Racine County CBRF Provider Inspection Summary
55
DEPARTMENT OF HEALTH SERVICES Division of Quality Assurance Printed 09/22/2021 STATE OF WISCONSIN Bureau of Assisted Living P.O. Box 7940 Madison WI 53707-7940 Provider Inspection Summary For the period 08/24/2018 to 08/23/2021 Notes This report includes Provider Inspection Summaries (Facility Profiles) for Community-Based Residential Facilities in Racine County. The report is a PDF (Adobe Acrobat) document and includes a total of 55.00 pages. If you wish to read the profile for a particular facility without scrolling through the rest of the document, use the Search feature in the Acrobat Reader to specify part of the name of the facility you wish to review. If you wish to print the profile for a particular facility, be sure to send only the desired pages to your computer printer. Otherwise you will be printing all pages in the document.
Transcript of Racine County CBRF Provider Inspection Summary
DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Notes
This report includes Provider Inspection Summaries (Facility Profiles) for Community-Based Residential Facilities in Racine County.The report is a PDF (Adobe Acrobat) document and includes a total of 55.00 pages. If you wish to read the profile for a particularfacility without scrolling through the rest of the document, use the Search feature in the Acrobat Reader to specify part of the name of the facility you wish to review.If you wish to print the profile for a particular facility, be sure to send only the desired pages to your computer printer. Otherwise you will be printing all pages in the document.

DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Facility Information
Facility Name: ARBOR VIEW COMMUNITIES (0017134)
Address: 34201 ARBOR LN, BURLINGTON, WI 53105
License Status: REGULAR
Licensed/Certified/Registered 06/22/2018 12:00:00AM
Regional Office: SOUTHEASTERN REGION (MILWAUKEE), (414) 227-2005
Survey History
Type: OTHER Purpose: SELF REPORT/VVSurvey ID: 0136353 End Date: 04/27/2021
Results: NO STATEMENT OF DEFICIENCY ISSUED
Type: STANDARD Purpose: SURVEY/COMPLAINTSurvey ID: 0135646 End Date: 02/04/2021
Results: ENFORCEMENT ACTION
Statement of Deficiency: #VRL411 Served 02/18/2021
Deficiencies Cited Subject Area CorrectedCompliance
VerifiedYes83.17(1) LICENSEE CONDUCT CAREGIVER
BACKGROUND CHECK4/27/21
Yes83.37(2)(d) DOCUMENTATION OF MEDICATION ADMINISTRATION
4/27/21
Yes83.38(1)(b) SUPERVISION 4/27/21Yes83.38(1)(g) HEALTH MONITORING 4/27/21
This is Page 2 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.

DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Type: STANDARD Purpose: SURVEY/COMPLAINTSurvey ID: 0129962 End Date: 03/06/2019
Results: STATEMENT OF DEFICIENCY ISSUED
Statement of Deficiency: #96WM11
Deficiencies Cited Subject Area CorrectedCompliance
VerifiedYes83.37(1)(j) PROOF-OF-USE RECORD 5/6/19
Enforcement History (ARBOR VIEW COMMUNITIES--0017134)
Date: 02/18/2021 SOD #VRL411 Appealed:
SanctionsORDER TO COMPLYFORFEITURE---83.38(1)(b)FORFEITURE---83.38(1)(g)
Complaint History (ARBOR VIEW COMMUNITIES--0017134)
Date Complaint Received: 12/30/2020 Date Investigation Completed: 02/04/2021
Subject Area(s) Result SOD #PROGRAM SERVICES NOT SUBSTANTIATED
This is Page 3 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.

DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Facility Information
Facility Name: ARBOR VIEW MEMORY CARE (0017133)
Address: 34111 ARBOR LN, BURLINGTON, WI 53105
License Status: REGULAR
Licensed/Certified/Registered 06/22/2018 12:00:00AM
Regional Office: SOUTHEASTERN REGION (MILWAUKEE), (414) 227-2005
Survey History
Type: OTHER Purpose: COMPLAINTSurvey ID: 0129225 End Date: 11/02/2019
Results: NO STATEMENT OF DEFICIENCY ISSUED
Type: STANDARD Purpose: SURVEY/COMPLAINTSurvey ID: 0130019 End Date: 03/04/2019
Results: STATEMENT OF DEFICIENCY ISSUED
Statement of Deficiency: #3V9T11
Deficiencies Cited Subject Area CorrectedCompliance
VerifiedYes83.37(1)(j) PROOF-OF-USE RECORD 5/6/19
This is Page 4 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.
DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Complaint History (ARBOR VIEW MEMORY CARE--0017133)
Date Complaint Received: 12/18/2018 Date Investigation Completed: 03/04/2019
Subject Area(s) Result SOD #PHYSICAL ENVIRONMENT/SAFETY NOT SUBSTANTIATED
3V9T11STAFF TRAINING AND PROFICIENCY SUBSTANTIATED
Date Complaint Received: 09/28/2018 Date Investigation Completed: 11/02/2018
Subject Area(s) Result SOD #STAFF TRAINING AND PROFICIENCY NOT SUBSTANTIATED
This is Page 5 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.
DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Facility Information
Facility Name: CALEBRIA HOUSE (0015143)
Address: 155 BETH COURT, BURLINGTON, WI 53105
License Status: REGULAR
Licensed/Certified/Registered 08/01/2015 12:00:00AM
Regional Office: SOUTHEASTERN REGION (MILWAUKEE), (414) 227-2005
This is Page 6 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.

DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Facility Information
Facility Name: HIL HILLSIDE (0009760)
Address: 373 CHURCH ST, BURLINGTON, WI 53105
License Status: REGULAR
Licensed/Certified/Registered 01/01/2002 12:00:00AM
Regional Office: SOUTHEASTERN REGION (MILWAUKEE), (414) 227-2005
Survey History
Type: ABBREVIATED Purpose: SURVEY/COMPLAINTSurvey ID: 0136549 End Date: 04/13/2021
Results: ENFORCEMENT ACTION
Statement of Deficiency: #4DXC11 Served 06/21/2021
Deficiencies Cited Subject Area CorrectedCompliance
Verified83.46(4)(c) ELECTRICAL PROTECTION
Type: OTHER Purpose: DESK REVIEWSurvey ID: 0133262 End Date: 04/20/2020
Results: NO STATEMENT OF DEFICIENCY ISSUED
Type: OTHER Purpose: COMPLAINTSurvey ID: 0132256 End Date: 12/09/2019
Results: NO STATEMENT OF DEFICIENCY ISSUED
This is Page 7 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.
DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
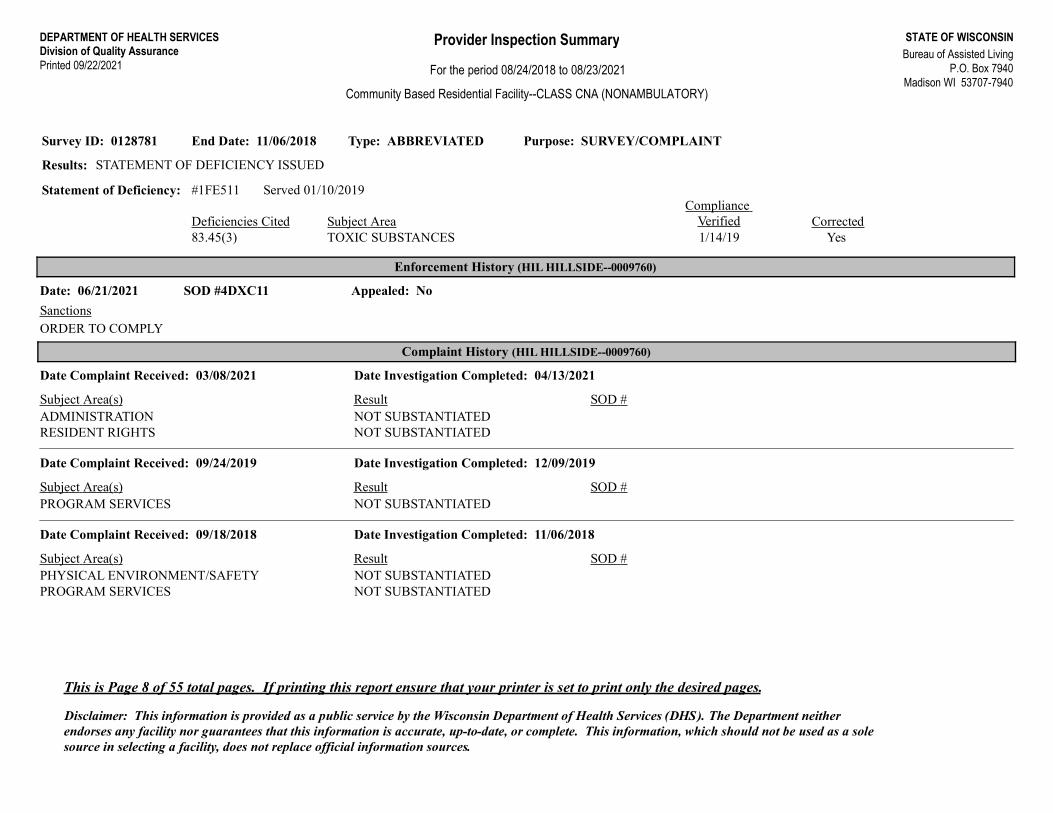
Type: ABBREVIATED Purpose: SURVEY/COMPLAINTSurvey ID: 0128781 End Date: 11/06/2018
Results: STATEMENT OF DEFICIENCY ISSUED
Statement of Deficiency: #1FE511 Served 01/10/2019
Deficiencies Cited Subject Area CorrectedCompliance
VerifiedYes83.45(3) TOXIC SUBSTANCES 1/14/19
Enforcement History (HIL HILLSIDE--0009760)
Date: 06/21/2021 SOD #4DXC11 Appealed: No
SanctionsORDER TO COMPLY
Complaint History (HIL HILLSIDE--0009760)
Date Complaint Received: 03/08/2021 Date Investigation Completed: 04/13/2021
Subject Area(s) Result SOD #ADMINISTRATION NOT SUBSTANTIATEDRESIDENT RIGHTS NOT SUBSTANTIATED
Date Complaint Received: 09/24/2019 Date Investigation Completed: 12/09/2019
Subject Area(s) Result SOD #PROGRAM SERVICES NOT SUBSTANTIATED
Date Complaint Received: 09/18/2018 Date Investigation Completed: 11/06/2018
Subject Area(s) Result SOD #PHYSICAL ENVIRONMENT/SAFETY NOT SUBSTANTIATEDPROGRAM SERVICES NOT SUBSTANTIATED
This is Page 8 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.
DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Facility Information
Facility Name: HIL KENDRICK HOME (0010610)
Address: 265 N KENDRICK AVE, BURLINGTON, WI 53105
License Status: REGULAR
Licensed/Certified/Registered 02/01/2006 12:00:00AM
Regional Office: SOUTHEASTERN REGION (MILWAUKEE), (414) 227-2005
Survey History
Type: OTHER Purpose: COMPLAINTSurvey ID: 0136572 End Date: 06/10/2021
Results: NO STATEMENT OF DEFICIENCY ISSUED
Type: STANDARD Purpose: SURVEYSurvey ID: 0135179 End Date: 11/12/2020
Results: NO STATEMENT OF DEFICIENCY ISSUED
Complaint History (HIL KENDRICK HOME--0010610)
Date Complaint Received: 09/24/2019 Date Investigation Completed: 06/10/2021
Subject Area(s) Result SOD #RESIDENT RIGHTS NOT SUBSTANTIATED
This is Page 9 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.
DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Facility Information
Facility Name: HIL WANDA FROGG VILLA/MEADOWHAVEN (0012315)
Address: 524 SUMMIT AVE, BURLINGTON, WI 53105
License Status: REGULAR
Licensed/Certified/Registered 12/01/2008 12:00:00AM
Regional Office: SOUTHEASTERN REGION (MILWAUKEE), (414) 227-2005
This is Page 10 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.

DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Facility Information
Facility Name: OAK PARK PLACE OF BURLINGTON (0016395)
Address: 1700 TEUT RD, BURLINGTON, WI 53105
License Status: REGULAR
Licensed/Certified/Registered 03/14/2017 12:00:00AM
Regional Office: SOUTHEASTERN REGION (MILWAUKEE), (414) 227-2005
Survey History
No survey activity during the period 8/24/18 to 8/23/21
This is Page 11 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.

DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Facility Information
Facility Name: PINE BROOK POINTE (0008582)
Address: 1001 S PINE ST, BURLINGTON, WI 53105
License Status: REGULAR
Licensed/Certified/Registered 02/01/2000 12:00:00AM
Regional Office: SOUTHEASTERN REGION (MILWAUKEE), (414) 227-2005
Survey History
Type: OTHER Purpose: COMPLAINT/VVSurvey ID: 0135908 End Date: 03/23/2021
Results: NO STATEMENT OF DEFICIENCY ISSUED
Type: OTHER Purpose: COMPLAINT/VVSurvey ID: 0134994 End Date: 09/08/2020
Results: ENFORCEMENT ACTION
Statement of Deficiency: #TMXW12 Served 10/22/2020
Deficiencies Cited Subject Area CorrectedCompliance
VerifiedYes83.32(3)(i) RIGHTS OF RESIDENTS: PROMPT AND
ADEQUATE TREATMENT3/23/21
Yes83.35(1)(c) LISTED AREAS FOR ASSESSMENTS 3/23/21Yes83.47(2)(d) FIRE DRILLS 3/23/21Yes83.47(2)(e) OTHER EVACUATION DRILLS 3/23/21
This is Page 12 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.
DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Type: STANDARD Purpose: SURVEY/COMPLAINTSurvey ID: 0133141 End Date: 10/15/2019
Results: ENFORCEMENT ACTION
Statement of Deficiency: #TMXW11 Served 04/06/2020
Deficiencies Cited Subject Area CorrectedCompliance
VerifiedYes50.065(2)(bm) OUT OF STATE BACKGROUND CHECKS 9/3/20Yes83.35(5)(b) ANNUAL EVALUATION OF EVACUATION
LIMITS9/3/20
Yes83.45(3) TOXIC SUBSTANCES 9/3/20No83.47(2)(d) FIRE DRILLS 9/3/20No83.47(2)(e) OTHER EVACUATION DRILLS 9/3/20
Enforcement History (PINE BROOK POINTE--0008582)
Date: 10/22/2020 SOD #TMXW12 Appealed:
SanctionsOTHER SANCTIONFORFEITURE---83.32(3)(i)FORFEITURE---83.35(1)(c)
Date: 04/06/2020 SOD #TMXW11 Appealed:
SanctionsCOMPLY WITH DEPARTMENT PLAN OF CORRECTIONCOMPLY WITH REQUIREMENTFORFEITURE---83.47(2)(d) 2nd cite
This is Page 13 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.

DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Complaint History (PINE BROOK POINTE--0008582)
Date Complaint Received: 12/21/2020 Date Investigation Completed: 03/23/2021
Subject Area(s) Result SOD #PHYSICAL ENVIRONMENT/SAFETY NOT SUBSTANTIATED
Date Complaint Received: 08/12/2020 Date Investigation Completed: 09/08/2020
Subject Area(s) Result SOD #PROGRAM SERVICES NOT SUBSTANTIATEDRESIDENT RIGHTS NOT SUBSTANTIATED
Date Complaint Received: 07/09/2020 Date Investigation Completed: 09/08/2020
Subject Area(s) Result SOD #RESIDENT RIGHTS NOT SUBSTANTIATEDPROGRAM SERVICES NOT SUBSTANTIATED
Date Complaint Received: 05/03/2020 Date Investigation Completed: 09/08/2020
Subject Area(s) Result SOD #PROGRAM SERVICES NOT SUBSTANTIATEDSTAFF TRAINING AND PROFICIENCY NOT SUBSTANTIATED
Date Complaint Received: 04/30/2020 Date Investigation Completed: 09/09/2020
Subject Area(s) Result SOD #TMXW12ADMINISTRATION SUBSTANTIATEDTMXW12PROGRAM SERVICES SUBSTANTIATEDTMXW12STAFF TRAINING AND PROFICIENCY SUBSTANTIATED
This is Page 14 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.

DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Facility Information
Facility Name: PARKVIEW GARDENS III (0016971)
Address: 5321 DOUGLAS AVE, CALEDONIA, WI 53402
License Status: REGULAR
Licensed/Certified/Registered 06/04/2018 12:00:00AM
Regional Office: SOUTHEASTERN REGION (MILWAUKEE), (414) 227-2005
Survey History
Type: STANDARD Purpose: SURVEY/VVSurvey ID: 0136646 End Date: 02/09/2021
Results: STATEMENT OF DEFICIENCY ISSUED
Statement of Deficiency: #T9QF12 Served 06/30/2021
Deficiencies Cited Subject Area CorrectedCompliance
VerifiedYes83.44(1)(c) CLOTHES DRYERS ENCLOSED AND VENTED 8/16/21
Type: OTHER Purpose: COMPLAINTSurvey ID: 0135034 End Date: 09/16/2020
Results: ENFORCEMENT ACTION
Statement of Deficiency: #T9QF11 Served 10/28/2020
Deficiencies Cited Subject Area CorrectedCompliance
VerifiedYes83.38(1)(b) SUPERVISION 2/8/21
Type: STANDARD Purpose: SURVEYSurvey ID: 0130356 End Date: 03/25/2019
Results: NO STATEMENT OF DEFICIENCY ISSUED
This is Page 15 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.
DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Enforcement History (PARKVIEW GARDENS III--0016971)
Date: 10/28/2020 SOD #T9QF11 Appealed:
SanctionsOTHER SANCTIONFORFEITURE---83.38(1)(b)
Complaint History (PARKVIEW GARDENS III--0016971)
Date Complaint Received: 07/30/2020 Date Investigation Completed: 09/16/2020
Subject Area(s) Result SOD #T9QF11ADMINISTRATION SUBSTANTIATEDT9QF11RESIDENT RIGHTS SUBSTANTIATED
Date Complaint Received: 08/22/2019 Date Investigation Completed: 09/16/2020
Subject Area(s) Result SOD #PROGRAM SERVICES NOT SUBSTANTIATED
This is Page 16 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.
DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Facility Information
Facility Name: WOODS OF CALEDONIA (0018358)
Address: 5737 ERIE STREET, CALEDONIA, WI 53402
License Status: PROBATIONARY
Licensed/Certified/Registered 01/16/2021 12:00:00AM
Regional Office: SOUTHEASTERN REGION (MILWAUKEE), (414) 227-2005
Survey History
Type: STANDARD Purpose: SURVEY/COMPLAINTSurvey ID: 0136907 End Date: 07/09/2021
Results: ENFORCEMENT ACTION
Statement of Deficiency: #2Z4I11 Served 08/05/2021
Deficiencies Cited Subject Area CorrectedCompliance
Verified83.12(6) DOCUMENTATION REQUIREMENTS FOR
WRITTEN REPORT83.17(2)(a) EMPLOYEES SCREENED FOR COMMUNICABLE
DISEASE83.18(1) EMPLOYEE RECORDS MAINTAINED AND
CURRENT83.20(1)(a) TRAINING TO BE DEPARTMENT APPROVED83.28(4)(a) RESIDENT HEALTH SCREENING AND
DOCUMENTATION83.37(1)(g) DISPOSITION OF MEDICATIONS83.37(2)(d) DOCUMENTATION OF MEDICATION
ADMINISTRATION83.43(1) ENVIRONMENT SAFE, CLEAN, AND
COMFORTABLE83.47(2)(d) FIRE DRILLS
This is Page 17 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.
DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
83.47(2)(e) OTHER EVACUATION DRILLS
Type: OTHER Purpose: COMPLAINTSurvey ID: 0136574 End Date: 05/25/2021
Results: NO STATEMENT OF DEFICIENCY ISSUED
Enforcement History (WOODS OF CALEDONIA--0018358)
Date: 08/05/2021 SOD #2Z4I11 Appealed: No
SanctionsORDER TO COMPLY
This is Page 18 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.
DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Complaint History (WOODS OF CALEDONIA--0018358)
Date Complaint Received: 06/09/2021 Date Investigation Completed: 07/09/2021
Subject Area(s) Result SOD #2Z4I11PROGRAM SERVICES SUBSTANTIATED
Date Complaint Received: 05/14/2021 Date Investigation Completed: 05/25/2021
Subject Area(s) Result SOD #ADMINISTRATION NOT SUBSTANTIATEDSTAFF TRAINING AND PROFICIENCY NOT SUBSTANTIATED
Date Complaint Received: 05/03/2021 Date Investigation Completed: 05/25/2021
Subject Area(s) Result SOD #ADMINISTRATION NOT SUBSTANTIATEDSTAFF TRAINING AND PROFICIENCY NOT SUBSTANTIATED
Date Complaint Received: 04/30/2021 Date Investigation Completed: 05/25/2021
Subject Area(s) Result SOD #STAFF TRAINING AND PROFICIENCY NOT SUBSTANTIATED
Date Complaint Received: 03/08/2021 Date Investigation Completed: 05/25/2021
Subject Area(s) Result SOD #PROGRAM SERVICES NOT SUBSTANTIATEDPROGRAM SERVICES NOT SUBSTANTIATED
This is Page 19 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.

DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Date Complaint Received: 02/16/2021 Date Investigation Completed: 05/25/2021
Subject Area(s) Result SOD #RESIDENT RIGHTS NOT SUBSTANTIATEDPHYSICAL ENVIRONMENT/SAFETY NOT SUBSTANTIATEDPROGRAM SERVICES NOT SUBSTANTIATEDRESIDENT RIGHTS NOT SUBSTANTIATEDSTAFF TRAINING AND PROFICIENCY NOT SUBSTANTIATEDRESIDENT RIGHTS NOT SUBSTANTIATEDRESIDENT RIGHTS NOT SUBSTANTIATED
This is Page 20 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.

DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Facility Information
Facility Name: MAGNOLIA HILL - MT PLEASANT C CBRF (0017186)
Address: 3820 OLD GREEN BAY RD, MOUNT PLEASANT, WI 53403
License Status: REGULAR
Licensed/Certified/Registered 06/27/2018 12:00:00AM
Regional Office: SOUTHEASTERN REGION (MILWAUKEE), (414) 227-2005
Survey History
Type: OTHER Purpose: COMPLAINT/VVSurvey ID: 0135576 End Date: 02/08/2021
Results: NO STATEMENT OF DEFICIENCY ISSUED
Type: STANDARD Purpose: SURVEY/COMPLAINTSurvey ID: 0134813 End Date: 08/27/2020
Results: ENFORCEMENT ACTION
Statement of Deficiency: #HSH911 Served 09/15/2020
Deficiencies Cited Subject Area CorrectedCompliance
VerifiedYes83.35(3)(d) SERVICE PLANS UPDATED ANNUALLY OR ON
CHANGES2/8/21
Yes83.37(1)(e) MEDICATION REGIMEN, ADMINISTRATION REVIEW
2/8/21
Yes83.37(1)(h) SCHEDULED PSYCHOTROPIC MEDICATIONS 2/8/21Yes83.37(1)(i) PRN PSYCHOTROPIC MEDICATION 2/8/21Yes83.47(2)(d) FIRE DRILLS 2/8/21Yes83.47(2)(e) OTHER EVACUATION DRILLS 2/8/21Yes83.48(1)(b) SMOKE AND HEAT DETECTORS PER NFPA 72 2/8/21Yes83.48(3)(a) FIRE DETECTION SYSTEMS INSPECTED
ANNUALLY2/8/21
This is Page 21 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.

DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Type: OTHER Purpose: DESK REVIEWSurvey ID: 0134634 End Date: 01/27/2020
Results: NO STATEMENT OF DEFICIENCY ISSUED
Enforcement History (MAGNOLIA HILL - MT PLEASANT C CBRF--0017186)
Date: 09/14/2020 SOD #HSH911 Appealed:
SanctionsOTHER SANCTIONFORFEITURE---83.37(1)(h)FORFEITURE---83.47(2)(d)FORFEITURE---83.47(2)(e)FORFEITURE---83.48(3)(a)
Complaint History (MAGNOLIA HILL - MT PLEASANT C CBRF--0017186)
Date Complaint Received: 10/20/2020 Date Investigation Completed: 02/08/2021
Subject Area(s) Result SOD #RESIDENT RIGHTS NOT SUBSTANTIATED
Date Complaint Received: 02/11/2020 Date Investigation Completed: 08/19/2020
Subject Area(s) Result SOD #ADMINISTRATION NOT SUBSTANTIATEDPROGRAM SERVICES NOT SUBSTANTIATED
This is Page 22 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.

DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Facility Information
Facility Name: MAGNOLIA HILL MOUNT PLEASANT A L MEMORY CARE D (0017949)
Address: 3810 OLD GREEN BAY ROAD, MOUNT PLEASANT, WI 53403
License Status: REGULAR
Licensed/Certified/Registered 05/01/2021 12:00:00AM
Regional Office: SOUTHEASTERN REGION (MILWAUKEE), (414) 227-2005
Survey History
Type: STANDARD Purpose: VERIFICATION VISITSurvey ID: 0136305 End Date: 05/19/2021
Results: NO STATEMENT OF DEFICIENCY ISSUED
Type: STANDARD Purpose: VERIFICATION VISITSurvey ID: 0135876 End Date: 02/25/2021
Results: ENFORCEMENT ACTION
Statement of Deficiency: #9CX012 Served 03/29/2021
Deficiencies Cited Subject Area CorrectedCompliance
VerifiedYes83.32(3)(h) RIGHTS OF RESIDENTS: TO RECEIVE
MEDICATION5/19/21
This is Page 23 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.
DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Type: STANDARD Purpose: SURVEY/COMPLAINT/SELF REPORTSurvey ID: 0135209 End Date: 10/27/2020
Results: ENFORCEMENT ACTION
Statement of Deficiency: #9CX011 Served 11/24/2020
Deficiencies Cited Subject Area CorrectedCompliance
VerifiedYes83.21(1)-(3) ALL EMPLOYEE TRAINING 2/18/21Yes83.22(1)-(4) TASK SPECIFIC TRAINING 2/18/21No83.32(3)(h) RIGHTS OF RESIDENTS: TO RECEIVE
MEDICATION2/18/21
Yes83.35(2) TEMPORARY SERVICE PLAN 2/18/21
Type: OTHER Purpose: COMPLAINTSurvey ID: 0134748 End Date: 08/27/2020
Results: NO STATEMENT OF DEFICIENCY ISSUED
Type: INITIAL Purpose: SURVEYSurvey ID: 0133612 End Date: 04/02/2020
Results: PROBATIONARY LICENSE ISSUED
Enforcement History (MAGNOLIA HILL MOUNT PLEASANT A L MEMORY CARE D--0017949)
Date: 03/29/2021 SOD #9CX012 Appealed:
SanctionsCOMPLY WITH DEPARTMENT PLAN OF CORRECTIONCOMPLY WITH REQUIREMENTORDER TO COMPLYFORFEITURE---83.32(3)(h)
Date: 11/24/2020 SOD #9CX011 Appealed:
SanctionsORDER TO COMPLYFORFEITURE---83.21(1-3)FORFEITURE---83.22(1)-(4)FORFEITURE---83.32(3)(h)
This is Page 24 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.

DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Complaint History (MAGNOLIA HILL MOUNT PLEASANT A L MEMORY CARE D--0017949)
Date Complaint Received: 07/22/2021 Date Investigation Completed: 08/24/2021
Subject Area(s) Result SOD #RESIDENT RIGHTS NOT SUBSTANTIATED
Date Complaint Received: 10/05/2020 Date Investigation Completed: 10/27/2020
Subject Area(s) Result SOD #PROGRAM SERVICES NOT SUBSTANTIATED
9CX011RESIDENT RIGHTS SUBSTANTIATED
Date Complaint Received: 07/28/2020 Date Investigation Completed: 09/01/2020
Subject Area(s) Result SOD #PHYSICAL ENVIRONMENT/SAFETY NOT SUBSTANTIATEDPROGRAM SERVICES NOT SUBSTANTIATEDRESIDENT RIGHTS NOT SUBSTANTIATEDSTAFF TRAINING AND PROFICIENCY NOT SUBSTANTIATED
This is Page 25 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.

DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Facility Information
Facility Name: MAGNOLIA HILL - MT PLEASANT A CBRF (0017189)
Address: 3820 OLD GREEN BAY RD, MOUNT PLEASANT, WI 53403
License Status: REGULAR
Licensed/Certified/Registered 06/27/2018 12:00:00AM
Regional Office: SOUTHEASTERN REGION (MILWAUKEE), (414) 227-2005
Survey History
Type: OTHER Purpose: COMPLAINT/SELF REPORT/VVSurvey ID: 0136932 End Date: 07/27/2021
Results: NO STATEMENT OF DEFICIENCY ISSUED
Type: OTHER Purpose: COMPLAINT/VVSurvey ID: 0135473 End Date: 01/04/2021
Results: ENFORCEMENT ACTION
Statement of Deficiency: #UETN12 Served 01/25/2021
Deficiencies Cited Subject Area CorrectedCompliance
VerifiedYes83.38(1)(i) BEHAVIOR MANAGEMENT 7/22/21
This is Page 26 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.
DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Type: STANDARD Purpose: SURVEY/COMPLAINTSurvey ID: 0134891 End Date: 08/27/2020
Results: ENFORCEMENT ACTION
Statement of Deficiency: #UETN11 Served 09/28/2020
Deficiencies Cited Subject Area CorrectedCompliance
VerifiedYes83.35(3)(d) SERVICE PLANS UPDATED ANNUALLY OR ON
CHANGES1/6/21
Yes83.37(1)(e) MEDICATION REGIMEN, ADMINISTRATION REVIEW
1/6/21
Yes83.37(1)(h) SCHEDULED PSYCHOTROPIC MEDICATIONS 1/6/21Yes83.37(1)(i) PRN PSYCHOTROPIC MEDICATION 1/6/21Yes83.47(2)(d) FIRE DRILLS 1/6/21Yes83.47(2)(e) OTHER EVACUATION DRILLS 1/6/21Yes83.48(1)(b) SMOKE AND HEAT DETECTORS PER NFPA 72 1/6/21Yes83.48(3)(a) FIRE DETECTION SYSTEMS INSPECTED
ANNUALLY1/6/21
Type: OTHER Purpose: DESK REVIEWSurvey ID: 0134629 End Date: 01/27/2020
Results: NO STATEMENT OF DEFICIENCY ISSUED
Enforcement History (MAGNOLIA HILL - MT PLEASANT A CBRF--0017189)
Date: 01/23/2021 SOD #UETN12 Appealed:
SanctionsORDER TO COMPLYFORFEITURE---83.38(1)(i)
Date: 09/26/2020 SOD #UETN11 Appealed: No
SanctionsOTHER SANCTION
This is Page 27 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.

DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Complaint History (MAGNOLIA HILL - MT PLEASANT A CBRF--0017189)
Date Complaint Received: 02/01/2021 Date Investigation Completed: 07/27/2021
Subject Area(s) Result SOD #ADMINISTRATION NOT SUBSTANTIATEDRESIDENT RIGHTS NOT SUBSTANTIATED
Date Complaint Received: 12/09/2020 Date Investigation Completed: 01/06/2021
Subject Area(s) Result SOD #UETN12PHYSICAL ENVIRONMENT/SAFETY SUBSTANTIATED
PROGRAM SERVICES NOT SUBSTANTIATED
Date Complaint Received: 02/11/2020 Date Investigation Completed: 08/27/2020
Subject Area(s) Result SOD #ADMINISTRATION NOT SUBSTANTIATEDPROGRAM SERVICES NOT SUBSTANTIATED
This is Page 28 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.

DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Facility Information
Facility Name: MAGNOLIA HILL - MT PLEASANT B CBRF (0017188)
Address: 3820 OLD GREEN BAY RD, MOUNT PLEASANT, WI 53403
License Status: REGULAR
Licensed/Certified/Registered 06/27/2018 12:00:00AM
Regional Office: SOUTHEASTERN REGION (MILWAUKEE), (414) 227-2005
Survey History
Type: STANDARD Purpose: SURVEY/COMPLAINTSurvey ID: 0134812 End Date: 08/27/2020
Results: ENFORCEMENT ACTION
Statement of Deficiency: #QH2B11 Served 09/15/2020
Deficiencies Cited Subject Area CorrectedCompliance
Verified83.37(1)(e) MEDICATION REGIMEN, ADMINISTRATION
REVIEW83.47(2)(d) FIRE DRILLS83.47(2)(e) OTHER EVACUATION DRILLS83.48(1)(b) SMOKE AND HEAT DETECTORS PER NFPA 7283.48(3)(a) FIRE DETECTION SYSTEMS INSPECTED
ANNUALLY
Type: OTHER Purpose: DESK REVIEWSurvey ID: 0134636 End Date: 01/27/2020
Results: NO STATEMENT OF DEFICIENCY ISSUED
This is Page 29 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.

DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Enforcement History (MAGNOLIA HILL - MT PLEASANT B CBRF--0017188)
Date: 09/14/2020 SOD #QH2B11 Appealed: Decision: PENDING
SanctionsOTHER SANCTIONFORFEITURE---83.47(2)(d)FORFEITURE---83.47(2)(e)FORFEITURE---83.48(3)(a)
Complaint History (MAGNOLIA HILL - MT PLEASANT B CBRF--0017188)
Date Complaint Received: 02/11/2020 Date Investigation Completed: 08/27/2020
Subject Area(s) Result SOD #ADMINISTRATION NOT SUBSTANTIATEDPROGRAM SERVICES NOT SUBSTANTIATED
This is Page 30 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.

DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Facility Information
Facility Name: PINE VIEW MANOR ASSISTED LIVING LLC (0018002)
Address: 6101 16TH STREET, MOUNT PLEASANT, WI 53406
License Status: PROBATIONARY
Licensed/Certified/Registered 10/29/2020 12:00:00AM
Regional Office: SOUTHEASTERN REGION (MILWAUKEE), (414) 227-2005
Survey History
Type: INITIAL Purpose: SURVEYSurvey ID: 0135189 End Date: 10/29/2020
Results: PROBATIONARY LICENSE ISSUED
This is Page 31 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.
DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Facility Information
Facility Name: NEW VISION HOME LLC II (0014935)
Address: 1449 N GREEN BAY ROAD, MT PLEASANT, WI 53406
License Status: REGULAR
Licensed/Certified/Registered 01/05/2015 12:00:00AM
Regional Office: SOUTHEASTERN REGION (MILWAUKEE), (414) 227-2005
Survey History
Type: ABBREVIATED Purpose: SURVEYSurvey ID: 0129649 End Date: 01/29/2019
Results: NO STATEMENT OF DEFICIENCY ISSUED
This is Page 32 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.
DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CA (AMBULATORY)
Facility Information
Facility Name: OPEN ARMS LINDEN I (0018254)
Address: 9033 LINDEN COURT, STURTEVANT, WI 53177
License Status: REGULAR
Licensed/Certified/Registered 10/14/2020 12:00:00AM
Regional Office: SOUTHEASTERN REGION (MILWAUKEE), (414) 227-2005
Survey History
Type: STANDARD Purpose: SURVEY/COMPLAINTSurvey ID: 0136594 End Date: 05/18/2021
Results: ENFORCEMENT ACTION
Statement of Deficiency: #1DY411 Served 06/25/2021
Deficiencies Cited Subject Area CorrectedCompliance
Verified50.09(1)(n) CARE PLANNING
Type: INITIAL Purpose: SURVEYSurvey ID: 0135012 End Date: 10/13/2020
Results: PROBATIONARY LICENSE ISSUED
Enforcement History (OPEN ARMS LINDEN I--0018254)
Date: 06/25/2021 SOD #1DY411 Appealed: Decision: PENDING
SanctionsORDER TO COMPLYFORFEITURE---50.09(1)(N)
This is Page 33 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.
DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CA (AMBULATORY)
Complaint History (OPEN ARMS LINDEN I--0018254)
Date Complaint Received: 04/29/2021 Date Investigation Completed: 05/18/2021
Subject Area(s) Result SOD #1DY411PROGRAM SERVICES SUBSTANTIATED
This is Page 34 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.

DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CA (AMBULATORY)
Facility Information
Facility Name: OPEN ARMS LINDEN II (0018253)
Address: 9034 LINDEN COURT, STURTEVANT, WI 53177
License Status: REGULAR
Licensed/Certified/Registered 10/14/2020 12:00:00AM
Regional Office: SOUTHEASTERN REGION (MILWAUKEE), (414) 227-2005
Survey History
Type: STANDARD Purpose: SURVEYSurvey ID: 0136349 End Date: 05/18/2021
Results: NO STATEMENT OF DEFICIENCY ISSUED
Type: INITIAL Purpose: SURVEYSurvey ID: 0135016 End Date: 10/13/2020
Results: PROBATIONARY LICENSE ISSUED
This is Page 35 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.
DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS AA (AMBULATORY)
Facility Information
Facility Name: EAGLE HOUSE (310369)
Address: 807 53RD DR, UNION GROVE, WI 53182
License Status: REGULAR
Licensed/Certified/Registered 11/01/1996 12:00:00AM
Regional Office: SOUTHEASTERN REGION (MILWAUKEE), (414) 227-2005
Survey History
Type: OTHER Purpose: COMPLAINTSurvey ID: 0132086 End Date: 11/07/2019
Results: STATEMENT OF DEFICIENCY ISSUED
Statement of Deficiency: #115Z11 Served 12/02/2019
Deficiencies Cited Subject Area CorrectedCompliance
Verified83.12(3)(b) DOCUMENTATION OF INVESTIGATIONS OF
INJURIES
Type: ABBREVIATED Purpose: SURVEY/COMPLAINTSurvey ID: 0128725 End Date: 10/15/2018
Results: NO STATEMENT OF DEFICIENCY ISSUED
Complaint History (EAGLE HOUSE--310369)
Date Complaint Received: 09/16/2019 Date Investigation Completed: 11/07/2019
Subject Area(s) Result SOD #RESIDENT RIGHTS NOT SUBSTANTIATED
This is Page 36 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.
DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Facility Information
Facility Name: TIMBER OAKS (310564)
Address: 1390 8TH AVE, UNION GROVE, WI 53182
License Status: REGULAR
Licensed/Certified/Registered 09/04/1991 12:00:00AM
Regional Office: SOUTHEASTERN REGION (MILWAUKEE), (414) 227-2005
Survey History
Type: OTHER Purpose: COMPLAINTSurvey ID: 0136550 End Date: 06/10/2021
Results: NO STATEMENT OF DEFICIENCY ISSUED
Type: OTHER Purpose: SURVEY/COMPLAINTSurvey ID: 0134572 End Date: 08/18/2020
Results: NO STATEMENT OF DEFICIENCY ISSUED
Complaint History (TIMBER OAKS--310564)
Date Complaint Received: 06/02/2020 Date Investigation Completed: 08/18/2020
Subject Area(s) Result SOD #PROGRAM SERVICES NOT SUBSTANTIATED
This is Page 37 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.

DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Facility Information
Facility Name: HIL FOX MEAD GROUP HOME (0009691)
Address: 516 FOX MEAD CROSSING, WATERFORD, WI 53185
License Status: REGULAR
Licensed/Certified/Registered 01/01/2002 12:00:00AM
Regional Office: SOUTHEASTERN REGION (MILWAUKEE), (414) 227-2005
Survey History
Type: OTHER Purpose: COMPLAINT/VVSurvey ID: 0137208 End Date: 08/17/2021
Results: NO STATEMENT OF DEFICIENCY ISSUED
Type: OTHER Purpose: COMPLAINT/VVSurvey ID: 0133428 End Date: 01/21/2020
Results: ENFORCEMENT ACTION
Statement of Deficiency: #YGZ812 Served 04/30/2020
Deficiencies Cited Subject Area CorrectedCompliance
VerifiedYes83.35(3)(d) SERVICE PLANS UPDATED ANNUALLY OR ON
CHANGES8/17/21
Type: STANDARD Purpose: COMPLAINTSurvey ID: 0131670 End Date: 08/12/2019
Results: ENFORCEMENT ACTION
Statement of Deficiency: #YGZ811 Served 10/09/2019
Deficiencies Cited Subject Area CorrectedCompliance
VerifiedYes83.36(1)(a) ADEQUATE STAFF TO MEET RESIDENT NEEDS 1/21/20
This is Page 38 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.

DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Type: ABBREVIATED Purpose: SURVEY/COMPLAINTSurvey ID: 0128573 End Date: 10/10/2018
Results: NO STATEMENT OF DEFICIENCY ISSUED
Enforcement History (HIL FOX MEAD GROUP HOME--0009691)
Date: 04/29/2020 SOD #YGZ812 Appealed:
SanctionsFORFEITURE---83.35(3)(d)
Date: 10/07/2019 SOD #YGZ811 Appealed:
SanctionsCOMPLY WITH REQUIREMENTFORFEITURE---83.36(1)(a)
This is Page 39 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.

DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Complaint History (HIL FOX MEAD GROUP HOME--0009691)
Date Complaint Received: 03/10/2020 Date Investigation Completed: 08/17/2021
Subject Area(s) Result SOD #PROGRAM SERVICES NOT SUBSTANTIATEDSTAFF TRAINING AND PROFICIENCY NOT SUBSTANTIATED
Date Complaint Received: 11/11/2019 Date Investigation Completed: 01/21/2020
Subject Area(s) Result SOD #RESIDENT RIGHTS NOT SUBSTANTIATED
Date Complaint Received: 09/24/2019 Date Investigation Completed: 01/21/2020
Subject Area(s) Result SOD #PHYSICAL ENVIRONMENT/SAFETY NOT SUBSTANTIATED
YGZ812PROGRAM SERVICES SUBSTANTIATEDYGZ812STAFF TRAINING AND PROFICIENCY SUBSTANTIATED
Date Complaint Received: 06/13/2019 Date Investigation Completed: 08/12/2019
Subject Area(s) Result SOD #YGZ811RESIDENT RIGHTS SUBSTANTIATED
Date Complaint Received: 09/18/2018 Date Investigation Completed: 10/10/2018
Subject Area(s) Result SOD #PHYSICAL ENVIRONMENT/SAFETY NOT SUBSTANTIATEDPROGRAM SERVICES NOT SUBSTANTIATED
This is Page 40 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.

DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CA (AMBULATORY)
Facility Information
Facility Name: LAKEVIEW CARE PARTNERS AT WATERFORD II (0016982)
Address: 1701 SHARP RD, WATERFORD, WI 53185
License Status: REGULAR
Licensed/Certified/Registered 09/19/2018 12:00:00AM
Regional Office: SOUTHEASTERN REGION (MILWAUKEE), (414) 227-2005
Survey History
Type: STANDARD Purpose: SURVEY/COMPLAINTSurvey ID: 0135440 End Date: 11/16/2020
Results: ENFORCEMENT ACTION
Statement of Deficiency: #8OPK11 Served 01/14/2021
Deficiencies Cited Subject Area CorrectedCompliance
Verified83.12(4)(c) REPORTING INCIDENTS WITH SERIOUS
INJURY83.20(2)(a)-(d) DEPARTMENT-APPROVED TRAINING COURSE
Withdrawn83.32(3)(i) RIGHTS OF RESIDENTS: PROMPT AND ADEQUATE TREATMENT
6/9/21
83.38(1)(g) HEALTH MONITORING83.47(2)(e) OTHER EVACUATION DRILLS
Type: INITIAL Purpose: SURVEYSurvey ID: 0128243 End Date: 09/19/2018
Results: LICENSE/CERT/REGISTRATION ISSUED
This is Page 41 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.
DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CA (AMBULATORY)
Enforcement History (LAKEVIEW CARE PARTNERS AT WATERFORD II--0016982)
Date: 01/14/2021 SOD #8OPK11 Appealed: Yes Decision: STIPULATION
SanctionsORDER TO COMPLYFORFEITURE---83.20(2)(a-d)FORFEITURE---83.32(3)(i)FORFEITURE---due to stip. agreement 83.38(1)(g)(1)
This is Page 42 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.
DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Facility Information
Facility Name: LAKEVIEW CARE PARTNERS AT WATERFORD (0016391)
Address: 1701 SHARP RD, WATERFORD, WI 53185
License Status: REGULAR
Licensed/Certified/Registered 09/01/2016 12:00:00AM
Regional Office: SOUTHEASTERN REGION (MILWAUKEE), (414) 227-2005
Survey History
Type: OTHER Purpose: COMPLAINT/SELF REPORTSurvey ID: 0136694 End Date: 07/01/2021
Results: NO STATEMENT OF DEFICIENCY ISSUED
Type: ABBREVIATED Purpose: SURVEY/COMPLAINT/SELF REPORTSurvey ID: 0136589 End Date: 03/12/2021
Results: ENFORCEMENT ACTION
Statement of Deficiency: #8PDQ11 Served 07/01/2021
Deficiencies Cited Subject Area CorrectedCompliance
Verified83.32(3)(g) RIGHTS OF RESIDENTS: FREE OF PHYSICAL
RESTRAINTS83.32(3)(h) RIGHTS OF RESIDENTS: TO RECEIVE
MEDICATION83.37(1)(a) WRITTEN ORDER FOR MEDICATIONS,
SUPPLEMENTS83.47(2)(e) OTHER EVACUATION DRILLS
This is Page 43 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.

DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Enforcement History (LAKEVIEW CARE PARTNERS AT WATERFORD--0016391)
Date: 07/01/2021 SOD #8PDQ11 Appealed: Decision: PENDING
SanctionsCOMPLY WITH DEPARTMENT PLAN OF CORRECTIONORDER TO COMPLYFORFEITURE---83.32(3)(G)FORFEITURE---83.32(3)(h)
Complaint History (LAKEVIEW CARE PARTNERS AT WATERFORD--0016391)
Date Complaint Received: 03/18/2021 Date Investigation Completed: 07/01/2021
Subject Area(s) Result SOD #RESIDENT RIGHTS NOT SUBSTANTIATED
Date Complaint Received: 02/04/2021 Date Investigation Completed: 03/12/2021
Subject Area(s) Result SOD #8PDQ11RESIDENT RIGHTS SUBSTANTIATED
This is Page 44 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.

DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Facility Information
Facility Name: MAPLEWOOD APPLEWOOD COTTAGE (0015968)
Address: 7711 BIG BEND RD, WATERFORD, WI 53185
License Status: REGULAR
Licensed/Certified/Registered 04/28/2016 12:00:00AM
Regional Office: SOUTHEASTERN REGION (MILWAUKEE), (414) 227-2005
Survey History
Type: STANDARD Purpose: SURVEY/COMPLAINT/VVSurvey ID: 0136010 End Date: 02/11/2021
Results: NO STATEMENT OF DEFICIENCY ISSUED
Type: OTHER Purpose: COMPLAINTSurvey ID: 0135331 End Date: 12/10/2020
Results: ENFORCEMENT ACTION
Statement of Deficiency: #HVVW11 Served 12/21/2020
Deficiencies Cited Subject Area CorrectedCompliance
VerifiedYes83.35(3)(d) SERVICE PLANS UPDATED ANNUALLY OR ON
CHANGES2/11/21
Type: OTHER Purpose: VERIFICATION VISITSurvey ID: 0134553 End Date: 08/10/2020
Results: NO STATEMENT OF DEFICIENCY ISSUED
This is Page 45 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.

DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Type: STANDARD Purpose: SURVEY/COMPLAINTSurvey ID: 0132037 End Date: 01/18/2019
Results: ENFORCEMENT ACTION
Statement of Deficiency: #IZUT11 Served 11/25/2019
Deficiencies Cited Subject Area CorrectedCompliance
VerifiedYes83.35(1)(a) PRE-ADMISSION AND ONGOING
ASSESSMENTS8/10/20
Yes83.35(3)(d) SERVICE PLANS UPDATED ANNUALLY OR ON CHANGES
8/10/20
Yes83.37(1)(h) SCHEDULED PSYCHOTROPIC MEDICATIONS 8/10/20Yes83.37(1)(i) PRN PSYCHOTROPIC MEDICATION 8/10/20Yes83.45(3) TOXIC SUBSTANCES 8/10/20Yes83.47(2)(e) OTHER EVACUATION DRILLS 8/10/20
Enforcement History (MAPLEWOOD APPLEWOOD COTTAGE--0015968)
Date: 12/21/2020 SOD #HVVW11 Appealed:
SanctionsORDER TO COMPLYFORFEITURE---83.35(3)(d)
Date: 11/22/2019 SOD #IZUT11 Appealed:
SanctionsCOMPLY WITH DEPARTMENT PLAN OF CORRECTIONFORFEITURE---83.35(3)(d)FORFEITURE---83.45(3) 2nd Cite
This is Page 46 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.

DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Complaint History (MAPLEWOOD APPLEWOOD COTTAGE--0015968)
Date Complaint Received: 01/07/2021 Date Investigation Completed: 02/11/2020
Subject Area(s) Result SOD #STAFF TRAINING AND PROFICIENCY NOT SUBSTANTIATED
Date Complaint Received: 12/12/2018 Date Investigation Completed: 01/18/2019
Subject Area(s) Result SOD #IZUT11PROGRAM SERVICES SUBSTANTIATED
ADMINISTRATION NOT SUBSTANTIATED
This is Page 47 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.

DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Facility Information
Facility Name: ROSEWOOD OAKWOOD COTTAGE (0015967)
Address: 7711 BIG BEND RD, WATERFORD, WI 53185
License Status: REGULAR
Licensed/Certified/Registered 04/28/2016 12:00:00AM
Regional Office: SOUTHEASTERN REGION (MILWAUKEE), (414) 227-2005
Survey History
Type: STANDARD Purpose: SURVEY/COMPLAINTSurvey ID: 0136598 End Date: 03/17/2021
Results: ENFORCEMENT ACTION
Statement of Deficiency: #1CQG11 Served 06/25/2021
Deficiencies Cited Subject Area CorrectedCompliance
Verified83.17(2)(a) EMPLOYEES SCREENED FOR COMMUNICABLE
DISEASE83.38(1)(g) HEALTH MONITORING83.41(3)(b) FOOD SAFETY
Type: OTHER Purpose: COMPLAINTSurvey ID: 0134516 End Date: 08/06/2020
Results: NO STATEMENT OF DEFICIENCY ISSUED
Type: OTHER Purpose: DESK REVIEWSurvey ID: 0133850 End Date: 06/08/2020
Results: NO STATEMENT OF DEFICIENCY ISSUED
This is Page 48 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.

DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Type: STANDARD Purpose: SURVEY/COMPLAINTSurvey ID: 0133657 End Date: 06/28/2019
Results: STATEMENT OF DEFICIENCY ISSUED
Statement of Deficiency: #874O11 Served 05/08/2020
Deficiencies Cited Subject Area CorrectedCompliance
VerifiedYes83.12(5)(a) NOTIFICATION: INCIDENT, INJURY, CHANGES 5/15/20Yes83.25 CONTINUING EDUCATION 6/1/20Yes83.35(3)(d) SERVICE PLANS UPDATED ANNUALLY OR ON
CHANGES5/15/20
No83.37(1)(h) SCHEDULED PSYCHOTROPIC MEDICATIONS 6/1/20Yes83.38(1)(h) MEDICATION ADMINISTRATION 6/1/20Yes83.42(1) RESIDENT RECORD MAINTAINED 6/1/20Yes83.47(2)(e) OTHER EVACUATION DRILLS 6/1/20
Enforcement History (ROSEWOOD OAKWOOD COTTAGE--0015967)
Date: 06/25/2021 SOD #1CQG11 Appealed: Decision: PENDING
SanctionsCOMPLY WITH DEPARTMENT PLAN OF CORRECTIONORDER TO COMPLYFORFEITURE---83.38(1)(g)FORFEITURE---83.41(3)(b)
This is Page 49 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.
DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Complaint History (ROSEWOOD OAKWOOD COTTAGE--0015967)
Date Complaint Received: 01/07/2021 Date Investigation Completed: 03/17/2021
Subject Area(s) Result SOD #STAFF TRAINING AND PROFICIENCY NOT SUBSTANTIATED
Date Complaint Received: 11/25/2020 Date Investigation Completed: 03/17/2021
Subject Area(s) Result SOD #ADMINISTRATION NOT SUBSTANTIATEDPROGRAM SERVICES NOT SUBSTANTIATEDSTAFF TRAINING AND PROFICIENCY NOT SUBSTANTIATED
Date Complaint Received: 11/19/2020 Date Investigation Completed: 03/17/2021
Subject Area(s) Result SOD #PROGRAM SERVICES NOT SUBSTANTIATEDRESIDENT RIGHTS NOT SUBSTANTIATED
Date Complaint Received: 11/10/2020 Date Investigation Completed: 03/15/2021
Subject Area(s) Result SOD #1CQG11PROGRAM SERVICES SUBSTANTIATED
Date Complaint Received: 08/05/2020 Date Investigation Completed: 08/06/2020
Subject Area(s) Result SOD #OTHER NOT SUBSTANTIATED
Date Complaint Received: 12/11/2018 Date Investigation Completed: 06/28/2019
Subject Area(s) Result SOD #ADMINISTRATION NOT SUBSTANTIATED
This is Page 50 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.
DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Date Complaint Received: 11/19/2018 Date Investigation Completed: 06/28/2019
Subject Area(s) Result SOD #874O11PROGRAM SERVICES SUBSTANTIATED
This is Page 51 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.
DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Facility Information
Facility Name: WATERFORD MEMORY CARE LLC (0014008)
Address: 301 S SIXTH ST, WATERFORD, WI 53185
License Status: REGULAR
Licensed/Certified/Registered 07/01/2013 12:00:00AM
Regional Office: SOUTHEASTERN REGION (MILWAUKEE), (414) 227-2005
Survey History
Type: OTHER Purpose: COMPLAINTSurvey ID: 0135942 End Date: 03/17/2021
Results: NO STATEMENT OF DEFICIENCY ISSUED
Type: ABBREVIATED Purpose: SURVEY/COMPLAINTSurvey ID: 0134814 End Date: 09/04/2020
Results: NO STATEMENT OF DEFICIENCY ISSUED
Complaint History (WATERFORD MEMORY CARE LLC--0014008)
Date Complaint Received: 02/23/2021 Date Investigation Completed: 03/17/2021
Subject Area(s) Result SOD #PROGRAM SERVICES NOT SUBSTANTIATEDRESIDENT RIGHTS NOT SUBSTANTIATED
Date Complaint Received: 08/21/2020 Date Investigation Completed: 09/02/2020
Subject Area(s) Result SOD #ADMINISTRATION NOT SUBSTANTIATEDPROGRAM SERVICES NOT SUBSTANTIATED
This is Page 52 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.

DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS AA (AMBULATORY)
Facility Information
Facility Name: LONG LAKE HOUSE (0011322)
Address: 8208 RACINE AVE, WIND LAKE, WI 53185
License Status: REGULAR
Licensed/Certified/Registered 03/01/2007 12:00:00AM
Regional Office: SOUTHEASTERN REGION (MILWAUKEE), (414) 227-2005
Survey History
Type: ABBREVIATED Purpose: SURVEYSurvey ID: 0130093 End Date: 02/07/2019
Results: ENFORCEMENT ACTION
Statement of Deficiency: #HGN912
Deficiencies Cited Subject Area CorrectedCompliance
Verified83.35(1)(a) PRE-ADMISSION AND ONGOING
ASSESSMENTS83.35(2) TEMPORARY SERVICE PLAN83.35(3)(b) SERVICE PLAN DEVELOPMENT: PARTIES
INVOLVED83.37(1)(h) SCHEDULED PSYCHOTROPIC MEDICATIONS83.37(1)(i) PRN PSYCHOTROPIC MEDICATION83.41(3)(b) FOOD SAFETY83.43(1) ENVIRONMENT SAFE, CLEAN, AND
COMFORTABLE83.45(3) TOXIC SUBSTANCES
This is Page 53 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.

DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS AA (AMBULATORY)
Enforcement History (LONG LAKE HOUSE--0011322)
Date: 05/01/2019 SOD #HGN912 Appealed: Decision: PENDING
SanctionsCOMPLY WITH DEPARTMENT PLAN OF CORRECTIONCOMPLY WITH REQUIREMENTFORFEITURE---83.35(1)(a)FORFEITURE---83.37(1)(h)FORFEITURE---83.37(1)(i)
This is Page 54 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.
DEPARTMENT OF HEALTH SERVICESDivision of Quality AssurancePrinted 09/22/2021
STATE OF WISCONSINBureau of Assisted Living
P.O. Box 7940Madison WI 53707-7940
Provider Inspection Summary
For the period 08/24/2018 to 08/23/2021
Community Based Residential Facility--CLASS CNA (NONAMBULATORY)
Facility Information
Facility Name: ROLLING MEADOWS (0012246)
Address: 8212 RACINE AVE, WIND LAKE, WI 53185
License Status: REGULAR
Licensed/Certified/Registered 05/01/2009 12:00:00AM
Regional Office: SOUTHEASTERN REGION (MILWAUKEE), (414) 227-2005
Survey History
No survey activity during the period 8/24/18 to 8/23/21
This is Page 55 of 55 total pages. If printing this report ensure that your printer is set to print only the desired pages.
Disclaimer: This information is provided as a public service by the Wisconsin Department of Health Services (DHS). The Department neither endorses any facility nor guarantees that this information is accurate, up-to-date, or complete. This information, which should not be used as a sole source in selecting a facility, does not replace official information sources.