
Quality and Innovation Centers: Kaiser...
18
12/11/2012 1 Quality and Innovation Centers: Kaiser Permanente By: Alide Chase, senior vice president Medicare Clinical Operations and Population Care And Lisa Schilling, RN MPH vice president Healthcare Performance Improvement Care Management Institute M14 These presenters have nothing to disclose. December 10, 2012 8:30am – 12:00 pm 2 Our Numbers 8 regions serving 9 states and the District of Columbia 8.9 million members (as of 2/11) 15,000 physicians 164,000 employees (including 45,000 nurses) 37 medical centers (with hospitals) 454 medical offices (ambulatory care buildings) $44 billion operating revenue (2010)
-
Upload
truongdang -
Category
Documents
-
view
221 -
download
0
Transcript of Quality and Innovation Centers: Kaiser...
12/11/2012
1
Quality and Innovation Centers: Kaiser PermanenteBy: Alide Chase, senior vice president Medicare Clinical Operations and Population Care
And
Lisa Schilling, RN MPH vice president Healthcare Performance Improvement
Care Management Institute
M14These presenters have
nothing to disclose.
December 10, 2012
8:30am – 12:00 pm
2
Our Numbers
� 8 regions serving 9 states and the District of Columbia� 8.9 million members (as of 2/11)� 15,000 physicians � 164,000 employees (including 45,000 nurses)� 37 medical centers (with hospitals)� 454 medical offices (ambulatory care buildings)� $44 billion operating revenue (2010)

12/11/2012
2
3
Kaiser Permanente Quality Improvement Journey
2005-2007
2008-2010
2011-Beyond
•Established strategic partnership
with IHI
•Develop enterprise quality strategy
•KP HealthConnect
implementation begins• Assess baseline capability
to improve
• Estalish KP’s big dots the “Big Q”
•Some best performance in KP and
high variation•Establish IHI scholarship program for
KP and safety net
• Develop Improvement Institute
•Hire master black belt mentors
•Adopt IHI’s execution model
in medical centers
• Focus on alignment,
portfolio management
achieving scale
•Deepen commitment to
analytics, evaluation and
research
• KP HealthConnect fully implemented, optimizing
•More PSO graduates than any
other organization
•Targeted participation in IHI
programming based on strategic need
• Align innovation, improvement in
key strategies
• Focus on technology integration,
informatics and improvement at
scale
• Develop deep capability at
regional levels
• Expand capability to operate as a
learning organization via
networks and KM
• 4 part series published in the Joint
Commission Journal
• KP NCQA results, Medicare Stars best
in class performance across KP
•Created Clinical Effectiveness Research
Center•Focus on total health
Our system is based on the attributes of high performing organizations
Best quality
Best service
Most affordable
Best place to
work
KP builds capability in these six areas in order to achieve breakthrough performance
© Kaiser Permanente 2010 reproduce by permission only

12/11/2012
3
To
p d
ow
n
Re
du
ce
va
ria
tio
n
Learning system
• Economic and social context for change
• Models of workplace learning
• Team performance
• Define organizational needs • Create system view• Plan/ manage improvement
• Align with strategy • ID drivers and portfolios • Build capability to improve
• Engaging the hearts and minds of the front line
• Creating “line of sight” to strategic goals
• Define high performing unit-based teams
Bo
ttom
up
Le
arn
ing
an
d im
pro
ve
me
nt
High Performing Organizations Build Culture and Capability
Principles What we “do”
© Kaiser Permanente 2010 reproduce by permission only
6
Building Will
Source: IHI 2008
Define Breakthrough
goals
Manage Local
ImprovementDevelop Capability
Spread and sustainProvide Leadership for
Large system Projects
Provide Day-to-Day
Leaders for Micro Systems
Source: IHI 2008
© Kaiser Permanente 2011 reproduce by permission only
12/11/2012
4
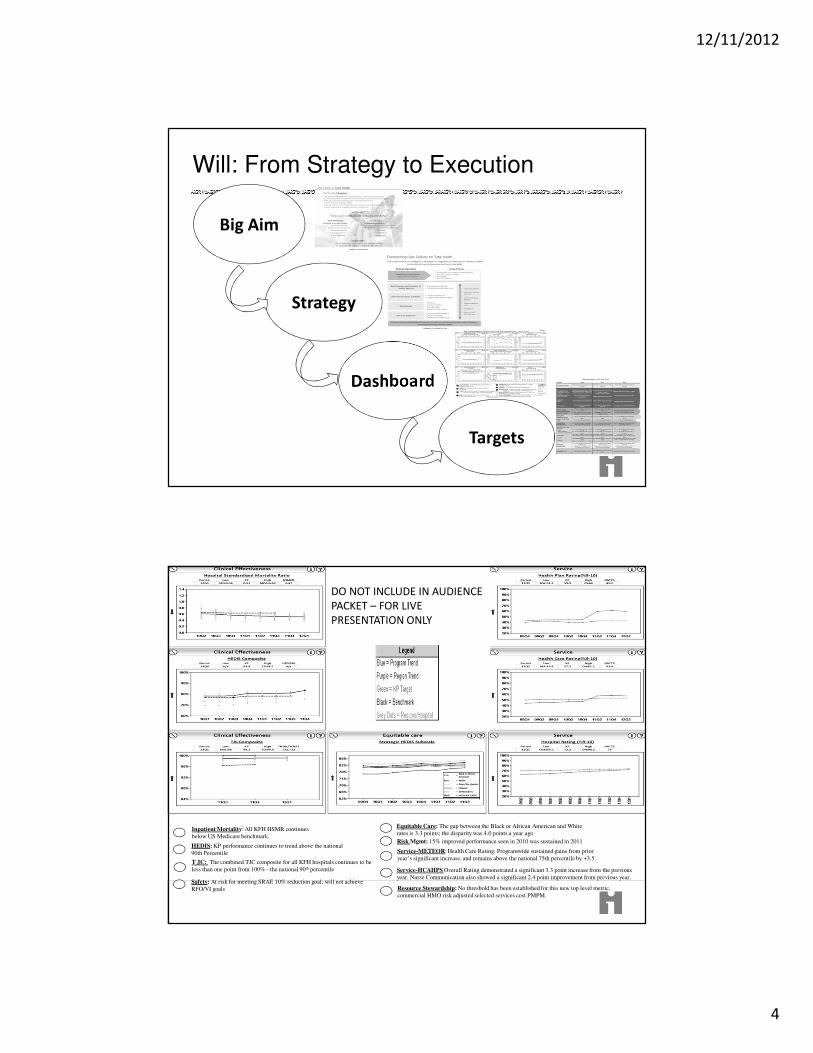
Will: From Strategy to Execution
Big Aim
Strategy
Dashboard
Targets
P8P8
Inpatient Mortality: All KFH HSMR continues
below US Medicare benchmark.
HEDIS: KP performance continues to trend above the national
90th Percentile
Safety: At risk for meeting SRAE 10% reduction goal; will not achieve
RFO/VI goals
Risk Mgmt: 15% improved performance seen in 2010 was sustained in 2011
Service-METEOR: Health Care Rating: Programwide sustained gains from prior
year’s significant increase, and remains above the national 75th percentile by +3.5.
Resource Stewardship: No threshold has been established for this new top level metric,
commercial HMO risk adjusted selected services cost PMPM.
Equitable Care: The gap between the Black or African American and White
rates is 3.3 points; the disparity was 4.0 points a year ago
.
T JC: The combined TJC composite for all KFH hospitals continues to be
less than one point from 100% - the national 90th percentile Service-HCAHPS Overall Rating demonstrated a significant 3.3 point increase from the previous
year. Nurse Communication also showed a significant 2.4 point improvement from previous year.
DO NOT INCLUDE IN AUDIENCE
PACKET – FOR LIVE
PRESENTATION ONLY

12/11/2012
5
9
Ideas: Manage Local Improvement
Define Breakthrough
goals
Manage Local
ImprovementDevelop Capability
Spread and sustainProvide Leadership for
Large system Projects
Provide Day-to-Day
Leaders for Micro Systems
Source: IHI 2008
© Kaiser Permanente 2011 reproduce by permission only
10
Identifying Levers of Improvement: Driver Diagrams
12/11/2012
6
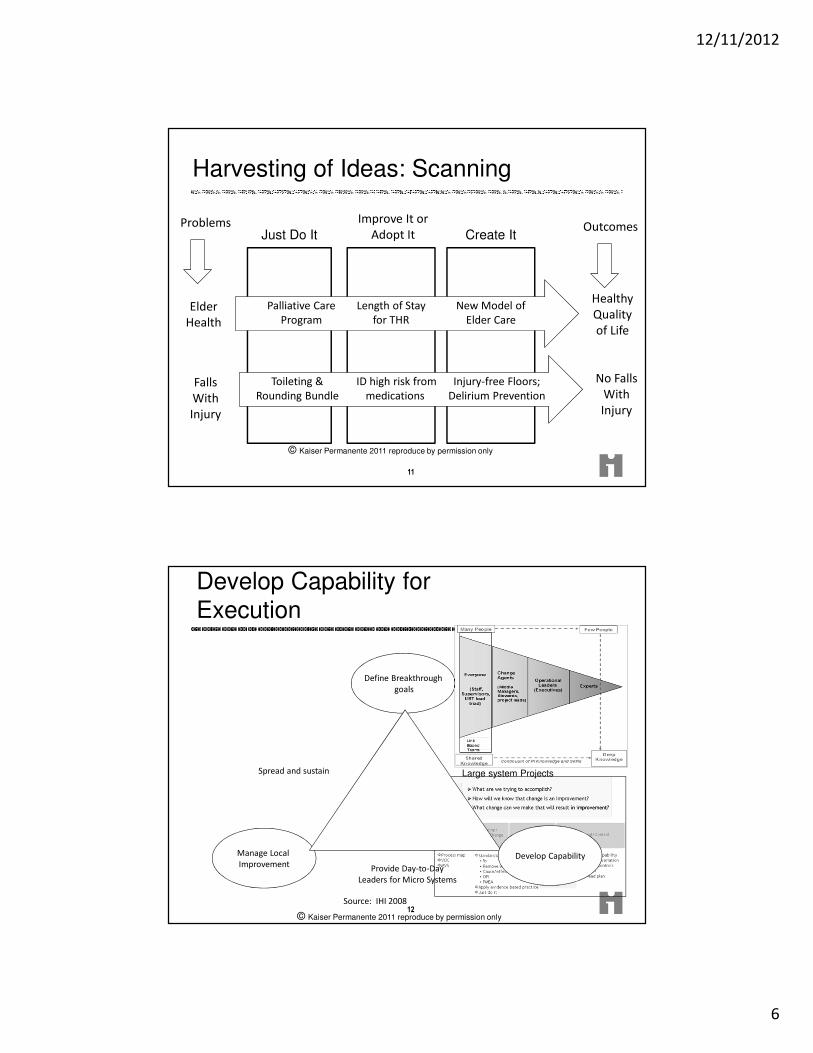
Harvesting of Ideas: Scanning
Just Do It
11
Create It
Improve It or
Adopt It
Elder
Health
Palliative Care
Program
Length of Stay
for THR
Problems Outcomes
New Model of
Elder Care
Healthy
Quality
of Life
Falls
With
Injury
Toileting &
Rounding Bundle
ID high risk from
medications
Injury-free Floors;
Delirium Prevention
No Falls
With
Injury
© Kaiser Permanente 2011 reproduce by permission only
12
Develop Capability for Execution
Source: IHI 2008
Define Breakthrough
goals
Manage Local
ImprovementDevelop Capability
Spread and sustainProvide Leadership for
Large system Projects
Provide Day-to-Day
Leaders for Micro Systems
© Kaiser Permanente 2011 reproduce by permission only

12/11/2012
7
Experts Operational
Leaders (Executives)
ChangeAgents
(Middle Managers, Stewards,
project leads)
Everyone
(Staff, Supervisors,
UBT lead triad)
Continuum of PI Knowledge and Skills
Deep
Knowledge
Many People Few People
Our approach will be to make sure that each group receives the knowledge and skill sets they need
when they need them and in the
appropriate amounts.
A key operating assumption of
building capacity is that different groups of people will have different levels of
need for PI knowledge and skill.
Content: What Skills Do We Need?
Shared
Knowledge
© Kaiser Permanente 2010 reproduce by permission only
On-boarding
Develo
pan
d T
est
the S
yste
m
at
a F
acilit
y l
evel
Developing deeper capability to achieve big results over time
Exp
an
dIm
pro
vem
en
t syste
m
to a
ll f
acilit
ies
Deep
en
imp
rovem
en
t kn
ow
led
ge w
ith
in f
acilit
ies
September 2008 June 2009 2010 & 2011
Waves of Improvement Institute
Learning and sharing systems regionally and program-wide Improvement Institute
Implementation ExpansionContinuous
ImprovementComplete
Thi
s
im
We are here
Level of Project
Difficulty
• All Regions• 500 IA’s• 15 internal faculty
Mentors• 3,000+ Operations
Managers• 20,000+ Front line staff• IHI Forum and courses
• 7 regions• 300 Improvement
Advisors • 35 UBTC’s• 1,250 Operations
managers• 8,000 Front line staff• IHI Forum and courses
• 5 regions• 65 Improvement Advisors• 300 operations managers• 3,500 Front line staff• IHI Forum
© Kaiser Permanente 2010 reproduce by permission only

12/11/2012
8
Improvement Institute
Week 1
15
SPCWeek 2
Assess, Plan
Medical
CenterResults
1,200 Graduates
$200 Million
Test, Implement
Control
90 Days: Apply Learning and Get Results
Medical
Center
© Kaiser Permanente 2010 reproduce by permission only
Regional Case Study: Sepsis Care
Across 20 Medical Centers
Video NCAL Sepsis
12/11/2012
9
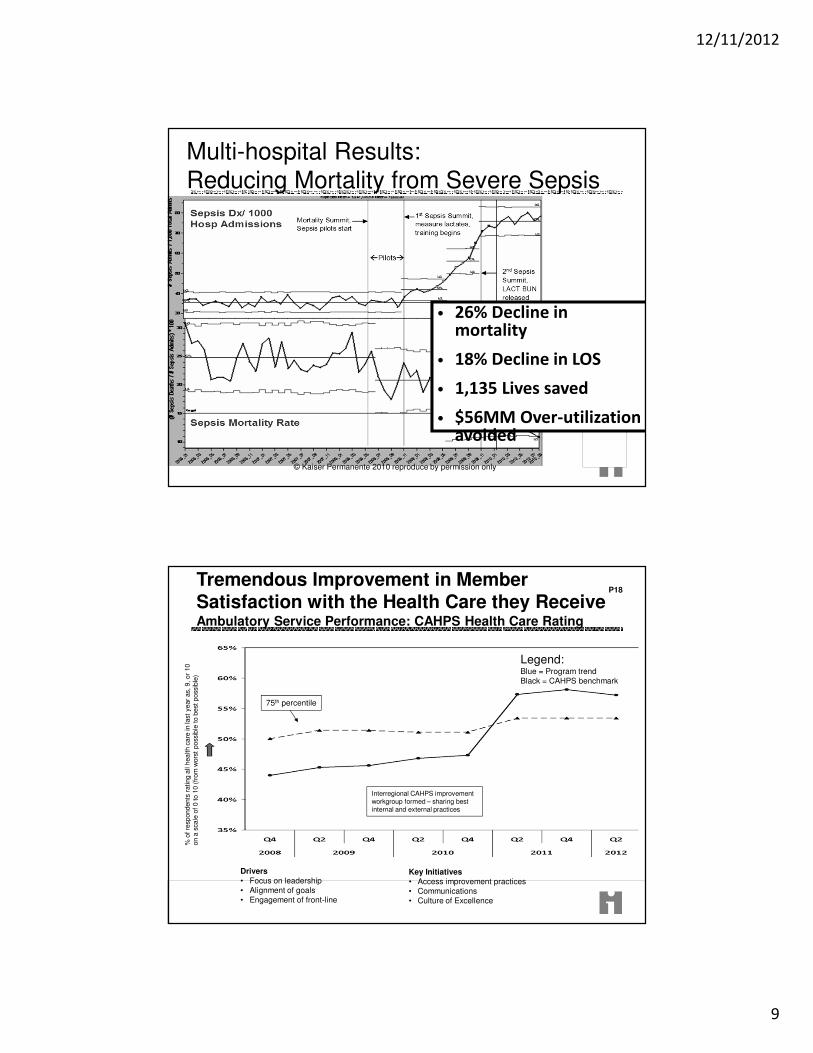
Multi-hospital Results: Reducing Mortality from Severe Sepsis
• 26% Decline in mortality
• 18% Decline in LOS
• 1,135 Lives saved
• $56MM Over-utilization avoided
© Kaiser Permanente 2010 reproduce by permission only
Tremendous Improvement in Member Satisfaction with the Health Care they Receive
P18
Ambulatory Service Performance: CAHPS Health Care Rating
Legend:Blue = Program trend
Black = CAHPS benchmark
% o
f re
spondents
rating a
ll health c
are
in la
st y
ear
as,
9, or
10
on a
scale
of 0 to 1
0 (
from
wors
t poss
ible
to b
est
poss
ible
)
Drivers• Focus on leadership
• Alignment of goals • Engagement of front-line
Key Initiatives• Access improvement practices
• Communications
• Culture of Excellence
75th percentile
Interregional CAHPS improvement workgroup formed – sharing best internal and external practices

12/11/2012
10
Leveraging the Power of Electronic Health Records: Improved Ambulatory Care
P19
Ambulatory Performance: HEDIS Composite
(PY Year 2008)
PY = Performance Year
% o
f elig
ible
mem
bers
receiv
ing a
ppro
pri
ate
am
bula
tory
care
Drivers• Population care
• Decision support
• KP.org
Clinical Effectiveness P20
Ra
tio
of
ob
se
rve
d t
o e
xp
ec
ted
mo
rta
lity
Inpatient Outcomes: Hospital Standardized Mortality Ratios
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
1.1
1.2
Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2
2008 2009 2010 2011 2012
KP - All Facilities
US Medicare Overall
Kaiser Foundation Hospital
DO NOT INCLUDE IN AUDIENCE
PACKET – FOR LIVE
PRESENTATION ONLY

12/11/2012
11
Current ChallengesAlide Chase, SVP, Medicare Clinical Operations and Population Care
Medicare Care Delivery
P21
Our Big Challenges
How to provide outstanding care in both clinical quality and care experience to our Medicare members while
reducing total cost of care?
P22
Answer:• Reliably execute on proven care• Remove variation• Transform care delivery
• Design entire system to be member/patient focused

12/11/2012
12
ValuesP23
KP's commitment to high quality of care and an excellent service experience are top priorities in the organization.
This commitment remains in place and serves as a "true north" as we face significant challenges with health care reform.
The focus on patient safety, particularly in our hospitals is a key component of the plan.
All of the Medicare initiatives will result in improved quality and service with improved efficiency and effectiveness that will help make healthcare more affordable for our members.
Our National Work
Align Care to Member Needs
Engage all of Kaiser Permanente
Spread and Execution of Proven Care
Reduce Variation
Accelerate the Development Cycle

12/11/2012
13
Care Delivery Needs Differ Across SegmentsSevere Frailty/ End of Life
Healthy Chronic Conditions
Advanced Illness
Medicare
Segmentation
15 to 20%60 to 65%
10 to 15%5 to 7%
Percent of
Members
PMPM Expense
Ratio 1X 2-3X 5-8X 15-20X
Care NeedsPopulation Care Complex CareUsual Care
P25
Data Capture and Predictive Ability
SEGMENT 1:
Healthy / RobustSEGMENT 2:
Chronic Conditions
SEGMENT 3:
Advanced Illness
SEGMENT 4:
Severe Frailty /
End-of-Life
Personalizing Care through Segmentation
Moira M Belikoff | 510-267-
2976
P26

12/11/2012
14
Insert Kat diagram here
Medicare Plan: Three Buckets of Work
First 5What we know
and do well
Unwarranted
Variation
Transformation
•Palliative Care
•Transitions
•Bone Health
•SNF ALF Rounding
•Clinical Onboarding
•Decrease unwarranted
admissions &
readmissions
•Decrease unwarranted
variation in services
•New provider roles
•Medical home
•Self Care
•Automation
•Care Planning
•Telemedicine
•Technology-enabled
community health
workers
+
+ Exce
llen
ce
28
P28
12/11/2012
15
29
• Most health
• Best care
• Most affordable
• Best people
Goal/Aim Primary Drivers Hypotheses - Secondary Drivers
Health
Care
People
Affordability
Act and Go Beyond
� EKG, angiography and imaging tests for low risk cardiac patients
� Antibiotics and imaging for sinusitis and headache
� Percent of women with second pap smear within 2 years, 6 months
� Redundant visits year after breast cancer is cured
� Screening PSA in men over 75 years of age
� Overly tight glucose control in some older adults with diabetes
� Using anticholinergic medications as a first line treatment of urinary
incontinence in older adults
Selected areas based on KP’s actionability and improvement of care :
Unwarranted Variation

12/11/2012
16
Transformation
Scanning Results
• We have identified promising tactics across all care delivery
domains
• No single strategy (internal or external) was both “high potential
impact” and “just spread now”
• Need to design and test our hypotheses for new operations and
workflows to achieve our goals
Innovation that Supports Transformation Now
• Hospital to Home: Identify way to move inpatient close to home
• Clinic to Home: Move ambulatory care from clinic to
“Everywhere” with telemedicine
• Integrate Complex Geriatric Care: Segment 3 & 4
Example of Programs IdentifiedAmerican
Physician House
Calls from TX
Advanced Illness
Care
Coordination-
Aetna
Grand-Aides Clinically HomePacific Group on
Health - CMS
Woodland Hills
“Geripal”
Program
Telepresence
visits in local
clinics
Healthy BonesSheffield Teaching
Hospitals
Univita HealthSILvR Network
InitiativeSeniorBridge
Ben Archer Health
Center
Pittsburgh
Regional Health
Initiative
Proactive Office
Encounter Work
Kaiser Special
Services (KSS)
Heart Failure
Transitional Care
Dementia Care
Birmingham, RAID
Community Care
of North Carolina
(CCNC)
medicare
innovations
collaborative
St. Vincent
Hospital
(indianapolis)
Beth Israel
Deaconess PACT
Providence
Portland Medical
Center
Complex Medical
Home- KPCares
Clinical Decision
Units
KPCO PATHWAAY
for Seniors.
Transforming
Community
Service
Nurses Improving
Care for
Healthsystem
Elders
Six Features of
effective
coordinated care
Care of the
Elderly, England
CareFirst
BlueCross Care
and Cost
Improvement
UCLA Alzheimers
and dementia care
Guided Care
ProgramPE 65
“One Stop Shop”
for Palliative Care
Primary Care and
Public Health
GRACE Team Care
(Indiana
University)
Janus Health Med StatU. of Missouri
LIGHT^2 - CMS
St. Francis
Healthcare Hawaii
Assisted Living
Facility ProgramAICC Pilot
San Rafael
Delerium
Management
Initiative
Stanford AICU
Teaching Geriatric
Skills to
Hospitalists
Council of Aging
of Southwestern
Ohio
Ocean Medical -
Advanced Care
Elderly
Developmental
Disabilities Health
Sanford Health
integrated primary
care
DriveABLE Geriatric EDPioneernetwork.n
etCapital Health Plan
Housecall
Providers, Inc.( in
Portland)
Erie St. ClairCareSouth
Carolina
Emory Critical Care
- CMS
Sutter Advanced
Illness
Management
(AIM)
Relay for Life
Advance Care
Planning
Respecting
Choices®
INTERACTBrooklyn House
Calls
Dementia Care
"Aging Brain
Care" Indiana U
UPENN
transitional care
model
Northwest
Advancing Quality
Alliance
Innovative
Oncology Business
Solutions
Indiana University
Community Rx
System
Memory Clinics Wellness ClinicsAcute Care for
EldersVitality 360
Hospital at Home
- Presbyterian Care Transitions Hospital at Home
CAPABLE for frail
dually eligible-
Johns Hopkins
University
Emergency
Medical Services
Home Visits Elder Care Clinic HELP (Yale)
Novant Health -
private duty
nursing
ACP Pilot in Palo
Alta
Janssen
Connected Care
Challenge
Finalists
Population Care
Management
Delirium detection
and prevention -
Methodist
Vanderbilt med
center - CMS
Palliative Care
Stand Alone
Clinics
Virtual Specialist PACE UCLA Scribing
P32

12/11/2012
17
KP
Care Settings
Technology Enabled
Care Settings
Community
Care Settings
Acute, Urgent & Emergent Care Encounters
Ambulatory Care Encounters
Population Care Encounters
Transformation SpacesHigh potential / high value tactics – We can improve care across our entire landscape of settings
and strategies – to provide the right care at the right time in the right place.
Geriatric
ED
Telemedicine
Monitoring
Telemedicine
Remote
Monitoring
Self Care
Mobile Apps
Self Care
Mobile Apps
Grand
Aides
Promatores
Hospital & ED
Clinic
Home
Everywhere
Call Centers / KP.OrgCare / Case
Management
Automated
Care Mgt
Continuum of Care
Neighborhoods
Social Networking
Internet Care
Communities
Internet Care
Communities
Care
Transitions
Bone Health
Palliative
Care
Assisted LivingAssisted Living
RoundingWellness
ClinicsGeriatricGeriatric
Specialty
Clinics
Geriatric
Med Home
SNF / ALF
HH
Internal
Self ServiceSelf Service
KP.org
Hosp at
HomeVirtual
Wards
Onboarding
Clinical
Onboarding
Primary Care
Home Visits
Primary Care
Home Visits
Naturally
Communities
Naturally
Occurring
Retirement
Communities
Neighborhood
Centers
Neighborhood
Health
Centers
P33
External
34Initial Demonstrations
Hospital to Home Clinic to Home Integrate Complex
Geriatric Ambulatory
Care
� Develop ways to move
inpatient care closer to
home
� Hospital to Home, Virtual
Wards
� Using telemedicine to
move ambulatory care
from the clinic to
“everywhere”
� Virtual visits,
Telemedicine, Remote
monitoring
� Address the clinical needs and
operations to support service
delivery for complex
members across the
continuum; clinic to home to
community
� Matching care to need: Think
through how operations for
the complex “micro-panel”
will integrate with the
“macro-panel” to achieve
greater affordability
• Shorten text here – get from Jann – Annie to write
KPPG Expectations: Each Participating Region and Demonstration Will:
• Designate a Health Plan and Medical Group executive who will be accountable for the Demonstration outcomes
• Define specific affordability hypotheses that can be quantified
• Set targets and define metric indicators for contributions to affordability, quality, and experience for the
Demonstration model, the region and KP-wide, by June 1, 2013
• Show your Demonstration is on a trajectory to hit your end-of-year Demonstration targets by June 1, 2013.
Show your Demonstration is on a trajectory to hit your regional targets by December 31, 2013
• Be prepared to share learning and progress toward objectives on a quarterly basis beginning in December 2012

12/11/2012
18
MEDICARE CARE DELIVERY STRATEGY
E4 = LEARNING + ACCELERATION
35
• Clinical Disciplines
• Business Disciplines
• Internal KP Accelerators
• Segmentation
• First 5
• Variation
• Demonstrations
• Technology
• Nursing, Pharmacy, P&S, etc
• Internal Communications
• External Communications
• CMS Advocacy
• Publication
• External Relationships
• Scanning
• Strategic Planning
• Opportunity Analysis
• Generative Events
• Leadership Dashboard ENVISION
Explore what’s possible?
Create roadmap amidst the
possibilities
EXCITE
Activate the organization
Articulate vision and how we are getting there
solve and plan execution
ENGAGE
Develop key partners
Create opportunities to problem solve and plan execution
EEXECUTE
Test hypotheses,
identify what works, and go
to scale
Member Voice
And
Experience
Engage the Whole Organization
Jann’s star clusters here


















