under consideration for cochle- ar implantation, the surgeon not only needs to identify con- genital abnormalities (such as coexisting middle ear abnor- malities, type of cochlear abnorma lity , pattern of cochlear ossication, and vestibular aqueduct abnormality) but also a vari ety of anatomic informati on, such as grade of mastoid bone aeration and internal auditory canal size and shape. The information helps in assessing the feasibility of cochlear implant ation, side of implanta tion, modica tion of implan - tation technique, and anticipation of complications. To provide this information to the clinician, a high-reso- lution CT protocol needs to be applied. We perform direct axial-plane imaging through the temporal bone parallel to the hard palate using a bone algorithm, 512 × 512 matrix, and contiguous 0.625-mm sections. At our institution, di- rect coronal imaging is omitted for patients with sensorineu- ral hearing loss to save radiation exposure. Instead, coronal reformatted images are generated. Sensorineural hearing loss is classied into congenital and acquired forms, the latter are further differentiated into sud- den onset and asymmetric presentations and are best evalu- ated with MRI to detect retrocochlear abnormalities, such as tumors of the internal auditory canal or cerebellopontine angle, labyrinthitis, cerebellar infarcts, demyelinating dis- ease, and pachymeningitis, to name a few [1]. About 50% of pediatric patients have a genetic cause for sensorineural hear- ing loss, such as congenital inner ear dysplasia or a syndrome associated with hearing impairment, such as CHARGE (coloboma, heart disease, atresia choanae, retarded growth and development, genital abnormalities, and ear anomalies). Between 20% and 40% of children develop sensorineural hearing loss as a consequence of prenatal injury , such as TORCH (toxoplasmosis, rubella, cytomegalovirus, herpes simplex virus, and congenital syphilis) or postnatal injury, such as meningitis or trauma. In about 30%, the cause of sensorineural hearing loss remains unknown [2]. F or optimal interpretation of high-resolution CT images, the radiologist must have comprehensiv e knowledge of the anatomy of the inner ear structures and the spectrum of pathology that can be encountered [2, 3]. Some inner ear structures require measurements. The most common con- genital inner ear abnormality seen on CT is a large vestibu- lar aqueduct (measuring > 1.5 mm in diameter) (Fig. 2). This is best measured at least 1 mm from the skull base opening (Fig. 3). Another reference for the maximum width of the vestib ular aqueduct is the diameter of the semicircu- lar canals. The vestibule should be smaller than or equal to
Transcript of Radio Logical Reasoning Congenital Sensorineural

8/3/2019 Radio Logical Reasoning Congenital Sensorineural
http://slidepdf.com/reader/full/radio-logical-reasoning-congenital-sensorineural 1/4

8/3/2019 Radio Logical Reasoning Congenital Sensorineural
http://slidepdf.com/reader/full/radio-logical-reasoning-congenital-sensorineural 2/4

8/3/2019 Radio Logical Reasoning Congenital Sensorineural
http://slidepdf.com/reader/full/radio-logical-reasoning-congenital-sensorineural 3/4
AJR:194, March 2010 WS3
Congenital Sensorineal Hearing Loss
(but not larger than) the bone width between the lateral
vestibular wall and the inner wall of the lateral semicircular
canal. The internal auditory canal should be larger than 2
mm; a smaller diameter has been shown to adversely impact
the long-term outcome with cochlear implantation. A small
internal auditory canal can indicate absence or small size of
the cochlear nerve, which is best further evaluated with
MRI [4, 5] (Fig. 4).
Some controversy exists about the classication of coch-
leovestibular malformations [6]. Especially the widespread
use of the term “Mondini malformation” has been subjectto scientic debate and has been differentiated into two
types of incomplete partitioning (IP), IP-I and IP-II. The
following classication and denitions have been proposed
by Sennaroglu and Saatci [6], listed here in descending or-
der of severity: labyrinthine aplasia, “Michel deformity,”
no inner ear structures have formed; cochlear aplasia, ab-
sence of cochlea; common cavity, single cavity of cochlea
and vestibule; IP-I, cystic cochlea and cystic vestibule; co-
chlear hypoplasia and cochlea with less than 2.5 turns (Fig.
5); and IP-II, Mondini deformity, incomplete partition be-
tween the middle and apical turns of the cochlea forming a
cystic apex, normal basal turn, large vestibular aqueduct,
and enlarged vestibule (Fig. 1).The correct identication of inner ear pathology helps
assessment for contraindications to cochlear implantation
A
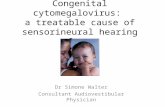
Fig. 5—Companion case in 2-year-old girl withhypoplastic cochlea.A, High-resolution CT image reormatted in coronalplane at level o cochlea shows hypoplastic rightbasal turn o cochlea (arrow ); middle and apical turnshave not ormed.B, High-resolution CT image reormatted in coronalplane at level o cochlea in healthy 3 -year-old boy isshown or comparison.
B
A
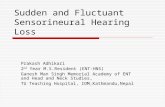
Fig. 4—Companion case in 5-year-old girl withhypoplastic internal auditory canal.A–C, Axial FIESTA (ast imaging employing steady-state acquisition) MR image (A) and sagittalreormations perpendicular to long axis o internalauditory canal (B and C). In axial FIESTA MR image,note abnormally small size o right internal auditorycanal compared with let (1.8 vs 3.2 mm). Sagittalreormation on right (B) shows absence o cochlear
nerve in expected anterior inerior location (arrow, B) as seen on contralateral side (long arrow, C). Notecranial nerve 7 normally visualized on let side inanterior superior portion o internal auditory canal(arrowhead, C) and normal superior and ineriorvestibular nerves posteriorly (small arrows, C).
CB

8/3/2019 Radio Logical Reasoning Congenital Sensorineural
http://slidepdf.com/reader/full/radio-logical-reasoning-congenital-sensorineural 4/4
Kadom and Sze
WS4 AJR:194, March 2010
and improves surgical planning. Successful cochlear implant
function requires functionality of the cochlear nerve and at
least some residual auditory cells. A small internal auditory
canal seen on CT can be an indirect sign of cochlear nerve
absence or hypoplasia, as conrmed by Glastonbury et al.
[7] by MRI correlation. However, deciency of the cochlear
nerve can exist in the setting of a normal size internal audi-tory canal, probably due to an insult that occurs after for-
mation is complete [7]. Some authors prefer high-resolution
MRI over high-resolution CT because it simultaneously
provides information about cochlear patency and presence
and size of the cochlear nerve [4]. Absence of the cochlea
and labyrinthine (Michel) aplasia are contraindications for
cochlear implant surgery. Cochlear dysplasia, although it
limits full insertion of the implant electrodes, still will yield
benet to the patient because of the residual auditory cells
present. Precise radiologic information also affects surgical
planning. For example, in the presence of a dysplastic co-
chlea there may also be a thinner barrier between the co-
chlea and subarachnoid space, which increases the risk of CSF leak, intracranial electrode insertion, and meningitis.
However, this can be surgically addressed by choosing an
appropriate electrode and imaging conrmation of correct
placement. CSF leak requires packing of the cochleostomy
site. Description of facial nerve position is important be-
cause an aberrant position may pose an increased risk of
facial nerve injury and requires more careful surgical tech-
nique and facial nerve monitoring [8].
Clinical ManagementThe audiology assessment showed bilateral moderate to
profound sensorineural hearing loss, left worse than right. The
patient received bilateral temporary hearing aids to bridge thetime to cochlear implantation. Extensive speech and language
testing was performed preoperatively and showed the patient
had a good foundation for auditory skills. The patient received
a left cochlear implant and postoperative follow-up implant
mapping showed excellent acoustic benet.
CommentaryThe incidence of sensorineural hearing loss in children is
about one in 1,000. Today, screening tests as part of new-
born evaluations facilitate the early detection of congenital
hearing impairment [9]. Cochlear implants bypass inner ear
dysfunction from structural abnormalities by direct elec-
trode activation of auditory nerve bers that reside in thecochlea with an electrode, thus improving hearing and sub-
sequent speech development [9]. There is emerging knowl-
edge that bilateral cochlear implants are benecial for de-
velopment of 3D sound localization when implanted within
the rst 3 years of life [9].
High-resolution CT plays a vital role in the diagnosis of
congenital sensorineural hearing loss and helps with surgical
decision making and planning, as discussed earlier. However,
additional imaging techniques are used in the pre- and post-operative evaluation of cochlear implant patients, and there
are additional applications for CT of the temporal bones in
this patient group. For example, it has been shown that pre-
operative functional studies of auditory response with MRI,
PET, or SPECT can provide useful information on brain ac-
tivity response to auditory stimuli. This, in turn, can help in
deciding the side of a single cochlear implant and help pre-
dict functional outcome after implantation [4]. Given that
most implant devices are not compatible with magnetic eld
exposure, the preferred methods for postoperative functional
auditory assessment are PET and SPECT [4]. CT can play an
additional role in postoperative assessment of the electrode
position [10]. Modern imaging protocols, such as BrainLab(BrainLAB), can be used for 3D planning of minimally inva-
sive surgery, using the imaging data to plan a drill path. Fur-
ther studies using this technique are under way at the Na-
tional Institutes of Health [11].
References1. St. Martin MB, Hirsch BE. Imaging o hearing loss. Otolaryngol Clin North
Am 2008; 41:157–178 [vi-vii]
2. Lowe LH, Vézina LG. Sensorineural hearing loss in children. RadioGraphics
1997; 17:1079–1093
3. Som PM, Curtin HD. Head and neck imaging, 4th ed. St Louis, MO: Mosby,
2003
4. Pappas DG Jr, Curé JK. Diagnostic imaging. Otolaryngol Clin North Am 2002;
35:1317–1363 [ix]
5. Wu CC, Lee YC, Chen PJ, Hsu CJ. Predominance o genetic diagnosis and
imaging results as predictors in determining the speech perception perormance
outcome ater cochlear implantation in children. Arch Pediatr Adolesc Med
2008; 162:269–276
6. Sennaroglu L, Saatci I. A new classifcation or cochleovestibular malorma-
tions. Laryngoscope 2002; 112:2230–2241
7. Glastonbury CM, Davidson HC, Harnsberger HR, Butler J, Kertesz TR, Shel-
ton C. Imaging fndings o cochlear nerve defciency. AJNR 2002; 23:635–643
8. Francis HW, Niparko JK. Cochlear implantation update. Pediatr Clin North Am
2003; 50:341–361 [viii]
9. O’Leary S, Chang A. Hearing impairment: technological advances and in-
sights. Aust Fam Physician 2008; 37:322–327
10. Verbist BM, Frijns JH, Geleijns J, van Buchem MA. Multisection CT as a valu-
able tool in the postoperative assessment o cochlear implant patients. AJNR
2005; 26:424–429
11. Labadie RF, Noble JH, Dawant BM, Balachandran R, Majdani O, Fitzpatrick JM. Clinical validation o percutaneous cochlear implant surgery: initial report.
Laryngoscope 2008; 118:1031–1039
F O R Y O U R I N F O R M A T I O N
The reader’s attention is directed to the Self-Assessment Module for this article, which appears on page S4.