QUALITY CARE GHANA - WHO | World Health · PDF fileA generic assessment tool adapted for use...
140
Better medicines for children in Ghana Ministry of Health GHANA Assessment of quality of care for children in selected hospitals in Ghana December 2011
-
Upload
nguyenxuyen -
Category
Documents
-
view
215 -
download
2
Transcript of QUALITY CARE GHANA - WHO | World Health · PDF fileA generic assessment tool adapted for use...

Better medicines for children in Ghana
Ministry of Health
GHANA
Assessment of quality of care for children in selected hospitals in Ghana
December 2011

© World Health Organization 2011
All rights reserved. Publications of the World Health Organization are available on the WHO web site (www.who.int) or can be purchased from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for noncommercial distribution – should be addressed to WHO Press through the WHO web site (http://www.who.int/about/licensing/copyright_form/en/index.html).
The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters. All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use.

Assessment of quality of care for children in selected hospitals in Ghana
Table of contents Acronyms........................................................................................................................................................... iii Acknowledgements ........................................................................................................................................... v Executive summary ......................................................................................................................................... vii 1. Introduction ................................................................................................................................................. 1
1.1 Background .............................................................................................................................................................. 1 1.2 Objectives.................................................................................................................................................................. 1 1.3 Methodology............................................................................................................................................................ 2
2. Key findings................................................................................................................................................. 3 2.1 General hospital information ................................................................................................................................. 3 2.2 Hospital infrastructure systems............................................................................................................................. 4 2.3 Emergency care services ......................................................................................................................................... 6 2.4 Paediatric ward........................................................................................................................................................ 9 2.5 Case management of common conditions ......................................................................................................... 10 2.6 Supportive care ...................................................................................................................................................... 15 2.7 Monitoring.............................................................................................................................................................. 15 2.8 Neonatal care ......................................................................................................................................................... 17 2.9 Paediatric surgerical care and rehabilitation...................................................................................................... 19 2.10 Other hospital wards with children .................................................................................................................... 20 2.11 Hospital administration........................................................................................................................................ 20 2.12 Access to hospital care .......................................................................................................................................... 20
3. Discussion .................................................................................................................................................. 24 3.1 Children are not adults ......................................................................................................................................... 24 3.2 Staffing .................................................................................................................................................................... 25 3.3 Support systems..................................................................................................................................................... 25 3.4 Hospital data.......................................................................................................................................................... 26 3.5 Drugs, equipment and supplies........................................................................................................................... 26 3.6 Emergency care...................................................................................................................................................... 26 3.7 Case management.................................................................................................................................................. 27 3.8 Supportive care ...................................................................................................................................................... 28 3.9 Hospital support systems..................................................................................................................................... 28 3.10 Hospital administration........................................................................................................................................ 29
4. Recommendations..................................................................................................................................... 30 4.1 Leadership and advocacy for improvement in quality of care........................................................................ 30 4.2 Improving hospital layout and facilities for children ....................................................................................... 30 4.3 Improving the quality of data on paediatric care.............................................................................................. 31 4.4 Improving the availability of medicines and supplies ..................................................................................... 31 4.5 Improving case management............................................................................................................................... 31 4.6 Strengthening quality assurance mechanisms within hospitals...................................................................... 32 4.7 Improving human resources................................................................................................................................ 32 4.8 Improving access to health facilities ................................................................................................................... 32
References.......................................................................................................................................................... 33

Assessment of quality of care for children in selected hospitals in Ghana
Page ii
Appendix I: Assessment of the quality of care for children in hospitals ‐‐ A generic assessment tool adapted for use in Ghana, June 2010........................................................... 35 Introduction ...................................................................................................................................................... 35 Overview of the assessment process ............................................................................................................ 36 1. General hospital information ................................................................................................................. 43
1.1 Layout of health facility........................................................................................................................................ 44
2. Hospital support systems ........................................................................................................................ 47 2.1 Hospital health statistics....................................................................................................................................... 48 2.2 Essential drugs, equipment and supplies........................................................................................................... 49 2.3 Laboratory support ............................................................................................................................................... 55
3. Emergency care.......................................................................................................................................... 57 3.1 Patient flow ............................................................................................................................................................ 57 3.2 Staff dealing with emergencies ............................................................................................................................ 59 3.3 Layout and structure of emergency area............................................................................................................ 59 3.4 Drugs, equipment and supplies........................................................................................................................... 61 3.5 Case management of emergency conditions...................................................................................................... 61
4. Children’s ward......................................................................................................................................... 63 4.1 Staffing and layout ................................................................................................................................................ 63 4.2 Standards and criteria in the childrenʹs ward.................................................................................................... 64
5. Case management of common diseases: ............................................................................................... 67 5.1 Cough or difficult breathing ................................................................................................................................ 67 5.2 Diarrhoea ................................................................................................................................................................ 71 5.3 Fever conditions..................................................................................................................................................... 73 5.4 Severe malnutrition............................................................................................................................................... 76 5.5 Children with HIV/AIDS...................................................................................................................................... 79
6. Supportive care.......................................................................................................................................... 83 7. Monitoring ................................................................................................................................................. 87 8. Neonatal care ............................................................................................................................................. 91
8.1 Nursery staffing and layout ................................................................................................................................. 91 8.2 Routine neonatal care............................................................................................................................................ 92 8.3 Nursery facilities.................................................................................................................................................... 94 8.4 Case management and sick newborn care ......................................................................................................... 96
9. Paediatric surgery and rehabilitation.................................................................................................... 99 9.1 Paediatric‐size anaesthesia equipment ............................................................................................................. 101
10. Other hospital wards with children .................................................................................................... 103 11. Hospital administration......................................................................................................................... 105 12. Access to hospital care: Interview with caretakers and health workers ....................................... 107 Annex 1: Interviews with caretakers .......................................................................................................... 115 Annex 2: Interviews with health workers.................................................................................................. 121

Assessment of quality of care for children in selected hospitals in Ghana
Page iii
Acronyms
AIDS Acquired Immunodeficiency Syndrome
ART Antiretroviral Therapy
ARV Antiretroviral
BMC Better Medicines for Children
CFR Case fatality rate
CSF Cerebrospinal fluid
DHIMS District Health Information Management System
ETAT Emergency Triage, Assessment and Treatment
GHS Ghana Health Service
HIV Human Immunodeficiency Virus
ICU Intensive Care Unit
IM Intramuscular
IMCI Integrated Management of Childhood Illness
IMNCI Integrated Management of Neonatal and Childhood Illness
KATH Komfo Anokye Teaching Hospital
LBW Low Birth Weight
MOH Ministry of Health
MUAC Mid‐Upper Arm Circumference
NG Nasogastric
NHIS National Health Insurance Scheme
NICU Neonatal Intensive Care Unit
OPD Outpatient Department
RUTF Ready‐to‐Use Therapeutic Food
SAM Severe Acute Malnutrition
TB Tuberculosis
UTI Urinary Tract Infection
WHO World Health Organization

Assessment of quality of care for children in selected hospitals in Ghana
Page iv

Assessment of quality of care for children in selected hospitals in Ghana
Page v
Acknowledgements
This study was made possible through funding from the Better Medicines for Children project in Ghana. We wish to thank the steering committee members, especially Mrs Martha Gyansa Lutterodt (Ghana National Drugs Programme) and Mrs Edith Andrews (WHO) for their support for this work. We also express our profound gratitude to the following members of the Better Medicines for Children Sub‐Committee on Quality of Care for providing technical oversight to the assessment: Dr Cynthia Bannerman, Ag Director Institutional Care Director (ICD), Ghana Health Service (GHS); Dr Isabella Sagoe‐Moses, National Child Health Coordinator; Professor Jennifer Welbeck, University of Ghana Medical School; and Dr Mary N.A. Brantuo, World Health Organization (WHO). We are grateful to the following individuals who worked tirelessly to adapt the WHO generic assessment tools, including: Dr Cynthia Bannerman, Ag Director ICD, GHS; Dr Isabella Sagoe‐Moses, National Child Health Coordinator; Professor Jennifer Welbeck, University of Ghana Medical School; Dr Mary N.A. Brantuo, WHO; Dr Emmanuel Addo‐Yobo, Paediatrician, Komfo Anokye Teaching Hospital (KATH); Dr Eric Siffah, Paediatrician, Princess Marie Louise Hospital; Dr Mira Taylor, Paediatrician, Koforiduah Regional Hospital; and Ms Agnes Gbormittah, Deputy Director Nursing, Ridge Hospital. Our Assessment Team visited the facilities to carry out the assessment and put together the report. Their effort is very much appreciated. Our thanks to: Dr Cynthia Bannerman, Ag Director ICD, GHS; Dr Isabella Sagoe‐Moses, National Child Health Coordinator; Dr Eric Siffah, Paediatrician, Princess Marie Louise Hospital; Dr Mary N.A. Brantuo, WHO; Dr Emmanuel Dzotsi, Public Health Division, GHS; Dr Nana Yaa Asante, Family Health Division, GHS; Dr Kwame Amponsa‐Achiano, Family Health Division, GHS; Dr Larko Owusu, KATH; Mr Eben Boahene, Greater Accra Regional Health Directorate; Ms Edna Adzigbli, Institutional Care Division, GHS; Mrs Christiana Akuffo, Institutional Care Division, GHS; Ms Faustina Asare, Koforidua Regional Hospital; and Mrs Margaret Kyei, Ridge Hospital. Many other people contributed in diverse ways — secretaries, drivers, hospital management teams, hospital staff, and the staff at the Ghana National Drugs Programme. Our gratitude goes to these individuals, as well as to the caregivers who patiently responded to our questions.

Assessment of quality of care for children in selected hospitals in Ghana
Page vi
Assessment of quality of care for children in selected hospitals in Ghana
Page vii
Executive summary
Improving quality of care is one of the priorities of the Ghanaian health sector and a number of initiatives have been put in place to achieve this goal, however, progress has been slow. The study, Assessment of quality care for children in selected hospitals in Ghana, was carried out as part of the Better Medicine for Children project in Ghana. Its purpose was to:
– assess the quality of paediatric care provided to children less than five years of age in selected hospitals by comparing aspects of paediatric care provided in these hospitals with prescribed standards of care;
– make recommendations for those facilities that were assessed to improve the gaps identified that fall within their mandate;
– make recommendations to guide national adaptation of guidelines to improve the quality of paediatric care in hospitals.
The assessment was carried out in 10 hospitals made up of one specialized children’s hospital, two regional hospitals and seven government district hospitals, including one faith‐based (mission) hospital. The WHO product, Assessment of the quality of care for children in hospitals: A generic assessment tool, was adapted by a group of experts using local standards and the WHO Pocket Book of Hospital Care for Children. A team of experienced health workers was trained on the use of the tools. The team then pre‐tested these tools, which were used to collect information from the selected hospitals. The key findings were as follows:
– Generally, hospital support systems were adequate (i.e. running water, electricity, backup generator, soap, etc.).
– Laboratory support was also good and laboratory results could be obtained in reasonable time (i.e. within two hours), although some hospitals did not carry out cerebrospinal fluid microscopy.
– Drugs needed for the management of common childhood illnesses were most often available at the pharmacy, but emergency drugs were not readily available on the wards and in emergency areas.
– There was a shortage of professional nurses; in most of the facilities, sick children were cared for by student nurses, health‐care assistants and ward aides who had inadequate skills and knowledge to do the job.
– There were gaps in the case management of common childhood illnesses, especially diarrhoea and malnutrition. Case management protocols and

Assessment of quality of care for children in selected hospitals in Ghana
Page viii
guidelines were most often not available. Best practice was observed in the management of children with HIV/AIDS where there were protocols and staff had been trained in their use.
– Monitoring the progress of sick children was poorly done and in some instances monitoring charts were not available.
– Ensuring adequate nutrition for sick children on admission was not considered part of the child’s management. This task was left to caregivers, with no supervision from health workers. Some hospitals did not provide food for inpatients.
– Barriers to accessing care included financial constraints (i.e. non‐insured clients), cultural beliefs, and transportation.
– Support for caregivers (i.e. hostel facilities, washing, etc.) was inadequate.
– Attitudes of health workers towards patients were varied and are best described as a mix of positive and negative viewpoints.
– Staff were concerned about the shortage of skilled personnel resulting in heavy workload.
Several recommendations were made, some of which include:
– Facility management should ensure that medicines and essential equipment are available in emergency areas and wards, and should determine a process for health staff to document what medicines have been administered and to account for the use of equipment.
– Case management needs to be improved through training and the provision of clinical care guidelines, including the use of monitoring charts and job aids. For this purpose, adaptation of the WHO pocket book is needed.
– Hospital management should invest in training staff in Integrated Management of Neonatal and Childhood Illness (IMNCI), management of acute malnutrition, Emergency Triage, Assessment and Treatment (ETAT), essential newborn care, and hospital care for the newborn.
– The policy on hospital feeding must be enforced and preparation of food by hospital caterers should take account of children who have been admitted.
– Training of nurses in paediatric care should be a priority. Negotiations that are currently under way should be accelerated to ensure early implementation of the programme.
– Guidelines for clinical audits must be developed and staff must be trained on its use. The regular conduct of clinical audits must be included in hospital managers’ performance indicators.
– The Ghana Health Service (GHS) customer care training should also be scaled up and hospitals encouraged to buy into the programme.

Assessment of quality of care for children in selected hospitals in Ghana
Page ix
– Facilitative and clinical supervision must be strengthened at all levels to ensure compliance with standards.
– The Ministry of Health (MOH)/GHS should designate best practice hospitals in paediatric care and use them for study tours and training sites and promote regular peer reviews.
– The health sector is implementing strategies to improve human resource output. Mechanisms for fair distribution must be instituted, as well as adequate compensation packages.
– The Paediatric Society of Ghana must press for the improvement of services for children in line with the recommendations in this report and promote local leadership for improvement among its members.
– Cost of hospital care is a significant barrier and communities must be encouraged to register all children in the National Health Insurance Scheme (NHIS) as they are in the exempt category.

Assessment of quality of care for children in selected hospitals in Ghana
Page x

Assessment of quality of care for children in selected hospitals in Ghana
Page 1
1. Introduction
1.1 Background
Improving the quality of paediatric care in hospitals is a key challenge in Ghana. An assessment of the hospital care for children in 2005 showed that the quality of care was not up to the standards recommended by WHO.1 Although the hospitals had good infrastructure such as available water and electricity, case management of common childhood conditions was below the recommended standard. Emergency care systems were not well established, there were no triaging systems in place, and the emergency units were not well equipped for managing emergencies. There was a lack of protocols and guidelines for in‐patient care of common childhood conditions (e.g. severe malaria, pneumonia, diarrhoea, malnutrition and HIV/AIDS) resulting in incomplete assessment, treatment and monitoring of cases. Some key recommendations were made following the assessment and included the introduction of emergency systems and provision of guidelines to support case management. As a result of these recommendations, the first training Emergency Triage Assessment and Treatment (ETAT) was conducted in the country in 2007, using WHO guidelines.2,3 The training included the introduction of the WHO Pocket Book of Hospital Care for Children,4 which provides guidelines on the management of common childhood illnesses. Training commenced in 2007, but limited funding resulted in the involvement of only a few facilities. An opportunity to scale up this initiative on improving the quality of care has now been provided by the Better Medicines for Children (BMC) project, which seeks to improve the availability and access to medicines for children in the country, in line with World Health Assembly Resolution 60.20 on BMC.5 One component of the BMC project is to adapt and produce guidelines for managing childhood illnesses in Ghana. WHO’s framework for quality improvement for hospital care for children6 outlines the steps needed to guide the quality improvement process in countries. This framework describes two key steps: 1) identifying stakeholders and 2) a situational analysis. This study assessed current paediatric care in hospitals in Ghana against established and accepted standards of care. The findings will provide the evidence to guide the national adaptation of guidelines and standard‐setting process. It is also aimed at improving the quality of paediatric care in hospitals.
1.2 Objectives
1. Assess the quality of paediatric care provided to children less than five years of age in hospitals by comparing aspects of paediatric care provided in hospitals with prescribed standards of care.
2. Make recommendations for those facilities that were assessed to improve the identified gaps that fall within their authority.

Assessment of quality of care for children in selected hospitals in Ghana
Page 2
3. Make recommendations to guide national adaptation of guidelines to improve the quality of paediatric care in hospitals.
1.3 Methodology
Study population
Ten facilities were purposefully selected for assessment. The selection of the facilities took into account regional and ecological differences, facility types (i.e. regional, district and specialist hospitals), and ownership (i.e. public and private/not‐for‐profit/faith‐based) hospitals. The following facilities were assessed:
– Northern Region: Tamale Central and Yendi Hospitals
– Volta Region: Volta Regional and Adidome Hospitals
– Ashanti Region: Bekwai and St Martin’s (Agroyesum) Hospitals
– Greater Accra Region: Princess Marie Louise (a children’s hospital) and Ada Hospitals
– Western Region: Kwesi Mintim and Tarkwa Government Hospitals
A team made up of paediatricians, public health physicians and nurses formed the working group with responsibility to oversee the adaptation process. The Institutional Care Division of the Ghana Health Service (GHS) led the process with support and collaboration from the Family Health Division and the Ghana National Drugs Programme. WHO was part of the working group and provided technical and administrative support to the process. The WHO generic assessment tool was reviewed and adapted to take into account disease conditions and the administrative set up within the health system of Ghana. The clinical management standards were based on the WHO Pocket Book of Hospital Care for Children,4 as well as the Standard Treatment Guidelines for Ghana.8 Ten assessors were selected to ensure a doctor–nurse team in each of the facilities to be visited. The assessors were trained on the use of the adapted tools, followed by pre‐testing in two hospitals not included in the facilities to be assessed. They worked together in teams and agreed on common criteria for assessing key areas of the facility as good or needing improvement.

Assessment of quality of care for children in selected hospitals in Ghana
Page 3
Facility visits were conducted from 7–10 June 2010 by five teams of assessors. Each team carried out the assessment of a hospital over a two‐day period. Each assessment was done through interviews with hospital managers and other health staff, review of documents and patient records, observation of patient management procedures, and interviews with staff, as well as caretakers of children. Information was gathered on:
– child morbidity and mortality;
– facility supports (i.e. drugs, equipment, supplies and laboratory services);
– emergency care;
– case management for neonates and children under five years of age;
– hospital set‐up to care for children;
– monitoring and supportive care;
– care‐seeking.
This assessment was considered to be a quality improvement exercise; for this reason, ethical clearance was not obtained. Letters were written to inform the regional and medical superintendents of the selected facilities for the visits, and follow‐up calls were made to ensure facility management were aware of the assessment. At the end of the assessment, the assessors debriefed the hospital managers and some key hospital staff. Each meeting presented the key findings of the assessment, focusing on the strengths and weaknesses observed and discussing actions to improve the care delivered.
2. Key findings
2.1 General hospital information
The facilities visited included one specialized children’s hospital, two regional hospitals and seven district hospitals, one of which was a faith‐based hospital. Two of the facilities were located in the northern zone, three in the middle belt, and five in the southern zones of the country. Four of the hospitals were in urban areas, while six were located in rural areas.
Layout of the facility
The hospitals did not have separate outpatient departments for children. Similarly there was no separate emergency area or ward for children in any of the hospitals visited. The emergency area was part of the general outpatient department (OPD) in most cases. All the hospitals visited had separate admission wards for children, and only four out of 10 had separate wards for sick newborns. For the hospitals that had isolation wards, none had a separate paediatric isolation ward. There was no neonatal intensive care unit (NICU) in any of the hospitals assessed. In six hospitals, the ward layout was such that children who were very ill were closest to the nurses’ station and therefore could receive more attention. Eight of the 10 hospitals had at

Assessment of quality of care for children in selected hospitals in Ghana
Page 4
least one qualified nurse per shift and this was complemented with auxiliary staff; e.g. ward assistants, health‐care assistants and student nurses. Two facilities kept sick children on the female ward during peak seasons, and neonates in the maternity ward as their neonatal units were not well equipped. One facility – a newly established district hospital referred all sick neonates to the next referral level – the regional hospital. In four of the hospitals, all children with surgical conditions were referred to other hospitals either because there were no theatres or no expertise to take care of them. In hospitals where paediatric surgeries were conducted, children were either admitted to the general paediatric ward or to the adult surgical ward. In one hospital, there was no doctor assigned to the paediatric ward; doctors had to be called on an ad hoc basis to attend to children which poses a challenge to under‐five and paediatric care. Assessors in one urban hospital observed that the shift system was especially weak as doctors do not wait to hand over before leaving their shift. Most hospital OPDs close at 17:00, after which children with emergencies were admitted straight to the wards.
2.2 Hospital infrastructure systems
Table1: Availability of hospital infrastructure
Number of facilities OPD/
Emergency Wards
Comments
Electricity continuously available 8 7 Backup power supply in the event of a power cut
9 8
Running water (pipe-borne) 10 10
Deep wells or bore-holes where the national water system was unavailable.
Soap and/or disinfectant available 10 9 A sharps disposal box available
6 8 Some of the boxes were improvised.
Functioning refrigerator available for drugs 3 8 Functioning refrigerator available for vaccines
Vaccines usually kept at the Reproductive and Child Health Unit of the District Health Administration.
Information desk or complaints/ suggestion box 9 1
The nurses’ station served the purpose of information desk on the ward.

Assessment of quality of care for children in selected hospitals in Ghana
Page 5
Generally, the support system was good. However, hospitals face power supply interruptions from the national grid, which affect the running of the emergency area/OPD and wards. Most of the hospitals assessed have a backup power supply. With the exception of one hospital, most of the backup power was from generators. Generators were usually turned off after about 22:00.
Veronica Bucket available in facilities that may not have a consistent supply of running tap water
Running water was available in the children’s ward and the emergency/OPD in all hospitals. For some hospitals, where the national water system was unavailable, water is piped in from deep wells or bore‐holes. Soap and disinfectants were available in the emergency areas or OPD and the children’s ward in most hospitals. There was a functioning refrigerator for drugs in the children’s ward in most of the hospitals, but this was not common in the emergency area or OPD. These refrigerators were used to store medicines, as well as water and food for staff in some of the hospitals. Refrigerators for vaccine storage were normally found in the Public Health unit in most of the hospitals and not on the children’s wards or in emergency areas or OPDs. Information desks were available in the emergency area or OPD, while the nurses’ station served the purpose of information desk on the children’s ward in most of the hospitals.
Hospital health statistics
The 2009 data available from six facilities show that the total annual outpatient attendance of children less than five years of age ranged from 3437 to 16748 children, for an average daily attendance ranging from 9 to 45 in the respective facilities. Age‐specific case fatality rate (CFR) was between 1% and 2% for all age groups in under‐fives. The hospitals’ annual health statistics were based on the District Health Information Management System (DHIMS). The DHIMS was not disaggregated to track children’s emergencies and neonates, as indicated in the standards used. The top five causes of admissions and deaths in children were similar in all the hospitals and included malaria, anaemia, acute respiratory infections/pneumonia, diarrhoeal diseases and septicaemia. In hospitals where surgeries were conducted, the top five most common
Assessment of quality of care for children in selected hospitals in Ghana
Page 6
surgeries included incision and drainage, hernia repair, hydrocoelectomy, excision of lumps, and repair of lacerations. Circumcision was commonly performed in the hospitals but not documented, thus records were not available in most cases. Additional surgeries carried out were reduction and immobilisation of fractures in one regional hospital, and skin grafting/reconstructive surgery in a district hospital within a buruli ulcer endemic area.
Essential drugs, equipment and supplies
The full complement of essential drugs, equipment and supplies needed for paediatric care were not available in all the facilities as shown in the table below. In some facilities, drugs were available at the pharmacy but were not found at the emergency area or ward. Also some programme drugs, such as anti‐tuberculous drugs, were managed at the District Health Directorate. Essential equipment and supplies, such as oxygen, nebulizers and glucometers, were not available in some children’s units. The hospital laboratories provided 24 hour support services in all the facilities visited, however some tests, such as cerebrospinal fluid (CSF) microscopy, blood grouping and cross‐matching, were not available in some of the facilities. If a differential diagnosis of meningitis was made, there was usually no way of confirming it due to the absence of a CSF microscopy test. In the case of one hospital, a private firm provides laboratory services. In most facilities, other emergency laboratory tests, such as haemoglobin, blood film, and grouping and cross matching, were provided not only during regular business hours, but also at night, at weekends and during holidays. Most of the laboratory tests were able to be done within two hours and for inpatients, the results were obtained within 24 hours.
Table 2: Availability of drugs, equipment, supplies and laboratory support
Number of facilities out of 10 found to be: Care assessed Good In need of some
improvement Comments
Availability of essential drugs 4 6 Availability of paediatric equipment 2 8 Infant-sized equipment not
available in some facilities. Adequate equipment is available in the emergency area and on the ward
2 8
Essential laboratory tests available and timely
4 6 Testing for CSF not available in all facilities.
2.3 Emergency care services
Patient flow
There was no separate outpatient department for children in any of the health facilities and children joined adults in the same queue for their hospital cards in all the facilities. There were designated health professionals to see sick children at the OPD in three facilities. Two had paediatricians, while in the other a staff member trained in integrated management of children’s illnesses (IMCI) solely sees children less than five years of age. All sick children at these three facilities, including emergencies and severely ill children, were received at the same place in the OPD.

Assessment of quality of care for children in selected hospitals in Ghana
Page 7
None of the facilities had the requisite layout, protocols, medications and staff capacity to provide emergency services according to the standards, as shown in Table 3.
Table 3: Management of emergencies
Number of facilities out of 10 found to be:
Good Needs to be improved
Comments
Layout and physical structure of the emergency department
1 9
Adequate staffing 0 10
Availability of essential drugs 5 5 Availability of essential laboratory support
6 4
Availability of essential equipment 2 8 Practice and case management of emergency conditions
3 7
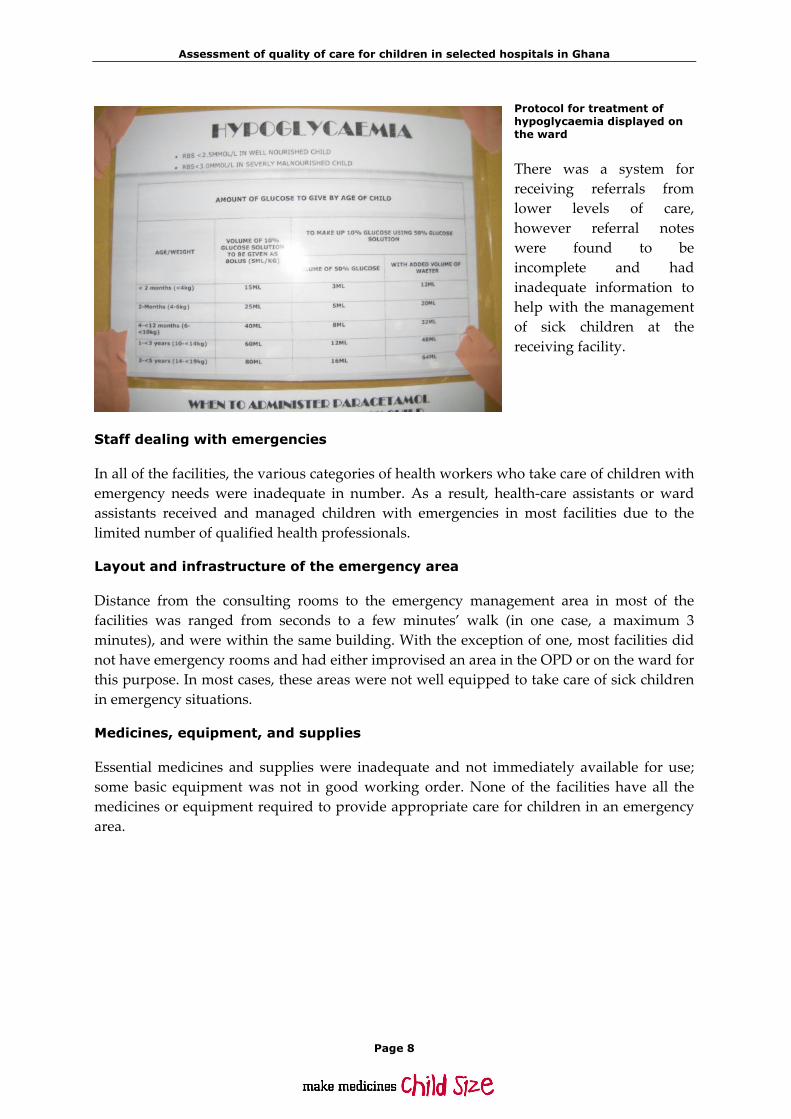
A triaging system was in place in only one hospital where the health‐care assistant is trained in Emergency Triage and Assessment and Treatment (ETAT). Health workers in other hospitals identified seriously ill children using a range of systems from a nurse going round looking for seriously ill children to announcements through a public address system calling for mothers with seriously ill children to report at the nurses’ station. In the absence of proper triaging, seriously ill and emergency patients were missed and had to wait in the queue to be seen. The exception was those with obvious emergencies, like seizures. Qualified health professionals were always available but most of them have not been trained in ETAT and therefore do not have adequate skills to manage emergencies. Protocols, or job aids to guide the management of emergencies, were not available in most of the facilities. The few that were displayed need to be updated and also contained very scanty information. Commonly displayed on walls were memos and notices that were very old, having outlived their usefulness and no longer relevant to the care of sick children. Three facilities had some staff trained in ETAT, as well as charts and protocols displayed on the walls in the children’s ward.
Assessment of quality of care for children in selected hospitals in Ghana
Page 8
Protocol for treatment of hypoglycaemia displayed on the ward
There was a system for receiving referrals from lower levels of care, however referral notes were found to be incomplete and had inadequate information to help with the management of sick children at the receiving facility.
Staff dealing with emergencies
In all of the facilities, the various categories of health workers who take care of children with emergency needs were inadequate in number. As a result, health‐care assistants or ward assistants received and managed children with emergencies in most facilities due to the limited number of qualified health professionals.
Layout and infrastructure of the emergency area
Distance from the consulting rooms to the emergency management area in most of the facilities was ranged from seconds to a few minutes’ walk (in one case, a maximum 3 minutes), and were within the same building. With the exception of one, most facilities did not have emergency rooms and had either improvised an area in the OPD or on the ward for this purpose. In most cases, these areas were not well equipped to take care of sick children in emergency situations.
Medicines, equipment, and supplies
Essential medicines and supplies were inadequate and not immediately available for use; some basic equipment was not in good working order. None of the facilities have all the medicines or equipment required to provide appropriate care for children in an emergency area.

Assessment of quality of care for children in selected hospitals in Ghana
Page 9
Some of the equipment at an emergency area
The equipment and supplies for emergency care that were commonly absent were:
– intravenous infusion (giving) sets with paediatric chambers;
– spacers with mask for administration of inhaled salbultamol;
– suction machines;
– weighing scales;
– self‐inflating bags for respiratory support;
– oxygen;
– nasogastric tubes (especially size 12).
Case management of emergency conditions
Case management of paediatric emergencies was better in facilities that had paediatricians. In facilities without paediatricians, health workers caring for sick children under five years of age often lacked adequate skills to recognize and manage paediatric emergencies.
2.4 Paediatric ward
Layout
Most facilities have a separate room or ward for children. The number of beds range from six to 31, which includes cots and adult‐sized beds, some without side rails. Children from birth to 12 years were admitted to these wards. Beds were well‐spaced and had mattresses; however, some patients did not receive bed sheets in some facilities. In these cases, the number of beds were not adequate and newly admitted patients had to wait for discharges to be made before they obtained beds. Insecticide‐treated nets were available in some wards but were not being used. Blankets were not routinely given to patients. Emotional support and play opportunities (toys) were available in only two facilities. In most of the facilities, meals were not provided for children on admission. Hostels or other

Assessment of quality of care for children in selected hospitals in Ghana
Page 10
lodging facilities for caretakers were not in existence, and toilets and bathrooms for sick children and their carertakers were inadequate and in poor condition. However, the wards were fairly clean and dangerous items were kept out of the reach of children.
Paediatric ward staffing
There was a shortage of all categories of health workers in all the hospitals visited. In some facilities, children’s wards were being managed by student nurses or health or ward assistants. However, there was always a doctor or medical assistant on call.
2.5 Case management of common conditions
Cough or difficult breathing
As shown in Table 4, health workers correctly assessed and diagnosed pneumonia and recognized severity of illness in three out of the 10 facilities. In the other facilities, although correct diagnosis was made, there was no classification of the severity of the pneumonia. The signs required for diagnosing and classifying pneumonia, such as respiratory rate, chest in‐drawing and subcostal recession, were not documented. This was important in determining the level of care for the sick child, as well as in reviewing the patient to ascertain if there had been an improvement or deterioration in their condition. Once the diagnosis of pneumonia was made, administration of antibiotics was considered appropriate in all facilities. Broad spectrum antibiotics, such as ampicillin, gentamycin or ceftriazone, were given. Patients with pneumonia were regularly reviewed in eight out of the 10 facilities and other diagnoses were considered.
Table 4: Management of cough or difficult breathing
Performance of hospitals (Number of hospitals out of 10)
Standards of care assessed
Good Needs to be improved
Cough/difficult breathing
Severity of pneumonia is correctly assessed and diagnosed 3 7
Appropriate antibiotics are administered for pneumonia 10 0
Oxygen is correctly administered when necessary 8 2
Correct use of chest x-ray 5 5
Appropriate diagnosis and management of tuberculosis 6 4
Inhaled bronchodilators are given appropriately, when indicated 7 3
Patient monitoring appropriately performed and charted 2 8
Supportive care provided appropriate for condition 3 7
In most facilities, oxygen was administered correctly to all children who needed it using nasal prongs or nasal catheters. However, in some cases, nasal prongs were reused. Some health staff used a much higher rate of oxygen flow compared to the recommended standard of 1‐2 litres per minute.

Assessment of quality of care for children in selected hospitals in Ghana
Page 11
The use of chest X‐rays in the diagnosis and management of pneumonia was good in five facilities. In the others, chest X‐rays were not requested for young infants with pneumonia, and in one facility chest X‐ray equipment was not available. Asthma was considered as a differential diagnosis of wheezing illness and children in need of bronchodilators were correctly identified or diagnosed. However, the management was inadequate as inhaled bronchodilators (including nebulizers) were available in only half of the facilities assessed. Follow up of children with asthma varied. It was best in one hospital that had an asthma clinic. Anti‐tuberculous treatment was given according to national guidelines in six facilities. In one hospital, cases with tuberculosis (TB) were referred to the regional hospital for management as the unit was not yet set up. In other hospitals, TB was not considered as a differential diagnosis in unresolved pneumonia or malnutrition as recommended by the standards.
Diarrhoeal conditions
Table 5: Management of diarrhoeal conditions
Standards of care assessed Performance of hospitals (Number of hospitals out of 10)
Good Needs to be improved
Diarrhoea
Dehydration is correctly assessed 5 5
Rehydration plan is appropriate to severity of dehydration, and rehydration appropriately monitored
4
6
Appropriate antibiotics only given when necessary 7 3
Appropriate (continued) feeding given during diarrhoea 2
8
From the review of patient case notes, it was observed that the signs for assessing dehydration were not documented, and dehydration was not correctly classified in half of the facilities. An adequate rehydration plan for managing diarrhoea was observed in less than half of all facilities. Some hospitals indicated the plan being used, whereas others gave no indication. Children were put on intravenous fluids — 1/5 normal saline in dextrose, ringers lactate, normal saline or oral rehydration therapy — however, they were not monitored appropriately. There were no input–output charts for the children with diarrhoea. Antibiotics were inappropriately used in the management of diarrhoea in three out of the 10 hospitals. Co‐trimoxazole, amoxicillin, or metronidazole were given in cases of diarrhoea when no signs of dysentery were present. In accordance with set standards, proper anti‐diarrhoea drugs were not administered in any of the hospitals. Feeding of children with diarrhoea was appropriate in only one facility. In the other facilities, there was no supervision or documentation of feeding by hospital staff, hence caregivers fed children using their own discretion. This has implications for the quality of care as traditionally food was withheld from children with diarrhoea. Related to this area of weakness was the inadequate

Assessment of quality of care for children in selected hospitals in Ghana
Page 12
monitoring and supportive care provided to children being treated for diarrhoea. This was attributed to the limited numbers of nursing staff available to care for the patients on the ward.
Fever
The assessment of fever considering differential diagnosis for other possible conditions was appropriate in three facilities (see Table 6). Some gaps observed in the other facilities included inadequate assessment and investigation to exclude other infections of the ear, throat and urinary tract.
Table 6: Management of fever
Standards of care assessed Performance of hospitals (Number of hospitals out of 10)
Good Needs to be improved
Fever
Differential diagnosis of fever considered and appropriate investigations undertaken
3
7
Correct diagnosis and management of meningitis 4 6
Severe complicated malaria correctly managed 6 4
Measles correctly managed 7 3
Other febrile conditions correctly managed 7 3
The diagnosis and management of meningitis was adequate in four facilities. In facilities where cerebrospinal meningitis was commonly seen during outbreaks, there was a system in place to perform lumbar punctures to confirm diagnosis. In other facilities, lumbar punctures were infrequently done due to limited expertise or the inability of the laboratory to conduct microbiological tests. Despite these limitations, once meningitis was suspected, adequate antibiotic treatment was started without delay in all but one facility. The preferred treatment for meningitis in that facility was cefuroxime (a second‐generation cephalosporin), which is not the drug of choice for meningitis. The recommended drug for meningitis was ceftriaxone (a third‐generation cephalosporin) which was available in that facility The complications of meningitis, such as hypoglycaemia and convulsions, were well‐managed in five hospitals. In the other hospitals, random blood sugar testing was not done for patients who were not on the National Health Insurance Scheme because of cost. Also some facilities gave dextrose intravenously, but did not pass nasogastric tubes for continued feeding. Monitoring of patients with meningitis was found to be inadequate as the state of consciousness, respiratory rate and pupil size were not charted. Diagnosis of malaria was confirmed in all facilities by microscopy or rapid diagnostic testing. The signs and symptoms required for making a diagnosis of severe malaria were not documented in a number of facilities. Intramuscular quinine was given in most facilities for severe malaria. One facility was found to be giving intravenous quinine, which needs very close monitoring and was not available in this particular hospital. Another facility gave
Assessment of quality of care for children in selected hospitals in Ghana
Page 13
intramuscular (IM) artemether to all suspected malaria cases irrespective of the severity. In one instance, a child was observed receiving both IM artemether and quinine.
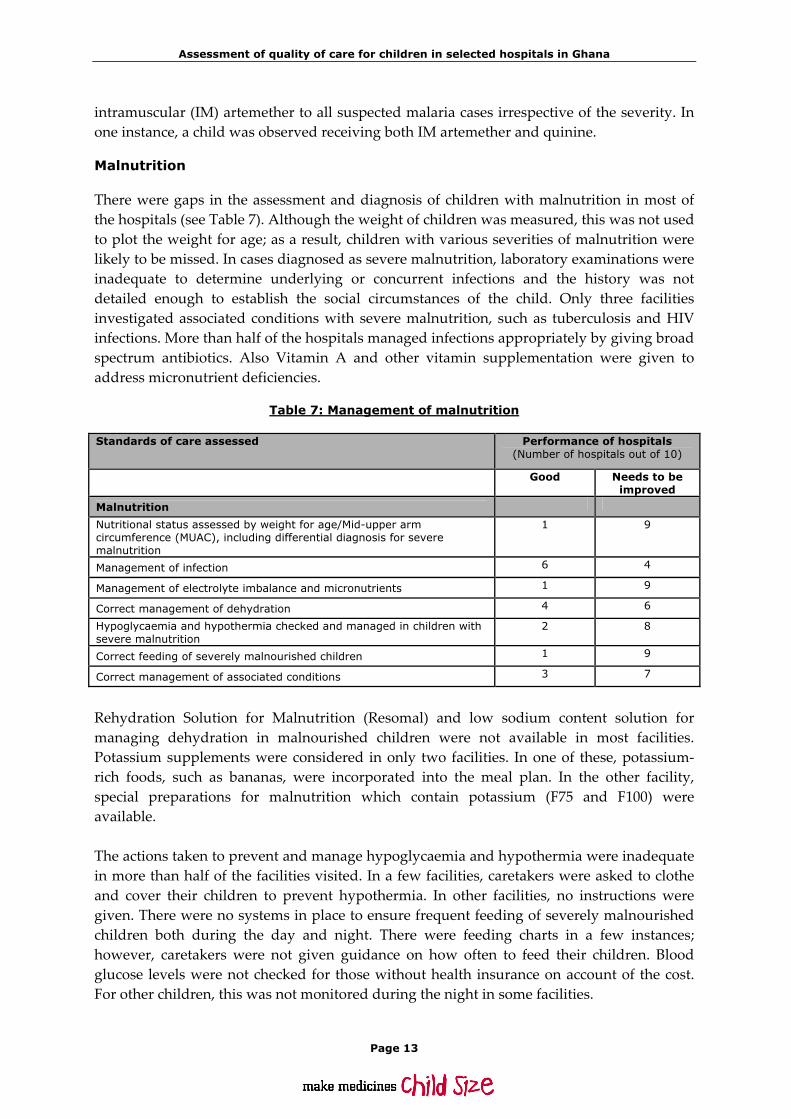
Malnutrition
There were gaps in the assessment and diagnosis of children with malnutrition in most of the hospitals (see Table 7). Although the weight of children was measured, this was not used to plot the weight for age; as a result, children with various severities of malnutrition were likely to be missed. In cases diagnosed as severe malnutrition, laboratory examinations were inadequate to determine underlying or concurrent infections and the history was not detailed enough to establish the social circumstances of the child. Only three facilities investigated associated conditions with severe malnutrition, such as tuberculosis and HIV infections. More than half of the hospitals managed infections appropriately by giving broad spectrum antibiotics. Also Vitamin A and other vitamin supplementation were given to address micronutrient deficiencies.
Table 7: Management of malnutrition
Standards of care assessed Performance of hospitals (Number of hospitals out of 10)
Good Needs to be improved
Malnutrition
Nutritional status assessed by weight for age/Mid-upper arm circumference (MUAC), including differential diagnosis for severe malnutrition
1 9
Management of infection 6 4
Management of electrolyte imbalance and micronutrients 1 9
Correct management of dehydration 4 6
Hypoglycaemia and hypothermia checked and managed in children with severe malnutrition
2 8
Correct feeding of severely malnourished children 1 9
Correct management of associated conditions 3 7
Rehydration Solution for Malnutrition (Resomal) and low sodium content solution for managing dehydration in malnourished children were not available in most facilities. Potassium supplements were considered in only two facilities. In one of these, potassium‐rich foods, such as bananas, were incorporated into the meal plan. In the other facility, special preparations for malnutrition which contain potassium (F75 and F100) were available. The actions taken to prevent and manage hypoglycaemia and hypothermia were inadequate in more than half of the facilities visited. In a few facilities, caretakers were asked to clothe and cover their children to prevent hypothermia. In other facilities, no instructions were given. There were no systems in place to ensure frequent feeding of severely malnourished children both during the day and night. There were feeding charts in a few instances; however, caretakers were not given guidance on how often to feed their children. Blood glucose levels were not checked for those without health insurance on account of the cost. For other children, this was not monitored during the night in some facilities.

Assessment of quality of care for children in selected hospitals in Ghana
Page 14
Severely malnourished children were correctly fed in two of the facilities visited. Commercially prepared or ready‐to‐use therapeutic foods (RUTF) and regimens, such as F75, F100, and “Plumpy’nut”, were not available in several of the facilities. In two facilities, F75 was prepared by the hospitals using milk, sugar, vegetable oil and cereal flour as recommended in the recipe. In another facility where “Plumpy’nut” was available, it was not used in accordance with the standards established for managing children with severe malnutrition. Frequent feeding during the day and night was observed in only two facilities. Generally, the feeding was left to the caretaker with no guidance on frequency. There was no documentation in most facilities to indicate the daily intake and weight gain of malnourished children, which is critical for monitoring a child’s progress. Most facilities observed correct treatment of associated conditions of malnutrition. Other clinicians, such as the eye nurse, were involved in the management of various conditions associated with malnutrition. There were no protocols in place for managing malnutrition in most facilities and this was compounded by the lack of dieticians to provide guidance in most hospitals on feeding malnourished children. Also, children with severe anaemia received blood transfusions. Sensory stimulation for children with severe malnutrition, through the provision of toys for play, was good in only two facilities.
HIV/AIDS
Table 8: Management of children with HIV/AIDS
Standards of care assessed Performance of hospitals (Number of hospitals out of 10)
Good Needs to be improved
Children with HIV
HIV tests used correctly and when indicated 10 0
Professional counselling services are in place with confidentiality ensured 9 1
Antiretroviral (ARV) treatment follows national guidelines 8 2
Nutritional advice provided 7 3
Immunizations and co-trimoxazole-prophylaxis administered correctly 10 0
Opportunistic infections correctly diagnosed/treated 8 2
Patients are referred for home-based care and palliative care focuses on symptom control
4
6
The management of HIV/AIDS was found to be either good or in little need of improvement in nine of the facilities visited. There were protocols for managing patients, in the form of charts, booklets and patient folders, which provided detailed guidance for the health staff managing the cases. The main area of weakness was supportive care and follow up on infected children.
Assessment of quality of care for children in selected hospitals in Ghana
Page 15
A few hospitals did not have any links for referring patients to home‐based care groups. Health workers observed that some of the patients lost interest in these groups after a short period of engagement. It was also observed that in cases where a child’s parents had died, the caregivers were more reluctant to attend follow up.
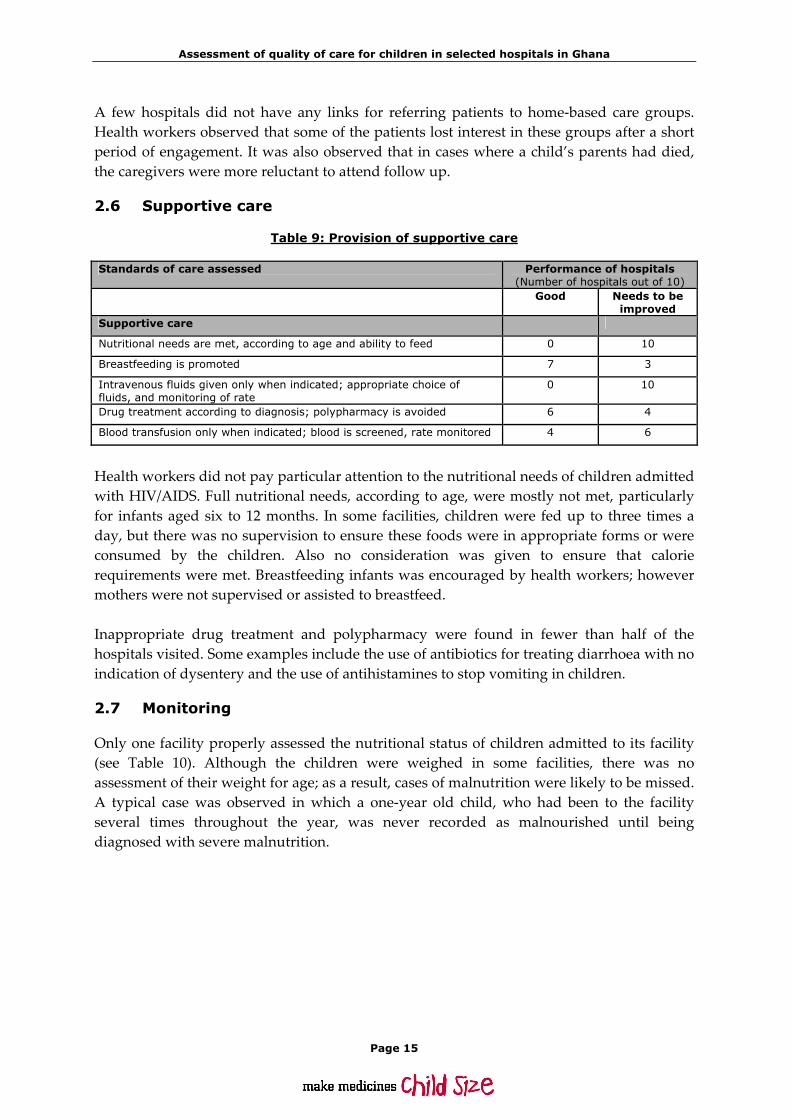
2.6 Supportive care
Table 9: Provision of supportive care
Standards of care assessed Performance of hospitals (Number of hospitals out of 10)
Good Needs to be improved
Supportive care
Nutritional needs are met, according to age and ability to feed 0 10
Breastfeeding is promoted 7 3
Intravenous fluids given only when indicated; appropriate choice of fluids, and monitoring of rate
0 10
Drug treatment according to diagnosis; polypharmacy is avoided 6 4
Blood transfusion only when indicated; blood is screened, rate monitored 4 6
Health workers did not pay particular attention to the nutritional needs of children admitted with HIV/AIDS. Full nutritional needs, according to age, were mostly not met, particularly for infants aged six to 12 months. In some facilities, children were fed up to three times a day, but there was no supervision to ensure these foods were in appropriate forms or were consumed by the children. Also no consideration was given to ensure that calorie requirements were met. Breastfeeding infants was encouraged by health workers; however mothers were not supervised or assisted to breastfeed. Inappropriate drug treatment and polypharmacy were found in fewer than half of the hospitals visited. Some examples include the use of antibiotics for treating diarrhoea with no indication of dysentery and the use of antihistamines to stop vomiting in children.
2.7 Monitoring
Only one facility properly assessed the nutritional status of children admitted to its facility (see Table 10). Although the children were weighed in some facilities, there was no assessment of their weight for age; as a result, cases of malnutrition were likely to be missed. A typical case was observed in which a one‐year old child, who had been to the facility several times throughout the year, was never recorded as malnourished until being diagnosed with severe malnutrition.

Assessment of quality of care for children in selected hospitals in Ghana
Page 16
Table 10: Monitoring progress of admitted children
Standards of care assessed Performance of hospitals (Number of hospitals out of 10)
Good Needs to be improved
Monitoring Nutritional status is assessed in all admitted children 1 9
Each child’s progress is individually monitored, and charts are used 2 8
The most ill children receive the highest attention 4 6
All admitted children are appropriately reassessed by a nurse 5 5
All admitted children are appropriately reassessed by a doctor 7 3
Monitoring of patients’ progress was not done in most of the facilities. A monitoring plan was available in only two facilities to assess the severity of a patient’s condition at the time of their admission. Standard monitoring charts were available for tracking temperature, pulse, respiratory rates and treatments given, but weight, blood pressure and feeding of children were not routinely monitored. It was also observed that vital signs were not checked correctly. In other facilities, only temperature was routinely checked and other signs, such as pulse and respiratory rate, were not monitored, even in children with all forms of pneumonia. Inadequate staffing was given as the reason for not monitoring patients correctly. In addition, some of the health workers lacked adequate knowledge and skills to identify complications and assess the severity of illness. In one facility, the only qualified nurse on the children’s ward was on duty from the morning until 15:00, so supervision was not adequate in the afternoons, at night, at weekends or at holidays. The doses and times for administering medications were properly documented in more than half of the facilities. The main gap observed in most facilities was the inadequate monitoring of administered intravenous fluids. There were no input and output charts, and there were no intravenous infusion (giving) sets to regulate the amount of fluid a child received (dorsiflow infusion sets, or infusion sets with calibrated burettes). The exception was in the specialized children’s hospital, where monitoring of malnourished children was found to be good. In this facility, oxygen saturation was also checked in children with respiratory distress. In eight facilities, patients who were admitted were seen by a doctor at least once a day. In two facilities, the number of doctors and nurses assigned to the children’s ward was inadequate. As a result, children were reviewed once or twice a week by a doctor. Follow up of children after discharge was not routinely done in any of the visited facilities. In one facility, a staff member indicated that provisions were made for follow up, but caretakers and patients usually did not return. A discharge note explaining the child’s condition was not always provided due to heavy workload and inadequate staffing.

Assessment of quality of care for children in selected hospitals in Ghana
Page 17
2.8 Neonatal care
Nursery staffing and layout
There was generally a shortage of staff designated for neonatal care in all of the facilities. However, staff were available on call during the weekends and at night to attend to deliveries. Only three facilities had nurseries for sick newborns, two of which had limited capacity for all the cases seen. The absence of nurseries was due mainly to inadequate space. At one of the regional hospitals, the nursery was not in operation due to staffing shortages. Sick neonates born outside the hospital or those older than two weeks were admitted to the children’s ward. In other facilities, all sick newborns were admitted to the children’s ward or the maternity ward. These wards were not well equipped with appropriate equipment vital for managing neonates.
Routine neonatal care
Table 11 shows a breakdown of facilities that adhered to various standards of routine neonatal care. Nine facilities out of the 10 visited conducted deliveries.
Table 11: Routine care for newborns
Standards of care assessed Performance of hospitals (Number of hospitals out of 10)
Good Needs to be improved
Routine neonatal care assessed in nine facilities conducting deliveries
Resuscitation procedures are correctly performed 5 4
Early and exclusive breastfeeding is promoted, skin contact is ensured 9 1
Clean delivery and newborn care is practiced 8 1
Thermal protection is practiced 7 3
Eye and Vitamin K prophylaxis and immunizations are given 3 7
Five of the facilities had written guidelines for neonatal resuscitation based on WHO recommendations, as well as resuscitation equipment, such as functioning, self‐inflating bags with newborn and premature size masks. It was observed that where guidelines were available, they were not always followed. Facilities that applied the guidelines had staff who had been trained in their use. Early and exclusive breastfeeding and skin contact was initiated immediately within the first half‐hour post‐delivery in all nine facilities where deliveries took place. Infant formula was not promoted by staff or distributed to mothers. Clean delivery were conducted using sterile instruments and proper hand hygiene, i.e. birth attendants washed their hands before and after each delivery, wore gloves and used sterilized instruments. Good thermal care for neonates was practiced in seven out of nine hospitals that conduct deliveries. The newborns were kept in a warm room, wrapped with dry cloth, and given to their mothers for breastfeeding. Bathing was done six hours post‐delivery. Problems
Assessment of quality of care for children in selected hospitals in Ghana
Page 18
identified in the two facilities that needed improvement were early bathing of neonates (i.e. within 30 minutes of delivery), and inadequate monitoring of body temperature. Eye prophylaxis, Vitamin K (ketamine), and immunizations (BCG for TB and OPV0 for polio) were given according to national guidelines in only three facilities. In one facility, it was explained that the evidence for giving Vitamin K was not clear to them, and no problems had been observed among neonates who had not received it. Because of this lack of clarity, the doctor in charge questioned the need for administering Vitamin K to normal neonates with no bleeding disorder.
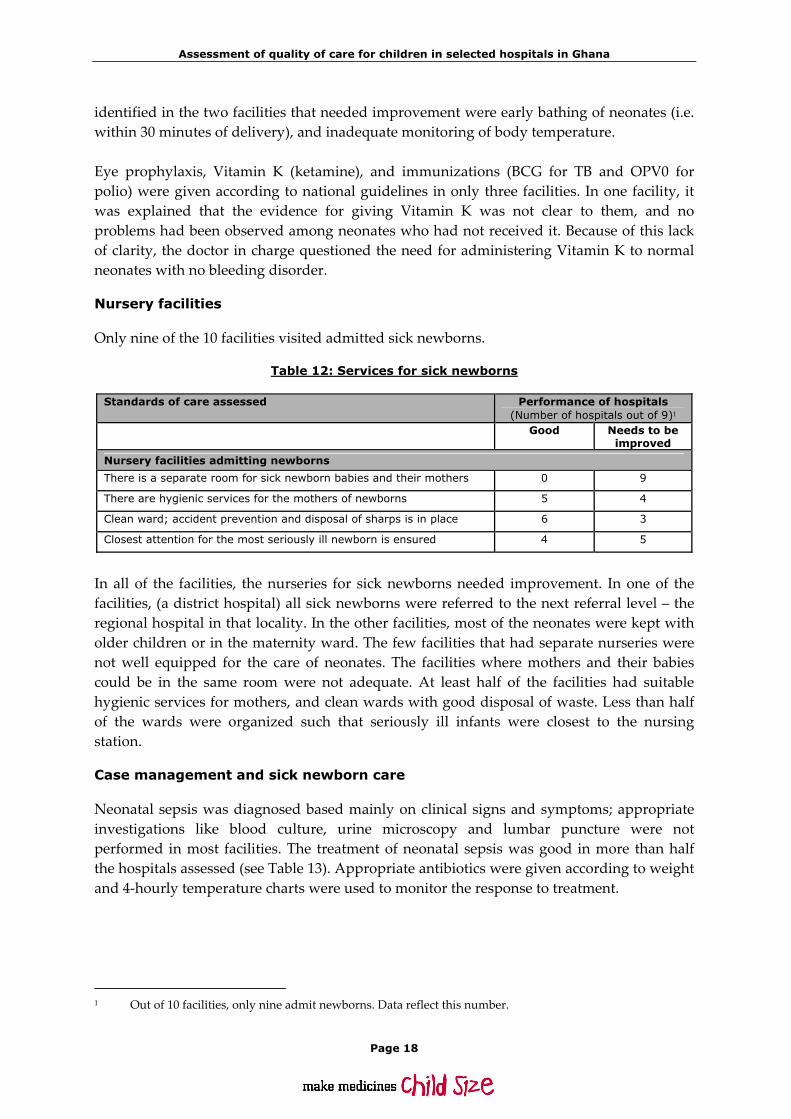
Nursery facilities
Only nine of the 10 facilities visited admitted sick newborns.
Table 12: Services for sick newborns
Standards of care assessed Performance of hospitals (Number of hospitals out of 9)1
Good Needs to be improved
Nursery facilities admitting newborns
There is a separate room for sick newborn babies and their mothers 0 9
There are hygienic services for the mothers of newborns 5 4
Clean ward; accident prevention and disposal of sharps is in place 6 3
Closest attention for the most seriously ill newborn is ensured 4 5
In all of the facilities, the nurseries for sick newborns needed improvement. In one of the facilities, (a district hospital) all sick newborns were referred to the next referral level – the regional hospital in that locality. In the other facilities, most of the neonates were kept with older children or in the maternity ward. The few facilities that had separate nurseries were not well equipped for the care of neonates. The facilities where mothers and their babies could be in the same room were not adequate. At least half of the facilities had suitable hygienic services for mothers, and clean wards with good disposal of waste. Less than half of the wards were organized such that seriously ill infants were closest to the nursing station.
Case management and sick newborn care
Neonatal sepsis was diagnosed based mainly on clinical signs and symptoms; appropriate investigations like blood culture, urine microscopy and lumbar puncture were not performed in most facilities. The treatment of neonatal sepsis was good in more than half the hospitals assessed (see Table 13). Appropriate antibiotics were given according to weight and 4‐hourly temperature charts were used to monitor the response to treatment.
1 Out of 10 facilities, only nine admit newborns. Data reflect this number.

Assessment of quality of care for children in selected hospitals in Ghana
Page 19
Table 13: Management of neonatal conditions
Standards of care assessed Performance of hospitals (Number of hospitals out of 9)
Good Needs to be improved
Sick newborns
Neonatal sepsis is appropriately diagnosed 2 7
Neonatal sepsis is appropriately treated 6 3
Specific feeding needs of sick young infants and those with low birth weight are met
3 6
Jaundice is adequately recognized and managed 3 6
Mothers were encouraged to breastfeed, but there were no feeding charts to monitor intake, particularly by low birth weight neonates. There were no dosiflow or infusion (giving) sets with calibrated burettes to adequately monitor intravenous fluids and prevent fluid overload. Kangaroo mother care was practiced in very few hospitals. Only two hospitals were set up for exchange transfusion and phototherapy, although all the laboratories could measure serum bilirubin levels. In one facility, jaundiced neonates were put in the early morning sun.
2.9 Paediatric surgerical care and rehabilitation
The standards of paediatric surgical care and rehabilitation are shown in the box below.
Standards of paediatric surgical care and rehabilitation
– Pre‐operative care was child‐friendly and fasting was kept to a minimum.
– Intra‐operative routine procedures prevent hypothermia and hypoglycaemia.
– Post‐operative care ensures safe recovery, including monitoring, pain relief and early feeding.
– The surgical ward was child friendly, provided food for children and opportunities for play.
– Paediatric size anaesthesia equipment was available (see Table below).
– Basic rehabilitation equipment was available.
Four facilities did not have surgical theatres and thus referred all surgical cases to better‐equipped hospitals. Only one facility had written standard procedures (i.e. a surgical pre‐operative checklist) in place to prepare a child for surgery. None of the facilities had written guidelines for the safe use of local anaesthetics. In most cases, the surgeon’s notes on the procedures that were performed were scanty. Post‐operative monitoring was infrequent due to staff shortages and inadequate infrastructure. Oxygen and suction equipment were readily available in most cases, but there were no guidelines on post‐operative pain management. After surgery, children were allowed to eat only after the doctor had seen the patient and given the go ahead. In all cases,

Assessment of quality of care for children in selected hospitals in Ghana
Page 20
medical and surgical cases were kept in the same room. Some facilities had a few toys for children to play with. Physiotherapy and rehabilitation facilities were available in only one facility. Staff complained that items like toys and crutches were often lost after children were discharged. Paediatric blood pressure cuffs were only used in one facility where the physiotherapy unit was privately owned and a patient could be seen for GHC 5.00 a day.
2.10 Other hospital wards with children
Only two of the facilities admitted children in wards or units other than the children’s ward. Children at these hospitals were either kept in the female ward during peak seasons or in the maternity ward, since the neonatal units were not well equipped. Very sick neonates were referred to other hospitals. Staffing was inadequate in all the wards. Midwives on the maternity ward also attended to sick neonates in addition to their mothers, thus compromising the level of monitoring for the neonate and the mother. Supplies and equipment, such as oxygen, were also inadequate and limited in quantity.
2.11 Hospital administration
Availability of adequate and updated treatment guidelines
Recent paediatric textbooks were found in two of the facilities. In the other facilities, a mix of current and out‐dated textbooks were found. Standard Treatment Guidelines were common, but there were no complementary wall charts or protocols. Wall charts and protocols on newborn resuscitation, in particular, were also not seen in most of the facilities. The most commonly seen charts were for managing fever, convulsions, and hypoglycaemia. Others included information for managing sickle cell crisis, cerebral malaria, asthma, severe anaemia and diarrhoea.
Performance of audits
Audits were organized in various forms in the facilities. A few facilities held audits once a month, while others held them when “time allow[ed]”. Clinical meetings were not a regular feature in most of the facilities. In a few facilities, the conduct of mortality audits was regular, but there was no clarity on the follow‐up actions to address problems identified. Not all the required staff categories participated in the audit meetings.
Transport for referral
Eight of the facilities assessed had ambulances, most of which were in poor condition. Some facilities relied on the National Ambulance Service, but this was sometimes unreliable. First‐level facilities lacked ambulances.
2.12 Access to hospital care
Referral by first level or primary health care
Referral notes written by first‐level workers did not have IMCI classifications. In some districts, medical assistants in surrounding subdistricts had been trained in IMCI, but the

Assessment of quality of care for children in selected hospitals in Ghana
Page 21
classifications were not being used. In addition, not all patients who were given referred had notes. In some of the cases, patients’ referral notes were not completely filled out (e.g. pre‐referral treatments or signs and symptoms of illness were not provided).
Transportation to hospitals
Geographically, most of the hospitals were accessible to their patients. For those living in island communities, hospitals were not situated in favourable areas as clients/patients had to rely on boats for transportation. Referrals were sometimes delayed due to a lack of transport options. A majority of those who were interviewed came to hospitals by commercial transport, such as taxis or minibuses. Only a few travelled in private vehicles. In all cases, availability and cost of transportation, especially in chartered taxis in the case of emergencies, was very expensive, often costing as much as GHC 30.00 within the Accra metropolitan area.
Care-seeking by parents
Most caretakers who were interviewed were able to recognize the signs and symptoms that require a visit to a hospital. However, despite this recognition, there were significant delays due to a number of factors, including: ignorance, cultural beliefs, lack of money, transportation difficulties, and so forth. Some caretakers said they visited chemical or pharmacy shops first before going to a hospital. For others, the hospital was their first choice. Caretakers of non‐insured children delayed reporting to a hospital because of cost implications; in some cases, seeking care from a prayer camp or traditional healer was a cheaper alternative. Cultural beliefs posed a barrier to care‐seeking. One caretaker said “I strongly believe in traditional medicine but only when the child is more than a year old, by which time the child’s intestines would be mature. I brought my child here because he is not yet one‐year old”. In another situation, a child who had convulsions was carried upside down and given to a male to send to a herbalist. Another child with fever was given herbal nasal drops and an enema. This child did not get better and only then was brought to a hospital. In the case of caretakers and patients from island communities, care seeking was hindered by the geographical location of health facilities.
Economic barriers to hospital care
The majority of clients or patients who visit some hospitals are not insured. Hospital fees pose a major barrier to hospital care for these clients. Some caretakers said they borrowed money for the care of a child, while others said they brought the child to the hospital with the hope that they would be allowed to pay the facility in instalments. Hospital fees were not officially communicated to caretakers. A few of those who were interviewed said they were told the fees only on request. In one facility, only fees for mortuary services were displayed. One caretaker said a nurse collected GHC 8.00 from her one night, explaining the fee was to pay for medication that had been administered through the child’s IV line.

Assessment of quality of care for children in selected hospitals in Ghana
Page 22
The management at one facility said that to help offset the economic burden on caretakers, prescribers often tried to stay within the limits of the insurance benefits package. Some hospitals employed social workers to make arrangements with non‐insured clients for the payment of hospital fees by instalments. In most cases, hospitals made a loss because the caretakers failed to pay for services received.
Traditional medicine
Some of the caretakers who were interviewed first visited traditional medicine practitioners prior to reporting to hospital thus causing delays in treatment. The managers of one facility reported, “The people are generally superstitious, so they prefer herbalists. Interestingly, most of those who patronize [their] services are insured, but they prefer to use herbal preparations alongside orthodox medicine”.
The experiences of caretakers in the outpatients’ department (OPD)
Positives
• Staff‐patient relationships were good.
• The reception given at the OPD was warm.
• Prompt attention was given to children and, in emergency situations, treatment was given before payment was demanded or before the folder was retrieved regardless of insurance status.
• Staff took their time to explain procedures to caretakers and generally exercised patience in their interactions. Caretakers were reassured of their child’s survival.
• In some cases, the waiting time was pleasantly short and, in cases where the child had high temperature, they were sponged down prior to seeing the prescriber.

Assessment of quality of care for children in selected hospitals in Ghana
Page 23
Negatives
• Some OPD bathrooms were an eyesore; the toilets were dirty and smelly.
• Caretakers were victims of insults by some staff at the OPD.
• One OPD was congested and had long waiting periods. There also was no separate queue for children.
• Caretakers experienced delays, because they had to join long queues to photocopy health insurance documents requested by the hospitals’ records staff.
• Some patients who reported to hospital before 6:00 were neglected by night nurses and made to wait until the arrival of the morning staff.
• Some patients had to wait to be admitted, because no beds were available.
• One caretaker mentioned that, although her child had a high temperature, none of the nurses at the OPD showed any concern.
Staff views
Health workers mentioned a number of factors necessary for improving the quality of child care. Some of the views expressed included:
– Inadequate staffing, resulting in shortages that affected staff of all grades, especially paediatricians, paediatric surgeons, general practitioners, nurses and midwives.
– Buildings need to be renovated.
– Most OPDs were shared by both children and adults, with prolonged waiting times for children.
– Some wards were found in a state of disrepair. Caretakers and sick children were often inundated by rain due to the absence of windows or louvre blades.
– The children’s wards were found to be particularly small and both surgical and medical cases were housed together.
– The wards were stuffy with some faulty fans seen hanging over sick children.
– Well‐equipped and well‐staffed nurseries are needed in most facilities.
– In terms of equipment, oxygen was mentioned as facing regular shortage. Some children’s units lacked refrigerators for storing essential drugs.
– Some beds needed side rails and screens, and bed sheets and blankets were inadequate.
– Stand‐by/back‐up generators were unable to supply power to some children’s wards during outages.

Assessment of quality of care for children in selected hospitals in Ghana
Page 24
– Brush and vegetation overgrowth surrounded some facilities, sheltering snakes and scorpions that were a threat to staff and patients.
– Most toilets and bathrooms needed urgent attention.
Staff’s perceptions on the common causes of death among children include malaria, pneumonia, diarrhoea, neonatal sepsis and malnutrition. Delay in seeking care was mentioned as the leading cause resulting in deaths. This was followed by lack of staff providing appropriate and adequate care and monitoring. Some staff believed they had the requisite skills to care for children, but they also mentioned emergency care and paediatric procedures/protocols as areas where they wished to be trained Reasons for staff dissatisfaction
• Inadequate staffing, resulting in work overload
• Delay in promotions
• Lack of motivation (e.g. transport for staff, drinking water)
• Lack of equipment
• Lack of refresher courses
• Failure on the part of supervisors to recognize the work of their staff
• Inadequate infrastructure
• Lack of funds for those in need
• Non‐involvement in decision‐making
• Inadequate communication of policies, etc.
3. Discussion
3.1 Children are not adults
Generally, there were separate wards for children, which was commendable. However, children who had undergone surgery were kept on adult wards. In some emergency units and at the OPD, children and adults were not separated. Treating children as adults and keeping them in the same queue has implications for prompt management of emergencies specific to children and generally have the tendency of quickly deteriorating into more severe situations. As a result of improper prioritization within the facility, caretakers often failed to understand the situation and, therefore, failed to complain when severely ill children were not given priority. In one of the hospitals, a practitioner trained in IMCI was given the sole responsibility for attending to children at the OPD.
Assessment of quality of care for children in selected hospitals in Ghana
Page 25
Most of the assessed facilities kept both healthy and sick newborns on their maternity units. This practice has to be reviewed in order to prevent cross‐infections and to allow adequate monitoring of sick newborns.
Location of the Nurses’ Station
The nurses’ station is a fulcrum of activity on an inpatient ward. Practically every function of the hospital intersects at this point, involving simultaneous clinical and administrative work processes. Standards for the location of nurses’ stations were met in most facilities. In some facilities, however, the station was located outside the ward, preventing direct oversight and delays in response to emergency situations. This type of set‐up arises when ward sizes are too small to accommodate a proper nurses’ station.
3.2 Staffing
An acute shortage of professional staff was observed in most health facilities. This can seriously compromise quality of care in many ways; e.g. treatments may not be given on time and time schedule and dosage for administration may not be followed. There may also be poor monitoring and documentation of progress of patients, etc. Time spent in providing care for individual patients may be inadequate. Student nurses or health assistants who complement staff are unlikely to have the requisite knowledge and skills and may be carrying out functions far beyond their competencies.
3.3 Support systems
Hospital support systems (i.e. water, electricity, etc.) were found to be adequate in most facilities. Hospital refrigerators for storage of medicines were also used to store water and food for staff. This practice is dangerous as food may be contaminated and frequent opening of the refrigerators minimizes optimal temperatures for safe storage of medicines. Hospitals were not child friendly; emotional support and play facilities were lacking in all but one hospital. Toilets and bathroom facilities were poor and lodging facilities for caretakers were non‐existent. Because of the lack of lodging or proper nutrition programmes, caretakers were often forced to sleep on the floors and to obtain food for themselves and their children. On the children’s wards, both cots and adult‐sized beds were available. Some have no side rails, which presents the potential danger of patients falling out their beds.
Assessment of quality of care for children in selected hospitals in Ghana
Page 26
3.4 Hospital data
The standards for hospital data for children were not met. There was no disaggregation for neonates. This could be traced to the DHIMS, which has made no provision for collection of such data. Data on emergency services were also not readily available. The top five causes of admissions and death were similar and include malaria, anaemia, acute respiratory infections/pneumonia, diarrhoeal diseases and septicaemia. This picture mirrors what pertains to the country as a whole. In hospitals where surgeries were performed, the top five most common surgeries include incision and drainage, hernia repair, hydrocoelectomy, excision of lumps and repair of lacerations. This may not reflect the whole picture, however, as circumcisions, which was often carried out by midwives, were not documented.
3.5 Drugs, equipment and supplies
Essential drugs and supplies were available in the pharmacies of most facilities, however on the wards and in emergency areas it was a different story. The lack of medicines in emergency units may be attributable to the difficulty in accounting for their use under the National Health Insurance Scheme (NHIS). As a result, patients with emergency conditions were required to have their prescriptions filled at the pharmacy in the hospital, leading to delays in initial treatment and managing emergencies. Basic equipment was also inadequate and often not available, including:
– Intravenous (giving) sets with paediatric chambers.
– Spacers with masks for administration of inhaled salbultamol.
– Suction machines.
– Weighing scales.
– Self‐inflating bags for respiratory support.
– Oxygen.
– Nasogastric tubes (especially size 12).
Laboratory support was good and results were often available within a reasonable time frame ranging from 30 minutes to 2 hours. The quality of laboratory tests, however, was not assessed in this study. In all the hospitals assessed, microscopy for cerebrospinal fluid was not done, thus the management of meningitis was based strictly on clinical diagnosis.
3.6 Emergency care
Improving emergency care is a priority in the Ghanaian health sector’s Programme of Work, yet inadequate attention has been paid to this area. As a result, emergency care was below standards with regard to infrastructure, equipment and staffing. Staffing was inadequate and among those staff who were available, some lacked the appropriate skills to manage emergencies. Health assistants who were not trained in emergency care were sometimes the only ones available to provide such care. Although GHS and WHO collaborated to organize

Assessment of quality of care for children in selected hospitals in Ghana
Page 27
training in ETAT for health staff in the northern and southern sectors, coverage is very low and the desired impact is thus not felt. Case management was better in facilities where there were paediatricians. This may be due to the fact that in‐service training in emergency care has not been institutionalized therefore medical doctors and other staff were not given opportunities to update their knowledge and skills.
3.7 Case management
Cough and difficult breathing
The assessment of sick children for pneumonia was not complete as patients with the disease were not classified for severity. As a result, patients with severe conditions were not properly monitored and complications were not identified. In general, the use of antibiotics was good. In a few facilities, the excessive use of third‐generation antibiotics may contribute to the development of resistance to antimicrobials. There were rarely problems with oxygen administration, but there were concerns about the reuse of nasal prongs as related to standards for infection prevention and control. Asthma was considered in the differential diagnosis of wheezing; however management and follow up need to be improved. The management of TB followed national guidelines, however the storage of TB drugs at district health directorates rather than in hospital pharmacies was surprising.
Diarrhoea
Although diarrhoea was common, the condition was not well managed in most cases. Rehydration plans were not used and monitoring was poor, with widespread lack of monitoring charts. The feeding of children was left to their caretakers and was not included in the management plan, therefore it was not supervised. Antibiotics were used in two facilities when there was no indication. It was encouraging to note that anti‐diarrhoeal agents were not used in any facility in accordance with the recommended standards.
Fever
The diagnosis and management of fever did not meet national standards. In a majority of the facilities, ear, nose and throat, and urinary infections were not considered for fever cases. Lumbar puncture and CSF microscopy were not carried out due to lack of skills. Monitoring of meningitis was generally poor, with little consideration for common complications in half of the facilities surveyed. Cost appears to be a barrier to testing for random blood sugar which, if found to be low, can often be easily corrected. On the other hand, the inability to diagnose low blood sugar can be fatal. The preferred use of intravenous fluids to the passage of nasogastric tubes for feeding unconscious patients could be due to the shortage of staff or lack of skills. This practice

Assessment of quality of care for children in selected hospitals in Ghana
Page 28
could adversely affect the nutritional status of children in prolonged states of unconsciousness. All of the assessed facilities were able to confirm malaria diagnosis due to the availability of microscopy or rapid diagnostic tests. The management of severe malaria varied among hospitals and included the inappropriate use of injection artemether and intravenous quinine in patients who were not monitored. Rapid administration of parenteral quinine is unsafe.1
Malnutrition
Less than half of the facilities diagnosed and managed malnutrition well. Areas of concern include inadequate assessment and investigation, lack of availability of rehydration solutions (i.e. Resomal) and preparations for feeding, inadequate feeding and poor documentation. This was due to inadequate staffing and the absence of protocols in most facilities. Although the training in management of Severe Acute Malnutrition (SAM) has started, coverage of this training is still very low and the impact is not obvious.
Case management and care of sick newborns
As with older children, case management for sick neonates was below standards. The same reasons given above for inadequate care for older children apply. There were no written guidelines for neonatal resuscitation in almost all the facilities visited. Neonatal sepsis diagnosis was based on clinical signs and symptoms. Appropriate investigations, including urine and CSF microscopy, blood culture and full blood count, were not done.
Children with HIV/AIDS
Management for HIV/AIDS patients was good. This was attributable to the level of support and funding for this programme which, over the years, has ensured training, availability of guidelines, protocols, equipment and drugs. The connection between home‐based care and hospital care remains an issue.
3.8 Supportive care
In most hospitals, supportive care for in‐patients was inadequate. The nutritional status of children who were admitted was not usually assessed, there was no monitoring plan, and monitoring was infrequent and poorly documented. Charts for monitoring (i.e. input‐output charts, feeding charts, etc.) were not available in some facilities. Where they were available, documentation was poor. The weak internal supervision could be a contributory factor.
3.9 Hospital support systems
Surgical facilities
Surgical facilities were not available in four out of the 10 facilities visited. Facilities did not have written standard procedures and guidelines for safe use of local anaesthetics, and post‐operative pain management guidelines were also unavailable. 1 Guidelines for the treatment of malaria ‐‐ 2nd edition. WHO Publication.
Assessment of quality of care for children in selected hospitals in Ghana
Page 29
Post‐operative notes were scanty and there were weaknesses in post‐operative monitoring. This aspect of care has not received much attention, even at the national level.
3.10 Hospital administration
Performance of audits
This activity, as well as clinical meetings, occurred infrequently and follow‐up actions could not be determined. Not all relevant staff participated when meetings were held. Lack of national guidelines and weak supervision at all levels could be among the contributing factors.
Transport for referrals
Most of the facilities have ambulances, however a majority of these were not in good condition. Coverage by the national ambulance service was limited to regional capitals and a few districts. There are plans to pool together ambulances to serve entire districts instead of individual facilities. This should improve the referral system.
Care seeking
Among those seeking care in hospital, delays in care were attributed to cultural beliefs, use of other systems, such as chemical sellers and traditional healers, and financial barriers (i.e. hospital fees for the uninsured). Care seeking has not been properly addressed as a strategy for improving child health.
Caretakers’ views
Caretakers gave mixed reviews of health workersʹ attitudes, a trend that has also been reported in other studies. GHS is concerned about the poor attitude of health workers and has instituted a customer care programme. Sleeping and toilet facilities for caretakers were inadequate and they sometimes slept on the hard floor because of a lack of lodgings.
Health worker interview
Health workers who were interviewed confirmed that staffing is inadequate in several categories for both inpatient and outpatient care. They were concerned about delays in attending to children in the OPD, including insufficient contact time with children and wards being managed by non‐professional staff, particularly at night and weekends. About one‐third of them identified this state of affairs as a possible cause of child deaths in health facilities. Dissatisfaction among staff was common with some of the reasons including work overload, lack of motivation and capacity building, lack of involvement in decision‐making, and inadequate communication between staff and management. Inadequate infrastructure, equipment and other resources for work were also mentioned as cause for frustration. It is refreshing to note that health workers were not only concerned about their own welfare, but also that of the children in their care, as well as the comfort and safety of children’s
Assessment of quality of care for children in selected hospitals in Ghana
Page 30
caregivers. Issues raised in this regard included the lack of feeding facilities or the poor quality of food provided for inpatients and the inadequate or, in some cases, poorly maintained toilet facilities. Common causes of death among children as identified by staff conform to the national picture, with malaria, pneumonia, diarrhoea, neonatal sepsis and malnutrition among the list of conditions. The consequences of delay in seeking care were most often identified as contributing to these deaths. This was followed by a lack of staff resulting in a parallel lack of care and monitoring. A majority of those who were surveyed did not identify insufficient drugs, equipment or laboratory diagnosis as contributors to death. Staff believe they have the requisite skills to care for children. However, they also mentioned emergency care and paediatric procedures/protocols as areas where many wish to receive training. The case management findings mentioned earlier, corroborates the training requisites made by staff as areas of weakness. Customer care was also identified as an area for improvement. The Ghana Health Service customer care package is currently available for training. GHS’ suggestion to use their own facilities and colleagues for on‐site training is laudable and may be a more cost effective and efficient means for scaling up in‐service training programmes. Useful suggestions were given on how to improve communication to caretakers and how to involve them in the provision of care. They identified the need for appropriate audio‐visuals for this purpose. Although the customer care materials partly address this issue, information, education, and communication (IEC) materials on paediatric conditions are generally lacking. Fortunately, many health facilities have audio‐visual equipment, which can be put to better use than is currently being done.
4. Recommendations
4.1 Leadership and advocacy for improvement in quality of care
The Paediatric Society must press for the improvement of services for children in line with the recommendations in this report and promote local leadership for improvement among its members.
4.2 Improving hospital layout and facilities for children
There should be separate facilities for children in health facilities. The separation must be incorporated in the design and construction of new health facilities. For older facilities with improved staffing and adequate space, hospital management should designate a separate outpatient department (OPD) for children. For existing facilities where there are no possibilities for creating a separate OPD, one or two practitioners should be assigned to attend to the children. Care needs to be taken to assign an adequate number of staff to cover the case load of children under the age of five. These practitioners should receive regular updates on current practices in child health.

Assessment of quality of care for children in selected hospitals in Ghana
Page 31
Within the records department, a separate window for serving children must be created. Hospital management should also commit resources to help ward make facilities more child‐friendly. This includes the provision of toys, children’s books, and decorating children’s wards and rooms in colours and schemes that are attractive to children. In designing new facilities, consideration should be given to providing adequate space for and situating nurses’ stations within the wards. Hostel facilities should be provided for mothers in health facilities where children are admitted.
4.3 Improving the quality of data on paediatric care
The review of the DHIMS and consequent upgrade to DHIMS2 should include all stakeholders and provide for the disaggregation of children’s statistics in order to provide more data for better planning. Facilities should be encouraged to analyse their data, provide feedback to staff and use reports to improve services.
4.4 Improving the availability of medicines and supplies
Facility management should ensure that medicines are available in emergency areas and wards, and should determine ways for health staff to document what has been given out and account for their use. Making medicines available in the emergency area will prevent delays in providing care for sick children and save lives. Procurement of paediatric equipment should be incorporated into facility and national procurement plans.
4.5 Improving case management
Case management needs to be improved through the provision of clinical care guidelines, including monitoring charts, job aids and training. The WHO Pocket Book of Hospital Care for Children needs to be adapted. Hospitals should invest in training their staff using local resources. In this regard, training and orientation in Integrated Management of Neonatal and Childhood Illness (IMNCI), Severe Acute Malnutrition (SAM), Emergency Triage, Assessment and Treatment (ETAT), Essential Newborn Care, and Hospital Care for the Newborn must be scaled up to address gaps in paediatric care at various levels. The policy on hospital feeding must be enforced and preparation of food by hospital caterers should be mindful of admitted children. Training of nurses in paediatric care should be a priority and negotiations that are currently underway should be accelerated to ensure early implementation of the programme.
Assessment of quality of care for children in selected hospitals in Ghana
Page 32
4.6 Strengthening quality assurance mechanisms within hospitals
Guidelines for clinical audits must be developed and staff trained in their use. The regular conduct of such audits must be included in hospital managers’ performance indicators. Caretakers’ concerns and views may be addressed by regular patient satisfaction surveys, and their views incorporated into health facility quality improvement initiatives. The GHS customer care training should also be scaled up with hospitals buying into the programme. Facilitative and clinical supervision must be strengthened at all levels to ensure compliance with standards. The MOH/GHS should designate best practice hospitals in paediatric care and use them for study tours and training sites, and promote regular peer reviews.
4.7 Improving human resources
The health sector is implementing strategies to improve human resource output, and mechanisms for fair distribution must be instituted, as well as adequate compensation packages. Communication between hospital management and staff can be improved by holding regular meetings/durbars and involving all categories of staff in such meetings, as well as conducting staff satisfaction surveys.
4.8 Improving access to health facilities
Health education materials for the education of caretakers should be developed in local languages and a variety of media used for their dissemination. Cost of hospital care is a significant barrier and communities must be educated regarding how to register children in the NHIS as they are in the exempt category.

Assessment of quality of care for children in selected hospitals in Ghana
Page 33
References
1. Assessment of Quality of Care for the Sick Child in Ghanaian hospitals. Accra, Ghana Health Service and World Health Organization, 2005.
2. Emergency Triage Assessment and Treatment: Manual for Participants. Geneva, World Health Organization, 2005. Available at: http://whqlibdoc.who.int/publications/2005/9241546875_eng.pdf.
3. Emergency Triage Assessment and Treatment: Facilitator Guide. Geneva, World Health Organization, 2005. Available at: http://whqlibdoc.who.int/publications/2005/9241546883_eng.pdf
4. Pocket Book of Hospital Care for Children, Guidelines for the management of common illnesses with limited resources, Geneva, World Health Organization, 2007. Available at: http://www.who.int/ child_ adolescent_health/documents/9241546700/en/index.html.
5. Better Medicines for Children. World Health Assembly Resolution 60.20. World Health Organization, 23 May 2007. Available at: http://www.who.int/childmedicines/ publications/ WHA6020.pdf.
6. Framework for Improving Hospital Care for Children in Developing Countries. Geneva, World Health Organization, 2009.
7. Assessment of the quality of care for children in hospitals: A generic assessment tool. Geneva, World Health Organization, 2008.
8. Standard Treatment Guidelines. Accra, Ministry of Health, Ghana National Drugs Programme, 2010.
9. Standards for the care of children and adolescents in health. Sydney, The Royal Australasian College of Physicians, 2008. Available at: www.wcha.asn.au/index.cfm/spid/1_7.cfm?paction=doc...id...

Assessment of quality of care for children in selected hospitals in Ghana
Page 34

Assessment of quality of care for children in selected hospitals in Ghana
Page 35
Appendix I: Assessment of the quality of care for children in hospitals
A generic assessment tool adapted for use in Ghana
June 2010
Introduction
This generic assessment tool helps to evaluate the quality of care for children in hospitals, based on standards derived from the WHO Pocket Book of Hospital Care for Children, and other relevant WHO materials. Before use in a country, the assessment tool should be reviewed by health professionals for its consistency with national standards and guidelines, such as an essential drugs list, and prevalence of diseases and adapted where necessary. This generic tool attempts to be comprehensive but not exhaustive in addressing the areas that are important to provide care for children in hospitals. The assessment tool provides some prioritization as it is recognized that some aspects of care for children are essential. It is suggested that hospitals ensure that these essential aspects are put in place first and other areas, though important, may be addressed later. Priority areas include triage, hygiene (including hand‐washing), availability of emergency and first‐line drugs, availability of updated standard treatment guidelines, emergency care and assessment and management of common conditions including cough and difficulty breathing, diarrhoea, fever, HIV/AIDS and newborn care. The assessment tool includes the following sections:
1. General hospital information
– Layout of health facility
2. Hospital support systems
– Hospital health statistics – Essential drugs, equipment and supplies – Laboratory support
3. Emergency care
– Patient flow – Staff – Layout and structure of emergency area – Drugs equipment and supplies – Case management of emergency conditions
4. Childrenʹs ward
– Staffing and layout – Standards and criteria

Assessment of quality of care for children in selected hospitals in Ghana
Page 36
5. Case management of common diseases:
– Cough or difficult breathing – Diarrhoea – Fever conditions – Malnutrition – Children with HIV/AIDS
6. Supportive care
7. Monitoring
8. Neonatal care
– Nursery staffing and layout – Routine neonatal care – Nursery facilities – Case management and sick newborn care
9. Paediatric surgery and rehabilitation
10. Other hospital wards with children
11. Hospital administration
12. Access to hospital care
The tool also includes a section that can be used to organize a Debriefing and action plan. In the annexes questionnaires for interviews with caretakers and health workers can be found. The tool is designed in sections so that during adaptation, sections may be removed if considered not to be a priority for a specific country. For example:
– A section on management of dengue fever will only be necessary in South‐East Asia or Central and South America.
– In some countries or parts of countries, the malaria component in the fever section may not be necessary.
– Paediatricians may only wish to assess medical care so the paediatric surgical section will not be required in this case.
– Hospitals may wish to assess only particular conditions or areas of care, for example, assessment of emergency care before and after implementation of a training course, such as emergency triage assessment and treatment (ETAT).
Overview of the assessment process
The hospital assessment may be embedded into a national quality improvement programme, or interested health authorities at a provincial, district, or hospital level, involving one or several hospitals, might conduct the assessment. After a period of change, the process of assessment can be repeated to document improvements.

Assessment of quality of care for children in selected hospitals in Ghana
Page 37
The core of the assessment is a hospital visit which lasts about two days. Assessors complete the assessment tool recording form. One recording form is used for each hospital. Information is collected from various sources as explained in detail below. At the end of the hospital visit, assessors and hospital administration meet for a debriefing and agree on a plan of action for immediate and later improvements.
Training of assessors
Before conducting the assessment, all the assessors need to be made thoroughly familiar with the standards, the guidelines as contained in the Pocket Book, and the assessment tool. Such a training course takes about three days, with training sessions on the Pocket Book (for which the case‐based studies in the CD accompanying the Pocket Book can be used), review of the forms, and practical sessions on hospital wards to become familiar with the forms and to agree between the assessors on scoring.
Guide to the assessment tool
To evaluate the different aspects of paediatric care in district hospitals, information is collected in various formats including:
– Brief questionnaires on hospital layout and structure with yes or no answers, and space for written information to be completed during observation when on the hospital visit or through interviews with staff;
– Checklists for equipment, drugs and supplies for completion;
– Forms documenting the management of different medical conditions based on accepted standards of care and criteria to meet these standards. The forms prompt documentation of whether practices are good or need improvement, summarize strengths and weaknesses, and require a final score of the area of observation.
Questionnaires and checklists
The first part of the assessment tool is in the form of a questionnaire with checklists that focus on information expected to be of importance for planning quality improvement interventions. Examples of information in this section include: hospital layout and structure, admission rates, case fatality rates for the most common conditions, availability of essential drugs, availability of diagnostic support and of therapeutic equipment. Information from the questionnaires/checklists will have to be reviewed together with information from on site observations of quality of care when interventions for individual hospitals are planned. Information from questionnaires or checklists should be cross‐checked during the hospital visit.
Hospital visit
The sections of the assessment tool for completion during the hospital visits include information from observations of case management and the physical environment, with information from interviews with hospital staff and caretakers of sick children. It is suggested that as much time as possible is spent on the children’s ward to gain first‐hand

Assessment of quality of care for children in selected hospitals in Ghana
Page 38
information by direct observation, especially on the management and care of children in the hospital. Try to establish by direct observation if the drugs and equipment are available in the emergency room, on the ward or in pharmacy. Also visit other wards in the hospital where children are being cared for. If possible have a look in theatre/operating room to check if paediatric‐size equipment is available. Try to verify information provided by the hospital staff or patients while observing during the visit.
Sources of information
Information for the hospital assessments may be collected from: Case observations: For clinical case management, this is the preferred source of information, and should be used wherever possible. The care for new arrivals and admitted children to the hospital should be observed without interference from the assessors. This is complemented by discussion of the case with staff, review of the case records and monitoring charts, and interviewing the mothers. Records: Assessors obtain information on the quality of care for admitted and recently discharged patients by checking records. If there are insufficient patients for direct case observations, assessors should ask staff if it is possible to review records. This source of information is particularly important for relatively rare, but severe conditions, such as meningitis, where there might be no case admitted during the time of the visit. Interviews: Assessors conduct interviews with hospital staff and caretakers to gain some idea of their perception of care for children in the hospitals. The assessment tool provides an outline for interviews with caretakers as well as health workers that can be found in Annexes 1 and 2 respectively. Also, if there are not enough cases for direct review of case management, simulated cases are presented to staff to assess clinical case management. Hospital visit: This concerns mainly items amenable to direct observation during the hospital visit and the round of the hospital, such as cleanliness and availability of items to mothers. Areas of doubt can be clarified by interviews.
Documenting and scoring the hospital assessment
Each section is scored based on standards and criteria to meet these standards. Standards are the minimum requirements for good quality of care for children. For the case management sections, the instructions in the assessment tool provide guidance to the standards, but do not cover all aspects of a given standard, and therefore reference is made to the guidelines in the sections of the WHO Pocket Book of Hospital Care for Children, indicating the relevant pages. All sections of the assessment tool leave sufficient space for comments and personal observations. Where possible additional information should be noted, especially on how the information has been obtained (chart review, staff interview, observation of care provided). Each of the different topics ends with a summary table, in which the findings can be condensed, marking strengths and weaknesses, to facilitate a quick overview of each chapter. This helps with remembering important points which should be covered during the final

Assessment of quality of care for children in selected hospitals in Ghana
Page 39
debriefing of the hospital director and staff. Finally, all topics are to be marked in a summary score in the summary evaluation sheet. This is particularly useful to monitor hospital improvement over time and to enable inter‐hospital comparison. Scoring system: For overall scoring, numbers from 5 to 1 are awarded, 5 being good practice complying with standards of care, 4 showing little need for improvement to reach standards of care, 3 meaning some need for improvement to reach standards of care, 2 indicating considerable need for improvement to reach standards of care and 1 being services not provided, totally inadequate care or potentially life‐threatening practices.
Table 1: Scoring system, summary score
Summary score essential drugs, equipment and supplies Good To be improved
(to be circled) 5 4 3 2 1
Please indicate the quality of support by marking one of the 5 numbers; 5 indicates good support, 4 to 1 indicating levels of necessary improvement (4=small need for improvement, 1=urgent need for improvement). Finally, all topics are marked in a summary score in the summary evaluation sheet. This can assist in monitoring hospital improvements over time and to make inter‐hospital comparison possible. Note that if sections of the tool are removed or edited, the total potential summary score should be revised.
Composition of the hospital assessment teams
The assessment teams should be composed of people with complementary backgrounds, to put the findings into perspective, such as a paediatrician, a general physician or clinical officer working in a hospital similar to the one which is being assessed, and a nurse with experience in caring for children. Depending on the purpose of the assessment, the teams can be composed of internal assessors only or a combination of internal and external assessors. This will have cost implications.
Conducting the hospital visit
The observation visit requires two working days, including the possibility to do observations also during the evening or night. The hospital director must have been informed in advance and have agreed to the assessment. It facilitates the work if the questionnaire/checklists (Part 1) have been forwarded to the hospital in advance or if the hospital administrator has been asked to prepare the requested information before the assessors arrive.

Assessment of quality of care for children in selected hospitals in Ghana
Page 40
Suggested timetable for the visit: Day 1: The assessors should arrive at the hospital on the day prior to the assessment or in the morning of the same day. Hospitals are usually busiest in the mornings with new admissions. Observations can be conducted irrespective of the day of the week. However, since the assessment begins and ends with hospital staff meetings the schedule should allow for these meetings during regular working hours. Introductory meeting Schedule a meeting with the hospital director and his/her staff prior to the start of the assessment. Introduce the purpose of the assessment and describe the assessment process. Emphasize that the assessment is a voluntary exercise that is part of an initiative to help hospitals improve the quality of paediatric care. The purpose of the assessment is to identify areas of care with a large potential for improvement. Explain that you will interview staff about hospital routines and practices and that you would like to observe care of as many patients as possible, those already admitted as well as new arrivals. Schedule a debriefing meeting at the end of the assessment. The debriefing can be planned in advance of the visit to ensure the participation of key staff. Hospital visit The assessment will normally start with a tour of the hospital. Ask to be shown all areas of the hospital that will be of relevance to paediatric care. In addition to the paediatric ward(s), the tour should include the following areas when they exist: the delivery ward, the neonatal nursery, intensive care unit, other wards where children might be admitted, such as surgical or infectious diseases ward, emergency area, outpatient department, pharmacy, laboratory unit, blood bank, and the radiology department. The assessors will then continue with the assessment, which does not have to be conducted in a certain order. Observation over time is important and new arrivals and new admissions to the hospital should be closely observed. It is an advantage if the assessors can sleep in the hospital and if the hospital is asked to alert them when new patients arrive. The assessors should not interrupt, interfere or guide medical work in any way. It is important that they are allowed to move around freely and are free to interview parents and staff. Day 2: Continue the assessment including interviews with staff and caretakers, case observations and going through records. Make sure that the necessary information in the protocol is obtained for all areas. This requires repeated review of the assessment tool for missing items still to be completed. The team might break up into sub‐teams to fulfil certain tasks. Findings should, however, be discussed by the whole team at certain intervals. Allow for sufficient time to prepare your findings for presentation at the debriefing. Transfer all findings onto the summary sheet of findings for discussion with hospital authorities at the debriefing.

Assessment of quality of care for children in selected hospitals in Ghana
Page 41
Debriefing visit with the hospital authorities Each hospital will receive immediate feedback at the end of the visit. The purpose of the feedback meeting is to review the assessment findings and commence planning for implementation of the improvement process. The meeting should be attended by the medical director, senior management and all staff participating in the assessment so that all those involved will continue to be involved in the planning and implementation of improvement interventions in their hospital. The hospital staff should be thanked for their cooperation and firstly the strengths should be highlighted and then the weaknesses discussed. Through discussion, three areas for improvement should be prioritized for action, based on the feasibility of improvement and their impact on mortality. It is best to select areas in which the hospital can actively engage leaving more structural problems aside for later action. It should be clear to everyone what the problems are and what can be done to improve the situation. An action plan should be constructed that will identify:
– what tasks are to be carried out;
– when each task will be carried out;
– who will carry out the task;
– how much it will cost to carry out each task, and where the budget will come from for this work.
Responsible persons should be assigned for each of the three identified areas. Any financial resources, supplies and equipment, training or supervision needs or other technical inputs should be identified and a time set when the hospital will review progress.

Assessment of quality of care for children in selected hospitals in Ghana
Page 42

Assessment of quality of care for children in selected hospitals in Ghana
Page 43
Assessment of the quality of hospital care for children Date: __/__/__/ Country: ____________________ Initials of Health Facility: __/__/ Initials of Assessor: __/__/
1. General hospital information
Source: Hospital walk‐through observation, and interviews with matron/staff. Instructions: Collect information on numbers and time. Several questions have space for you to describe your answer in more detail.
Date of assessment: __/__/__/
Name of interviewer(s): _____________________
Name of the health facility: _____________________
District: _____________________ Region: _____________________
Type of health facility:
District Hospital Regional Hospital
Ownership of facility:
Public Private
Mission (faith‐based) Quasi Hospital

Assessment of quality of care for children in selected hospitals in Ghana
Page 44
1.1 Layout of health facility
Does the health facility have a separate outpatient department? Y N
Comments:
Is the paediatric outpatient separate from the adult outpatient department? Y N
Comments:
At what time does the paediatric outpatient department open? _____________________ hrs
At what time does the paediatric outpatient department close? _____________________ hrs Does the health facility have a separate emergency department/unit? Y N
Is it open 24 hours? Y N If not, what hours is it open? _____________________ hrs
Does the health facility have a ward for admitting children? Y N
If so, how many beds? _____________________ How many cots? _____________________
Does the health facility have a separate ward or room for admitting sick newborns? Y N
If so, how many beds? _____________________ How many cots? _____________________ How many incubators? _____________________
Does the health facility have a separate room or ward for admitting paediatric infectious cases (isolation ward)? Y N
If so, how many beds? _____________________
If so, is this separate from the adult infectious cases? Y N
Describe:
Where are children with surgical conditions admitted?
Describe:

Assessment of quality of care for children in selected hospitals in Ghana
Page 45
Where are children with severe conditions requiring special or intensive care admitted?
Describe:
Are the most seriously ill children cared for in a section where they receive closest attention? (near the nursing station)
Describe:
Is a qualified nurse (State Registered Nurse or Enrolled Nurse) available 24 hrs per day on the childrenʹs ward? (check duty roster)
Describe:
What is the estimated HIV prevalence in your region?

Assessment of quality of care for children in selected hospitals in Ghana
Page 46
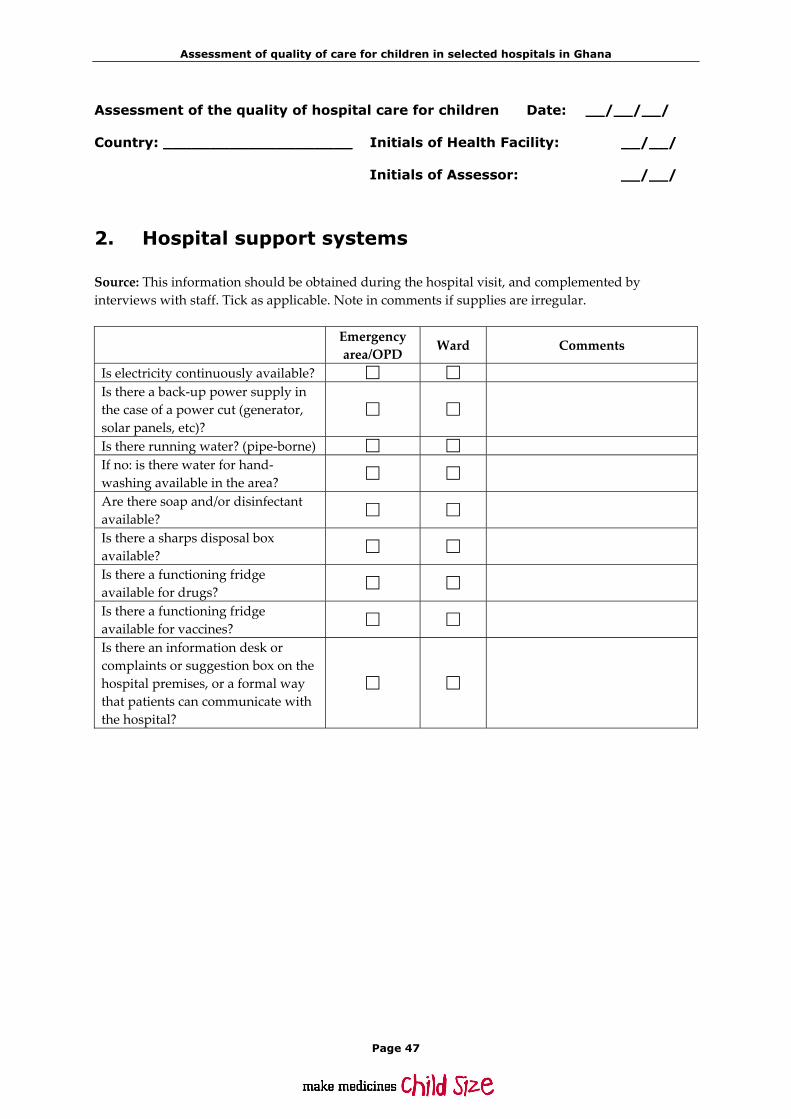
Assessment of quality of care for children in selected hospitals in Ghana
Page 47
Assessment of the quality of hospital care for children Date: __/__/__/ Country: ____________________ Initials of Health Facility: __/__/ Initials of Assessor: __/__/
2. Hospital support systems
Source: This information should be obtained during the hospital visit, and complemented by interviews with staff. Tick as applicable. Note in comments if supplies are irregular.
Emergency area/OPD
Ward Comments
Is electricity continuously available? Is there a back‐up power supply in the case of a power cut (generator, solar panels, etc)?
Is there running water? (pipe‐borne) If no: is there water for hand‐washing available in the area?
Are there soap and/or disinfectant available?
Is there a sharps disposal box available?
Is there a functioning fridge available for drugs?
Is there a functioning fridge available for vaccines?
Is there an information desk or complaints or suggestion box on the hospital premises, or a formal way that patients can communicate with the hospital?

Assessment of quality of care for children in selected hospitals in Ghana
Page 48
2.1 Hospital health statistics
Source: Routine statistics. Collect the information from the hospital administration early in the visit. Make use of routine statistics; adjust the categories accordingly (e.g. age groups) where necessary.
2.1.1 Patient load
Indicate the total number of paediatric medical outpatient visits, emergency visits and admissions per year by age groups and as a total. Include all medical diagnosis but exclude children dead on arrival. Note: If data are not disaggregated according to the suggested age‐groups, compile the data available indicating the age‐groups compiled. Year: 2009
Outpatient visits
Emergency visits
Admissions Deaths
Age‐specific fatality rate
0 – 28 days _________ _________ _________ _________ ________
1 up to 12 months _________ _________ _________ _________ ________
1 up to 5 years _________ _________ _________ _________ ________
>5 years _________ _________ _________ _________ ________
Total (all age groups) _________ _________ _________ _________ ________
2.1.2 Admission details
List the five most frequent medical reasons (diagnoses) for outpatient visits, emergency visits and hospital admissions in children under five Outpatient
visits Emergency visits
Hospital admissions
Deaths *Diagnosis‐specific case fatality rate
1.
2.
3.
4.
5.
* This refers to any data available on malaria, diarrhoea and other conditions.

Assessment of quality of care for children in selected hospitals in Ghana
Page 49
2.1.3 Paediatric surgery details
Source: Routine statistics. Collect the information from the hospital administration early in the visit. Make use of routine statistics.
Most common paediatric surgical procedures performed in 2009
Procedure Annual number of procedures
Performed by – health worker category
1.
2.
3.
4.
5.
How often are the following paediatric surgical procedures performed?
Regularly Infrequently Never
Performed by – health worker category
Referred to another facility
Circumcision
Hernia repair
Fractures
Skin grafting
Laparotomy including appendectomy
Incision and drainage for abscesses/ pyomyositis
2.2 Essential drugs, equipment and supplies
Source: Collect the information from the emergency area, the ward and the pharmacist early in the visit, and adjust drugs according to local alternatives.
2.2.1 Drugs
Availability of drugs varies considerably in different regions. Please indicate the drugs available. For those drugs marked with an asterisk (*), local adaptations of use might be necessary. If drugs are only available for sale and not freely available for children, make a note. Check for the presence of drugs and enquire with staff whether drugs are regularly available. Check expiry dates. Note whether drugs with the earliest expiry date are for first use (in the front‐row). Comment on how readily available drugs are for the non‐insured, insured and the poor.
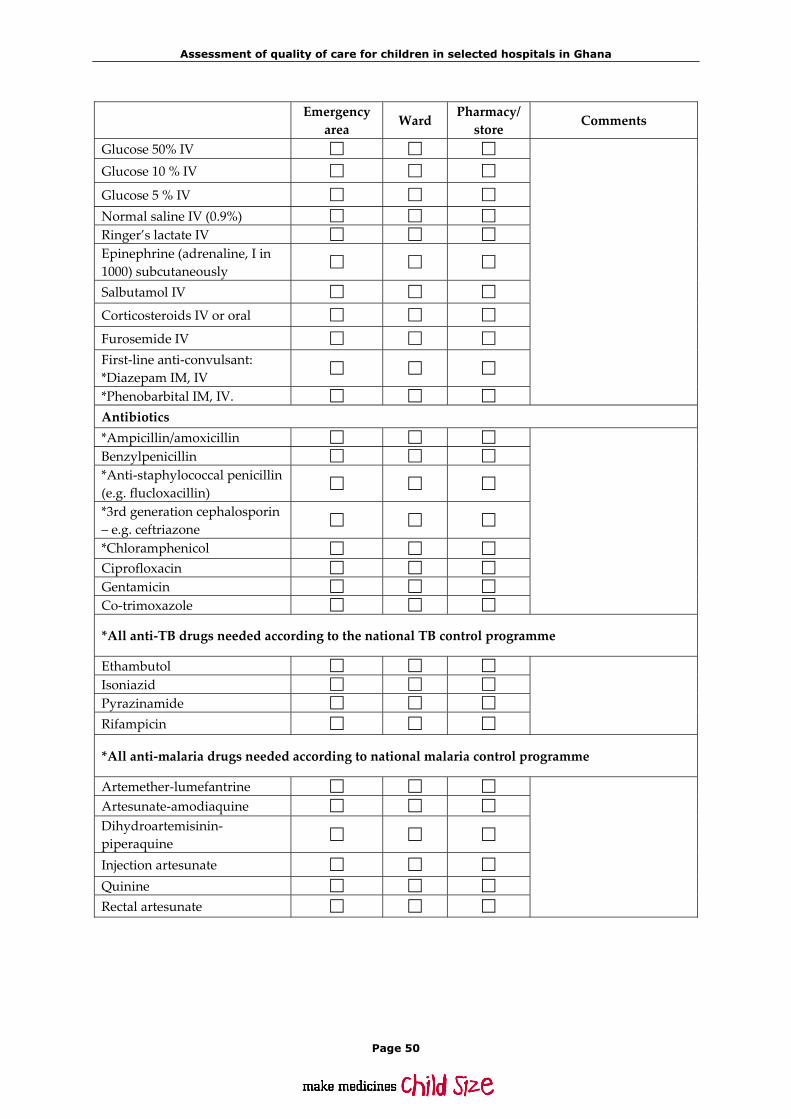
Assessment of quality of care for children in selected hospitals in Ghana
Page 50
Emergency area
Ward Pharmacy/store
Comments
Glucose 50% IV
Glucose 10 % IV
Glucose 5 % IV Normal saline IV (0.9%) Ringer’s lactate IV Epinephrine (adrenaline, I in 1000) subcutaneously
Salbutamol IV
Corticosteroids IV or oral
Furosemide IV First‐line anti‐convulsant: *Diazepam IM, IV
*Phenobarbital IM, IV. Antibiotics *Ampicillin/amoxicillin Benzylpenicillin *Anti‐staphylococcal penicillin (e.g. flucloxacillin)
*3rd generation cephalosporin – e.g. ceftriazone
*Chloramphenicol Ciprofloxacin Gentamicin Co‐trimoxazole
*All anti‐TB drugs needed according to the national TB control programme
Ethambutol Isoniazid Pyrazinamide Rifampicin
*All anti‐malaria drugs needed according to national malaria control programme
Artemether‐lumefantrine Artesunate‐amodiaquine Dihydroartemisinin‐piperaquine
Injection artesunate Quinine Rectal artesunate
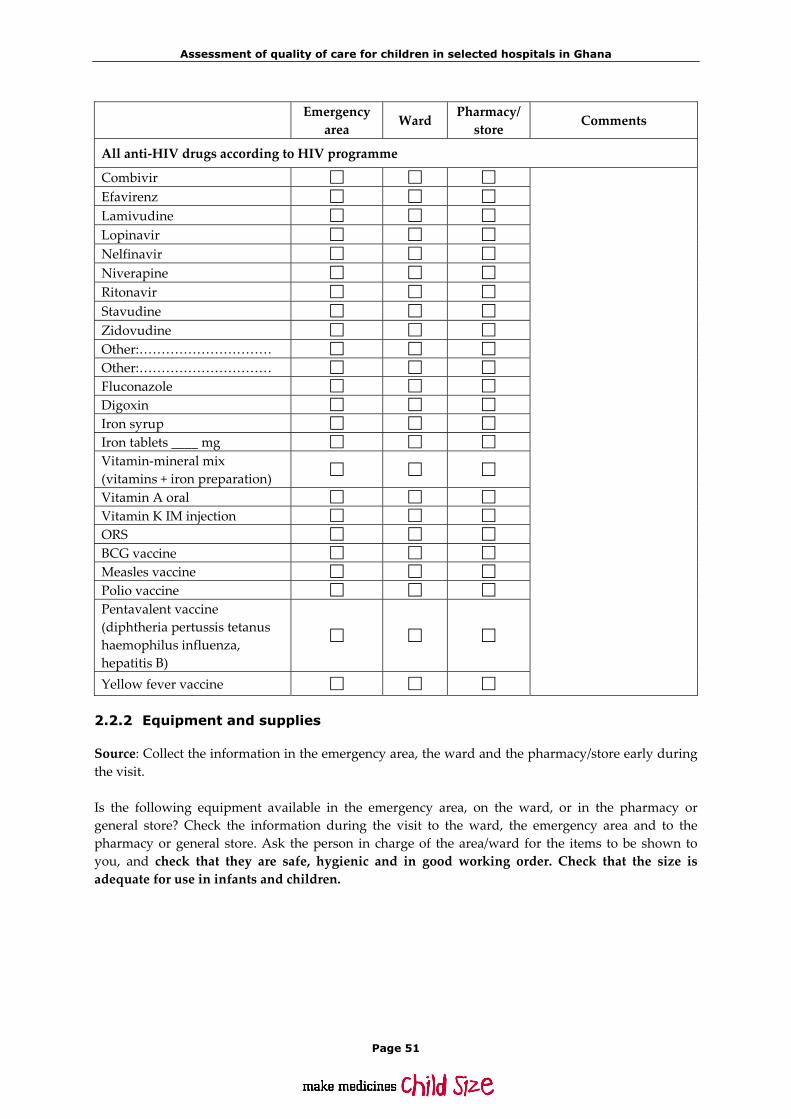
Assessment of quality of care for children in selected hospitals in Ghana
Page 51
Emergency area
Ward Pharmacy/store
Comments
All anti‐HIV drugs according to HIV programme
Combivir Efavirenz Lamivudine Lopinavir Nelfinavir Niverapine Ritonavir Stavudine Zidovudine Other:………………………… Other:………………………… Fluconazole Digoxin Iron syrup Iron tablets ____ mg Vitamin‐mineral mix (vitamins + iron preparation)
Vitamin A oral Vitamin K IM injection ORS BCG vaccine Measles vaccine Polio vaccine Pentavalent vaccine (diphtheria pertussis tetanus haemophilus influenza, hepatitis B)
Yellow fever vaccine
2.2.2 Equipment and supplies
Source: Collect the information in the emergency area, the ward and the pharmacy/store early during the visit. Is the following equipment available in the emergency area, on the ward, or in the pharmacy or general store? Check the information during the visit to the ward, the emergency area and to the pharmacy or general store. Ask the person in charge of the area/ward for the items to be shown to you, and check that they are safe, hygienic and in good working order. Check that the size is adequate for use in infants and children.
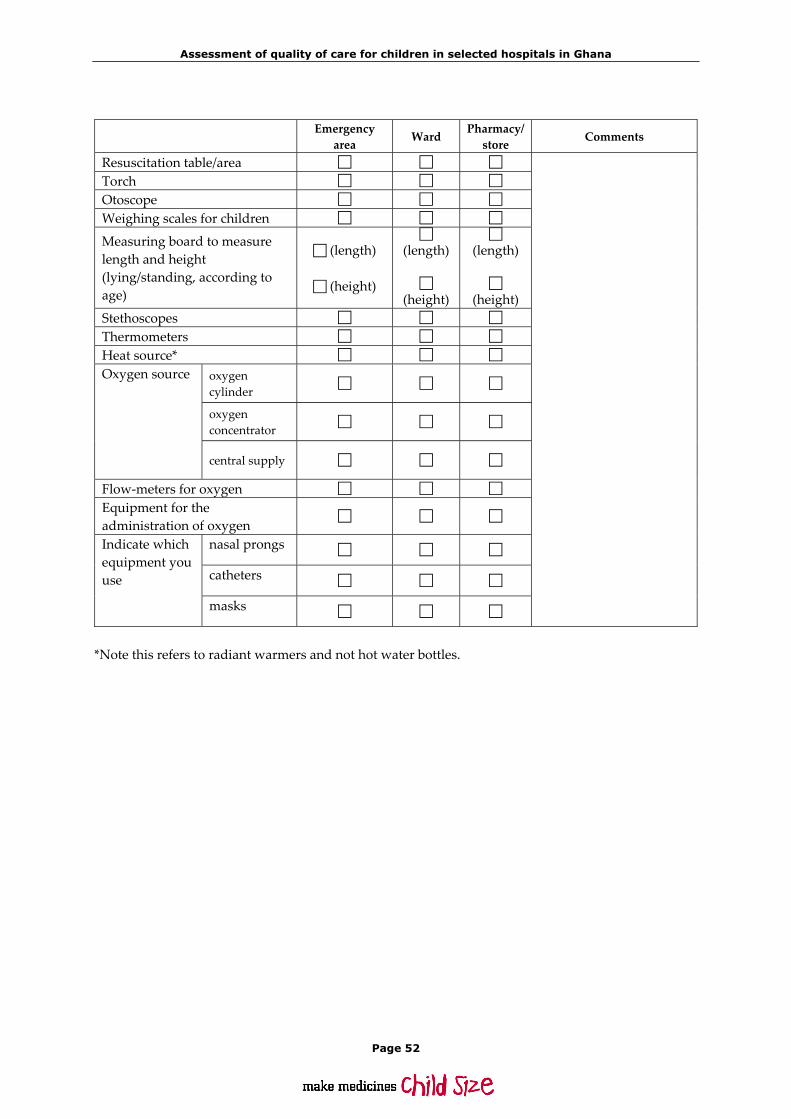
Assessment of quality of care for children in selected hospitals in Ghana
Page 52
Emergency
area Ward Pharmacy/store Comments
Resuscitation table/area Torch Otoscope Weighing scales for children
Measuring board to measure length and height (lying/standing, according to age)
(length)
(height)
(length)
(height)
(length)
(height) Stethoscopes Thermometers Heat source*
oxygen cylinder
oxygen concentrator
Oxygen source
central supply
Flow‐meters for oxygen Equipment for the administration of oxygen
nasal prongs
catheters
Indicate which equipment you use
masks *Note this refers to radiant warmers and not hot water bottles.

Assessment of quality of care for children in selected hospitals in Ghana
Page 53
Emergency
area Ward Pharmacy/ store Comments
Self‐inflating bags for resuscitation
Infant size
Child size
Masks
Adult size IV‐transfusion (giving) sets with chambers for paediatric use
Butterflies and/or cannulae in paediatric sizes (21‐25)
NG‐tubes, paediatric size (No 5, 8, 12)
Equipment for intra‐osseous fluid administration (wide bore needle)
Suction equipment Chest tubes Nebulizers for the administration of salbutamol
Electricity driven
Oxygen driven
Indicate type of nebulizer:
Foot pump driven
Spacers with masks for the administration of metered doses (spray) of salbutamol

Assessment of quality of care for children in selected hospitals in Ghana
Page 54
2.2.3 Standards for drugs, equipment and supplies
An adequate essential drugs list exists for the hospital with all drugs being available. Essential equipment is ready to use and in good working order. Paediatric size anaesthesia equipment is available and in good working order. See p 44.
Please note: Refer to the completed tables above to mark this section.
Standards and criteria
Good To be improved
Comments
Availability of essential drugs
An essential drugs list exists in the hospital (or a National Health Insurance Medicine List) and is available to prescribers. Drugs on the list are adequate for the management of most common conditions. Essential drugs are available on the ward and in the emergency area and immediately accessible. Drugs are not expired. Oldest drugs are used first.
Availability of supplies and equipment
Essential equipment is immediately available for use. Essential equipment is safe and in working order.Essential supplies are available immediately, and are adequate for use in children.
Summary table essential drugs, equipment and supplies
Good To be improved
Comments
Essential drugs are available, not expired and old drugs are used first.
Paediatric‐size anaesthesia equipment is available and in good working condition (child‐sized mask, ventilation bag and mask).
Adequate equipment is available in the emergency area and on the ward.
There is an adequate range of IV fluids.
Summary score essential drugs, equipment and supplies Good To be improved
(to be circled) 5 4 3 2 1
Please indicate the quality of support by marking one of the 5 numbers; 5 indicates good support, 4 to 1 indicating levels of necessary improvement (4=small need for improvement, 1=urgent need for improvement).

Assessment of quality of care for children in selected hospitals in Ghana
Page 55
2.3 Laboratory support
Source: Collect the information from the laboratory and chief laboratory technician early in the visit . Try to see as many essential laboratory investigations being carried out as possible. Are the following laboratory investigations and their results available reasonably quickly at this hospital? (E.g. blood glucose, Hb, PCV within 30 minutes, other investigations 1‐2 hours). If available, indicate the time normally taken to obtain the results. Not
available Available Time to get results Comments
Blood glucose
Haemoglobin
Haematocrit (PCV)
Microscopy for malaria parasites
Rapid diagnostic test (RDT) for malaria
CSF microscopy
Urine microscopy
Urine dip‐stick (albumin, glucose, nitrite, leukocytes; please indicate)
HIV‐serology
Blood grouping and cross‐matching
Bilirubin
CD4 counts according to national guidelines
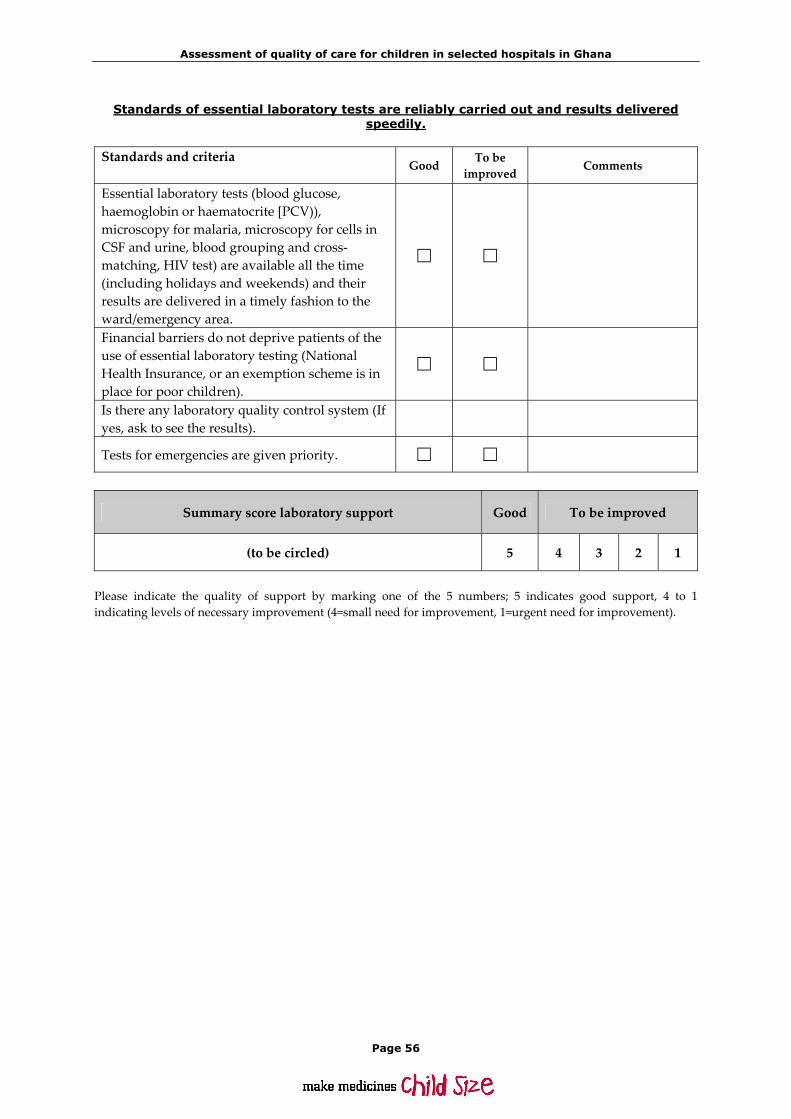
Assessment of quality of care for children in selected hospitals in Ghana
Page 56
Standards of essential laboratory tests are reliably carried out and results delivered speedily.
Standards and criteria Good
To be improved Comments
Essential laboratory tests (blood glucose, haemoglobin or haematocrite [PCV)), microscopy for malaria, microscopy for cells in CSF and urine, blood grouping and cross‐matching, HIV test) are available all the time (including holidays and weekends) and their results are delivered in a timely fashion to the ward/emergency area.
Financial barriers do not deprive patients of the use of essential laboratory testing (National Health Insurance, or an exemption scheme is in place for poor children).
Is there any laboratory quality control system (If yes, ask to see the results).
Tests for emergencies are given priority.
Summary score laboratory support Good To be improved
(to be circled) 5 4 3 2 1
Please indicate the quality of support by marking one of the 5 numbers; 5 indicates good support, 4 to 1 indicating levels of necessary improvement (4=small need for improvement, 1=urgent need for improvement).
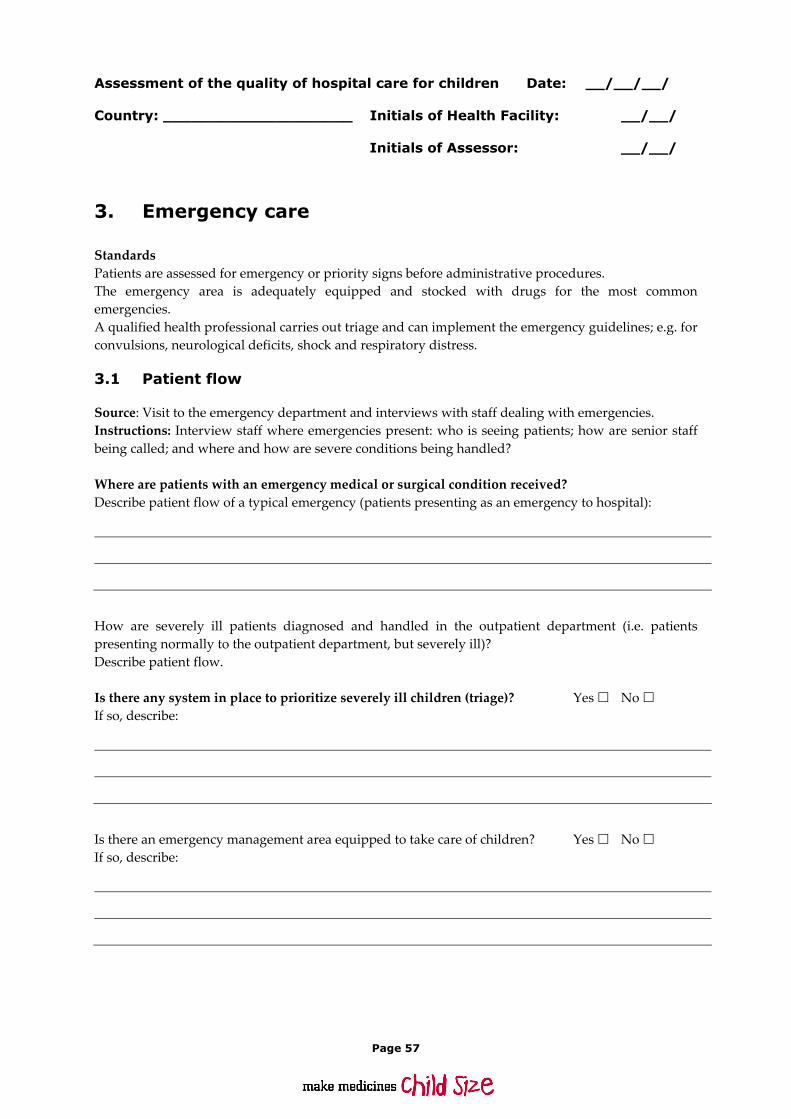
Page 57
Assessment of the quality of hospital care for children Date: __/__/__/ Country: ____________________ Initials of Health Facility: __/__/ Initials of Assessor: __/__/
3. Emergency care
Standards Patients are assessed for emergency or priority signs before administrative procedures. The emergency area is adequately equipped and stocked with drugs for the most common emergencies. A qualified health professional carries out triage and can implement the emergency guidelines; e.g. for convulsions, neurological deficits, shock and respiratory distress.
3.1 Patient flow
Source: Visit to the emergency department and interviews with staff dealing with emergencies. Instructions: Interview staff where emergencies present: who is seeing patients; how are senior staff being called; and where and how are severe conditions being handled? Where are patients with an emergency medical or surgical condition received? Describe patient flow of a typical emergency (patients presenting as an emergency to hospital):
How are severely ill patients diagnosed and handled in the outpatient department (i.e. patients presenting normally to the outpatient department, but severely ill)? Describe patient flow. Is there any system in place to prioritize severely ill children (triage)? Yes No If so, describe:
Is there an emergency management area equipped to take care of children? Yes No If so, describe:

Assessment of quality of care for children in selected hospitals in Ghana
Page 58
Is this separate from the normal outpatient facility dealing with non‐referred children? Yes No If so, describe:
Do patients come with referral notes when they have been referred from first level units? Never Sometimes Always Comments:
Are there any job aids/guidelines/protocols (wall charts, chart booklets) displayed for the management of paediatric emergencies? Yes No If so, describe what aids/guidelines/protocols are provided, and comment on their adequacy:
Distance from the reception area to the emergency management area:
In the same building, distance (meters/walking time):
In another building, distance (meters/walking time):
Distance from consultation area to emergency management area:
In the same building, distance (meters/walking time):
In another building, distance(meters/walking time):

Assessment of quality of care for children in selected hospitals in Ghana
Page 59
3.2 Staff dealing with emergencies
This concerns staff who are immediately available to deal with emergencies and their level of training
Cadre of staff
During working hours
Present/not present
If present, number
After working hours
Present/not present
If present, number
Trained in assessment
of emergency conditions Yes/No
Trained in management/ aspects of emergency conditions Yes/No
Comments
Gateman
Records clerk
Triage nurse
Nurse
Auxiliary
Medical assistant
Medical officer
Paediatric specialist
3.3 Layout and structure of emergency area
Standards Patients are assessed for emergency or priority signs before administrative procedures. The emergency area is adequately equipped and stocked with drugs for the most common emergencies. A qualified health professional carries out triage and can implement the emergency guidelines; e.g. for convulsions, neurological deficits, shock and respiratory distress.
Standards and criteria Good To be improved
Comments
Children are assessed for severity/priority signs (triaged) immediately upon arrival. Patients do not have to wait for their turn, registration, payment etc. before a first assessment is done and action taken. A wall chart or job aid for identifying children by severity of condition is located in the emergency admissions area.

Assessment of quality of care for children in selected hospitals in Ghana
Page 60
Standards and criteria Good To be improved
Comments
Drugs, equipment and supplies* (see below)
Essential drugs for emergency conditions (anticonvulsants, glucose, IV fluids) are always available without prior demand for payment.
Essential laboratory tests (glucose, Hb or PCV) are available and results are obtained in a timely manner. Essential equipment (needles and syringes, nasogastric tubes, oxygen equipment, self‐inflating resuscitation bags with masks of different sizes, nebulizers or spacers) is available.
Staffing
A qualified staff member is designated to carry out triage. A health professional is available without delay to manage children determined to have an emergency condition.
Case management** (see below) Staff doing triage are trained in the ETAT guidelines and can implement them appropriately, particularly when the emergency room gets busy during peak hours.
Staff are skilled in the management of common emergency conditions and start treatment without delay: management of severe respiratory distress, shock, convulsions, lethargy and severe dehydration.
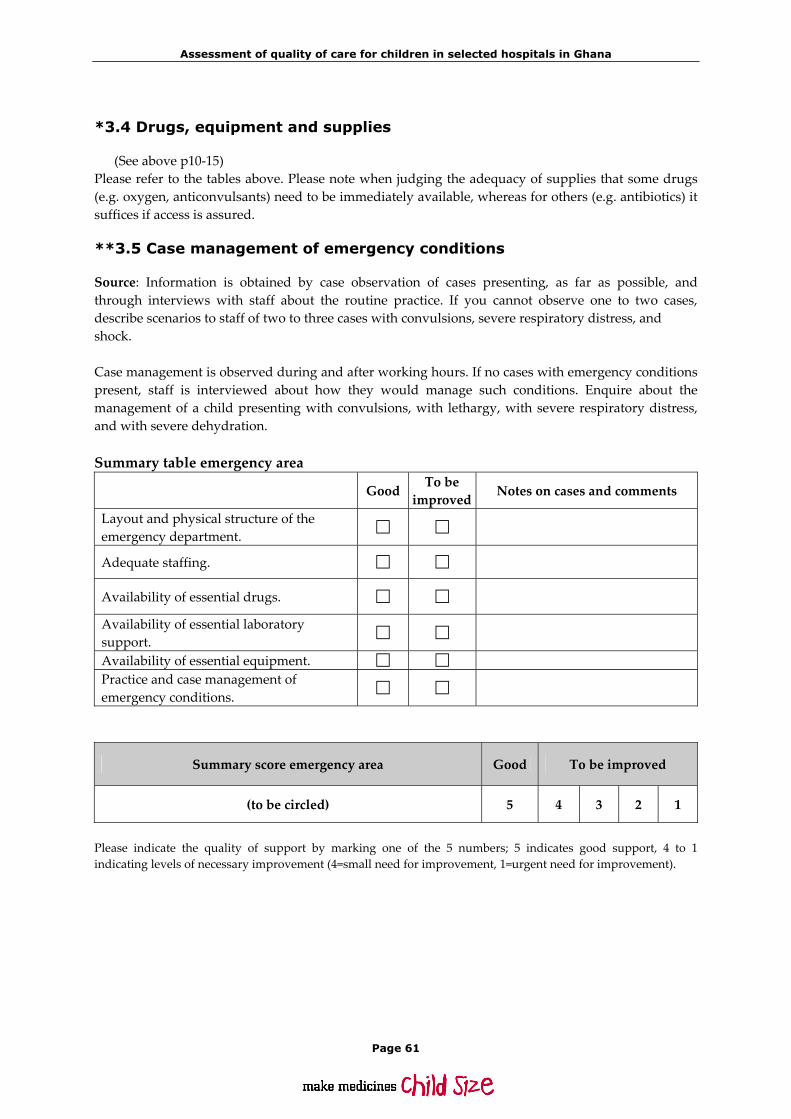
Assessment of quality of care for children in selected hospitals in Ghana
Page 61
*3.4 Drugs, equipment and supplies
(See above p10‐15) Please refer to the tables above. Please note when judging the adequacy of supplies that some drugs (e.g. oxygen, anticonvulsants) need to be immediately available, whereas for others (e.g. antibiotics) it suffices if access is assured.
**3.5 Case management of emergency conditions
Source: Information is obtained by case observation of cases presenting, as far as possible, and through interviews with staff about the routine practice. If you cannot observe one to two cases, describe scenarios to staff of two to three cases with convulsions, severe respiratory distress, and shock. Case management is observed during and after working hours. If no cases with emergency conditions present, staff is interviewed about how they would manage such conditions. Enquire about the management of a child presenting with convulsions, with lethargy, with severe respiratory distress, and with severe dehydration. Summary table emergency area
Good To be improved Notes on cases and comments
Layout and physical structure of the emergency department.
Adequate staffing.
Availability of essential drugs.
Availability of essential laboratory support.
Availability of essential equipment. Practice and case management of emergency conditions.
Summary score emergency area Good To be improved
(to be circled) 5 4 3 2 1
Please indicate the quality of support by marking one of the 5 numbers; 5 indicates good support, 4 to 1 indicating levels of necessary improvement (4=small need for improvement, 1=urgent need for improvement).

Assessment of quality of care for children in selected hospitals in Ghana
Page 62

Assessment of quality of care for children in selected hospitals in Ghana
Page 63
Assessment of the quality of hospital care for children Date: __/__/__/ Country: ____________________ Initials of Health Facility: __/__/ Initials of Assessor: __/__/
4. Children’s ward
4.1 Staffing and layout
Source: Observation during the visit to the ward, and interviews with staff and guardians of patients. How many beds does the ward have? How many patients are currently admitted? Is this high‐season for paediatric admissions or off‐season? Has the number of paediatric patients increased over the last three years? Please comment:
Which age groups are admitted to the paediatric ward? ____ to ____ years Paediatric ward staffing During week days Staff category at
post No. during morning shift
No. during afternoon shift
No. during night shift
Comments
Doctors Nurses Others (please specify)
During weekends/holidays Staff category at
post No. during morning shift
No. during afternoon shift
No. during night shift
Comments
Doctors Nurses Others (please specify)

Assessment of quality of care for children in selected hospitals in Ghana
Page 64
Layout Check the following Is there a toilet in the ward? For patients? Yes No
For staff? Yes No
Is the toilet clean? Yes No
Are the beds safe (bedside railing) and well maintained? Yes No
Are the beds well spaced (one meter apart) Yes No
Are there mattresses? Yes No
Do patients receive bed‐sheets? Yes No
Are the beds clean? Yes No
Is there an emergency management area in or near to the ward? Yes No
Is there a heat source on the ward? Yes No
Are Insecticide treated bed nets available for patients’ use? Yes No
Comments and observations:
4.2 Standards and criteria in the children's ward
Standards Children are seen in OPD by a designated health professional only. Closest attention for the most seriously ill children is ensured. There is a separate childrenʹs ward or room for children. There is a separate room for sick neonates with their mothers. Hygienic and sufficient services facilitate the stay of mother and child. Staff can wash their hands on the ward and there are sharps disposals available.

Assessment of quality of care for children in selected hospitals in Ghana
Page 65
Standards and criteria Good To be improved Comments
Children are only seen in OPD by the designated health professional in the designated room/area.
Closest attention for the most seriously ill children
The most seriously ill children are cared for in a section where they receive closest attention.
This section is close to the nursing station so that children can be directly observed most of the time.
Separate ward for children. Children are kept in a separate ward or separate area of a ward.
Severely ill children are kept apart from adults in wards such as those for infectious diseases or intensive care.
Children with surgical conditions are at least kept in a separate room, with staff aware of the special needs for children, such as feeding and warmth.
Arrangements are made to meet these needs.
In cold weather children are kept warm (blankets etc...).
Separate room for sick neonates with their mothers Sick newborns are kept separate from healthy babies.
Mothers of sick newborns are rooming in with their babies, and have adequate facilities.
Hygiene and accident prevention
Staff have access to hand washing facilities (tap/veronica bucket, soap and single use towels. The ward is kept clean and dangerous items are inaccessible for children.
Sharps are disposed of in a special container, preventing accidents.

Assessment of quality of care for children in selected hospitals in Ghana
Page 66
Standards and criteria Good To be
improved Comments
Hygienic and sufficient services facilitate the stay of mother and child
There are sufficient and adequate toilets which are easily accessible.
Mothers have access to running water and to an appropriate space, near the ward, to wash themselves and their child.
Mothers have access to a washing facility, in order to wash themselves and their child’s clothes.
Patients are kept in a bed/cot with a clean mattress.
Patients receive bed sheets.
Beds are equipped with insecticide‐treated bed nets.
Summary table paediatrics ward
Good To be improved
Notes on cases and comments
There is a separate ward for children.
There is a separate room for sick newborn babies with their mothers.
The hygiene of services for children and their mothers is adequate.
Closest attention is provided for the most seriously ill children.
Hygiene and accident prevention is in place.
Summary score childrenʹs ward and facilities Good To be improved
(to be circled) 5 4 3 2 1
Please indicate the quality of support by marking one of the 5 numbers; 5 indicates good support, 4 to 1 indicating levels of necessary improvement (4=small need for improvement, 1=urgent need for improvement).

Assessment of quality of care for children in selected hospitals in Ghana
Page 67
Assessment of the quality of hospital care for children Date: __/__/__/ Country: ____________________ Initials of Health Facility: __/__/ Initials of Assessor: __/__/
5. Case management of common diseases:
5.1 Cough/difficult breathing (p 69‐107*) 5.2 Diarrhoea (p109‐130) 5.3 Fever conditions (p133‐171) 5.4 Malnutrition (p173‐196) 5.5 HIV/AIDS (p199‐224) Source: This information should be collected by observing the treatment and care of children with the relevant condition and interviewing staff and carers, and reviewing patient’ records (5‐10 records) * Please note: the page‐references refer to the English version of the WHO Pocket Bock of Hospital Care for Children.
5.1 Cough or difficult breathing
Standards Pneumonia is diagnosed and classified based on diagnostic signs. Appropriate antibiotics are administered to children who need them. Oxygen therapy is administered to all children who need it. Correct indications for chest X‐ray are applied. Children with wheezing receive correctly administered inhaled bronchodilators. TB treatment is given according to national guidelines. Adequate monitoring and supportive care is ensured.
Standards and criteria Good To be improved
Comments
Assessment of pneumonia
Health workers correctly diagnose pneumonia and classify/recognize severity pp 69‐74,78. Signs such as chest‐indrawing, respiratory rate, presence of cyanosis and general condition are used pp 70‐73.
Administration of appropriate antibiotics
Antibiotics are given only to children with cough and difficult breathing who need them (pneumonia, severe pneumonia, very severe pneumonia or very severe disease).pp 74,75, 79,80 Not to children without signs of pneumonia or unless there is another reason for

Assessment of quality of care for children in selected hospitals in Ghana
Page 68
Standards and criteria Good To be improved
Comments
antibiotics p 82. Appropriate antibiotics at correct doses and duration are administered for pneumonia according to severity and weight pp 74,75,79,80.
If child has not improved after two days or condition worsens, a health professional looks for complications or considers other diagnoses pp 76, 79.
Oxygen therapy
Oxygen is administered to all children who need it. pp 75,79,281‐284. Oxygen is not given if there is no clinical indication for oxygen therapy (sign of hypoxaemia) p 75.
Oxygen is administered correctly (prongs or catheter, correct flow, no interruptions) and monitored. Oxygen mask and headbox are avoided due to waste of oxygen and risks pp 281‐284.
Use of chest X‐ray Chest x‐rays are performed when signs of pneumonia are present in: Young infants Cases with very severe pneumonia Cases with suspected complications (e.g. empyema, pneumothorax, abscess) Patients not responding to appropriate antibiotic treatment for > 48 hours Chest x‐ray is not performed in patients with uncomplicated pneumonia or cough and cold unless there is a clear indication pp 76‐77.
Wheezing Children in need of bronchodilators are correctly identified/diagnosed pp 87,88.
Inhaled bronchodilators are correctly administered (way, dose and frequency) by spacer or nebulizer pp 88‐89. Inhaled bronchodilators are affordable (without prior demand for payment).
Children with asthma who are discharged have follow‐up treatment prescribed and explained to parents p 91.

Assessment of quality of care for children in selected hospitals in Ghana
Page 69
Standards and criteria Good To be improved
Comments
TB treatment
Correct anti‐tuberculous treatment is given to children with suspected TB according to national guidelines pp 101‐104.
TB is considered as differential diagnosis of un‐resolving pneumonia and malnutrition p 76. Not every child with malnutrition receives anti‐TB treatment (balance of the likelihood of having TB) p 192.
Monitoring and supportive care
See monitoring and supportive care, sections 10 and 11 pp 261ff and 289ff.
Summary table cough/difficult breathing
Good To be improved
Notes on cases and comments
Severity of pneumonia is correctly assessed and diagnosed.
Appropriate antibiotics are administered for pneumonia and other respiratory diagnoses.
Oxygen is correctly administered when necessary.
Correct use of chest X‐ray.
Appropriate diagnosis and management of TB.
Inhaled bronchodilators are given appropriately when indicated.
Patient monitoring appropriately performed and charted (see section 11).
Supportive care provided appropriate for condition (see section 10).

Assessment of quality of care for children in selected hospitals in Ghana
Page 70
Main strengths:
Main weaknesses:
Summary score cough and difficult breathing Good To be improved
(to be circled) 5 4 3 2 1
Please indicate the quality of support by marking one of the 5 numbers; 5 indicates good support, 4 to 1 indicating levels of necessary improvement (4=small need for improvement, 1=urgent need for improvement).
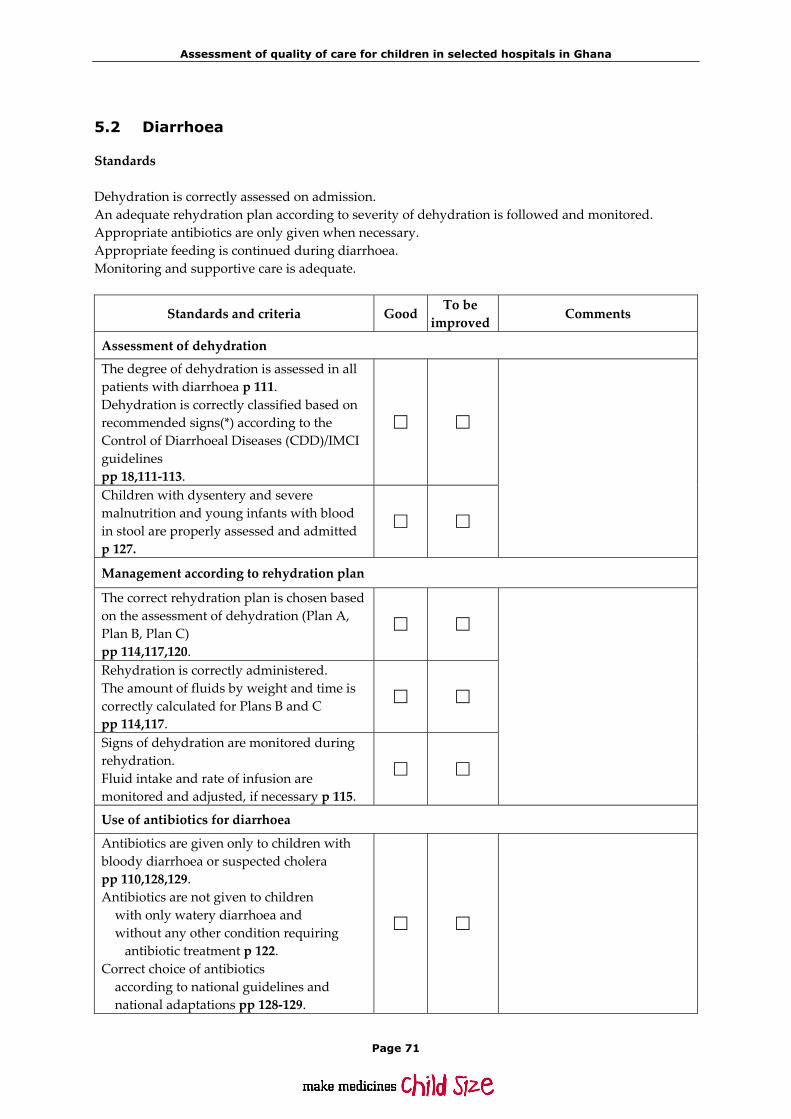
Assessment of quality of care for children in selected hospitals in Ghana
Page 71
5.2 Diarrhoea
Standards Dehydration is correctly assessed on admission. An adequate rehydration plan according to severity of dehydration is followed and monitored. Appropriate antibiotics are only given when necessary. Appropriate feeding is continued during diarrhoea. Monitoring and supportive care is adequate.
Standards and criteria Good To be improved
Comments
Assessment of dehydration
The degree of dehydration is assessed in all patients with diarrhoea p 111. Dehydration is correctly classified based on recommended signs(*) according to the Control of Diarrhoeal Diseases (CDD)/IMCI guidelines pp 18,111‐113.
Children with dysentery and severe malnutrition and young infants with blood in stool are properly assessed and admitted p 127.
Management according to rehydration plan
The correct rehydration plan is chosen based on the assessment of dehydration (Plan A, Plan B, Plan C) pp 114,117,120.
Rehydration is correctly administered. The amount of fluids by weight and time is correctly calculated for Plans B and C pp 114,117.
Signs of dehydration are monitored during rehydration. Fluid intake and rate of infusion are monitored and adjusted, if necessary p 115.
Use of antibiotics for diarrhoea
Antibiotics are given only to children with bloody diarrhoea or suspected cholera pp 110,128,129. Antibiotics are not given to children with only watery diarrhoea and without any other condition requiring antibiotic treatment p 122. Correct choice of antibiotics according to national guidelines and national adaptations pp 128‐129.
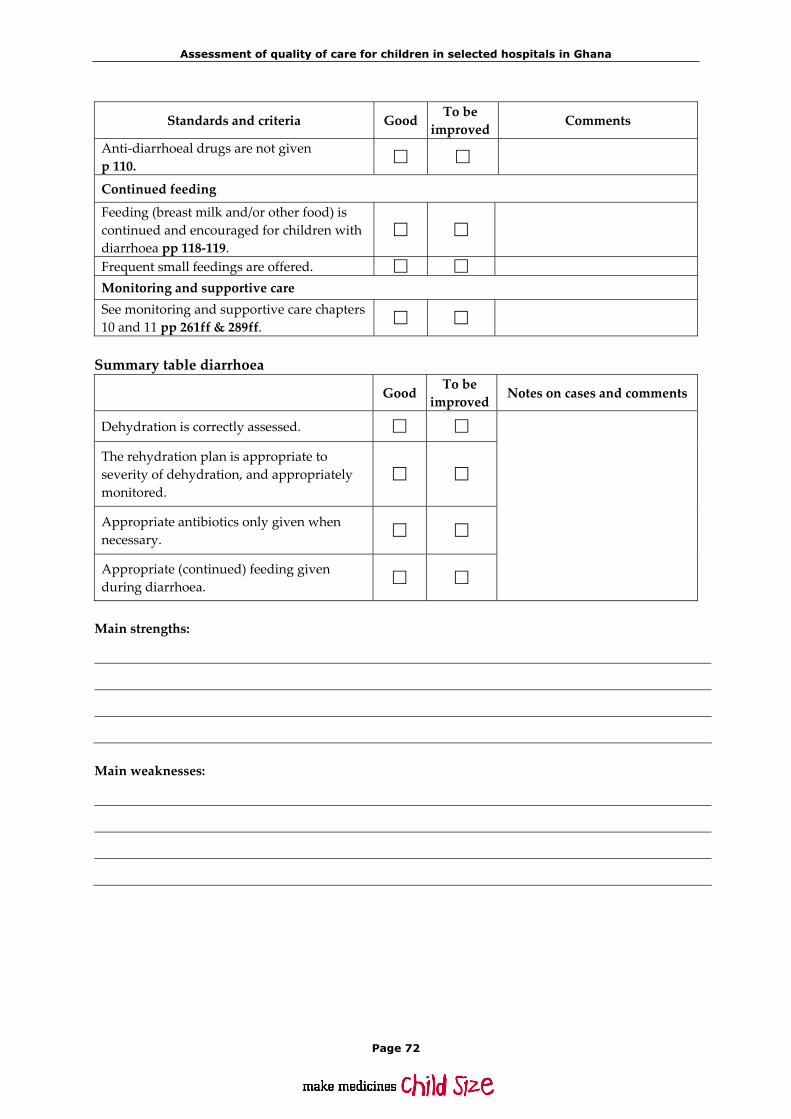
Assessment of quality of care for children in selected hospitals in Ghana
Page 72
Standards and criteria Good To be improved
Comments
Anti‐diarrhoeal drugs are not given p 110.
Continued feeding
Feeding (breast milk and/or other food) is continued and encouraged for children with diarrhoea pp 118‐119.
Frequent small feedings are offered. Monitoring and supportive care See monitoring and supportive care chapters 10 and 11 pp 261ff & 289ff.
Summary table diarrhoea
Good To be improved Notes on cases and comments
Dehydration is correctly assessed.
The rehydration plan is appropriate to severity of dehydration, and appropriately monitored.
Appropriate antibiotics only given when necessary.
Appropriate (continued) feeding given during diarrhoea.
Main strengths:
Main weaknesses:

Assessment of quality of care for children in selected hospitals in Ghana
Page 73
Summary score management of diarrhoea Good To be improved
(to be circled) 5 4 3 2 1
Please indicate the quality of support by marking one of the 5 numbers; 5 indicates good support, 4 to 1 indicating levels of necessary improvement (4=small need for improvement, 1=urgent need for improvement).
5.3 Fever conditions
Standards A differential diagnosis of fever is considered and appropriate investigations are undertaken. Meningitis is correctly diagnosed and managed. Severe complicated malaria is correctly diagnosed and managed. Measles is correctly diagnosed and managed. Other febrile conditions are correctly diagnosed and managed. Adequate monitoring and supportive care is ensured.
Standards and criteria Good To be improved
Comments
Differential diagnosis and investigations
Appropriate assessment is undertaken for all children with febrile conditions pp 133‐134 ‐history ‐examination ‐laboratory.
Children admitted with fever have a differential diagnosis for possible and likely conditions considered p 135.
Appropriate examinations/investigations are undertaken to establish a diagnosis (lumbar puncture, blood film for malaria, urine examination, chest x‐ray) p 137.
Diagnosis and management of meningitis Lumbar puncture is performed without delay when meningitis is suspected p 149
Adequate antibiotic treatment is started without delay when bacterial meningitis is suspected p 150.
Complications of meningitis are diagnosed and treated appropriately: ‐convulsions ‐hypoglycaemia etc. p 153.
Appropriate patient monitoring is performed and charted p 153 ‐state of consciousness ‐respiratory rate ‐pupil size.

Assessment of quality of care for children in selected hospitals in Ghana
Page 74
Standards and criteria Good To be improved
Comments
Diagnosis and management of severe or complicated malaria
Malaria diagnosis is confirmed by microscopy or a rapid diagnostic test p 137.
For possible cerebral malaria and malaria associated respiratory distress, alternative diagnoses are ruled out (lumbar puncture for meningitis, x‐ray for e.g. pneumonia) pp 139‐140.
Correct anti‐malarial treatment is given pp 140‐141.
Patients are monitored adequately, and complications such as hypo‐glycaemia are prevented pp 143‐144.
Complications are correctly diagnosed and treated pp 142‐144 ‐coma ‐severe anemia ‐hypoglycemia ‐acidosis ‐aspiration pneumonia etc.
Diagnosis and management of measles Measles cases are assessed for complications and treated appropriately p 154.
Vitamin A is given to all patients with measles p 155.
Appropriate nutritional support is given p 155 Public health measures are taken when a child is admitted with measles p 157 Notify Public Health/Disease Control Unit ‐isolation ‐patients are checked for immunization status, and ‐immunized if necessary
Other severe febrile conditions are assessed and managed correctly (typhoid, mastoiditis, UTI, septic arthritis and osteomyelitis) Appropriate assessment and differential diagnosis performed pp 133‐138.
Correct treatment given. Monitoring and supportive care (see chapters 10 and 11) pp 261ff & 289ff.

Assessment of quality of care for children in selected hospitals in Ghana
Page 75
Summary table fever
Good To be improved
Notes on cases and comments
Differential diagnosis of fever considered and appropriate investigations undertaken.
Correct diagnosis and management of meningitis.
Severe complicated malaria correctly managed.
Measles correctly managed
Other febrile conditions correctly managed.
Main strengths:
Main weaknesses:
Summary score management of fever conditions Good To be improved
(to be circled) 5 4 3 2 1
Please indicate the quality of support by marking one of the 5 numbers; 5 indicates good support, 4 to 1 indicating levels of necessary improvement (4=small need for improvement, 1=urgent need for improvement).

Assessment of quality of care for children in selected hospitals in Ghana
Page 76
5.4 Severe malnutrition
Standards Nutritional status is assessed by weight for age/MUAC and differential diagnoses for severe malnutrition are considered. Infections are appropriately managed by giving empiric treatment. Micronutrients are appropriately supplemented. Dehydration and electrolyte imbalance are appropriately assessed, treated and monitored. Hypoglycaemia and hypothermia are prevented, checked and managed. Feeding with correct type, frequency and amount of food in severely malnourished children is ensured. Associated conditions of severe malnutrition are appropriately managed. Monitoring and supportive care is adequate.
Standards and criteria Good To be improved Comments
Assessment of nutritional status, including differential diagnoses for severe malnutrition
Scale available, weight for age correctly calculated p 174.
An appropriate history is taken and laboratory examinations done pp 174‐175.
Clinical examination for: wasting, oedema, skin changes, signs of dehydration, eye signs of Vitamin A deficiency, severe palmar pallor, localizing signs of infection, mouth ulcers, fever/hypothermia etc. pp 174‐175.
Differential diagnosis considered for severe malnutrition, if doubt about protein‐energy malnutrition as likely cause (rule out TB, HIV/AIDS infection, malabsorption, etc.) pp 174‐175.
Management of infection and micronutrients
Broad spectrum antibiotics are administered to all severely malnourished patients pp 182‐183.
Measles vaccination if needed pp 182.
Treatment of worms with mebendazole/albendazole p 183.
Vitamin A given orally p 184.
Vitamin/mineral supplementation given pp 183,184.
Iron only given in the recovery phase p 183
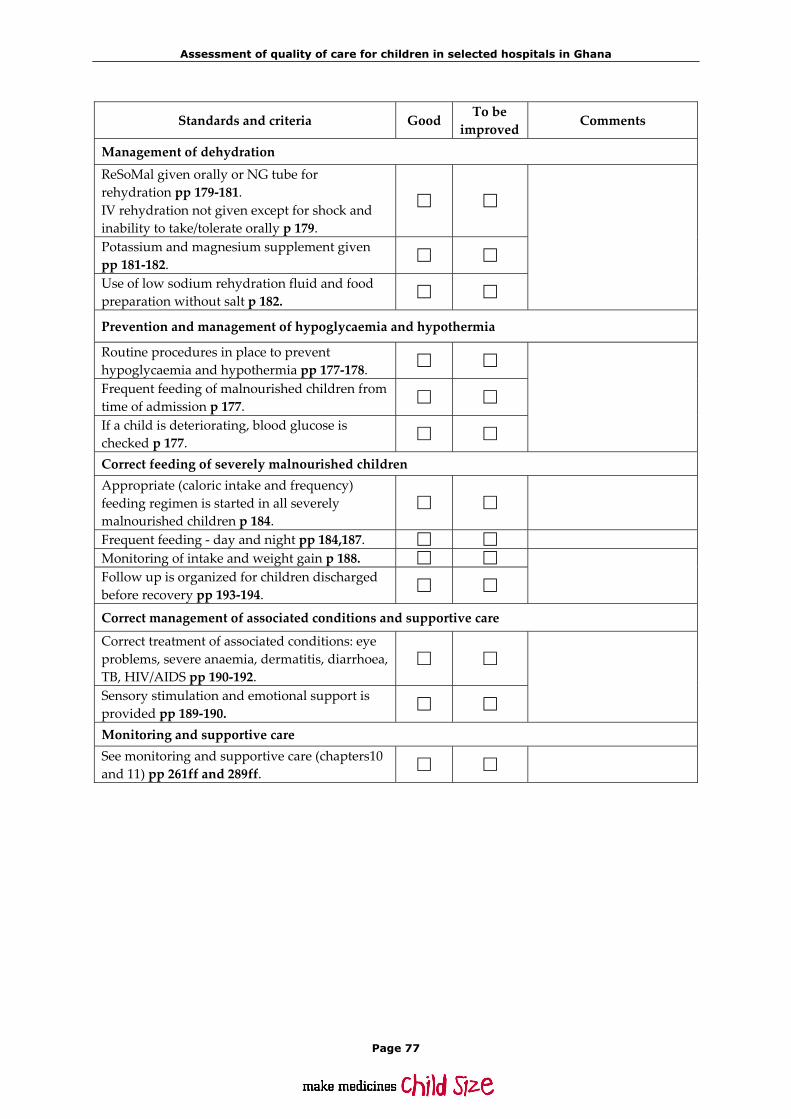
Assessment of quality of care for children in selected hospitals in Ghana
Page 77
Standards and criteria Good To be improved
Comments
Management of dehydration ReSoMal given orally or NG tube for rehydration pp 179‐181. IV rehydration not given except for shock and inability to take/tolerate orally p 179.
Potassium and magnesium supplement given pp 181‐182.
Use of low sodium rehydration fluid and food preparation without salt p 182.
Prevention and management of hypoglycaemia and hypothermia
Routine procedures in place to prevent hypoglycaemia and hypothermia pp 177‐178.
Frequent feeding of malnourished children from time of admission p 177.
If a child is deteriorating, blood glucose is checked p 177.
Correct feeding of severely malnourished children Appropriate (caloric intake and frequency) feeding regimen is started in all severely malnourished children p 184.
Frequent feeding ‐ day and night pp 184,187. Monitoring of intake and weight gain p 188. Follow up is organized for children discharged before recovery pp 193‐194.
Correct management of associated conditions and supportive care
Correct treatment of associated conditions: eye problems, severe anaemia, dermatitis, diarrhoea, TB, HIV/AIDS pp 190‐192.
Sensory stimulation and emotional support is provided pp 189‐190.
Monitoring and supportive care See monitoring and supportive care (chapters10 and 11) pp 261ff and 289ff.
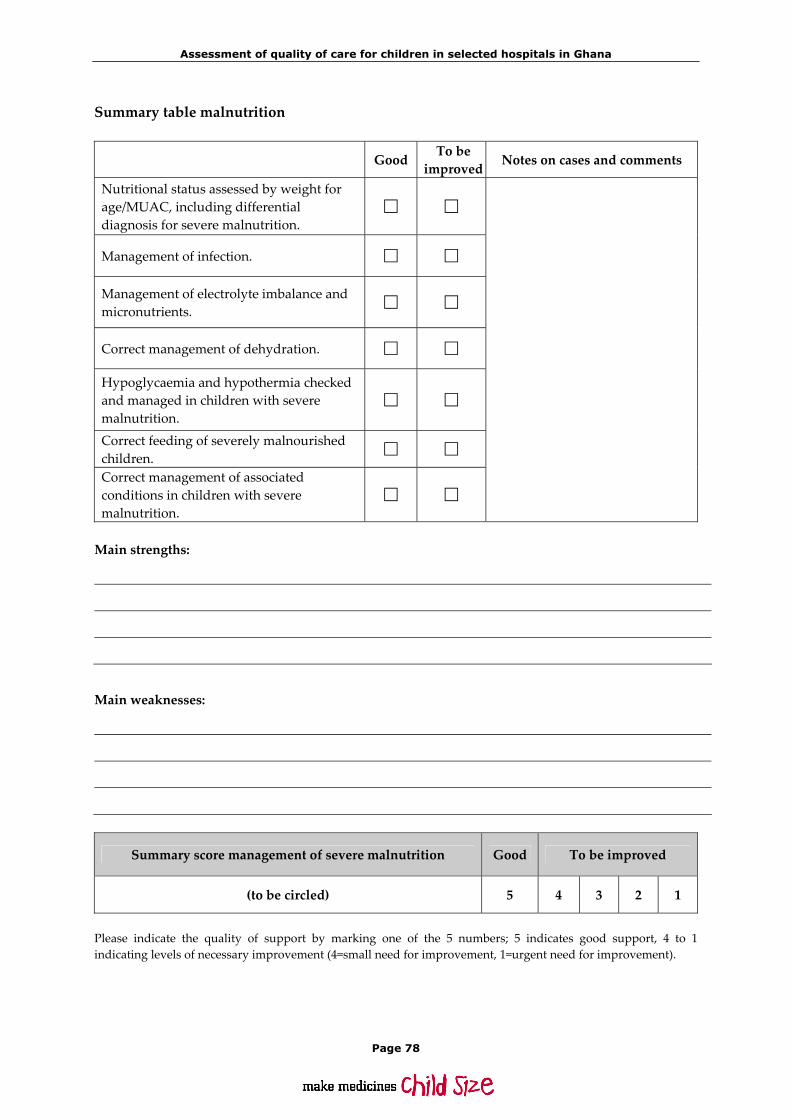
Assessment of quality of care for children in selected hospitals in Ghana
Page 78
Summary table malnutrition
Good To be improved
Notes on cases and comments
Nutritional status assessed by weight for age/MUAC, including differential diagnosis for severe malnutrition.
Management of infection.
Management of electrolyte imbalance and micronutrients.
Correct management of dehydration.
Hypoglycaemia and hypothermia checked and managed in children with severe malnutrition.
Correct feeding of severely malnourished children.
Correct management of associated conditions in children with severe malnutrition.
Main strengths:
Main weaknesses:
Summary score management of severe malnutrition Good To be improved
(to be circled) 5 4 3 2 1
Please indicate the quality of support by marking one of the 5 numbers; 5 indicates good support, 4 to 1 indicating levels of necessary improvement (4=small need for improvement, 1=urgent need for improvement).

Assessment of quality of care for children in selected hospitals in Ghana
Page 79
5.5 Children with HIV/AIDS
Standards Guidelines are in place for counselling, diagnosing and staging of paediatric HIV. Guidelines are in place for the ART and treatment of opportunistic infections and monitoring of antiretroviral therapy. All HIV infected children receive standard immunizations, prophylaxis/treatment of opportunistic infections and supportive care. Monitoring and supportive care is adequate.
Standards and criteria Good To be
improved Comments
Counselling and diagnosis of paediatric HIV
Counselling is done in a separate room and confidentiality is ensured pp 201‐203.
During breastfeeding counselling, the importance of exclusive breastfeeding for 6 months is stressed. If breast milk substitute feeding is considered, the financial and hygienic requirements are explained pp 219,220.
Counsellors receive formal training in HIV counselling, are regularly updated and do receive adequate supervision and support p 202.
Detailed counselling‐documentation is done Women attending ANC and delivering in the hospital have been offered an HIV test. Those found to be positive receive breast‐feeding counselling and learn about symptoms of paediatric HIV. A follow‐up appointment is given.
Clinical signs of paediatric HIV infection are recognized and an HIV test is offered routinely for a child with clinical signs of possible HIV infection pp 200,201.
HIV testing against the will or without the knowledge of the family is prohibited.
All family members of children with a positive HIV test are offered HIV testing and counselling p 201.
A high proportion of current inpatients with severe malnutrition or TB show a documented offer of HIV screening.
DNA/RNA tests are used for children <18 months and HIV antibody tests for those >18months pp 203,204.
The staging is done according to the WHO paediatric clinical staging system pp 204‐206.
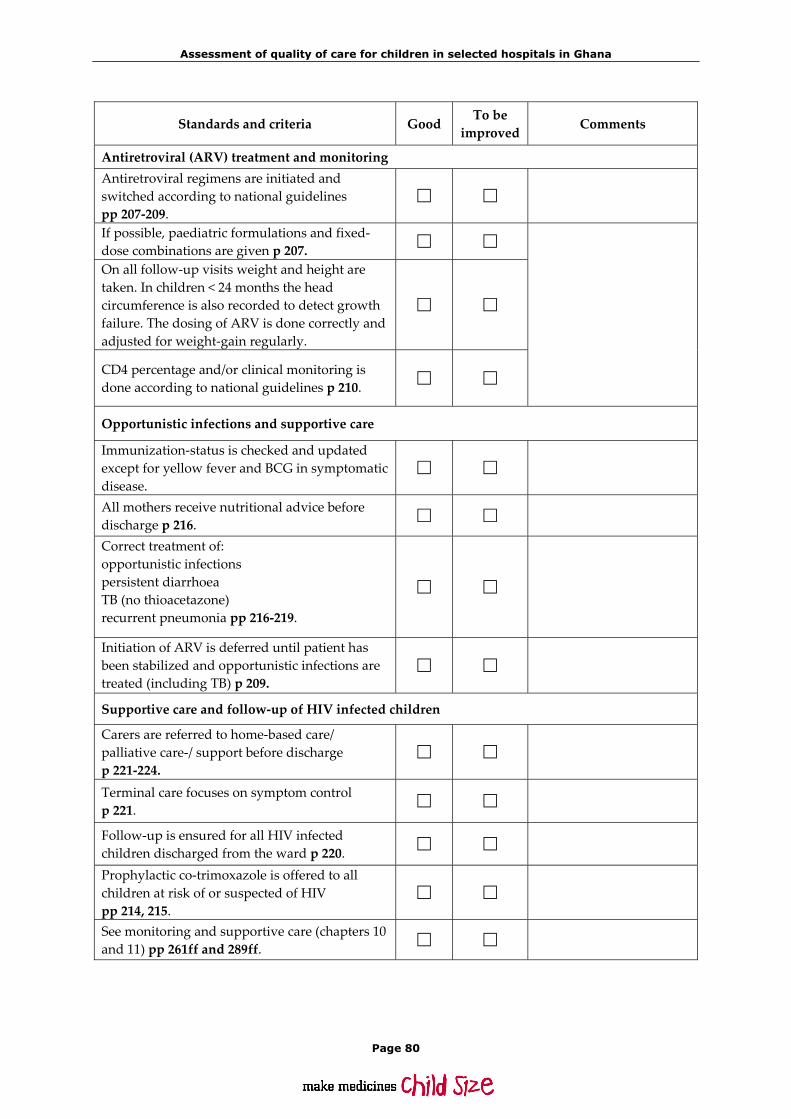
Assessment of quality of care for children in selected hospitals in Ghana
Page 80
Standards and criteria Good To be
improved Comments
Antiretroviral (ARV) treatment and monitoring Antiretroviral regimens are initiated and switched according to national guidelines pp 207‐209.
If possible, paediatric formulations and fixed‐dose combinations are given p 207.
On all follow‐up visits weight and height are taken. In children < 24 months the head circumference is also recorded to detect growth failure. The dosing of ARV is done correctly and adjusted for weight‐gain regularly.
CD4 percentage and/or clinical monitoring is done according to national guidelines p 210.
Opportunistic infections and supportive care
Immunization‐status is checked and updated except for yellow fever and BCG in symptomatic disease.
All mothers receive nutritional advice before discharge p 216.
Correct treatment of: opportunistic infections persistent diarrhoea TB (no thioacetazone) recurrent pneumonia pp 216‐219.
Initiation of ARV is deferred until patient has been stabilized and opportunistic infections are treated (including TB) p 209.
Supportive care and follow‐up of HIV infected children
Carers are referred to home‐based care/ palliative care‐/ support before discharge p 221‐224.
Terminal care focuses on symptom control p 221.
Follow‐up is ensured for all HIV infected children discharged from the ward p 220.
Prophylactic co‐trimoxazole is offered to all children at risk of or suspected of HIV pp 214, 215.
See monitoring and supportive care (chapters 10 and 11) pp 261ff and 289ff.

Assessment of quality of care for children in selected hospitals in Ghana
Page 81
Summary table HIV/AIDS
Good To be improved
Notes on cases and comments
HIV tests used correctly and when indicated.
Professional counselling services are in place with confidentiality ensured.
ARV treatment follows national guidelines.
Nutritional advice provided, (on exclusive breastfeeding for 6 months/breast milk substitute).
Immunizations and co‐trimoxazole‐prophylaxis given correctly.
Opportunistic infections correctly diagnosed/treated.
Patients are referred for home‐based care and palliative care focuses on symptom control.
Main strengths:
Main weaknesses:
Summary score management of HIV/AIDS Good To be improved
(to be circled) 5 4 3 2 1
Please indicate the quality of support by marking one of the 5 numbers; 5 indicates good support, 4 to 1 indicating levels of necessary improvement (4=small need for improvement, 1=urgent need for improvement).

Assessment of quality of care for children in selected hospitals in Ghana
Page 82
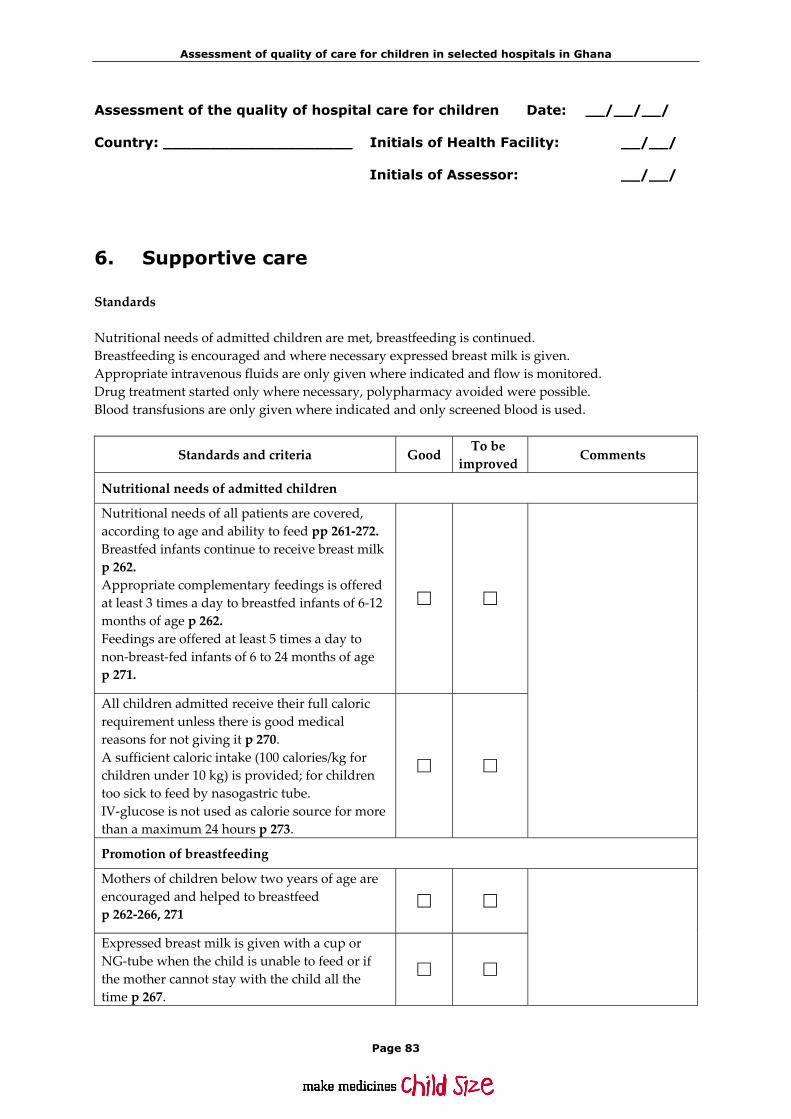
Assessment of quality of care for children in selected hospitals in Ghana
Page 83
Assessment of the quality of hospital care for children Date: __/__/__/ Country: ____________________ Initials of Health Facility: __/__/ Initials of Assessor: __/__/
6. Supportive care
Standards Nutritional needs of admitted children are met, breastfeeding is continued. Breastfeeding is encouraged and where necessary expressed breast milk is given. Appropriate intravenous fluids are only given where indicated and flow is monitored. Drug treatment started only where necessary, polypharmacy avoided were possible. Blood transfusions are only given where indicated and only screened blood is used.
Standards and criteria Good To be improved Comments
Nutritional needs of admitted children
Nutritional needs of all patients are covered, according to age and ability to feed pp 261‐272. Breastfed infants continue to receive breast milk p 262. Appropriate complementary feedings is offered at least 3 times a day to breastfed infants of 6‐12 months of age p 262. Feedings are offered at least 5 times a day to non‐breast‐fed infants of 6 to 24 months of age p 271.
All children admitted receive their full caloric requirement unless there is good medical reasons for not giving it p 270. A sufficient caloric intake (100 calories/kg for children under 10 kg) is provided; for children too sick to feed by nasogastric tube. IV‐glucose is not used as calorie source for more than a maximum 24 hours p 273.
Promotion of breastfeeding
Mothers of children below two years of age are encouraged and helped to breastfeed p 262‐266, 271
Expressed breast milk is given with a cup or NG‐tube when the child is unable to feed or if the mother cannot stay with the child all the time p 267.

Assessment of quality of care for children in selected hospitals in Ghana
Page 84
Standards and criteria Good To be improved
Comments
Use of intravenous fluids
Intravenous fluids are given only when indicated p 273.
Appropriate fluids are chosen p 273. The flow rate is monitored closely p 273.
Drug treatment and avoidance of polypharmacy
Drugs are only given for an established or highly suspected diagnosis. No drugs are given without a good reason. No routine use of sedative drugs or anti‐histamines. Corticosteroids are only given for a clear indication for which steroids are useful p 151.
Blood transfusion
Blood is only given when indicated p 277. Only screened blood is used p 277. The flow rate is monitored p 279.
Summary table supportive care
Good To be improved
Notes on cases and comments
Nutritional needs are met, according to age and ability to feed.
Breastfeeding is promoted.
Intravenous fluids given only when indicated, appropriate choice of fluids, and monitoring of rate.
Drug treatment according to diagnosis, polypharmacy is avoided.
Blood transfusion only when indicated, blood is screened, rate monitored.
Main strengths:

Assessment of quality of care for children in selected hospitals in Ghana
Page 85
Main weaknesses:
Summary score supportive care Good To be improved
(to be circled) 5 4 3 2 1
Please indicate the quality of support by marking one of the 5 numbers; 5 indicates good support, 4 to 1 indicating levels of necessary improvement (4=small need for improvement, 1=urgent need for improvement).

Assessment of quality of care for children in selected hospitals in Ghana
Page 86

Assessment of quality of care for children in selected hospitals in Ghana
Page 87
Assessment of the quality of hospital care for children Date: __/__/__/ Country: ____________________ Initials of Health Facility: __/__/ Initials of Assessor: __/__/
7. Monitoring
This section covers topics which are applicable for sick children with different diagnoses. Information should be predominantly by care observation and review of the charts of currently admitted children. Between 3 and 5 observations should be made in this category. Standards All children are assessed for their nutritional status on admission. Every child has a monitoring chart according to severity of condition where individual progress is monitored. Reassessment and monitoring is adequately done and correctly recorded by the nurses and a senior health professional is called when needed. Admitted children are reassessed by a doctor regularly according to severity of illness. Follow up is arranged prior to discharge with a discharge note explaining the condition and further treatment needed.
Standards and criteria Good To be improved
Comments
Nutritional status is assessed in all admitted children
Monitoring of individual progress
At the time of admission, a monitoring plan is prescribed according to the severity of the patientʹs condition pp 289,290.
A standard monitoring chart is used with the following information: patient details; vital signs; clinical signs depending on condition; treatments given, feeding and outcome pp 290,369.
Reassessment and monitoring by nurses
Key risk signs are monitored and recorded by a nurse twice a day and at least four times a day for critically ill patients p 289,290.
Doses and time are recorded for medications and IV‐fluids given by the nurse for every patient receiving medication or IV‐fluids p 289,290.

Assessment of quality of care for children in selected hospitals in Ghana
Page 88
Standards and criteria Good To be improved
Comments
Additional special monitoring is performed and recorded appropriately when needed to follow the progress of particular conditions: e.g. in malnourished children, fluid balance (input – output) in severe dehydration, oxygen, coma scale for unconscious children p 289.
Nurses use the results of patient monitoring to alert the physicians of problems or changing patient status warranting their attention.
Reassessment of admitted children by a doctor
Seriously ill patients are reassessed by a doctor upon admission and reviewed at least twice daily until improved p 289.
All patients are reassessed daily during working days by a doctor. Sick patients or new admissions are also reviewed by a physician at weekends and during holidays p 289.
Follow up
Before discharge follow up is arranged in the health facility closest to the patientʹs home that provides the necessary follow‐up treatment.
All children receive a discharge note explaining their condition and providing information for the staff at the follow‐up facility
Summary table monitoring
Good To be improved
Notes on cases and comments
Nutritional status is assessed in all admitted children.
Each child’s progress is individually monitored, and charts are used.
The most ill children receive closest attention.
All admitted children are appropriately reassessed by a nurse.
All admitted children are appropriately reassessed by a doctor.

Assessment of quality of care for children in selected hospitals in Ghana
Page 89
Main strengths:
Main weaknesses:
Summary score monitoring Good To be improved
(to be circled) 5 4 3 2 1
Please indicate the quality of support by marking one of the 5 numbers; 5 indicates good support, 4 to 1 indicating levels of necessary improvement (4=small need for improvement, 1=urgent need for improvement).

Assessment of quality of care for children in selected hospitals in Ghana
Page 90

Assessment of quality of care for children in selected hospitals in Ghana
Page 91
Assessment of the quality of hospital care for children Date: __/__/__/ Country: ____________________ Initials of Health Facility: __/__/ Initials of Assessor: __/__/
8. Neonatal care
8.1 Nursery staffing and layout 8.2 Routine neonatal care, (pp 42‐47) 8.3 Nursery facilities 8.4 Case management and sick newborn care, (pp 47‐61)
8.1 Nursery staffing and layout
Source: This information should ideally be collected partly before the visit (see Annex 3: postal questionnaire), and be available for reference during the visit. If it has not been collected before, collect the information early during the visit from the doctor/nurse in charge. Staffing of delivery room and newborn nursery
Newborn nursery Delivery room Indicate the staff available for the Day Night Day Night Doctor Medical assistant Midwives Auxiliary staff Who is available during the weekend?
If senior staff members are not available all the time, how are they called?
Layout How many cots/beds does the nursery have? Number of cots/beds:?
Up to what age are newborns admitted to the nursery? Age in days/weeks: _______ days/weeks
Are out‐born infants admitted in the nursery? Yes No
If so, are they admitted in a separate room? Yes No

Assessment of quality of care for children in selected hospitals in Ghana
Page 92
Check the following: Where is the toilet?
Is the toilet clean? Yes No
Are the beds safe and well maintained? Yes No
Are there mattresses? Yes No
Do patients receive bed sheets? Yes No
Are the beds clean? Yes No
Is there an emergency management area in or near to the ward? Yes No
Is there a heat source on the ward? Yes No
Are insecticide treated bed nets available for patient use? Yes No
Are the mattresses with covered with mackintosh? Yes No
8.2 Routine neonatal care
Source: Please collect the information by observing the treatment and care of children with the relevant condition and interviewing staff and carers and reviewing patients record(s) (5‐10). Standards Neonatal resuscitation guidelines are available and staff is trained in their use. Early and exclusive breastfeeding and skin contact are ensured. Clean delivery with clean instruments and hands is practiced. Neonates are kept warm. Eye prophylaxis, Vitamin K and immunizations are given.
Standards and criteria Good To be improved
Comments
Neonatal resuscitation guidelines are available and staff are trained in their use Written guidelines for resuscitation and care of the newborn are available, followed, practiced and documented pp 42‐46.
There is a resuscitation place with heating and equipment ready to use.
A functioning self‐inflating bag with newborn‐ + premature size masks is available p 45.
If a neonate is not breathing, ventilation by self‐inflating bag is initiated according to WHO guidelines p 44.
There is a plan to call a senior health professional for resuscitation, if required p 43.
Early and exclusive breastfeeding and skin contact are ensured Within the first ½ hour, a newborn has prolonged skin contact with the mother p 42.

Assessment of quality of care for children in selected hospitals in Ghana
Page 93
Standards and criteria Good To be improved
Comments
Mothers are assisted with the first breastfeeding: correct attachment and positioning is demonstrated p 42.
There is no promotion of infant formula on the ward or distributed to mothers/staff
There are no restrictions on the frequency or length of breastfeeds
Mothers stay with their infants in the same room day and night
Clean delivery with clean instruments and hands
The birth attendants hands are clean during delivery p 46.
Clean (sterile) instruments are used p 46,47. Nothing is applied to the cord p 46.
Children are kept warm
Newborns are kept in a warm room, with no draught p 46.
Newborns are cleaned with dry/warm cloth, no bathing or washing p 46.
Body temperature is monitored.
Eye prophylaxis, Vitamin K and immunizations are given according to local policy p 46.
Summary table routine neonatal care
Good To be improved
Notes on cases and comments
Resuscitation procedures are correctly performed.
Early and exclusive breastfeeding is promoted, skin contact ensured.
Clean delivery and newborn care is practiced.
Thermal protection is practiced.
Eye and vitamin K prophylaxis and immunizations are given

Assessment of quality of care for children in selected hospitals in Ghana
Page 94
Main strengths:
Main weaknesses:
Summary score routine neonatal care Good To be improved
(to be circled) 5 4 3 2 1
Please indicate the quality of support by marking one of the 5 numbers; 5 indicates good support, 4 to 1 indicating levels of necessary improvement (4=small need for improvement, 1=urgent need for improvement).
8.3 Nursery facilities
Standards There is a separate room for sick newborn babies with their mothers. There are hygienic services for mothers. There is adequate accident prevention in place and safe disposal of sharps. Closest attention for the most seriously ill newborns/infants is provided.
Standards and criteria Good To be improved Comments
There is a separate room for sick newborn babies with their mothers Sick newborns are kept in a separate unit or room from healthy babies
Mothers of sick newborns are rooming in with their babies, with adequate facilities.
There are hygienic services for mothers
Toilets are adequate & easily available.
The mother has access to running water and to an appropriate space, near the ward, to wash herself and her child.
Mothers have access to a washing facility, to wash their own hers and their childrenʹs clothes

Assessment of quality of care for children in selected hospitals in Ghana
Page 95
Standards and criteria Good To be improved
Comments
There is adequate accident prevention in place and safe disposal of sharps
The ward is kept clean
Sharps are disposed of in a special container preventing accidents
Mothers and children sleep under insecticide treated bed nets
Closest attention for the most seriously ill newborns is provided
Summary table nursery facility
Good To be improved
Notes on cases and comments
There is a separate room for sick newborn babies with their mothers
There are hygienic services for the mothers of the newborns
Clean ward; accident prevention and disposition of sharps is in place
Closest attention for the most seriously ill newborn is ensured
Summary score routine neonatal care Good To be improved
(to be circled) 5 4 3 2 1
Please indicate the quality of support by marking one of the 5 numbers; 5 indicates good support, 4 to 1 indicating levels of necessary improvement (4=small need for improvement, 1=urgent need for improvement).

Assessment of quality of care for children in selected hospitals in Ghana
Page 96
8.4 Case management and sick newborn care
Note: Sick newborns might be admitted in different areas, the maternity ward or the infant ward. Information should be primarily by case observation Standards Neonatal sepsis is appropriately diagnosed and investigated Neonatal sepsis is adequately treated Specific feeding needs of sick young infants and those with low birth weight are taken care of Severe jaundice is recognized and appropriately managed
Standards and criteria Good To be improved Comments
Diagnosis and investigation of neonatal sepsis
Neonatal sepsis is suspected in neonates with signs such as fever or difficulty feeding and appropriately investigated (e.g. urine microscopy, foci of infection) pp 47, 53.
Lumbar puncture is done to rule out/confirm meningitis pp 49,50,316.
Newborns receive oxygen if cyanosed or in severe respiratory distress p 52.
Treatment of neonatal sepsis
Effective antibiotics are given according to age and weight of the baby p 49‐50,62‐66.
The response to treatment is monitored p 48.
Specific feeding needs of sick young infants and those with low birth weight
All efforts are made to give mother’s milk to LBW babies p 53‐55.
Frequent feedings (at least 8 x per day) are provided to LBW‐babies and intake is monitored p 54.
To children unable to feed expressed breast milk is given by cup and spoon or fed by nasogastric tube in adequate amounts according to age. Intake is monitored p 55.
If IV‐fluids are given, they are recorded and precautions are in place to prevent fluid overload p 51,52.
In LBW‐babies, heat loss is minimized by kangaroo‐care and a cap on the head p 54.
Recognition and management of jaundice
Facilities for exchange transfusion are available, or there are guidelines when to refer a child p 58.

Assessment of quality of care for children in selected hospitals in Ghana
Page 97
Standards and criteria Good To be improved
Comments
Phototherapy and guidelines when to use it are available, and adequate hydration is ensured pp 58, 59.
Procedures are in place to check the bilirubin level.
Summary table case management and sick newborn care
Good To be improved
Comments
Neonatal sepsis is appropriately diagnosed.
Neonatal sepsis is appropriately treated.
Specific feeding needs of sick young infants and those with low birth weight, are met.
Jaundice is adequately recognized and managed.
Main strengths:
Main weaknesses:
Summary score case management and sick newborn care Good To be improved
(to be circled) 5 4 3 2 1
Please indicate the quality of support by marking one of the 5 numbers; 5 indicates good support, 4 to 1 indicating levels of necessary improvement (4=small need for improvement, 1=urgent need for improvement).

Assessment of quality of care for children in selected hospitals in Ghana
Page 98

Assessment of quality of care for children in selected hospitals in Ghana
Page 99
Assessment of the quality of hospital care for children Date: __/__/__/ Country: ____________________ Initials of Health Facility: __/__/ Initials of Assessor: __/__/
9. Paediatric surgery and rehabilitation
(p. 227‐259) Source: This information should be collected by observing the treatment and care of children undergoing surgical treatment, interviewing staff and carers and reviewing guidelines, if available. Standards Pre‐operative care is child‐friendly and fasting is kept to a minimum. Intra‐operatively, routine procedures prevent hypothermia and hypoglycaemia. Post‐operative care ensures save recovery including monitoring, pain relief and early feeding. The surgical ward is child friendly, provides food for children and opportunities to play. Paediatric‐size anaesthesia equipment is available (see table below). Basic rehabilitation equipment is available.
Standards and criteria Good To be improved
Comments
Pre‐operative care Standard procedures are in place to prepare a child for surgery: weight, haemoglobin level, blood group of the child and consent of the carer is recorded p 228‐229.
Fasting is kept to a minimum (8hrs no solids/6hrs no formula/4 hrs no milk or clear liquids) and children are put first on the operating list to avoid unnecessary starving p 228.
Intra‐operative care
The child is kept warm during surgery and IV‐fluids containing glucose are given for long procedures (e.g. 0.45% NaCl + 5% glucose) p 231.
Guidelines are in place for the safe use of local anaesthetic (weight adjusted) p 229.
Blood loss is monitored p 231.
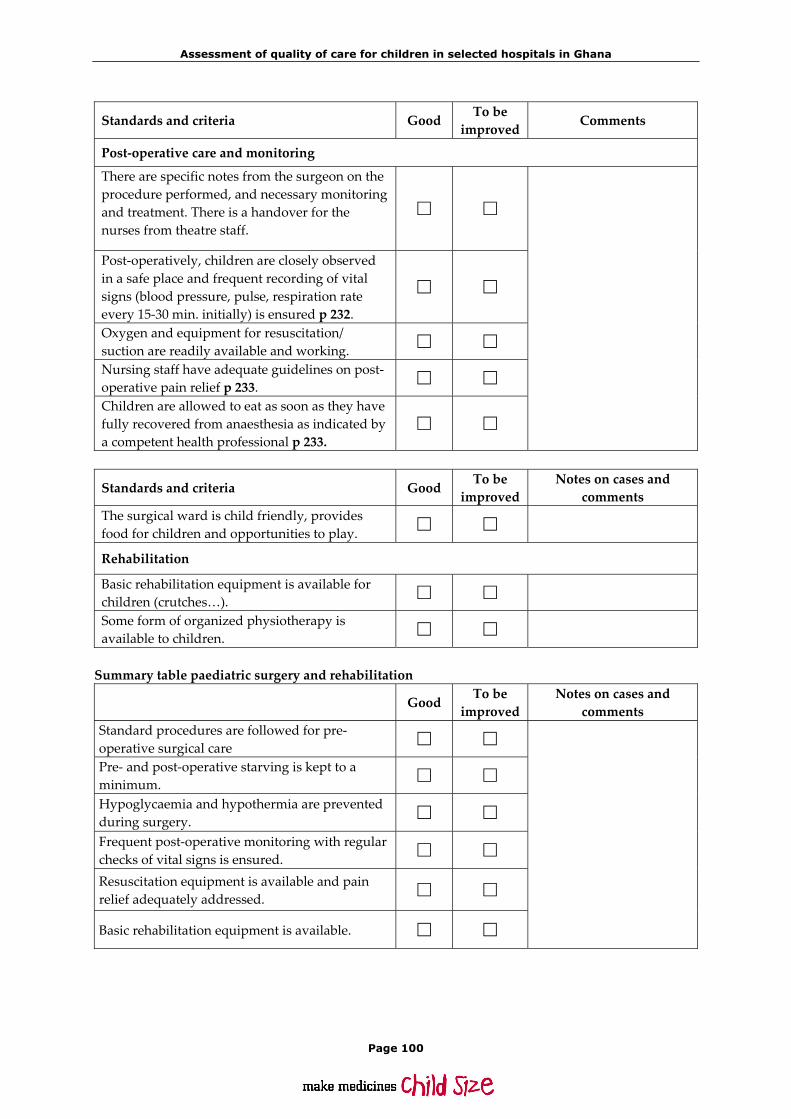
Assessment of quality of care for children in selected hospitals in Ghana
Page 100
Standards and criteria Good To be improved
Comments
Post‐operative care and monitoring
There are specific notes from the surgeon on the procedure performed, and necessary monitoring and treatment. There is a handover for the nurses from theatre staff.
Post‐operatively, children are closely observed in a safe place and frequent recording of vital signs (blood pressure, pulse, respiration rate every 15‐30 min. initially) is ensured p 232.
Oxygen and equipment for resuscitation/ suction are readily available and working.
Nursing staff have adequate guidelines on post‐operative pain relief p 233.
Children are allowed to eat as soon as they have fully recovered from anaesthesia as indicated by a competent health professional p 233.
Standards and criteria Good To be improved
Notes on cases and comments
The surgical ward is child friendly, provides food for children and opportunities to play.
Rehabilitation
Basic rehabilitation equipment is available for children (crutches…).
Some form of organized physiotherapy is available to children.
Summary table paediatric surgery and rehabilitation
Good To be improved
Notes on cases and comments
Standard procedures are followed for pre‐operative surgical care
Pre‐ and post‐operative starving is kept to a minimum.
Hypoglycaemia and hypothermia are prevented during surgery.
Frequent post‐operative monitoring with regular checks of vital signs is ensured.
Resuscitation equipment is available and pain relief adequately addressed.
Basic rehabilitation equipment is available.

Assessment of quality of care for children in selected hospitals in Ghana
Page 101
Summary score paediatric surgery and rehabilitation Good To be improved
(to be circled) 5 4 3 2 1
Please indicate the quality of support by marking one of the 5 numbers; 5 indicates good support, 4 to 1 indicating levels of necessary improvement (4=small need for improvement, 1=urgent need for improvement).
9.1 Paediatric-size anaesthesia equipment
Paediatric size are: available, in good working condition
not always available not available
Tracheal tubes
Face masks
Laryngoscope blades
Oropharyngeal airways
Breathing valves
Resuscitation bags
Blood pressure‐cuffs

Assessment of quality of care for children in selected hospitals in Ghana
Page 102

Assessment of quality of care for children in selected hospitals in Ghana
Page 103
Assessment of the quality of hospital care for children Date: __/__/__/ Country: ____________________ Initials of Health Facility: __/__/ Initials of Assessor: __/__/
10. Other hospital wards with children
Check whether children are admitted to other hospital departments, such as the infectious disease ward or intensive care unit. Assess the adequacy of the layout for children, staffing with paediatric expertise, availability of supplies for children (e.g. paediatric size cannulae, food supply), and knowledge of monitoring and case management of children. Notes and comments: Layout:
Staffing:
Supplies and equipment for paediatric care:
Monitoring of children:

Assessment of quality of care for children in selected hospitals in Ghana
Page 104
Supportive therapy for children:

Assessment of quality of care for children in selected hospitals in Ghana
Page 105
Assessment of the quality of hospital care for children Date: __/__/__/ Country: ____________________ Initials of Health Facility: __/__/ Initials of Assessor: __/__/
11. Hospital administration
This section builds on findings in the section ʺGeneral hospital informationʺ obtained during the visit. It complements this information by findings during the visit, and might pull together items that were obtained by different team members. Standards Adequate and updated treatment guidelines are available and implemented. Audits with all staff participating and in regular intervals are performed. Essential drugs are stocked, a safe supply ensured and old drugs used first. Essential equipment is available and serviced. Essential lab tests are reliably performed and results speedily forwarded. Transport for referral is available. Standards and criteria Good To be
improved Comments
Availability of adequate and updated treatment guidelines A recent paediatric textbook is easily available (last five years). Standard treatment guidelines are available as pocket instructions, wall charts or job aids . Recommended antibiotics for common infections according to hospital essential drugs list are available. Pocket guidelines, protocols and wall charts for emergency care are available. Newborn resuscitation is described in wall charts.
Performance of audits
Audits and regular staff meetings are conducted to review clinical practice and mortality problems with the organization at the hospital. The audits take into account monitoring, hospital flow and quality of care as well as more academic aspects on diagnosis. All staff categories participate in the audit.
Essential drugs (see list above) are always available and there is no demand for prior payment p 14,15.
Essential equipment (see list above) is available and functioning properly pp 16,17.

Assessment of quality of care for children in selected hospitals in Ghana
Page 106
Standards and criteria Good To be improved
Comments
Essential laboratory tests (see list above) are available and delivered in a timely manner p 19.
Transport for referral is available.
Summary table hospital administration Good To be
improved Comments
Adequate and updated treatment guidelines are available at the hospital.
Audits on hospital deaths and clinical practice are performed.
Essential drugs are available.
Essential equipment is available.
Essential laboratory support is available.
Transport is available for referral.
Main strengths:
Main weaknesses:
Summary score hospital administration Good To be improved
(to be circled) 5 4 3 2 1
Please indicate the quality of support by marking one of the 5 numbers; 5 indicates good support, 4 to 1 indicating levels of necessary improvement (4=small need for improvement, 1=urgent need for improvement).

Assessment of quality of care for children in selected hospitals in Ghana
Page 107
Assessment of the quality of hospital care for children Date: __/__/__/ Country: ____________________ Initials of Health Facility: __/__/ Initials of Assessor: __/__/
12. Access to hospital care: Interview with caretakers and health workers
Interview 2‐3 mothers or caretakers about their experience of care seeking before coming to hospital. This part of the form is intended to provide a background to the child’s condition, and to document factors which are outside the hospital. Where necessary, complement with interviews of staff to obtain their perspective.
Standards and criteria Notes Referral by first level or primary health care worker Patients referred from first‐level facilities are correctly assessed and classified for the most common conditions requiring referral (IMCI standards for districts where IMCI has been implemented). Expected classifications (and reasons for referral would be: severe pneumonia or very severe disease, very severe febrile disease, etc. ‐ see IMCI guidelines for classifications requiring referral). Check referral notes. Referred patients receive appropriate pre‐referral treatment when indicated. Referred patients are provided with referral notes stating the condition, reason for referral and any treatment given.
Transport to hospital Lack of transport to hospital is not a cause of delayed referral. Own or commercial transport is available to get to hospital. The hospital is geographically accessible Cost for transport does not represent a major barrier to referral.
Care seeking by parents Parents adequately recognize signs and symptoms that require contact with health services. Ask the mother open questions on how her child fell ill and probe into what she did, in which order and when and why she decided to seek help. Sick children are brought to health services without significant delay. If delays in care seeking exist, try to find out why. Parents bring their children to hospital without major delay when advised by first‐level health staff that the child is in need of referral care.

Assessment of quality of care for children in selected hospitals in Ghana
Page 108
Standards and criteria Notes Economic barriers to hospital care Hospital fees do not pose a major barrier to hospital care for the majority of patients. (Ask about all types of fees, such as: admission fees, cost of drugs or laboratory investigations, examinations, equipment used at the hospital). “major” to be defined as high enough to represent, for some families, a barrier to seeking and obtaining hospital care or the need for the parents to borrow money to be able to have access to care. Hospital fees are clearly communicated to the carers and fees are displayed in the ward/hospital. Did carers at any point have to pay a fee without knowing which services payment was for?
Traditional medicine Was a traditional practitioner consulted prior to going to the hospital? If yes: Why was the traditional medicine practitioner preferred (fees, transport, culture…)? What treatment was received? How much was paid for the traditional medicine (incl. goods)? Why did they come to the hospital now (referred,…) By how much was the hospital visit delayed due to the visit?
Summary table access to hospital care interview Good To be
improved Comments
Appropriate referral by PHC.
Transport easily available.
Appropriate care‐seeking by parents.
No significant fees or economic barriers to hospital services.
Traditional medicine no barrier to access to hospital.
Main strengths:

Assessment of quality of care for children in selected hospitals in Ghana
Page 109
Main weaknesses:
Summary score access to hospital care Good To be improved
(to be circled) 5 4 3 2 1
Please indicate the quality of support by marking one of the 5 numbers; 5 indicates good support, 4 to 1 indicating levels of necessary improvement (4=small need for improvement, 1=urgent need for improvement).

Assessment of quality of care for children in selected hospitals in Ghana
Page 110

Assessment of quality of care for children in selected hospitals in Ghana
Page 111
Summary evaluation score
Summarize the individual items found above in this summary sheet to guide the discussion with senior hospital staff at the debriefing.
Good To be improved
5 4 3 2 1
1. Summary score essential drugs, supplies and equipment
2. Summary score laboratory support
3. Summary score emergency area and management
4. Summary score childrenʹs ward and facilities
5. Summary score cough or difficult breathing
6. Summary score diarrhoea
7. Summary score fever conditions
8. Summary score malnutrition
9. Summary score HIV/AIDS
10. Summary score supportive care
11. Summary score monitoring
12. Summary score routine neonatal care
13. Summary score nursery facilities
14. Summary score case management and sick newborn care
15. Summary score paediatric surgery and rehabilitation
16. Summary score hospital administration
17. Summary score access to hospital
Total score
Hospital summary score = total score/17

Assessment of quality of care for children in selected hospitals in Ghana
Page 112

Assessment of quality of care for children in selected hospitals in Ghana
Page 113
Debriefing and action plan
Discuss above summary of hospital findings with the senior hospital management, giving details as appropriate. Discuss their perception of the findings, and how action could be taken to improve services for children. Discuss importance in terms of morbidity and mortality, and the feasibility to take action. Develop a plan of action, using the following list.
Summary score
Impact on mortality and
morbidity
Action needed Feasibility Priority Timetable and responsible person
Items
To be strongly
improved
To be improved
Not to be
High
Low
High
Low
High
Low

Assessment of quality of care for children in selected hospitals in Ghana
Page 114

Assessment of quality of care for children in selected hospitals in Ghana
Page 115
Annex 1: Interviews with caretakers
Caretaker's view on patient's care
Caretaker interview
Age of interviewee: Education of interviewee:
Date child was admitted: Length of stay:
Relationship to patient: Ward
1) Time on ward with child: <25% 25%‐50% 50%‐75<% >75%
2a) How far away do you live from the hospital?
Kilometers: Hours:
3) What type of transport did you use to come to the hospital?
After arrival at the hospital, we would like to know how you were treated in the OPD.
4a) Were there any other good things about the time your child spent in outpatients? 4b) Were there any other bad things about the time your child spent in outpatients? 5) What do you think about the care in OPD, before your child was admitted:
Worse than expected
As expected
Better than expected
5a) The actual time you had to wait was ___ hours. This was: □ □ □ 5b) The politeness with which you were treated: □ □ □ 5c) The care the prescriber took in the history and examination (the completeness of his/her assessment) of your child’s problem
□ □ □
6) Was the reason for admission explained to you? Yes/No
7) What was the reason for admission?

Assessment of quality of care for children in selected hospitals in Ghana
Page 116
We are also interested in what you thought about the ward and care of your child.
8) Once your child was on the ward what did you think about:
Better than expected
As expected
Worse than expected
8a) The amount of space for you and your child to stay? Comment □ □ □ 8b) The place/bed where you and your child slept? If worse than expected what was bad about it? Comment:
□ □ □
8c) The place to wash and the toilet If worse what was bad about it? Comment
□ □ □
8d) The cleanliness of the ward Comment □ □ □ 8e) The number of nurses available to look after the sick children. The number was □ □ □ 8f) The care the doctor took over re‐examining your child on the ward (the completeness of his/her assessment)? □ □ □ 8g) Did the nurses/doctors check your child often enough? □ □ □ 8h) The nurses/doctors examined your child well/long enough? □ □ □ 9) Are there other things about the ward itself or the hospital site that concern you?
We now would like to know what you thought about the medical care on the ward.
10) What do you think about the actual medical treatment your child received:
Too often/ much
OK Too few/ little
N/A
10a) Blood was taken____ times. This was…..? □ □ □ □ 10b) The amount of blood taken was: □ □ □ □ 10c) Injections were given ____ times. This was….? □ □ □ □ 10d) Intravenous fluids were given: □ □ □ □

Assessment of quality of care for children in selected hospitals in Ghana
Page 117
11) What other tests/treatments were done (lumbar puncture, blood transfusion etc.)? What did you feel about each of these (were they harmful/necessary/explained/useful?) 12a) What have you been told your child is suffering from? 12b) From whom did you receive most information about the disease of your child? 12c) Who was the person you could ask most easily about the care of your child? 13) Did you want to know more about the sickness your child had and the tests and treatment s/he had? Yes/No If yes, what did you want to know more about? 14) Did you learn anything new on how to keep your child healthy while on the ward? Yes/No If yes what did you learn and who told you about it?
We now want to ask you what you thought about the staff looking after your child.
15) What was the attitude of the different types of staff towards you and your child most of the time? Polite, helpful
Good or bad at different times
Rude, unhelpful
15a) Doctors □ □ □ 15b) Nurses □ □ □ 15c) Cleaning/kitchen staff/junior staff □ □ □ 15d) Other hospital staff (e.g. nutritionists/x‐ray / physiotherapists/laboratory etc.)
□ □ □ 16a) Can you think of any examples or ways in which you were spoken to or dealt with well? 16b) Can you think of any examples or ways in which you were spoken to or dealt with badly?

Assessment of quality of care for children in selected hospitals in Ghana
Page 118
Finally, we would like to ask you about your discharge from hospital.
17) What do you think of the condition of your child now (at the time of discharge)?
Very good OK Still poor
18) Do you think the amount of time spent in hospital was?
Too long Just right Too short
19) Is your child to be sent home on medicines? Yes/No
20) Did the ward staff tell you how much to give? Yes/No
21) Did the ward staff tell you how often to give the medicines to take home? Yes/No
22) Did the ward staff tell you how many days you should give the medicines when you are at home?
Yes/No
23) Did you receive a follow‐up appointment to see how your child is doing? 23a) If yes, why do you have to go? If no, go to question 27.
Yes/No
24) Did the doctor/ward staff tell you where to go? Yes/No
25) Do you know when to go to the follow‐up appointment? Yes/No
26) Did you receive a discharge/follow‐up note explaining the illness of your child and providing information for the staff at the follow up clinic and the time/place of follow‐up? * Verify that the details are included as discussed.
Yes/No
27a) Is your child on NHIS Yes/No 27b) If no, what do you think about the cost of treatment at the hospital? (Add questions on how the family finance the hospital stay of the child?/If costs are clearly communicated?/If they had to pay fees without being clear what they were for?) 28) Looking back on the time your child was in hospital what, if any, are the areas that you think need most improvement to make the admission and stay easier to bear? 29) Overall, how satisfied are you with the care of your child at the hospital?

Assessment of quality of care for children in selected hospitals in Ghana
Page 119
Summary table interviews with caretakers Good To be
improved Notes on cases and
comments Caretaker is satisfied with procedures at OPD, knows reason for admission.
On the ward procedures are explained and staff is supportive.
Carer knows how to continue medicine and knows when and where to go for follow up.
Main strengths:
Main weaknesses:
Summary score caretakersʹ satisfaction with hospital care Good To be improved
(to be circled) 5 4 3 2 1
Please indicate the quality of support by marking one of the 5 numbers; 5 indicates good support, 4 to 1 indicating levels of necessary improvement (4=small need for improvement, 1=urgent need for improvement).

Assessment of quality of care for children in selected hospitals in Ghana
Page 120

Assessment of quality of care for children in selected hospitals in Ghana
Page 121
Annex 2: Interviews with health workers
A 2.1 Guidance for health workers' interview
All groups of health workers should be considered for this interview. This includes cleaners, health assistants, nurses, matron, medical assistants and doctors. We would like to record the health workersʹ honest opinions. For this it is important that the health workers understand the aims of the survey and know and trust that the information will be stored and used while maintaining confidentiality. Please let them know that their names or initials will not be mentioned in any report or to supervisors in the hospital. Please do not leave forms lying about or in a place where people who are not members of the team can read them. Try to interview two staff each from the above mentioned categories of health workers so that a minimum of six to eight forms should be completed during the assessment visit. Health workers are welcome to fill in the forms themselves, however, please do not let them take the form away and return it later, due to the shortness of your stay. Ask the questions in a face‐to‐face interview in a suitable place. At the end of the interview you should be happy for the health worker to read whatever is written down, and they should be offered the chance to read the form and make any changes. Try to record comments as they are spoken rather than trying to summarize the views expressed. Recording the real words used often helps to properly represent what the person is trying to say. When doing this please put the comments in quotation marks. For example: “We have a real problem with the water supply, sometimes days go by without piped water, how can we wash our hands to prevent spreading infection?” To start, please fill in the date, the hospital name and the health workerʹs initials on all five sheets. After this, please fill in the small amount of information on the interviewee, so that the answers in the questionnaire can be put in better perspective. Question 1: We begin the interview with an open question. Some health workers may have several things to say without prompting them with specific questions. For these people it is important to allow them the chance to speak and to record what they actually say as far as possible. Question 2 : In question 1, you are asked to mark the quality of the facilities of the childrenʹs ward. Please see the criteria below for the four possible responses:

Assessment of quality of care for children in selected hospitals in Ghana
Page 122
Table 2: Explanation of the scale ʺGoodʺ to ʺUsually inadequateʺ Usually inadequate On four or more out of ten times when something is used or wanted
or on four or more out of ten visits to an area things are unavailable or not of an acceptable standard.
Occasionally inadequate On two to three out of ten times when something is used or wanted or two to three out of ten visits to an area things are unavailable or are not of an acceptable standard.
Fair On one out of ten times when something is used or wanted or once out of ten visits to an area things are unavailable or are not of an acceptable standard.
Good Only rarely are things unavailable or are not of an acceptable standard.
Question 3: This question is meant to highlight the understanding of the health worker about which disease contributes most to inpatient mortality. In question 3b) difficulties in the care of these important conditions are explored. Question 4: To answer this question please refer to Table 1. Question 5: Please write down the words as spoken by the interviewee. Questions 6‐10: To answer the questions, please refer to Table 1. Question 14: All forms of training should be considered from on‐the‐job training, introduction to new equipment/procedures to workshops or courses taught outside the hospital. Question 15: In a number of institutions, nursing staff is rotated within different wards at regular intervals. Please find out if this is the case, what the interviewee thinks about it and to which professional groups this applies. Questions 16, 17: In this question we are interested in if there are some form of meetings which reflect on the quality of care in the hospital/ward and the communication within the hospital. Question 18: Please mention the type of guidelines (books, posters, charts, oral guidelines, etc.). Questions 19‐21: Please refer to Table 1. Finally: Before thanking the interviewee, please ensure that all questions are answered. If a health worker does not want to answer a particular question please note this and proceed to the next question. Offer the health worker the opportunity to read what you have written. If s/he wishes s/he should be allowed to make changes. Please thank her/him for forwarding the information.

Assessment of quality of care for children in selected hospitals in Ghana
Page 123
A2.2 Health worker interview
Health worker interview
Position of health worker being interviewed:
Current place of work (childrenʹs ward, paediatric OPD, nursery etc.):
How long have you worked at this hospital?
How long have you been working in the nursery, paediatric OPD or childrenʹs ward?
We are first interested in your views on the childrenʹs ward.
1) Are there any things about the hospital buildings/ward that you think are good or things that could be improved?
2) For children admitted to the hospital Good Satis‐ factory
Occasionally inadequate
Usually inadequate
2a) the accommodation (space/beds) for patients is □ □ □ □ 2b) the toilets and washing facilities for patients are □ □ □ □
2c) the cleanliness of the ward is … □ □ □ □
2d) the food given to the children is … □ □ □ □
Now we would like to ask you what the causes of childrenʹs death are in the hospital.
3) In your opinion what are the commonest illnesses resulting in childhood deaths in the hospital?
1.
2
3
4
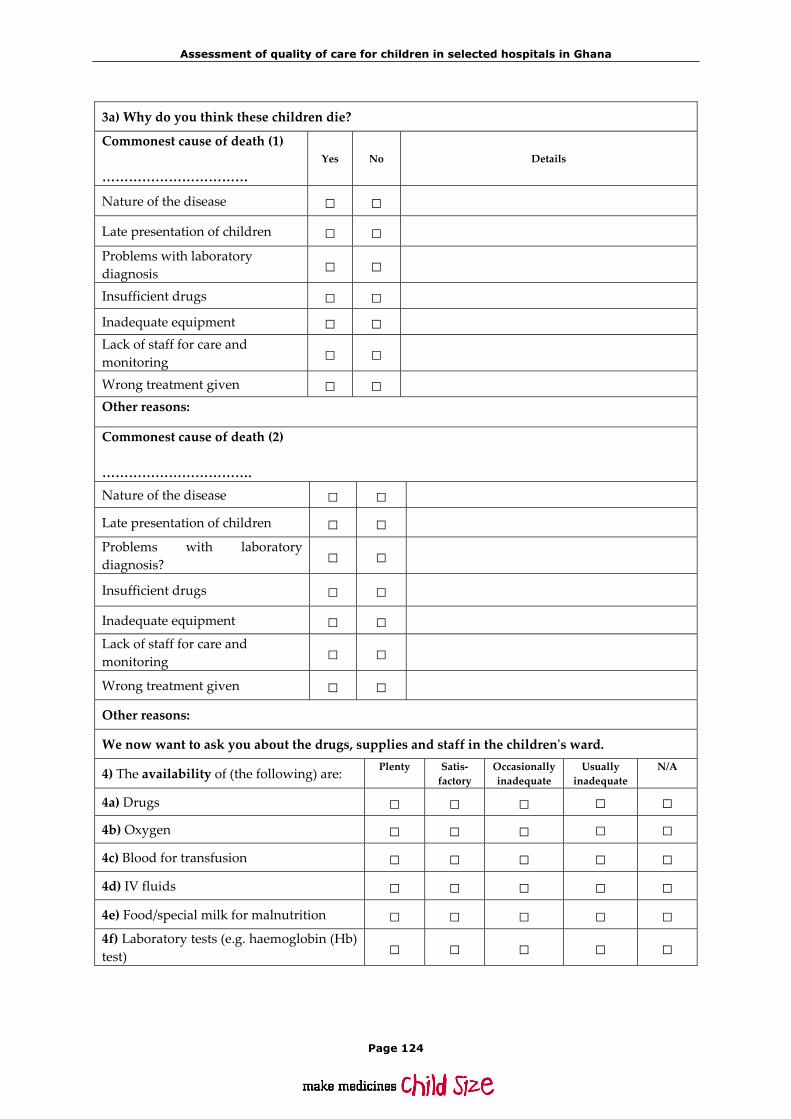
Assessment of quality of care for children in selected hospitals in Ghana
Page 124
3a) Why do you think these children die?
Commonest cause of death (1) ……………………………
Yes No Details
Nature of the disease □ □
Late presentation of children □ □
Problems with laboratory diagnosis □ □
Insufficient drugs □ □
Inadequate equipment □ □ Lack of staff for care and monitoring □ □
Wrong treatment given □ □ Other reasons:
Commonest cause of death (2) ……………………………. Nature of the disease □ □
Late presentation of children □ □ Problems with laboratory diagnosis? □ □
Insufficient drugs □ □
Inadequate equipment □ □ Lack of staff for care and monitoring □ □
Wrong treatment given □ □
Other reasons:
We now want to ask you about the drugs, supplies and staff in the childrenʹs ward.
4) The availability of (the following) are: Plenty Satis‐ factory
Occasionally inadequate
Usually inadequate
N/A
4a) Drugs □ □ □ □ □ 4b) Oxygen □ □ □ □ □ 4c) Blood for transfusion □ □ □ □ □ 4d) IV fluids □ □ □ □ □ 4e) Food/special milk for malnutrition □ □ □ □ □ 4f) Laboratory tests (e.g. haemoglobin (Hb) test) □ □ □ □ □

Assessment of quality of care for children in selected hospitals in Ghana
Page 125
5) Do you have problems with/lack any other equipment or supplies that make it hard to look after sick children well or are supplies generally good? The availability of staff: Plenty Satisfactory
Occasionally inadequate
Usually inadequate
6) Do you think the number of staff available to care for sick children is? □ □ □ □ 7) Do you think there is enough time available to care for a child in the best way you know how to (the way you were trained)?
□ □ □ □
8) There is sufficient nursing staff during the night. □ □ □ □ 9) There is sufficient nursing staff during the weekend. □ □ □ □ 10) If you have a problem with a sick child is supervision/support (e.g. from more senior clinical staff) available to you?
□ □ □ □
11) Do you think the hospital lacks any important staff to help look after sick children? Are the number and quality of staff in general good? 12) If you have problems getting help when you think you need it is it because: ...there are not enough skilled people to call? …you are unable to contact the right people? …the response to your request is too slow? …another reason?

Assessment of quality of care for children in selected hospitals in Ghana
Page 126
What do you think about the training of staff and the organization of your work?
Training of staff Very good OK Occasionally inadequate
Usually inadequate
13) How is your own knowledge about the illnesses of children? □ □ □ □ 13a) If it is sometimes inadequate what areas do you think you need more training on or are there areas you would like to improve your knowledge of further? 14) Are there possibilities for further in‐service training in your hospital? Please explain. 15) Is there a fixed rotation of nursing staff within the hospital at regular intervals? Yes/No 15a) If yes, how often do you rotate? 15b) What do you think about this? 16) Are there regular meetings of all nurses/other staff/doctors who work on the childrenʹs ward? Please explain who participates, frequency and nature of meetings. 17) Is there a regular feedback/audit session in terms of quality of care/mortality in the childrenʹs ward? Please explain. 18) Do you have clear guidelines on the work you are doing. Please explain:

Assessment of quality of care for children in selected hospitals in Ghana
Page 127
We would like to know what you think about the care you/the hospital give to children
Very good OK
Occasionally inadequate
Usually inadequate
19) The information/explanations families are given about their child’s illness is … □ □ □ □
20) The time you have to explain to the parents and children about their illness is … □ □ □ □
21) How do you think the caretakers view the care on the ward? □ □ □ □ 22) Can you think of any ways to improve parents’ understanding of their children’s illness? 23) Care of children Can you remember a child you looked after recently when you were pleased with how things turned out? Yes/No 23a) If yes, were you pleased with how you helped the child do well? 23b) What aspects of your own performance/role pleased you? 24) Can you think of a child you looked after recently when you were disappointed with how things turned out? Yes/No 24a) If yes, what aspects of the child’s care/progress did you think went badly and what do you think were the reasons for this? Always Often Sometimes Rarely Never
25) Overall are you pleased with what this hospital is able to do to help sick children while on the ward?
□ □ □ □ □

Assessment of quality of care for children in selected hospitals in Ghana
Page 128
26) Are there any other things that were not mentioned yet that could be changed to improve the care of children in the hospital? 27) Have you ever suggested these improvements to matron/doctors/management and with what results? 28) Do you think the majority of your colleagues are generally satisfied with their work in the hospital? Yes/No 28a) What things do you think make people dissatisfied with their work? 28b) What about the working conditions? 28c) What could be improved to make people in the hospital more satisfied with their work?