QIA REVIEW SESSION: BASIC SCIENCE IN APHERESIS · PDF fileQIA REVIEW SESSION: BASIC SCIENCE IN...
46
QIA REVIEW SESSION: BASIC SCIENCE IN APHERESIS Nicole Aqui, M.D. Chief, Transfusion and Apheresis Services Division of Transfusion Medicine Department of Pathology and Laboratory Medicine University of Pennsylvania
Transcript of QIA REVIEW SESSION: BASIC SCIENCE IN APHERESIS · PDF fileQIA REVIEW SESSION: BASIC SCIENCE IN...

QIA REVIEW SESSION: BASIC SCIENCE IN APHERESIS Nicole Aqui, M.D. Chief, Transfusion and Apheresis Services Division of Transfusion Medicine Department of Pathology and Laboratory Medicine University of Pennsylvania

Disclosure • No relevant conflicts.

Outline • Immunohematology/Genetics
• ABO • Blood component therapy
• Immunology • HLA • Antibodies • Antibody-mediated diseases
• Apheresis

Immunohematology/Genetics: ABO
Adapted from U.S. National Library of Medicine

A and B Antigens • Carbohydrates antigens • On RBC membrane and secreted GPs • Copies per RBC
• A1 800,000 – 1,170,00 • A2 240,000 – 290,00 • B 610,00 – 830,00

ABO Antigen Structure
Gal GlcNAc
Gal
Fuc
Gal
Gal-NAc
Gal GlcNAc
Gal
Fuc
Gal GlcNAc
Gal
Fuc
transferase
A
B
H Antigen (O) A Antigen
B Antigen

A and B Antibodies • IgM • Naturally occurring
• Exposure to bacteria • Detected in the first months of life
• 95% have isohemagglutinin by 1 yr age • Anti-A,B is IgG found in type O

ABO Summary of Antigen/Antibody

Why do we bother with ABO typing?
End Organ Damage

Immunohematology/Genetics: ABO
Hemolysis

ABO Frequency and Compatibility
+ - - + 41 A,O A, AB
- + + - 10 B,O B, AB
+ + - - 4 All AB
- - + + 45 O All AB
A B
O
α-A
A1
Freq (%) Comp RBCs
Comp Plasma
Reagent anti-sera
Reagent red cells

Measurement of Agglutination

Distribution in different populations

Immunohematology/Genetics: Blood Component Therapy

Blood Component Therapy Component Storage
Temp/Shelf Life Vol Indication
Whole blood 2-6oC / 35 days
500 ml Acute hypovolemic anemia, exchange transfusions
Packed red cells 2-6oC / 35 - 42 days
250 - 300 ml
Symptomatic anemia
Single donor platelets
20-24oC / 5 days
150 - 300 ml
Bleeding due to thrombocytopenia or platelet defects
Fresh frozen plasma
-18oC / 12 months
250 ml Replacement of multiple coagulation factors, DIC, TTP, warfarin reversal
Cryoprecipitate -18oC / 12 months
5 - 10 ml Replacement of fibrinogen, FVIII, vWF
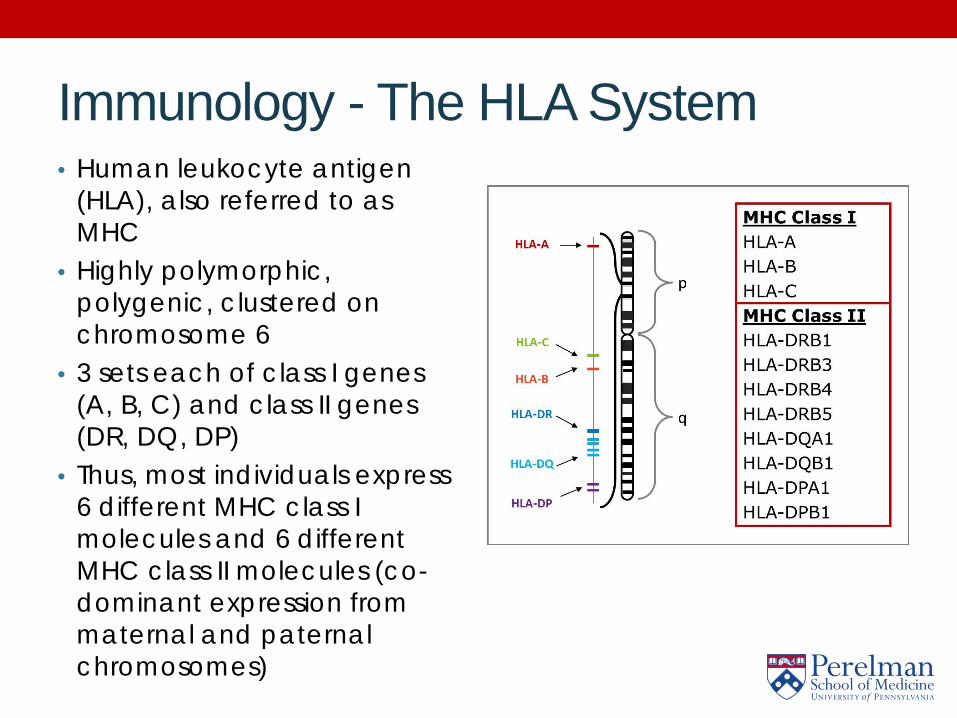
Immunology - The HLA System • Human leukocyte antigen
(HLA), also referred to as MHC
• Highly polymorphic, polygenic, clustered on chromosome 6
• 3 sets each of class I genes (A, B, C) and class II genes (DR, DQ, DP)
• Thus, most individuals express 6 different MHC class I molecules and 6 different MHC class II molecules (co-dominant expression from maternal and paternal chromosomes)
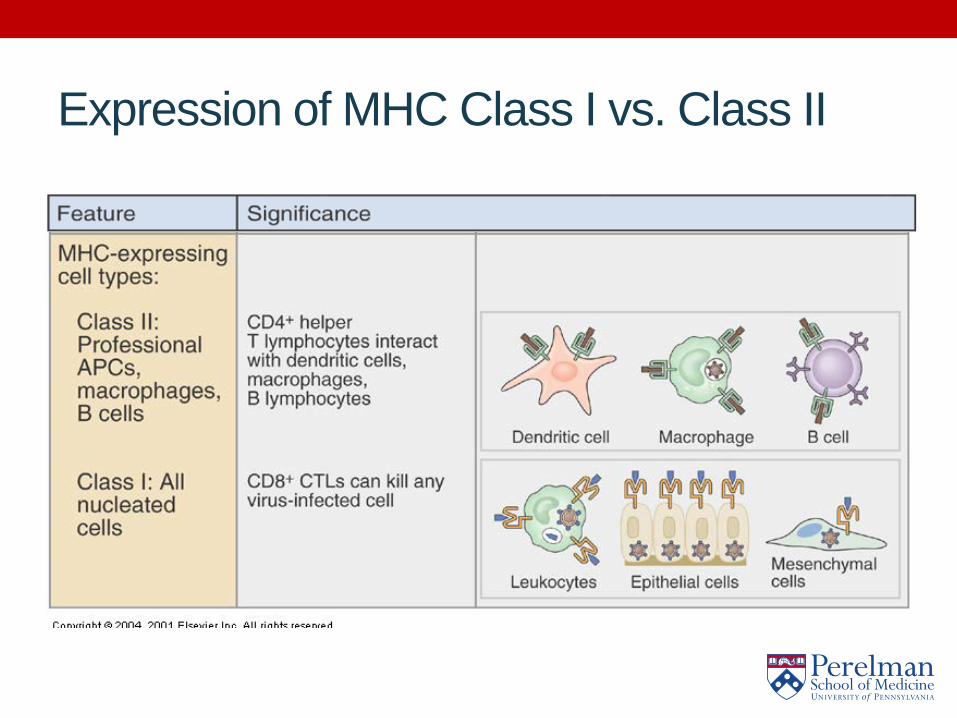
Expression of MHC Class I vs. Class II
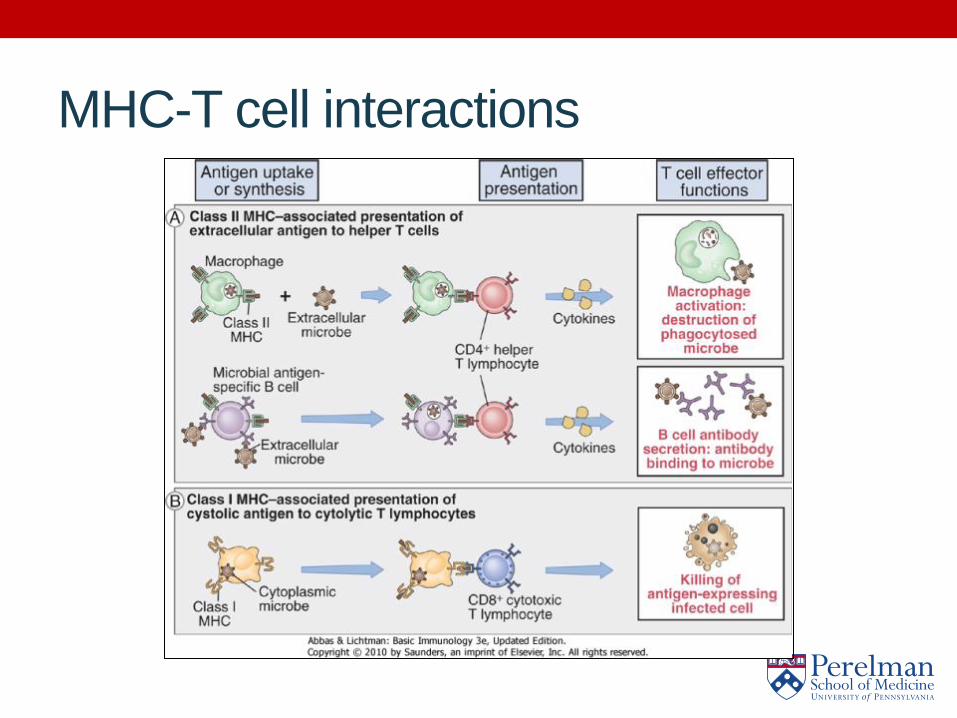
MHC-T cell interactions

T cell activation requires 2 signals
TCR
CD40L CD40
Antigen
MHC Class II CD4+
T cell
Dendritic cell

T cell responses are restricted
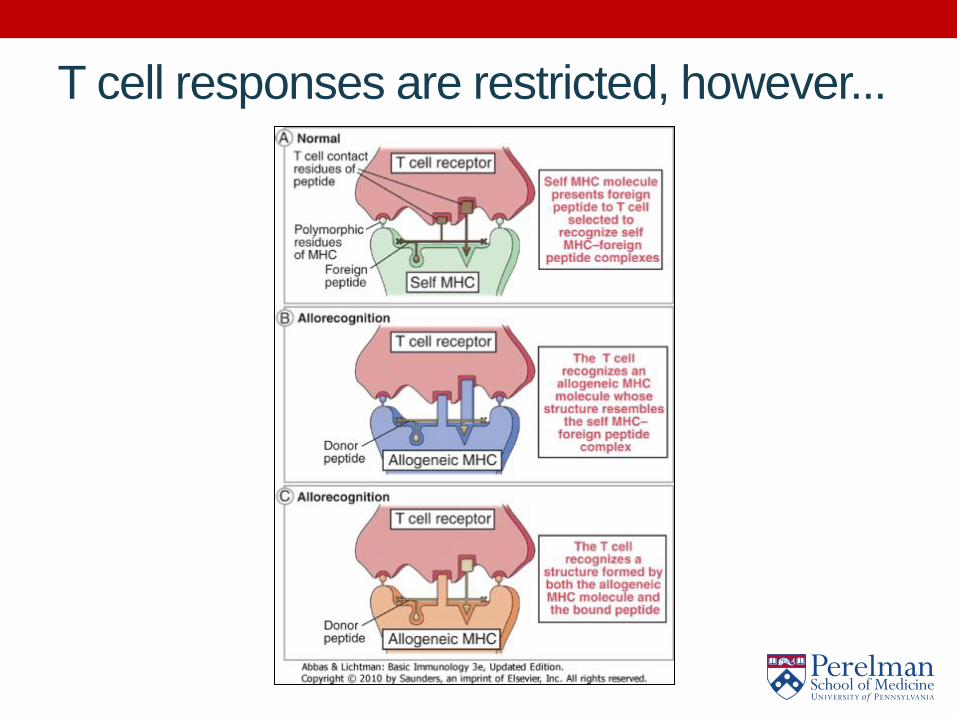
T cell responses are restricted, however...

Mechanisms of Allorecognition

Immunology - Antibodies

Antibody Functions

Mechanisms Antibody-Mediated Diseases
Examples of Antibody-Mediated Diseases • Myasthenia gravis • Guillain-Barre syndrome • Chronic inflammatory demyelinating polyneuropathy
(CIDP) • Goodpasture’s syndrome • Transplant rejection

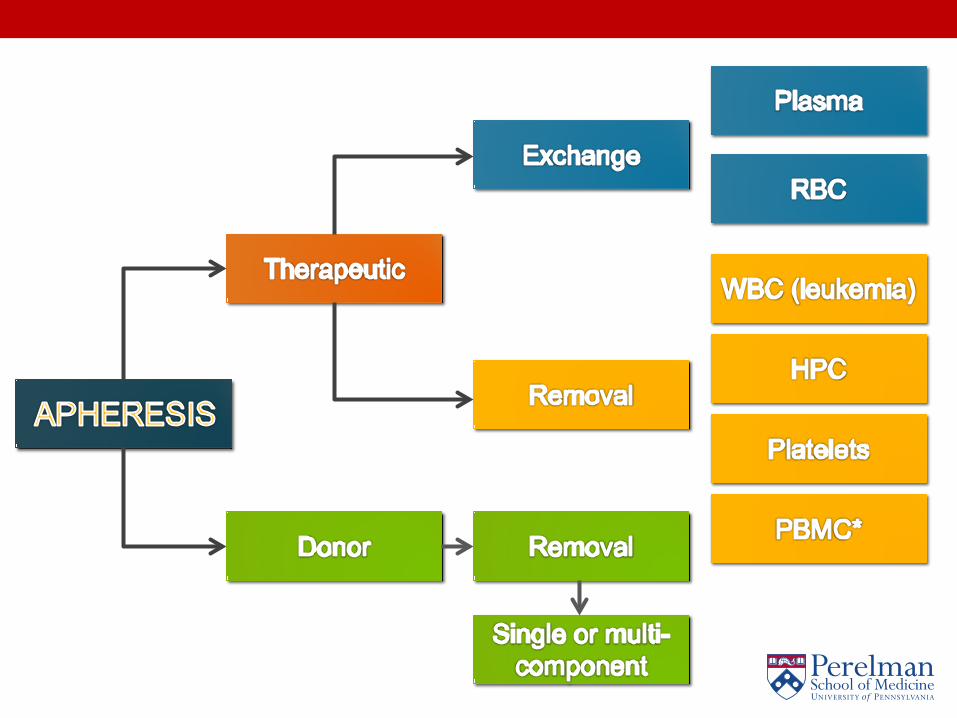
FINALLY - Apheresis • Apheresis is Greek for “to take away” or “subtract” • In hemapheresis we take away part of the blood
• Plasmapheresis – remove plasma • Leukopheresis – remove white blood cells • Erythropheresis – remove red blood cells • Plateletpheresis – remove platelets
• Originally performed discontinuously • Now performed with continuous removal and
separation of blood components
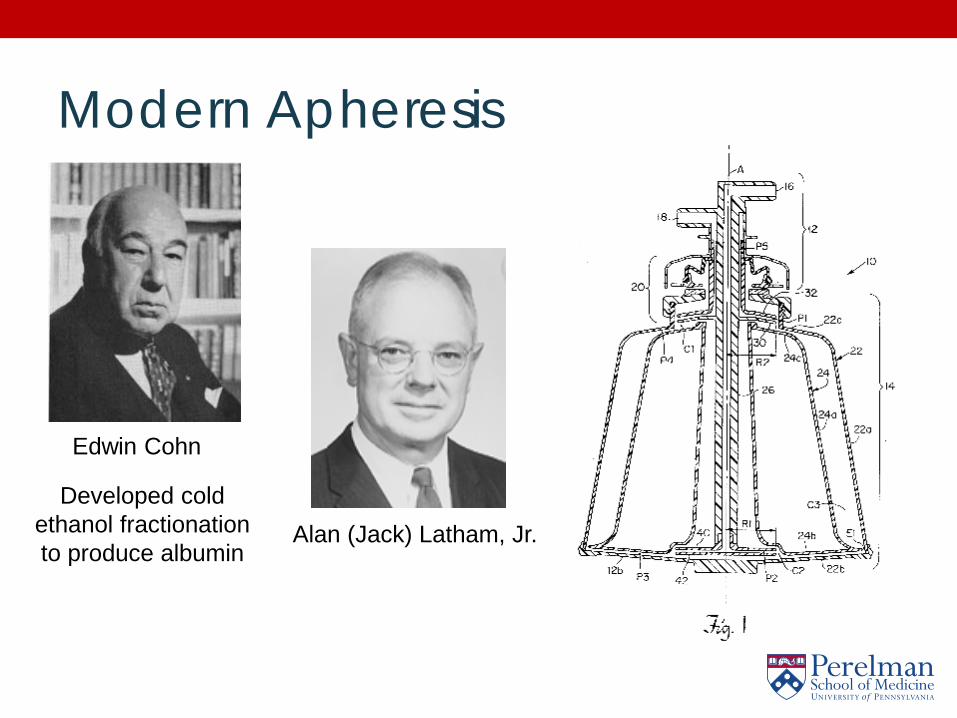
Modern Apheresis
Alan (Jack) Latham, Jr.
Edwin Cohn
Developed cold ethanol fractionation to produce albumin

Methods of Separation • Centrifugation • Membrane Filtration

Methods of Separation: Centrifugation

Methods of Separation: Membrane Filtration
Outline of an Apheresis Procedure • IV access obtained (single vs. double needle) • Drawn blood is anticoagulated (citrate or heparin)
prior to entry into separator • Anticoagulated blood is pumped into bowl/belt
chamber • Blood components are separated by density and
desired component is removed • Remaining blood is returned, mixed with
replacement fluid if required.

Plasma Exchange Circuit

Centrifugation vs. Filtration
Centrifugation
• Low blood flow rate • Citrate • Special equipment, but
more versatile
Filtration
• High blood flow rate • Heparin • Existing dialysis
machines • Simpler • Limited to plasma
exchange
Replacement Fluid in Plasma Exchange • Cystalloid (normal saline)
• Cheap • Hypo-oncotic • No coagulation factors or immunoglobulins
• Colloid (albumin) • EXPENSIVE • Slightly hyper-oncotic, can result in volume expansion • Very low risk of infectious disease transmission • No coagulation factors or immunoglobulins
• Plasma • Cheaper than albumin • Iso-oncotic • Associated risks of all blood product transfusions (infectious
disease, allergic reactions, TRALI)

Selective removal/adsorption column • Plasma separated by centrifugation or filtration • Passed over a selective column/filter
• LDL Apheresis: dextran sulfate column

Plasma Line
LIPOSORBER® Column
Plasma Pump
LIPOSORBER® SYSTEM
Blood Pump
Heparin Pump
Blood Return
Plasma Separator
Regeneration Pump
Re-Priming Solution
Regeneration Solution
Waste Line
Kanaka Pharma America Corporation

Effects of Plasma Exchange
From McLeod; Apheresis: Principals and Practice (2003)
• Dose = Plasma volume (PV) • PV = BV x (1-Hct) = (70ml/kg x Wt) x (1-Hct) • 1 PV = ~60% removal • No benefit in exchanging > 2
PV

Alteration in Blood Constituents
From McLeod; Apheresis: Principals and Practice (2003)
Constituent Percent Decrease from Baseline
Percent Recovered at 48 Hours
Clotting factors 25 – 50 80 – 100
Fibrinogen 63 65
Immunoglobulins 63 ~45
Paraproteins 33 – 60 Variable
Liver enzymes 55 – 60 100
Bilirubin 45 100
C3 63 60 – 100
Platelets 25 – 30 75 – 100
Removal of Drugs • In general, drugs with a low volume of distribution
(Vd) and/or a high rate of protein binding are most likely to be removed during plasma exchange • Cisplatin • Vincristine • Propanolol • Gentamycin • Vancomycin • Rituximab • IVIG
Pharmacotherapy 2007;27(11):1529–1549

Adverse Reactions • Vascular Access
• Hematoma • Clotting of line • Insufficient for pressures required
• Central line • Fistula • Graft
• Infection • More problematic with central lines than with
anticubital access
Adverse Reactions • Vaso-vagal reactions
• Pallor • Hypotension • Diaphoresis • Bradycardia • Nausea/vomiting
• More common with plasmapheresis than with cytapheresis
• ACE inhibitors exacerbate

Adverse Reactions • Citrate toxicity
• Temporary decrease in Cai2+
• Tingling, numbness, nausea • Calcium supplementation: calcium carbonate, calcium
gluconate, calcium chloride • Coagulation alterations
• Daily TPE without plasma replacement can deplete coagulation factors and increase bleeding
• Consider FFP replacement with daily exchange and in patients with coagulation abnormalities
• Monitor fibrinogen

Summary • ABO is the most important blood antigen group. • The HLA system is complex, highly polymorphic and
polygenic. • Antibodies have several protective functions, but
can also cause disease. • It is important for the apheresis operator to have an
understanding of basic transfusion medicine, as well as immunology and the mechanisms underlying broad categories of disease.

Acknowledgments UPENN Transfusion Medicine Faculty • Don Siegel, MD PhD • Una O’Doherty, MD PhD • Taku Kambayashi, MD PhD • Vijay Bhoj, MD PhD • Andrew Fesnak, MD PhD • Carl June, MD • Bruce Levine, PhD
UPENN Apheresis Staff • Leah Irwin, Nurse Manager • Lita Jamensky • Caitlin Cahill • Melissa Murter • Jane Mason • Jennifer Green • Marcia Hole • Kevin Schell • Jennifer Schwartz • Julie Colanero • Kelli Hines • Colleen Henry