
Queensland Health Smoking Cessation Clinical Pathway...
1
Background/Problem The Smoking Cessation Clinical Pathway is an initiative of the Statewide Respiratory Clinical Network in Queensland. Version 1 was released in 2012. The pathway uses modified Bittoun algorithm for treatment and management of nicotine dependence. The SCCP was revised in November 2014 as part of the biennial review process and used to support the Department of Health’s quality improvement incentive payment initiative for smoking cessation and part of a broader package of Smoking Cessation initiatives across Queensland. A biennial review was again completed in 2016 to review feedback and evidence. Smoking rates have declined in Queensland over recent decades, having halved since 1998. The greatest decline has been among young people with lower rates of decline in older people and no change in rates in the oldest age groups. While fewer people are taking up smoking and others are quitting, more needs to be done to assist people to quit. In 2004–05 tobacco was estimated to cost Australian society $31.49 billion, an estimated $6.1 billion in Queensland. To meet the challenge, the Queensland Government passed legislation that bans smoking in public places, including within five metres of the boundaries of hospitals and health service facilities. In support of the legislation, the Department of Health has implemented initiatives such as the Quality Improvement Payment which is an incentive payment to help clinicians assess smoking behaviour at point of care. Queensland Health Clinical Pathways team established a small working party with representatives from Medicine, General Practice, Pharmacy, Nursing, Public Health, Tobacco Control, Quitline, and Consumers. The team used a ‘Knowledge To Action Framework’ to develop an evidence based tool which could be used by staff within the Inpatient or Community setting to access smoking dependence and manage the withdrawal processes. Methods Clinicians assess and record inpatient/outpatient/oral health client smoking status. Complete the smoking cessation clinical pathway for those that identify as current smokers. Clinicians do not need to be a brief intervention specialist to use the tool. Clinical application Step 1: Knowledge generation An extensive literature review explored current evidence to support clinical pathway content. Prioritisation of knowledge based on clinical assessment of effectiveness and consumer involvement. Step 2: Knowledge Synthesis Synthesis of knowledge to include in clinical pathway. Identification of critical information to focus on validity. Step 3: Development of tool End user decision making tool for the application of knowledge. Moving from awareness to agreement. Deliberately engineering change using a knowledge to action framework Key tactics and impact An evidence based decision support tool for staff to assist patients to quit smoking and manage withdrawls in hospital 12% of adults smoke daily, and another 4% smoke occasionally. Figure 1: Smoking prevalence, adults, Queensland 2015 Never smoked Ex-smoker Current – not daily Current daily 0 10 20 30 40 50 60 14 4 28 56 Percentage Coded Nicotine Dependence for Identified Smoker Pe r cen t ag e coded Pe r cen t ag e T a c t i c I m p a c t Stakeholder engagement Interdisciplinary involvement in the development of the SCCP Early engagement of users Identification of clinical champions Consumer engagement General practitioner engagement Literature Review Provision of evidence to support the key elements of the clinical content of the clinical pathway Assess nicotine dependence Increase in smokers receiving brief intervention from 12% in 2014 to 46% in 2016 Advice on Nicotine Replacement Therapy (NRT) and NRT prescribing processes Timely initiated NRT Streamlined management of smoking in the hospitals Evidence based pharmacological support for our patients Referral Processes to ensure appropriate follow up and assistance with quitting smoking Threefold increase in referrals to Quitline in 2015 and 57% increase in 2016 to date from baseline Increased referrals to General Practitioner Enable clinical coding Clinical coding to determine incentive payments Website and logo Provision of easy access to clinical pathway tools and additional resources Access to posters to advertise clinical pathway Outcomes and impact Queensland Health Smoking Cessation Clinical Pathway (SCCP) Select and tailor implement interventions Monitor knowledge use Evaluate outcomes Sustain knowledge use Identify problem and knowledge needed Adapt knowledge to local content Assess barriers to knowledge D O S T U D Y A C T P L A N Knowledge-to-Action Framework. Adapted from Graham, et al. [2006]. Queensland Health Scanned QR code to go to My Quit buddy Authors Denise Curran, Deepali Gupta, Henry Marshall, Kate Giles, Katrina Lewis, Shelley Peardon and the Statewide Respiratory Clinical Network and Smoking Cessation Clinical Pathway Workgroup. 0 10 20 30 40 50 60 2016 2015 2014 2013 2012 2011 2010 SCCP commenced SCCP Quality Improvement Payment commenced 10 20 30 40 50 May-16 Feb-16 Nov-15 Aug-15 May-15 Feb-15 Nov-14 QIP smoking cessation performance statewide % smokers where a clinician has completed page one of the smoking cessation pathway form Targets reset 2258 529 SMOKING CESSATION CLINICAL PATHWAY k6:Fm v5.00 - 08/2016 Mat. no.: 10267567 SW321 This tool is for screening smoking behaviour and to guide support for those who temporarily cannot smoke or wish to reduce/quit smoking. Clinical pathways never replace clinical judgement. Care outlined in this pathway must be altered if it is not clinically appropriate for the individual patient. Category Date: / / Ask (all patients) 1. Have you smoked tobacco in the last 30 days? Yes (continue with pathway) No FRQJUDWXODWH VLJQ DQG ¿OH Electronic cigarettes (may require nicotine replacement therapy (NRT) in hospital) If you are unable to complete this pathway, document the reason in the comments section below. See comment 2. Do you want to quit smoking? Yes No (still offer NRT for inpatients to manage withdrawals) Assess 3. Nicotine dependence: a. How many cigarettes do you smoke in a typical day? ............ Is this more than 10 cigarettes? Yes No b. 'R \RX VPRNH \RXU ¿UVW FLJDUHWWH ZLWKLQ PLQXWHV RI ZDNLQJ" Yes No c. Do you have a history of withdrawal symptoms/cravings from quitting smoking? Yes No If yes to one or more of the above, then the patient is considered nicotine dependent and should be offered NRT. 4. Is the patient nicotine dependent? Yes No 5. Are you currently using any of the following? No NRT (continue regimen referring to algorithm on page 2) Varenicline (Champix ® )* Bupropion (Zyban ® )* *Advise treating team to prescribe Champix ® /Zyban ® OR if not available offer NRT (for inpatients only). Advise 6. Advise all smokers to quit using clear but non-confrontational language: » “As a health professional the best advice that I can give you is to try to stop smoking” » ³*LYLQJ XS VPRNLQJ LV KDUG EXW LW ZLOO KHOS ZLWK HJ VXUJHU\ KHDOLQJ PHGLFDWLRQ ¿QDQFHV KHDOWK DQG ¿WQHVV´ » “Using NRT and behavioural support considerably increases your long term success in quitting” » “NRT is available from most retail stores, however patches and medications (Champix ® and Zyban ® ) are cheaper on PBS” PRESCRIBING Assist (discuss treatment and other options) 7. Special considerations (medical approval may be required prior to initiating NRT depending on unit preference): Any local precautions/protocols (e.g. microvascular surgery, skin grafts etc) Children <12 years of age Pregnant/lactating Recent cardiovascular event <48 hours Clozapine Note: Patients who stop smoking with or without NRT may require a medication dose change (e.g. opioids, antipsychotics, EHQ]RGLD]HSLQHV LQVXOLQ DQG ZDUIDULQ 6HHN 0HGLFDO 2I¿FHU DGYLFH LI DQ\ RI WKH DERYH DUH WLFNHG INAPTIENT ONLY 8. Offer NRT to relieve nicotine withdrawal and/or assist with quitting. If smoking/withdrawals persist, NRT should be titrated to achieve effect VHH ÀRZ FKDUW SDJH 157 FDQ EH LQLWLDWHG E\ D PHGLFDO RI¿FHU QXUVH RU SKDUPDFLVW DFFRUGLQJ WR \RXU ORFDO SROLF\ Patient offered NRT and accepted treatment HQVXUH GLVFKDUJH VFULSW LV ZULWWHQ IRU RQJRLQJ WUHDWPHQW Patient offered NRT and declined treatment (ask again during stay as needed) 3DWLHQW XQDEOH WR EH RIIHUHG 157 5HIHU WR 0HGLFDO 2I¿FHU (see Q7) or reason: .................................................................................................................................................................................................................. PBS9. Prescribed pharmacotherapy (NRT patches/Champix ® /Zyban ® ) Yes No If no, document reason: ................................................................................................................................................................................ Arrange follow-up 10. Patient provided with a copy of “self-help” resource (e.g. ‘Quit Because You Can’ booklet) Yes No 11. Did patient consent to referral to any of these services? (tick all that apply) a. Quitline Service ([email protected] Fax: 07 3259 8217 Patient phone: ..................................... ) Yes No b. Local smoking cessation support/tobacco treatment specialist services in the HHS Yes No c. GP follow up (remind patients of subsidised PBS products – see page 2) Yes No )D[ ZLWK FRYHU VKHHW RU SRVW FRS\ ZLWK GLVFKDUJH VXPPDU\ DIWHU FRPSOHWLRQ WR WKH VHUYLFHV DERYH Comments: Assessment completed by – Name: Designation: Signature: Date: Tick if you would like Quitline to send a report on the patient’s progress Initial: ...................... Assessment review completed by (if required) – Name: Designation: Signature: Date: DO NOT WRITE IN THIS BINDING MARGIN Page 1 of 2 $I¿[ LGHQWL¿FDWLRQ ODEHO KHUH URN: Family name: Given name(s): Address: Date of birth: Sex: M F I Smoking Cessation Clinical Pathway Facility: ......................................................................................................... © State of Queensland (Queensland Health) 2016 Contact: [email protected] References Tobacco Addiction. Cochrane Review 2015 (http://tobacco.cochrane.org/evidence) Supporting smoking cessation. A guide for health professionals. RACGP Guidelines 2015 (http://www.racgp.org.au/your-practice/guidelines/smoking-cessation/)
Transcript of Queensland Health Smoking Cessation Clinical Pathway...
Background/ProblemThe Smoking Cessation Clinical Pathway is an initiative of the Statewide Respiratory Clinical Network in Queensland. Version 1 was released in 2012. The pathway uses modified Bittoun algorithm for treatment and management of nicotine dependence. The SCCP was revised in November 2014 as part of the biennial review process and used to support the Department of Health’s quality improvement incentive payment initiative for smoking cessation and part of a broader package of Smoking Cessation initiatives across Queensland. A biennial review was again completed in 2016 to review feedback and evidence.
Smoking rates have declined in Queensland over recent decades, having halved since 1998. The greatest decline has been among young people with lower rates of decline in older people and no change in rates in the oldest age groups. While fewer people are taking up smoking and others are quitting, more needs to be done to assist people to quit. In 2004–05 tobacco was estimated to cost Australian society $31.49 billion, an estimated $6.1 billion in Queensland. To meet the challenge, the Queensland Government passed legislation that bans smoking in public places, including within five metres of the boundaries of hospitals and health service facilities.
In support of the legislation, the Department of Health has implemented initiatives such as the Quality Improvement Payment which is an incentive payment to help clinicians assess smoking behaviour at point of care.
Queensland Health Clinical Pathways team established a small working party with representatives from Medicine, General Practice, Pharmacy, Nursing, Public Health, Tobacco Control, Quitline, and Consumers. The team used a ‘Knowledge To Action Framework’ to develop an evidence based tool which could be used by staff within the Inpatient or Community setting to access smoking dependence and manage the withdrawal processes.
Methods
Clinicians assess and record inpatient/outpatient/oral health client smoking status.Complete the smoking cessation clinical pathway for those that identify as current smokers.Clinicians do not need to be a brief intervention specialist to use the tool.
Clinical application
Step 1: Knowledge generation An extensive literature review explored current evidence to support clinical pathway content.Prioritisation of knowledge based on clinical assessment of effectiveness and consumer involvement. Step 2: Knowledge SynthesisSynthesis of knowledge to include in clinical pathway. Identification of critical information to focus on validity. Step 3: Development of toolEnd user decision making tool for the application of knowledge. Moving from awareness to agreement.
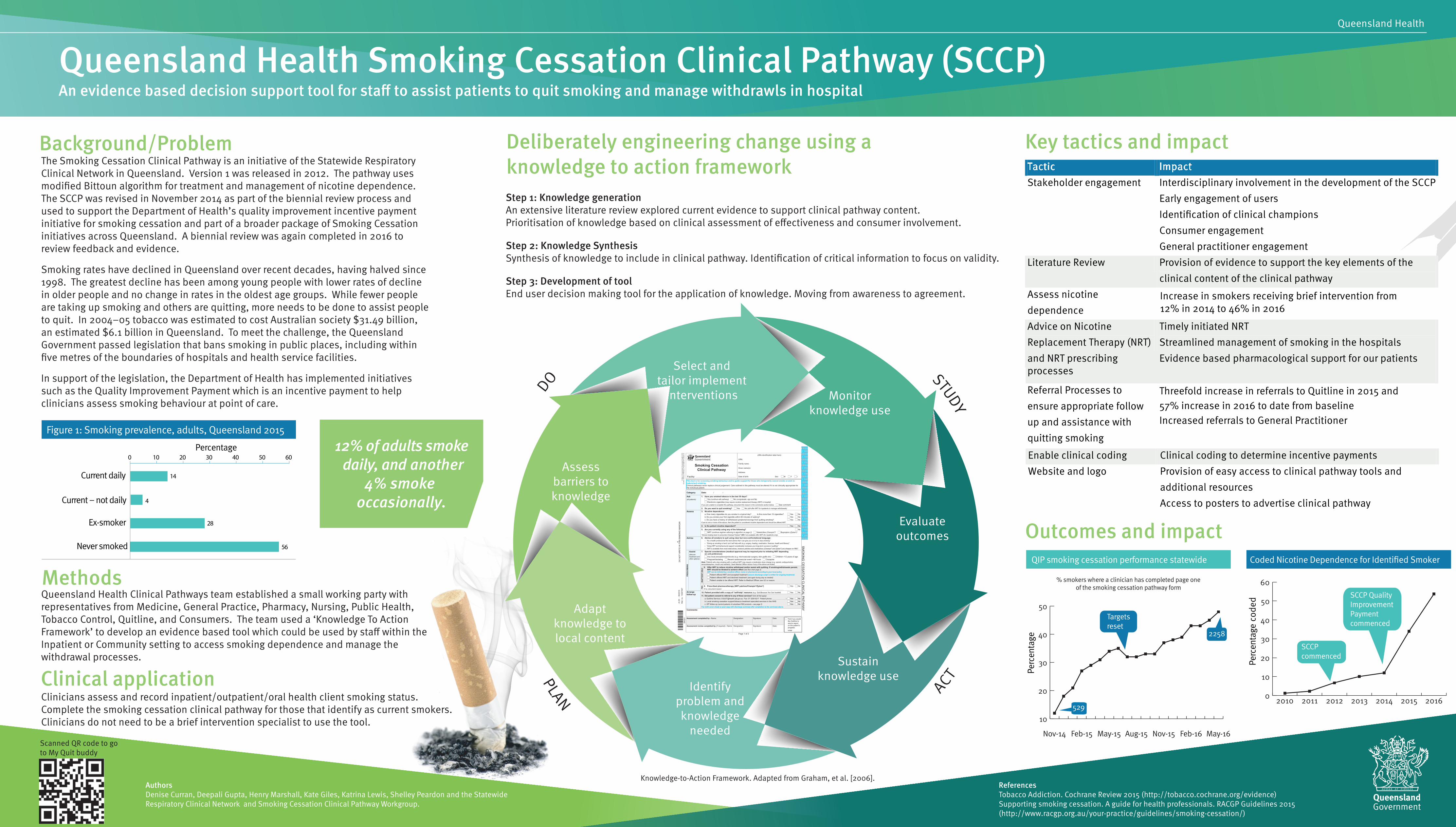
Deliberately engineering change using a knowledge to action framework
Key tactics and impact
An evidence based decision support tool for staff to assist patients to quit smoking and manage withdrawls in hospital
12% of adults smoke daily, and another
4% smoke occasionally.
Figure 1: Smoking prevalence, adults, Queensland 2015
Never smoked
Ex-smoker
Current – not daily
Current daily
0 10 20 30 40 50 60
14
4
28
56
Percentage
Coded Nicotine Dependence for Identified Smoker
Perc
enta
ge c
oded
Perc
enta
ge
Tactic Impact Stakeholder engagement Interdisciplinary involvement in the development of the SCCP
Early engagement of users Identification of clinical champions Consumer engagement General practitioner engagement
Literature Review Provision of evidence to support the key elements of the clinical content of the clinical pathway
Assess nicotine dependence
Increase in smokers receiving brief intervention from 12% in 2014 to 46% in 2016
Advice on Nicotine Replacement Therapy (NRT) and NRT prescribingprocesses
Timely initiated NRTStreamlined management of smoking in the hospitals Evidence based pharmacological support for our patients
Referral Processes to
ensure appropriate follow up and assistance with quitting smoking
Threefold increase in referrals to Quitline in 2015 and 57% increase in 2016 to date from baselineIncreased referrals to General Practitioner
Enable clinical coding Clinical coding to determine incentive payments Website and logo Provision of easy access to clinical pathway tools and
additional resources Access to posters to advertise clinical pathway
Outcomes and impact
Queensland Health Smoking Cessation Clinical Pathway (SCCP)
Select and tailor implement
interventions Monitor knowledge use
Evaluate outcomes
Sustain knowledge use
Identify problem and knowledge
needed
Adapt knowledge to local content
Assess barriers to knowledge
D
O
STUDY
A
CT PLAN
Knowledge-to-Action Framework. Adapted from Graham, et al. [2006].
Queensland Health
Scanned QR code to go to My Quit buddy
AuthorsDenise Curran, Deepali Gupta, Henry Marshall, Kate Giles, Katrina Lewis, Shelley Peardon and the Statewide Respiratory Clinical Network and Smoking Cessation Clinical Pathway Workgroup.
0
10
20
30
40
50
60
2016201520142013201220112010
SCCPcommenced
SCCP Quality Improvement Payment commenced
10
20
30
40
50
May-16Feb-16Nov-15Aug-15May-15Feb-15Nov-14
QIP smoking cessation performance statewide
% smokers where a clinician has completed page oneof the smoking cessation pathway form
Targets reset
2258
529
SM
OK
ING
CE
SS
ATION
CLIN
ICA
L PATHW
AY
v5.0
0 -
08/
2016
Mat
. no.
: 102
6756
7S
W32
1
This tool is for screening smoking behaviour and to guide support for those who temporarily cannot smoke or wish to reduce/quit smoking.Clinical pathways never replace clinical judgement. Care outlined in this pathway must be altered if it is not clinically appropriate for the individual patient.
Category Date: / /
Ask(all patients)
1. Have you smoked tobacco in the last 30 days? Yes (continue with pathway) No Electronic cigarettes (may require nicotine replacement therapy (NRT) in hospital)
If you are unable to complete this pathway, document the reason in the comments section below. See comment
2. Do you want to quit smoking? Yes No (still offer NRT for inpatients to manage withdrawals)
Assess 3. Nicotine dependence:a. How many cigarettes do you smoke in a typical day? ............ Is this more than 10 cigarettes? Yes Nob. Yes Noc. Do you have a history of withdrawal symptoms/cravings from quitting smoking? Yes No
If yes to one or more of the above, then the patient is considered nicotine dependent and should be offered NRT.
4. Is the patient nicotine dependent? Yes No
5. Are you currently using any of the following? No NRT (continue regimen referring to algorithm on page 2) Varenicline (Champix®)* Bupropion (Zyban®)*
*Advise treating team to prescribe Champix®/Zyban® OR if not available offer NRT (for inpatients only).
Advise 6. Advise all smokers to quit using clear but non-confrontational language: » “As a health professional the best advice that I can give you is to try to stop smoking” » » “Using NRT and behavioural support considerably increases your long term success in quitting” » “NRT is available from most retail stores, however patches and medications (Champix® and Zyban®) are cheaper on PBS”
PRES
CR
IBIN
G
Assist(discuss treatment and other options)
7. Special considerations (medical approval may be required prior to initiating NRT depending on unit preference):
Any local precautions/protocols (e.g. microvascular surgery, skin grafts etc) Children <12 years of age Pregnant/lactating Recent cardiovascular event <48 hours Clozapine
Note: Patients who stop smoking with or without NRT may require a medication dose change (e.g. opioids, antipsychotics,
INA
PTIE
NT
ON
LY
8. Offer NRT to relieve nicotine withdrawal and/or assist with quitting. If smoking/withdrawals persist, NRT should be titrated to achieve effect
Patient offered NRT and accepted treatment Patient offered NRT and declined treatment (ask again during stay as needed)
(see Q7) or reason:..................................................................................................................................................................................................................
PBS 9. Prescribed pharmacotherapy (NRT patches/Champix®/Zyban®) Yes No
If no, document reason: ................................................................................................................................................................................Arrange follow-up
10. Patient provided with a copy of “self-help” resource (e.g. ‘Quit Because You Can’ booklet) Yes No
11. Did patient consent to referral to any of these services? (tick all that apply)a. Quitline Service ([email protected] Fax: 07 3259 8217 Patient phone: ..................................... ) Yes Nob. Local smoking cessation support/tobacco treatment specialist services in the HHS Yes Noc. GP follow up (remind patients of subsidised PBS products – see page 2) Yes No
Comments:
Assessment completed by – Name: Designation: Signature: Date: Tick if you would like Quitline to send a report on the patient’s progressInitial: ......................
Assessment review completed by (if required) – Name: Designation: Signature: Date:
DO
NO
T WR
ITE IN
THIS
BIN
DIN
G M
AR
GIN
DO
NO
T W
RIT
E IN
TH
IS B
IND
ING
MA
RG
IN
Page 1 of 2
URN:
Family name:
Given name(s):
Address:
Date of birth: Sex: M F I
Smoking Cessation Clinical Pathway
Facility: .........................................................................................................
© S
tate
of Q
ueen
slan
d (Q
ueen
slan
d H
ealth
) 201
6C
onta
ct: C
linic
al_P
athw
ays_
Pro
gram
@he
alth
.qld
.gov
.au
ReferencesTobacco Addiction. Cochrane Review 2015 (http://tobacco.cochrane.org/evidence)Supporting smoking cessation. A guide for health professionals. RACGP Guidelines 2015 (http://www.racgp.org.au/your-practice/guidelines/smoking-cessation/)


















