PVK WGMIRGI 1 viexqirx Viwtsrwiw mr WHL1hiÄgmirx KMW;
24
LRG SCIENCE - Treatment Responses in SDH-deficient GIST ABSTRACT Background The behavior of Succinate Dehydrogenase-Deficient Gastrointestinal Stromal Tumor (SDH-deficient GIST) can vary from extended periods of stability to rapidly progressive disease. This variable behavior combined with the rarity of the disease and the sparsity of objective responses to treatments makes the evaluation of treatments extremely difficult. In addition, many KIT/PDGFRA wildtype GIST patients were diagnosed in the era before SDH immunohistochemistry testing was common, resulting in a significant number of patients who today lack a definitive diagnosis but who are likely SDH-deficient. Methods In this retrospective cohort study of 1709 GIST patients from The Life Raft Group (LRG) Patient Registry, patients were classified into four study groups: • Known SDH-deficient (Known) • Likely SDH-deficient (Likely) • Combined Known and Likely SDH-deficient groups (Combined) • All other patients (All Others) The Likely group was defined using previously reported characteristics of known SDH-deficient patients and refined using supporting LRG data. Patient-reported outcomes were examined. Results No significant differences were observed between the Known and Likely groups in self-reported progression- free survival (srPFS) from first line (1L) through fourth line (4L) or overall survival (OS) from 1L through 4L or OS from the time of diagnosis. For the Combined group the median srPFS times for first line (1L) imatinib (n = 57), second line (2L) sunitinib (n = 42), and third line/ post-third line (3L+) regorafenib (n = 9) treatment were: 14.7 months (mo.), 18.0 mo., and 42.9 mo. respectively (p = 0.46). In a separate analysis, when all 1L (n = 57), 2L (n = 42) and 3L (n = 21) drugs were used, the median srPFS did not differ for the Combined group: 13.6 mo., 18.0 mo. and 19.1 mo. respectively (p = 0.7). The Combined group had a significant reduction in risk of death compared to the Corresponding author: Jerry W. Call, The Life Raft Group, 155 Route 46 West, Suite 202, Wayne, NJ 07470 Phone: 973-837-9092 Fax: 973-837-9095 Email: [email protected] Treatment Responses in SDH-deficient GIST Patient-reported Treatment Responses in Known/Likely SDH-deficient GISTS: An Analysis of The Life Raft Group Observational Registry Jerry W. Call 1 , Yu Wang 1 , Sara Rothschild 1 , Denisse Montoya 1 , Pete Knox 1 , Mary Garland 1 , Carolyn Tordella 1 , Norman J. Scherzer 1 1 The Life Raft Group, Wayne, NJ AUGUST 2019 This study, directed by LRG Data Analyst Jerry Call and the Real World Evidence team, provides an innovative workaround to address the issue of limited patient data for a rare subtype of a rare cancer called GIST, namely those with SDH-deficiency. The number of patients who are definitively classified as SDH-deficient GIST based upon mutational testing is low, as there are many GIST patients who do not receive the further testing necessary to clearly identify or exclude them as SDH-deficient. By creating a “Likely SDH-deficient” group using an algorithm to sort the data available in the Life Raft Group Patient Registry, the number of patients available for analysis tripled. Although this is clearly not a substitute for the long-term solution of expanding mutational testing, it provides an immediate interim approach to exploring off-label treatment options and other important issues needed to help this important sub-group of patients, many of whom are quite young.
Transcript of PVK WGMIRGI 1 viexqirx Viwtsrwiw mr WHL1hiÄgmirx KMW;
LRG SCIENCE - Treatment Responses in SDH-deficient GIST
ABSTRACTBackgroundThe behavior of Succinate Dehydrogenase-Deficient Gastrointestinal Stromal Tumor (SDH-deficient GIST) can vary from extended periods of stability to rapidly progressive disease. This variable behavior combined with the rarity of the disease and the sparsity of objective responses to treatments makes the evaluation of treatments extremely difficult. In addition, many KIT/PDGFRA wildtype GIST patients were diagnosed in the era before SDH immunohistochemistry testing was common, resulting in a significant number of patients who today lack a definitive diagnosis but who are likely SDH-deficient.MethodsIn this retrospective cohort study of 1709 GIST patients from The Life Raft Group (LRG) Patient Registry, patients were classified into four study groups:
• Known SDH-deficient (Known)• Likely SDH-deficient (Likely)• Combined Known and Likely SDH-deficient groups
(Combined)• All other patients (All Others)
The Likely group was defined using previously reported characteristics of known SDH-deficient patients and refined using supporting LRG data. Patient-reported outcomes were examined. ResultsNo significant differences were observed between the Known and Likely groups in self-reported progression-free survival (srPFS) from first line (1L) through fourth line (4L) or overall survival (OS) from 1L through 4L or OS from the time of diagnosis. For the Combined group the median srPFS times for first line (1L) imatinib (n = 57), second line (2L) sunitinib (n = 42), and third line/post-third line (3L+) regorafenib (n = 9) treatment were: 14.7 months (mo.), 18.0 mo., and 42.9 mo. respectively (p = 0.46). In a separate analysis, when all 1L (n = 57), 2L (n = 42) and 3L (n = 21) drugs were used, the median srPFS did not differ for the Combined group: 13.6 mo., 18.0 mo. and 19.1 mo. respectively (p = 0.7). The Combined group had a significant reduction in risk of death compared to the
Corresponding author: Jerry W. Call, The Life Raft Group, 155 Route 46 West, Suite 202, Wayne, NJ 07470 Phone: 973-837-9092 Fax: 973-837-9095 Email: [email protected]
Treatment Responses in SDH-deficient GISTPatient-reported Treatment Responses in Known/Likely SDH-deficient GISTS: An Analysis of The Life Raft Group Observational RegistryJerry W. Call1, Yu Wang1, Sara Rothschild1, Denisse Montoya1, Pete Knox1, Mary Garland1, Carolyn Tordella1, Norman J. Scherzer1
1The Life Raft Group, Wayne, NJ
AUGUST 2019
This study, directed by LRG Data Analyst Jerry Call and the Real World Evidence team, provides an innovative workaround to address the issue of limited patient data for a rare subtype of a rare cancer called GIST, namely those with SDH-deficiency. The number of patients who are definitively classified as SDH-deficient GIST based upon mutational testing is low, as there are many GIST patients who do not receive the further testing necessary to clearly identify or exclude them as SDH-deficient. By creating a “Likely SDH-deficient” group using an algorithm to sort the data available in the Life Raft Group Patient Registry, the number of patients available for analysis tripled. Although this is clearly not a substitute for the long-term solution of expanding mutational testing, it provides an immediate interim approach to exploring off-label treatment options and other important issues needed to help this important sub-group of patients, many of whom are quite young.

2 3
LRG SCIENCE - Treatment Responses in SDH-deficient GIST
All Others group. The risk of death was reduced >60% (range 62% - 83%) from 1L (treatment for advanced GIST) through 4L (p value range <0.00001 – 0.007). ConclusionsThe rarity of SDH-deficient GIST, frequent periods of stability even when disease is present, combined with few objective responses to drugs makes it difficult to evaluate treatment efficacy. Criteria were developed to identify Likely patients, tripling the number of patients available for analysis. We were unable to detect any differences in srPFS or OS between the Known and Likely group, which supports the sensitivity of the categorization criteria and also supports combining these groups to create a larger group for comparisons. This analysis is one of the first to compare different treatments and to include comparison groups representative of more typical GISTs. The categorization criteria used here may also enable identification of Likely SDH-deficient patients currently diagnosed as KIT/PDGFRA wildtype who might benefit from further immunohistochemistry (IHC) and mutational testing.BACKGROUNDGastrointestinal stromal tumors (GISTs) are soft tissue sarcomas that arise from interstitial cells of Cajal (ICC) or from stem cells that differentiate towards ICC. Primary tumors most commonly occur in the stomach or small intestine with frequent metastases to the liver or peritoneum. GISTs went from obscurity to becoming well-known with the discovery of KIT as the most common driver mutation1 followed by the remarkable treatment response to imatinib2. Imatinib was one of the earliest and most successful tyrosine kinase inhibitors (TKIs) approved as a cancer treatment2, 3, 4. Approximately 75% to 80% of GISTs have activating mutations in KIT. In 2003, PDGFRA mutations were also discovered in GIST5,6. About 7%-16% of GIST patients have PDGFRA mutations7,8. The most common mutation is the D842V mutation in exon 18. This mutation is resistant to TKI’s currently approved for GIST. Other mutations in PDGFRA are generally imatinib-sensitive7. Effective D842V inhibitors are in late-phase clinical studies9,10. After the discovery of PDGFRA gene mutations in GIST, tumors without KIT or PDGFRA mutations were commonly referred to as Wildtype (WT) GIST. A more accurate, preferred term is KIT/PDGFRA WT. Approximately 15% of GIST patients are KIT/PDGFRA WT. In 2007, succinate dehydrogenase (SDHB, SDHC, and SDHD) mutations were discovered in GISTs11. Mutations were subsequently found in SDHA12. In 2014, epigenetic changes affecting SDHC without a detectable mutation were identified13. This latter type of GIST is called SDHC-epimutant GIST. All of these defects result in loss of function/deficiency in the succinate dehydrogenase protein and all result in loss of expression of SDHB which can be seen via immunohistochemistry (IHC staining). Thus, deficiency in succinate dehydrogenase, a tumor-
suppressor protein, is the common element bringing together not only these genetic defects, but previously described syndromes including; pediatric GIST, Carney Triad, and Carney-Stratakis syndrome. Unlike KIT/PDGFRA mutant GIST, SDH-deficient GIST has a major hereditary component with frequent germline mutations. Both germline mutant and epimutant SDH-deficient GIST patients are at risk for other tumor types such as paragangliomas and chondromas and have different monitoring requirements. Families of patients with germline mutant SDH-deficient GIST are also advised to seek genetic counseling.The frequency of SDH-deficient GIST is somewhat difficult to determine due to incomplete testing in the general GIST population. Thus far, the largest SDH-deficiency study in GISTs, including 1134 cases, identified 66 (5.8%) SDH-deficient cases14. In this study, all 66 SDH-deficient cases were gastric GISTs and made up 8.7% of the gastric GISTs (7.5% of unselected cases).SDH-deficient GIST is the most common type of GIST in younger patients making up almost all GISTs diagnosed below the age of 20 and a significant percentage of those diagnosed below the age of 4014. It occurs more frequently in females. Metastases to the liver are common and patients frequently live many years with active disease14. Response of known and likely SDH-deficient patients to TKI’s has generally been characterized as poor. As an example of response to TKI’s, the National Institutes of Health’s Wildtype and Pediatric GIST clinic (est. 2008) has reported that only 1 of 49 SDH-deficient GIST patients treated with imatinib had a documented objective response (2%). Response to sunitinib was higher with 7 of 38 patients (18%) having an objective response (1 complete, 3 partial, and 3 mixed, defined as regression at some sites and progression at others). According to the authors in this observational study, “stable disease was difficult to ascribe to treatment because protracted periods of stable disease also occurred in untreated patients”15.In another retrospective study of 9 pediatric/young adult GIST patients (age 11-21) treated with sunitinib, the best response was stable disease lasting from 1 to > 73 months with a median progression-free survival time of 15 months16. A third report of response to sunitinib from 7 Likely patients was reported from a treatment use protocol for patients that were 10-17 years old at enrollment. In this study, 1 patient had a partial response (14%), 1 had progressive disease (14%) and 5 had disease stability (72%) lasting from 7 to 21+ months with a mean of 15 months. Time to tumor progression was longer on sunitinib than on prior imatinib for five of six patients17.METHODSThe Life Raft Group (LRG) is an international non-profit medical research and advocacy organization. The LRG
2 3
LRG SCIENCE - Treatment Responses in SDH-deficient GIST
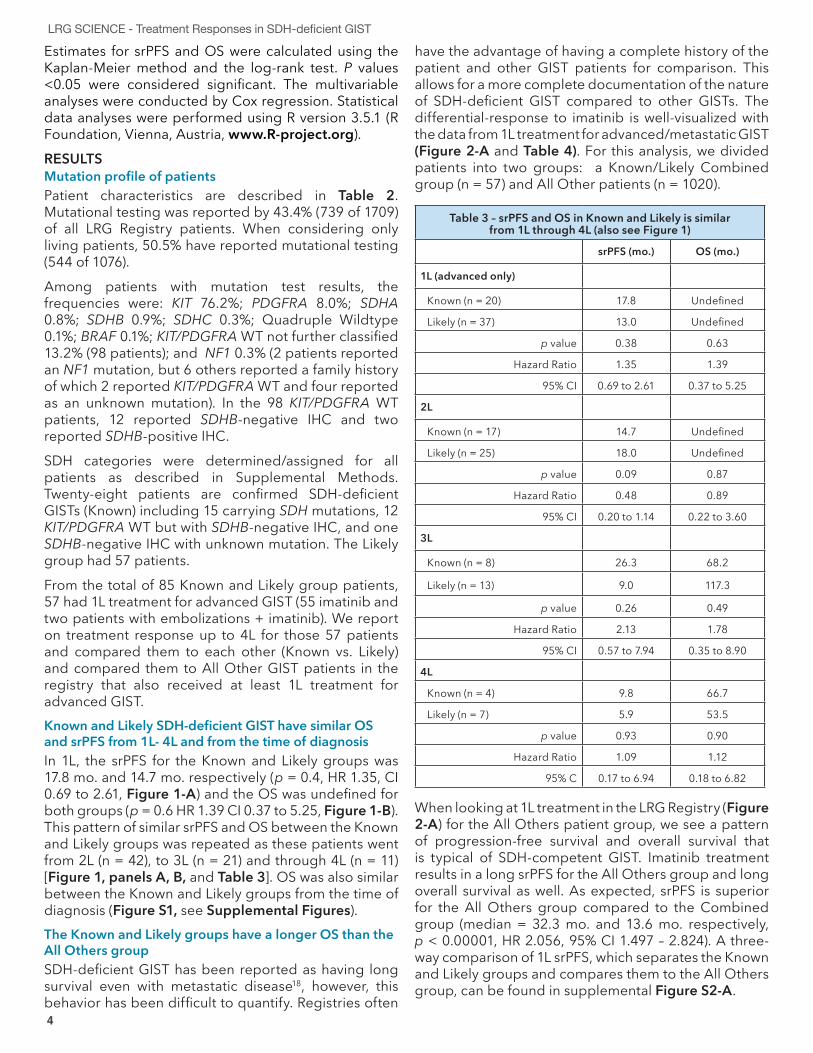
Patient Registry included 1709 GIST patients at the time of data cutoff (4/17/2017). This is a retrospective analysis of a long-term observational study of those patients.Since the total number of known SDH-deficient patients is small, we wanted to know if it was reasonable to use likely SDH-deficient patients in order to triple the number of treatments available for analysis. Patients with any reported SDH mutation or with a negative SDHB stain on IHC were considered to be Known SDH-deficient. To create a Likely category, we used a combination of previously reported criteria typical of SDH-deficient GIST and supportive data from the LRG Registry to predict their SDH status, which tripled the number of cases available for analysis. This prediction might include some non-SDH-deficient patients; however, it is more likely to exclude some SDH-deficient patients (it is predicted to have better sensitivity than specificity). We then compared Known group patients to Likely group patients to see if they had similar treatment responses and survival. To do that, for patients that received treatment for advanced GIST, we compared self-reported progression-free survival (srPFS) and Overall Survival (OS) for Known and Likely in 1st line (1L, n = 57) through 4th (4L, n = 11) lines of treatment. We also compared OS from the time of diagnosis for all Known (n = 28) and Likely patients (n = 57), including those that did not receive TKI treatment. Once satisfied that the Likely group was comparable to the Known group, we combined the Known and Likely groups into a Known/Likely combined group (Combined) for further analyses. This provided greater numbers for drug response analyses and provided better visualization of the differences in OS compared to the All Others group.
Table 1 - SDH category criteria
Description #Pts Criteria
Known 28 Negative SDHB stain and/or known SDHx mutation
Likely 57 Stomach Primary Tumor and• < 18 at diagnosis• KIT/PDGFRA WT, 18 - 35 at diagnosis,
female• KIT/PDGFRA WT, age 35 - 40 at diagnosis,
multi-focal primary• Unknown mutation, 18 - 35 at diagnosis,
multi-focal primary• Diagnosis of Carney Triad (that did not fit
criteria above) - Report of a paraganglioma and/or
chondroma was supportive of Carney Triad
All Others 1623 All other patients
1709 Total patients in The LRG Registry
The Known (n = 28) and Likely (n = 57) were 2 of 7 groups as described briefly in Table 1 above and in detail in Supplemental Methods. The other 5 categories
were combined into 1 category called All Others (n = 1623) total patients and n = 1020 receiving 1L TKI treatment for advanced GIST). Although the All Others group will have some SDH-deficient patients due to both incomplete mutational testing and less than 100% specificity of our categorization algorithm, it can generally be thought of as non-SDH-deficient GIST (or SDH-competent GIST).
Table 2 - Patient characteristics
Known Likely Combined All Others Total
Patients (n) 28 57 85 1624 1709
Alive 25 (89.3%) 49 (86.0%) 74 (87.1%) 1002 (61.7%)
1076 (63.0%)
Dead 3 (10.7%) 8 (14.0%) 11 (12.9%) 622 (38.3%) 633 (37%)
Female 20 (71.4%) 47 (82.5%) 67 (78.8%) 790 (48.6%) 857 (50.1%)
Male 8 (28.6%) 10 (17.5%) 18 (21.2%) 834 (51.4%) 852 (49.9%)
Age at Diagnosis
Median/ Range
23.9 (7-62)
17.7 (5-41)
21.0 (5-62)
53.1 (10-92)
52.4 (5-92)
<18 8 (28.6%) 30 (52.6%) 38 (44.7%) 3 (0.2%) 41 (2.4%)
≥18-35 12 (42.9%) 23 (40.4%) 35 (41.2%) 130 (8.0%) 165 (9.7%)
≥35 8 (28.6%) 4 (7.0%) 12 (14.1%) 1485 (91.4%)
1497 (87.6%)
Unknown - - - 6 (0.4%) 6 (0.4%)
Follow-up (median) 8.2 yrs 10.5 yrs 9.7 yrs 8.7 yrs 8.8 yrs
Mutations
KIT - - - 563 (34.7%) 563 (32.9%)
PDGFRA - - - 59 (3.6%) 59 (3.5%)
WT for KIT/PDGFRA 12 (42.9%) 36 (63.2%) 48 (56.5%) 50 (3.1%) 98 (5.7%)
SDHA 6 (21.4%) 6 (7.1%) - 6 (0.4%)
SDHB 7 (25.0%) - 7 (8.2%) - 7 (0.4%)
SDHC 2 (7.1%) - 2 (2.4%) - 2 (0.1%)
BRAF - - 1 (0.1%) 1 (0.1%)
NF1 - - - 2 (0.1%) 2 (0.1%)
Quadruple Wildtype - - - 1 (0.1%) 1 (0.1%)
Unknown 1 (3.6%) 21 (36.8%) 22 (25.9%) 948 (58.4%) 970 (56.8%)
Primary Tumor
Stomach 27 (96.4%) 57 (100%) 84 (98.8%) 663 (40.8%)
Small Intestine 1 (3.6%) - 1 (1.2%) 620 (38.3%)
Rectum/Anus 53 (3.3%)
Colon 48 (3.0%)
Unknown 109 (6.4%)
Other 131 (8.1%)
Total 28 (1.6%) 57 (3.3%) 85 (5.0%) 1624 (95.0%)
1709 (100.0%)
4 5
LRG SCIENCE - Treatment Responses in SDH-deficient GIST
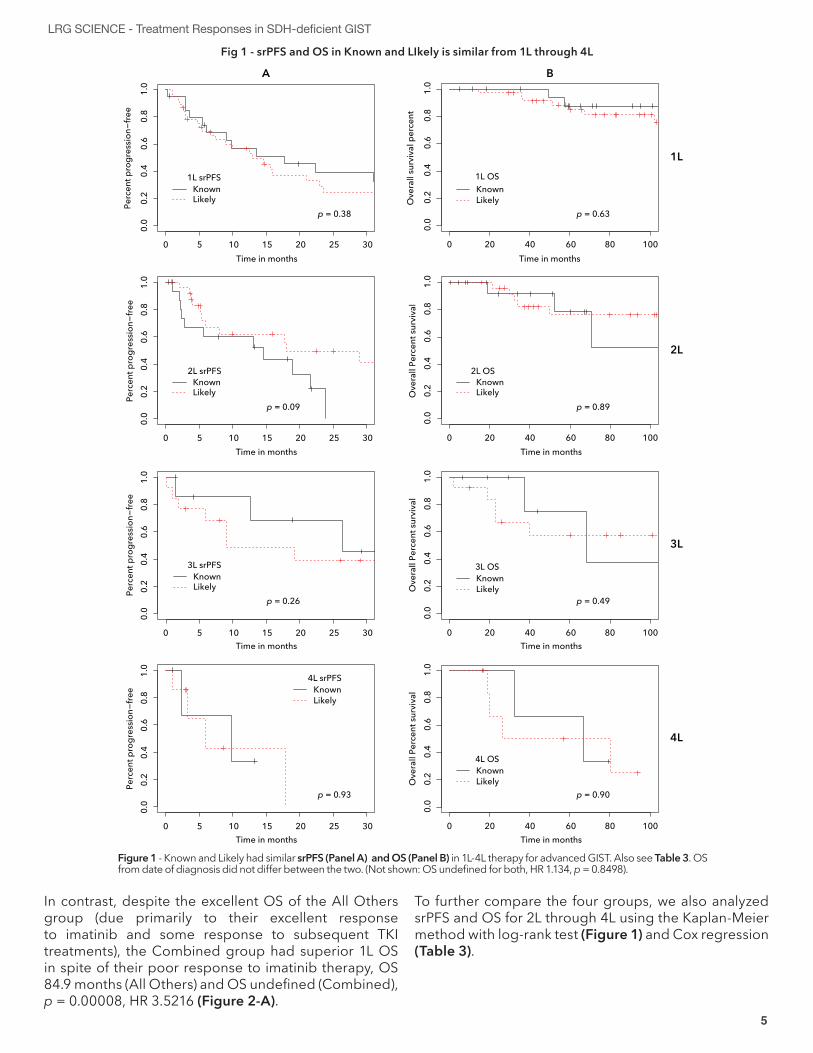
Estimates for srPFS and OS were calculated using the Kaplan-Meier method and the log-rank test. P values <0.05 were considered significant. The multivariable analyses were conducted by Cox regression. Statistical data analyses were performed using R version 3.5.1 (R Foundation, Vienna, Austria, www.R-project.org).RESULTSMutation profile of patientsPatient characteristics are described in Table 2. Mutational testing was reported by 43.4% (739 of 1709) of all LRG Registry patients. When considering only living patients, 50.5% have reported mutational testing (544 of 1076). Among patients with mutation test results, the frequencies were: KIT 76.2%; PDGFRA 8.0%; SDHA 0.8%; SDHB 0.9%; SDHC 0.3%; Quadruple Wildtype 0.1%; BRAF 0.1%; KIT/PDGFRA WT not further classified 13.2% (98 patients); and NF1 0.3% (2 patients reported an NF1 mutation, but 6 others reported a family history of which 2 reported KIT/PDGFRA WT and four reported as an unknown mutation). In the 98 KIT/PDGFRA WT patients, 12 reported SDHB-negative IHC and two reported SDHB-positive IHC. SDH categories were determined/assigned for all patients as described in Supplemental Methods. Twenty-eight patients are confirmed SDH-deficient GISTs (Known) including 15 carrying SDH mutations, 12 KIT/PDGFRA WT but with SDHB-negative IHC, and one SDHB-negative IHC with unknown mutation. The Likely group had 57 patients.From the total of 85 Known and Likely group patients, 57 had 1L treatment for advanced GIST (55 imatinib and two patients with embolizations + imatinib). We report on treatment response up to 4L for those 57 patients and compared them to each other (Known vs. Likely) and compared them to All Other GIST patients in the registry that also received at least 1L treatment for advanced GIST.Known and Likely SDH-deficient GIST have similar OS and srPFS from 1L- 4L and from the time of diagnosisIn 1L, the srPFS for the Known and Likely groups was 17.8 mo. and 14.7 mo. respectively (p = 0.4, HR 1.35, CI 0.69 to 2.61, Figure 1-A) and the OS was undefined for both groups (p = 0.6 HR 1.39 CI 0.37 to 5.25, Figure 1-B). This pattern of similar srPFS and OS between the Known and Likely groups was repeated as these patients went from 2L (n = 42), to 3L (n = 21) and through 4L (n = 11) [Figure 1, panels A, B, and Table 3]. OS was also similar between the Known and Likely groups from the time of diagnosis (Figure S1, see Supplemental Figures).The Known and Likely groups have a longer OS than the All Others group SDH-deficient GIST has been reported as having long survival even with metastatic disease18, however, this behavior has been difficult to quantify. Registries often
have the advantage of having a complete history of the patient and other GIST patients for comparison. This allows for a more complete documentation of the nature of SDH-deficient GIST compared to other GISTs. The differential-response to imatinib is well-visualized with the data from 1L treatment for advanced/metastatic GIST (Figure 2-A and Table 4). For this analysis, we divided patients into two groups: a Known/Likely Combined group (n = 57) and All Other patients (n = 1020).
Table 3 – srPFS and OS in Known and Likely is similar from 1L through 4L (also see Figure 1)
srPFS (mo.) OS (mo.)
1L (advanced only)
Known (n = 20) 17.8 Undefined
Likely (n = 37) 13.0 Undefined
p value 0.38 0.63
Hazard Ratio 1.35 1.39
95% CI 0.69 to 2.61 0.37 to 5.25
2L
Known (n = 17) 14.7 Undefined
Likely (n = 25) 18.0 Undefined
p value 0.09 0.87
Hazard Ratio 0.48 0.89
95% CI 0.20 to 1.14 0.22 to 3.60
3L
Known (n = 8) 26.3 68.2
Likely (n = 13) 9.0 117.3
p value 0.26 0.49
Hazard Ratio 2.13 1.78
95% CI 0.57 to 7.94 0.35 to 8.90
4L
Known (n = 4) 9.8 66.7
Likely (n = 7) 5.9 53.5
p value 0.93 0.90
Hazard Ratio 1.09 1.12
95% C 0.17 to 6.94 0.18 to 6.82
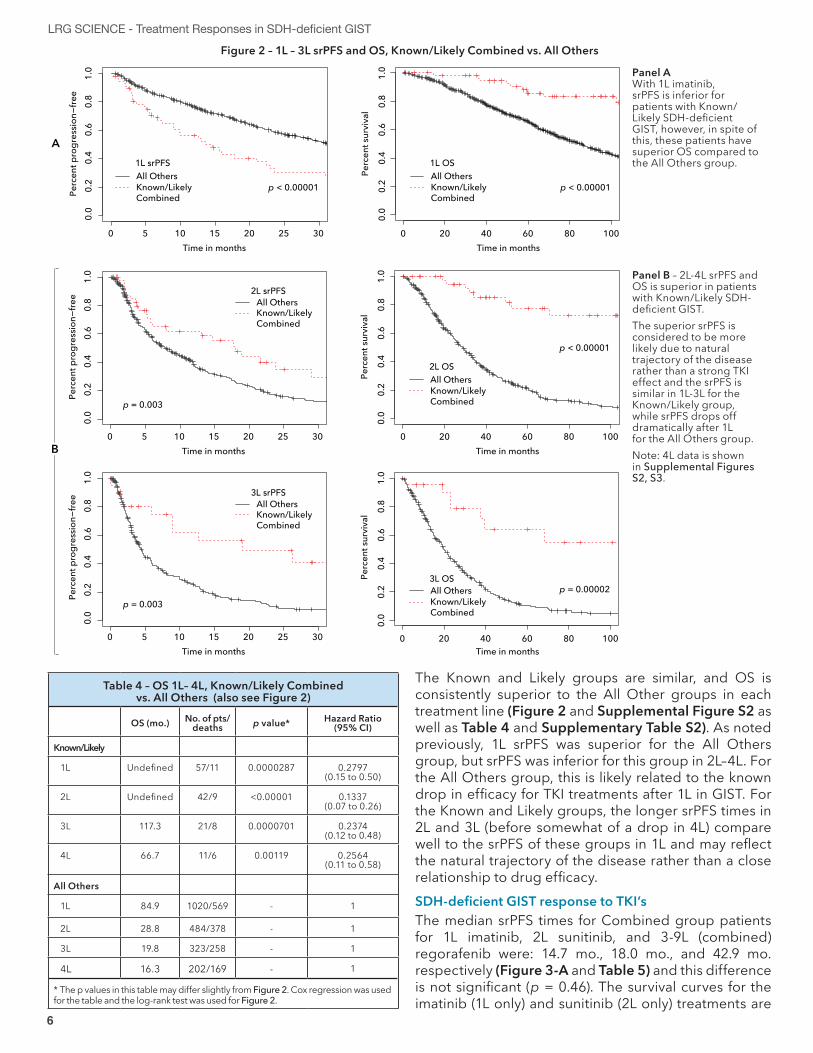
When looking at 1L treatment in the LRG Registry (Figure 2-A) for the All Others patient group, we see a pattern of progression-free survival and overall survival that is typical of SDH-competent GIST. Imatinib treatment results in a long srPFS for the All Others group and long overall survival as well. As expected, srPFS is superior for the All Others group compared to the Combined group (median = 32.3 mo. and 13.6 mo. respectively, p < 0.00001, HR 2.056, 95% CI 1.497 – 2.824). A three-way comparison of 1L srPFS, which separates the Known and Likely groups and compares them to the All Others group, can be found in supplemental Figure S2-A.
4 5
LRG SCIENCE - Treatment Responses in SDH-deficient GIST
In contrast, despite the excellent OS of the All Others group (due primarily to their excellent response to imatinib and some response to subsequent TKI treatments), the Combined group had superior 1L OS in spite of their poor response to imatinib therapy, OS 84.9 months (All Others) and OS undefined (Combined), p = 0.00008, HR 3.5216 (Figure 2-A).
To further compare the four groups, we also analyzed srPFS and OS for 2L through 4L using the Kaplan-Meier method with log-rank test (Figure 1) and Cox regression (Table 3).
Fig 1 - srPFS and OS in Known and LIkely is similar from 1L through 4L
1050 15 20 25 30
0.0
0.2
0.4
0.6
0.8
1.0
Time in months
Perc
ent p
rogr
essio
n−fre
e
Time in months
Ove
rall
surv
ival
per
cent
1000 20 40 60 80
0.0
0.2
0.4
0.6
0.8
1.0
1050 15 20 25 30
0.0
0.2
0.4
0.6
0.8
1.0
1000 20 40 60 800.
00.
20.
40.
60.
81.
0
1050 15 20 25 30
0.0
0.2
0.4
0.6
0.8
1.0
1000 20 40 60 80
0.0
0.2
0.4
0.6
0.8
1.0
1050 15 20 25 30
0.0
0.2
0.4
0.6
0.8
1.0
1000 20 40 60 80
0.0
0.2
0.4
0.6
0.8
1.0
A
1L srPFSKnownLikely
p = 0.38
2L srPFSKnownLikely
p = 0.09
Time in months
Perc
ent p
rogr
essio
n−fre
e
2L
3L srPFSKnownLikely
p = 0.26
Time in months
Perc
ent p
rogr
essio
n−fre
e
3L
4L srPFSKnownLikely
p = 0.93
Time in months
Perc
ent p
rogr
essio
n−fre
e
4L
B
Time in months
Time in months
Time in months
Ove
rall
Perc
ent s
urvi
val
Ove
rall
Perc
ent s
urvi
val
Ove
rall
Perc
ent s
urvi
val
1L1L OSKnownLikely
p = 0.63
3L OSKnownLikely
p = 0.49
4L OSKnownLikely
p = 0.90
2L OSKnownLikely
p = 0.89
Figure 1 - Known and Likely had similar srPFS (Panel A) and OS (Panel B) in 1L-4L therapy for advanced GIST. Also see Table 3. OS from date of diagnosis did not differ between the two. (Not shown: OS undefined for both, HR 1.134, p = 0.8498).
6 7
LRG SCIENCE - Treatment Responses in SDH-deficient GIST
Table 4 – OS 1L– 4L, Known/Likely Combined vs. All Others (also see Figure 2)
OS (mo.) No. of pts/deaths p value* Hazard Ratio
(95% CI)
Known/Likely
1L Undefined 57/11 0.0000287 0.2797 (0.15 to 0.50)
2L Undefined 42/9 <0.00001 0.1337 (0.07 to 0.26)
3L 117.3 21/8 0.0000701 0.2374 (0.12 to 0.48)
4L 66.7 11/6 0.00119 0.2564 (0.11 to 0.58)
All Others
1L 84.9 1020/569 - 1
2L 28.8 484/378 - 1
3L 19.8 323/258 - 1
4L 16.3 202/169 - 1
* The p values in this table may differ slightly from Figure 2. Cox regression was used for the table and the log-rank test was used for Figure 2.
Figure 2 – 1L – 3L srPFS and OS, Known/Likely Combined vs. All Others
10 15 20 25 30
0.0
0.2
0.4
0.6
0.8
1.0
Time in months
Perc
ent p
rogr
essio
n−fre
e
A
0 5 100
0.0
0.2
0.4
0.6
0.8
1.0
1L OSAll OthersKnown/Likely Combined
Time in months
Perc
ent s
urvi
val
0 20 40 60 80
p < 0.00001
1L srPFSAll OthersKnown/Likely Combined
p < 0.00001
Panel AWith 1L imatinib, srPFS is inferior for patients with Known/Likely SDH-deficient GIST, however, in spite of this, these patients have superior OS compared to the All Others group.
3L OSAll OthersKnown/Likely Combined
2L OSAll OthersKnown/Likely Combined
2L srPFSAll OthersKnown/Likely Combined
3L srPFSAll OthersKnown/Likely Combined
p = 0.003
p = 0.003
10 15 20 25 30
0.0
0.2
0.4
0.6
0.8
1.0
Time in months
Perc
ent p
rogr
essio
n−fre
e
0 5
10 15 20 25 30
0.0
0.2
0.4
0.6
0.8
1.0
Time in months
Perc
ent p
rogr
essio
n−fre
e
0 5
Time in months
Time in months
Perc
ent s
urvi
val
Perc
ent s
urvi
val
100
0.0
0.2
0.4
0.6
0.8
1.0
0 20 40 60 80
100
0.0
0.2
0.4
0.6
0.8
1.0
0 20 40 60 80
p < 0.00001
p = 0.00002
B
Panel B – 2L-4L srPFS and OS is superior in patients with Known/Likely SDH-deficient GIST. The superior srPFS is considered to be more likely due to natural trajectory of the disease rather than a strong TKI effect and the srPFS is similar in 1L-3L for the Known/Likely group, while srPFS drops off dramatically after 1L for the All Others group. Note: 4L data is shown in Supplemental Figures S2, S3.
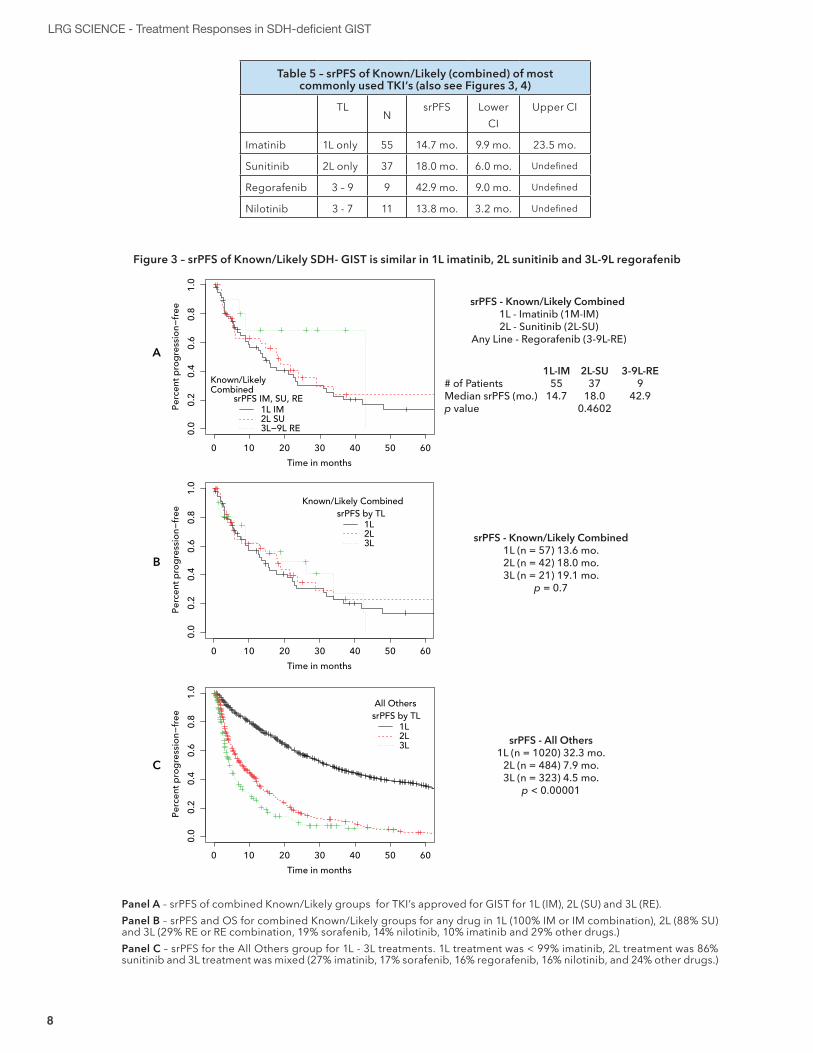
The Known and Likely groups are similar, and OS is consistently superior to the All Other groups in each treatment line (Figure 2 and Supplemental Figure S2 as well as Table 4 and Supplementary Table S2). As noted previously, 1L srPFS was superior for the All Others group, but srPFS was inferior for this group in 2L–4L. For the All Others group, this is likely related to the known drop in efficacy for TKI treatments after 1L in GIST. For the Known and Likely groups, the longer srPFS times in 2L and 3L (before somewhat of a drop in 4L) compare well to the srPFS of these groups in 1L and may reflect the natural trajectory of the disease rather than a close relationship to drug efficacy. SDH-deficient GIST response to TKI’sThe median srPFS times for Combined group patients for 1L imatinib, 2L sunitinib, and 3-9L (combined) regorafenib were: 14.7 mo., 18.0 mo., and 42.9 mo. respectively (Figure 3-A and Table 5) and this difference is not significant (p = 0.46). The survival curves for the imatinib (1L only) and sunitinib (2L only) treatments are

6 7
LRG SCIENCE - Treatment Responses in SDH-deficient GIST
extremely similar and crisscross repeatedly. While the regorafenib treatments appear somewhat better at first glance, the small number of patients (almost half of which are censored) make the curve of this group and the resulting median srPFS time (42.9 mo.) volatile rather than well-defined. A similar pattern (p = 0.7) is seen in Figure 3-B, where all 1L and 2L treatments are included. The similarity of the 1L, 2L, and 3L curves is even more apparent in this graph compared to Figure 3-A. The inclusion of all treatments did not change the number of 1L treatments (imatinib = 57), however it resulted in five additional 2L treatments (sunitinib = 37, other drugs = 5) and all 3L treatments are included (regorafenib = 5, other drugs = 16). In comparison to the Combined group, there is a marked difference in srPFS between 1L, 2L, and 3L in the All Others group, Figure 3-C (p < 0.00001). Supplementary Figures S3 (OS) and S4 (srPFS) provide a more detailed view of the data in Figure 2 with additional data such as median times and hazard ratios. Figure 1 allows for a comprehensive view of both OS and srPFS lines at the same time, while supplementary Figures S3 and S4 provide more detailed data. DISCUSSIONChallenges for SDH-deficient GISTSDH-deficient GIST is a very rare disease and most patients remain undiagnosed. In fact, in the LRG Registry, approximately half of all living patients have had no mutational testing at all. In the half that has had testing, about 16% are KIT/PDGFRA WT, but for 70% of these patients, this is the last reported step in mutational testing; only 30% of the KIT/PDGFRA WT patients have advanced mutational testing, sufficient to classify their disease as SDH-deficient or another type, such as NF1 GIST or a BRAF mutation. It is possible that some of these patients may have had additional testing and either do not understand that they have had additional testing or they may not have reported the additional testing to the LRG Registry. Nearly all SDH-deficient GISTs have a primary tumor located in the stomach, but one case, a 29-year-old male with a germline SDHB mutation had a primary tumor originating in the small bowel19. The LRG Registry contains a second case (previously unreported) of an SDH-deficient patient (SDHB negative IHC) with a small bowel primary tumor.Although the term indolent has sometimes been used to describe SDH-deficient GIST, 11 of the 85 identified Known or Likely group patients have died. So, while SDH-deficient GIST may be less aggressive than typical GISTs, it is still a formidable and sometimes fatal disease and more effective treatments are needed. The sometimes slow-growing/chronic nature makes it more difficult to evaluate treatments. This is compounded by the questionable efficacy of treatments. Is a period of stability due to drug treatment, or is it due to the chronic nature of the disease?
Summary of challenges for SDH-deficient GIST:• This disease is very rare.• Most cases are undiagnosed. Not only is this bad
for the patient, but it limits the number of patients available to contribute to research.
• Tumors are often slow-growing even in cases of metastatic disease confounding attempts to measure treatment efficacy.
• SDH-deficient GISTs objective response to the KIT/PDGFRA inhibitors used to treat mutant GIST has been described as poor or lacking. Reports of efficacy have been limited by small cohort sizes and retrospective nature.
To address these challenges, we created an SDH category system to identify Likely SDH-deficient patients thereby tripling the number of patients available for analysis. We then compared the Known to the Likely groups in terms of srPFS and OS to gauge the sensitivity of the Likely categorization. There was no detectable difference in either srPFS or OS between the Known and Likely groups in any analysis. We then combined these groups and compared this resulting Combined group to All Other patients in our registry. This increased cohort size allowed for a more complete picture of the chronic nature of SDH-deficient GIST as well as a preliminary look at TKI efficacy. The chronic nature of SDH-deficient GISTSDH-deficient GIST tumors have sometimes been described as indolent. Frequent periods of slow-growth or stability even with advanced disease are not uncommon. These periods of slow growth or stability seem to contribute to longer overall survival in SDH-deficient GIST compared to the All Others group of GIST patients, in spite of less effective therapies. However, the term indolent does not adequately capture the toll of the disease. Patients with KIT/PDGFRA mutant GIST are not typically affected until their 6th or 7th decade of life. Patients with SDH-deficient GIST are typically affected starting in their second or third decade of life and often live with the disease for many years. As a hypothetical example, an SDH-deficient patient with 20 years of survival (actual survival is unknown/has not been reached) might still die before reaching the age of 40, compared to a patient with KIT/PDGFRA mutant GIST that might live 10 years with disease and die at age 70. Thus, even though the SDH-deficient patient may have half of the risk of dying over a period of time (as typically expressed by a hazard ratio), it’s possible that as a group they may die at a younger age than typical KIT/PDGFRA mutant GIST patients, while having to endure cancer for twice as long. It’s important to understand that when we say SDH-deficient GIST has longer, or superior survival, we are referring to survival over a specific period of time, such as the period after diagnosis, we are not referring to overall life expectancy.
8 9
LRG SCIENCE - Treatment Responses in SDH-deficient GIST
Panel A – srPFS of combined Known/Likely groups for TKI’s approved for GIST for 1L (IM), 2L (SU) and 3L (RE).Panel B – srPFS and OS for combined Known/Likely groups for any drug in 1L (100% IM or IM combination), 2L (88% SU) and 3L (29% RE or RE combination, 19% sorafenib, 14% nilotinib, 10% imatinib and 29% other drugs.)Panel C – srPFS for the All Others group for 1L - 3L treatments. 1L treatment was < 99% imatinib, 2L treatment was 86% sunitinib and 3L treatment was mixed (27% imatinib, 17% sorafenib, 16% regorafenib, 16% nilotinib, and 24% other drugs.)
20 30 40 50 60
0.0
0.2
0.4
0.6
0.8
1.0
Time in months
Perc
ent p
rogr
essio
n−fre
e
A
B
C
0 10
20 30 40 50 60
0.0
0.2
0.4
0.6
0.8
1.0
Time in months
Perc
ent p
rogr
essio
n−fre
e
0 10
20 30 40 50 60
0.0
0.2
0.4
0.6
0.8
1.0
Time in months
Perc
ent p
rogr
essio
n−fre
e
0 10
Known/Likely Combined
srPFS IM, SU, RE1L IM2L SU3L−9L RE
Known/Likely CombinedsrPFS by TL
1L2L3L
All OtherssrPFS by TL
1L2L3L
srPFS - Known/Likely Combined 1L - Imatinib (1M-IM)2L - Sunitinib (2L-SU)
Any Line - Regorafenib (3-9L-RE)
# of PatientsMedian srPFS (mo.)p value
1L-IM55
14.7
2L-SU37
18.00.4602
3-9L-RE9
42.9
srPFS - Known/Likely Combined1L (n = 57) 13.6 mo.2L (n = 42) 18.0 mo.3L (n = 21) 19.1 mo.
p = 0.7
srPFS - All Others1L (n = 1020) 32.3 mo.
2L (n = 484) 7.9 mo.3L (n = 323) 4.5 mo.
p < 0.00001
Figure 3 – srPFS of Known/Likely SDH- GIST is similar in 1L imatinib, 2L sunitinib and 3L-9L regorafenib
Table 5 – srPFS of Known/Likely (combined) of most commonly used TKI’s (also see Figures 3, 4)
TLN
srPFS LowerCI
Upper CI
Imatinib 1L only 55 14.7 mo. 9.9 mo. 23.5 mo.
Sunitinib 2L only 37 18.0 mo. 6.0 mo. Undefined
Regorafenib 3 – 9 9 42.9 mo. 9.0 mo. Undefined
Nilotinib 3 - 7 11 13.8 mo. 3.2 mo. Undefined
8 9
LRG SCIENCE - Treatment Responses in SDH-deficient GIST
With this perspective in mind, it still may be useful to have some idea how the survival of SDH-deficient patients compares to All Others. This is useful for several reasons. First, it lets the SDH-deficient patient know that survival times cited for typical GIST do not appear to apply to SDH-deficient GIST. Secondly, it may be useful for understanding how inclusion of SDH-deficient GIST patients in studies, including completed studies, may impact the overall results. Interpretation of trial results might be improved when SDH-deficient status is considered.One of the unique characteristics of a patient advocate group registry is the ability to look at diverse groups of patients and follow them over time and through multiple treatments. Registries contain not only the population of interest, but built-in comparison groups that are often missing from other retrospective studies and even some prospective studies, e.g., most Phase II studies. In this study, due in part to the available comparison groups, the LRG Registry provides one of the most comprehensive views to date of the chronic nature of SDH-deficient GIST, something that has been widely suspected/known, but hard to quantify.This sometimes chronic nature is most easily visualized by comparing the OS of Combined patients to All Others (Supplemental Figure S3). In this group of advanced patients, as we follow them from 1L treatment for advanced/metastatic disease to 4L treatment, the risk of death is reduced >62% (range 62%-87%) compared to All Other patients in the same treatment lines. This reduced risk of death can also be seen if we compare all of the Combined patients (including those that never had any drug treatments) from the time of diagnosis to All Others (Supplemental Figure S5); the risk of death is reduced by 78% (HR 0.2199, CI 0.1524 to 0.3173). In the OS from time of diagnosis analysis, patients diagnosed prior to the imatinib era (prior to 2000) are excluded to reduce survivor’s bias.There are some limitations in quantifying the survival of SDH-deficient GIST patients. A number of LRG members who would have been in the Known or Likely groups have died without becoming participants in the registry. We also defined an additional category of patients (not previously discussed) who are described as Possibly SDH-deficient (Possibly). ‘Possibly’ patients were all females with stomach primary diagnosed between 18-35 years old but without mutation testing (unknown mutation). This category (n = 22) almost certainly has some SDH-deficient patients and for unknown reasons has a trend towards worse OS compared to Known patients (p = 0.06399, HR 3.411, CI 0.916 – 12.70). Had these unregistered and ‘Possibly’ patients been included in our analysis OS may have been negatively impacted. Because of these limitations, our current analysis may overestimate the survival of SDH-deficient GIST patients.
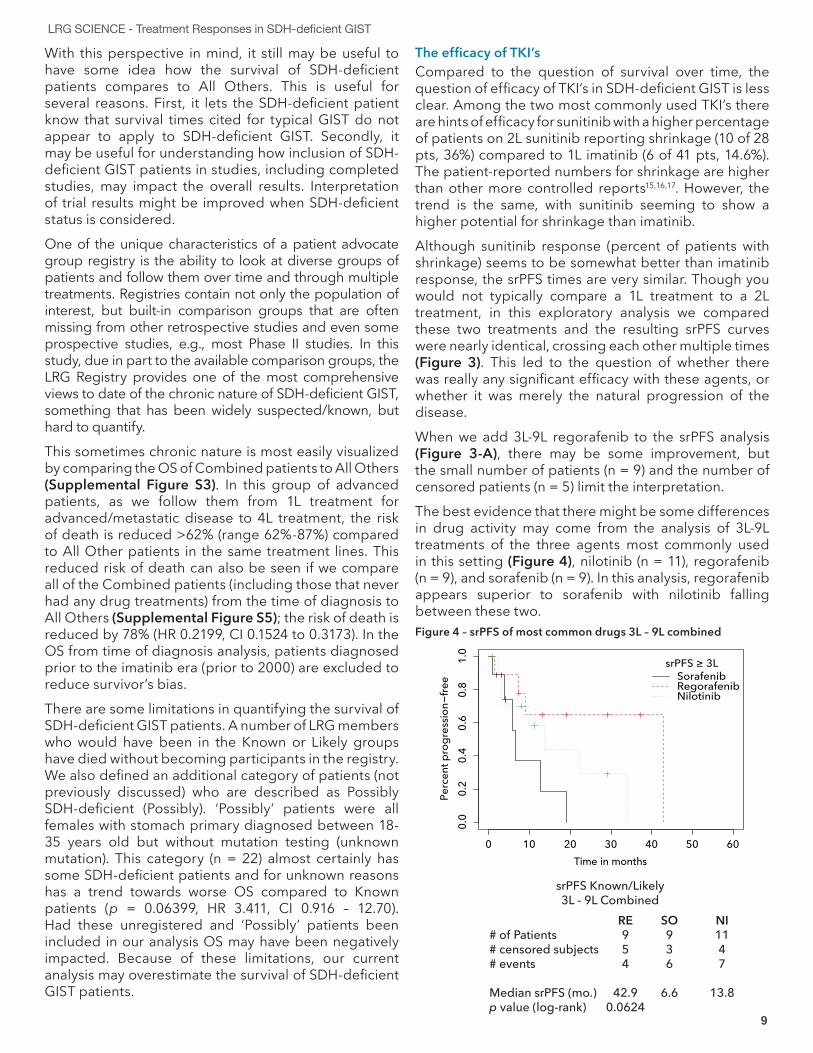
The efficacy of TKI’sCompared to the question of survival over time, the question of efficacy of TKI’s in SDH-deficient GIST is less clear. Among the two most commonly used TKI’s there are hints of efficacy for sunitinib with a higher percentage of patients on 2L sunitinib reporting shrinkage (10 of 28 pts, 36%) compared to 1L imatinib (6 of 41 pts, 14.6%). The patient-reported numbers for shrinkage are higher than other more controlled reports15,16,17. However, the trend is the same, with sunitinib seeming to show a higher potential for shrinkage than imatinib. Although sunitinib response (percent of patients with shrinkage) seems to be somewhat better than imatinib response, the srPFS times are very similar. Though you would not typically compare a 1L treatment to a 2L treatment, in this exploratory analysis we compared these two treatments and the resulting srPFS curves were nearly identical, crossing each other multiple times (Figure 3). This led to the question of whether there was really any significant efficacy with these agents, or whether it was merely the natural progression of the disease. When we add 3L-9L regorafenib to the srPFS analysis (Figure 3-A), there may be some improvement, but the small number of patients (n = 9) and the number of censored patients (n = 5) limit the interpretation. The best evidence that there might be some differences in drug activity may come from the analysis of 3L-9L treatments of the three agents most commonly used in this setting (Figure 4), nilotinib (n = 11), regorafenib (n = 9), and sorafenib (n = 9). In this analysis, regorafenib appears superior to sorafenib with nilotinib falling between these two. Figure 4 – srPFS of most common drugs 3L – 9L combined
20 30 40 50 60
0.0
0.2
0.4
0.6
0.8
1.0
Time in months
Perc
ent p
rogr
essio
n−fre
e
0 10
srPFS Known/Likely3L - 9L Combined
# of Patients# censored subjects# events
Median srPFS (mo.)p value (log-rank)
RE954
42.90.0624
SO936
6.6
NI1147
13.8
srPFS ≥ 3LSorafenibRegorafenibNilotinib

10 11
LRG SCIENCE - Treatment Responses in SDH-deficient GIST
However, the numbers remain too small to reach any definitive conclusions. This is further confounded by the fact that the treatments occurred in various stages of disease (3L-9L). The median srPFS of 42.9 months for regorafenib is volatile rather than well-defined with small numbers and five of the nine patients censored.Given the chronic nature of the disease, it is tempting to speculate that, in addition to efficacy, the tolerability of drugs may play a role that’s as important. For example, despite the questions of efficacy for imatinib, there are multiple cases where Known and Likely patients have long-term treatment histories with imatinib. There are cases where patients have longer treatment with sunitinib compared to imatinib and also cases with longer treatment with imatinib compared to sunitinib. Meeting the challenges of SDH-deficient GISTOne of the biggest challenges with SDH-deficient GIST is that most patients remain undiagnosed. This results in a small pool of patients available to contribute to research. The LRG is a part of the Pediatric & SDH-Deficient GIST Consortium which is dedicated to SDH-deficient GIST research. Working with expert GIST pathologists, the Consortium has created an algorithm that recommends immunohistochemical staining for SDHB for all GIST patients with a primary tumor located in the stomach. This testing should be done at the time of diagnosis and, if fully implemented, will increase the number of SDH-deficient patients receiving the proper diagnosis by as much as 500% (based on testing rates in the LRG Registry). More information about the Pediatric & SDH-Deficient GIST Consortium can be found at: www.liferaftgroup.org/pediatric-sdh-deficient-gist-consortium/.The second challenge associated with SDH-deficient GIST is finding more effective treatments. The current treatment paradigm typically involves treating these patients similarly to GIST, with TKI’s approved or frequently used for GIST. Given the difficulties in
evaluating these treatments in this population, it is unclear if these agents have significant activity. Dramatically increasing the diagnosis rate will increase the number of patients/treatments available for analysis and possibly allow for inclusion of comparison groups including patients not on any treatment. Additional areas that need to be explored include treatments that are more targeted to the underlying genetic defect, SDH deficiency. At least two efforts are currently underway with a Phase II study at the National Institutes of Health (NIH) for the demethylating agent, guadecitabine (NCT03165721) and a Phase II study of temozolomide (NCT03556384). The guadecitabine study is the result of research showing that global hypermethylation is a unique feature of all types of SDH-deficient GIST20. Next stepsThis report is based on data with a data cutoff of 4/17/2017. The next step for LRG data (using an updated data set with a cutoff in 2019) will be a more detailed look at individual patients’ response to imatinib, sunitinib and regorafenib using waterfall charts. This may show, in more detail, the differential intra-patient responses between these agents. Periods of no treatment would ideally be included as well, although in older cases, these are not as well documented in the registry. We also plan to do a comparison of Known and Likely patients versus an age-matched cohort of patients in the registry without SDH-deficiency, although this may be limited by the number of young patients without SDH-deficiency. In addition to SDH-deficiency itself, it is possible that the younger age of SDH-deficient patients may play a role in longer survival. Further refinement, optimization, and validation of the algorithm used to create the Likely group and other SDH categories might allow for more extensive investigation into treatment response utilizing other GIST registries or collaborative studies.
DisclaimerWe saw hints of drug effect with more patient-reported shrinkage on sunitinib compared to other drugs and with a longer time on treatment before reported progression for regorafenib. However, the numbers were too small to reach any definitive conclusions about drug efficacy. We cannot confirm or exclude a positive effect from the TKI treatments describe in this study. Future studies should incorporate a “no treatment” comparison if possible.
10 11
LRG SCIENCE - Treatment Responses in SDH-deficient GIST
1. Hirota, S. et al. Gain-of-function mutations of c-kit in human gastrointestinal stromal tumors. Science 279, 577–580 (1998).
2. Demetri, G. D. et al. Efficacy and safety of imatinib mesylate in advanced gastrointestinal stromal tumors. N Engl J Med 347, 472–480 (2002).
3. Druker, B. J. et al. Efficacy and Safety of a Specific Inhibitor of the BCR-ABL Tyrosine Kinase in Chronic Myeloid Leukemia. New England Journal of Medicine 344, 1031–1037 (2001).
4. Soverini, S., Mancini, M., Bavaro, L., Cavo, M. & Martinelli, G. Chronic myeloid leukemia: the paradigm of targeting oncogenic tyrosine kinase signaling and counteracting resistance for successful cancer therapy. Mol. Cancer 17, 49 (2018).
5. Heinrich, M. C. et al. PDGFRA Activating Mutations in Gastrointestinal Stromal tumors. Science 299, 708–710 (2003).
6. Hirota, S. et al. Gain-of-function mutations of platelet-derived growth factor receptor α gene in gastrointestinal stromal tumors. Gastroenterology 125, 660–667 (2003).
7. Corless, C. L. PDGFRA mutations in gastrointestinal stromal tumors: frequency, spectrum and in vitro sensitivity to Imatinib. J Clin Oncol 23, 5357–5364 (2005).
8. Cassier, P. A. et al. A prospective epidemiological study of new incident GISTs during two consecutive years in Rhone Alpes region: incidence and molecular distribution of GIST in a European region. Br J Cancer 103, 165–170 (2010).
9. Heinrich, M. C. et al. Crenolanib Inhibits the Drug-Resistant PDGFRA D842V Mutation Associated with Imatinib-resistant Gastrointestinal Stromal Tumors. Clin Cancer Res (2012). doi:10.1158/1078-0432.CCR-12-0625
10. Schneider-Stock, R. BLU-285—the breakthrough in treatment of patients with aggressive systemic mastocytosis and gastrointestinal stromal tumor. Ann Transl Med 6, (2018).
11. Pasini, B. et al. Clinical and molecular genetics of patients with the Carney-Stratakis syndrome and germline mutations of the genes coding for the succinate dehydrogenase subunits SDHB, SDHC, and SDHD. Eur J Hum Genet 16, 79–88 (2007).
12. Pantaleo, M. A. et al. SDHA Loss-of-Function Mutations in KIT-PDGFRA Wild-Type Gastrointestinal Stromal Tumors Identified by Massively Parallel Sequencing. J Nat Cancer Institute 103, 983–987 (2011).
13. Haller, F. et al. Aberrant DNA hypermethylation of SDHC: a novel mechanism of tumor development in Carney triad. Endocr Relat Cancer ERC-14-0254 (2014). doi:10.1530/ERC-14-0254
14. Miettinen, M. et al. Succinate dehydrogenase deficient gists - a clinicopathologic, immunohistochemical, and molecular genetic study of 66 gastric GISTs with predilection to young age. Am J Surg Pathol 35, 1712–1721 (2011).
15. Boikos, S. A. et al. Molecular Subtypes of KIT/PDGFRA Wild-Type Gastrointestinal Stromal Tumors: A Report From the National Institutes of Health Gastrointestinal Stromal Tumor Clinic. JAMA Oncol 2, 922–928 (2016).
16. Rutkowski, P., Magnan, H., Chou, A. J. & Benson, C. Treatment of gastrointestinal stromal tumours in paediatric and young adult patients with sunitinib: a multicentre case series. BMC Cancer 17, 717 (2017).
17. Janeway, K. A. et al. Sunitinib treatment in pediatric patients with advanced GIST following failure of imatinib. Pediatr Blood Cancer 52, 767–771 (2009).
18. Miettinen, M. & Lasota, J. Succinate dehydrogenase deficient gastrointestinal stromal tumors (GISTs) – A REVIEW. Int J Biochem Cell Biol 0, 514–519 (2014).
19. Elston, M. S. et al. A Duodenal SDH-Deficient Gastrointestinal Stromal Tumor in a Patient With a Germline SDHB Mutation. J. Clin. Endocrinol. Metab. 102, 1447–1450 (2017).
20. Killian, J. K. et al. Succinate dehydrogenase mutation underlies global epigenomic divergence in gastrointestinal stromal tumor. Cancer Discov (2013). doi:10.1158/2159-8290.CD-13-0092.
REFERENCES
12 13
LRG SCIENCE - Treatment Responses in SDH-deficient GIST
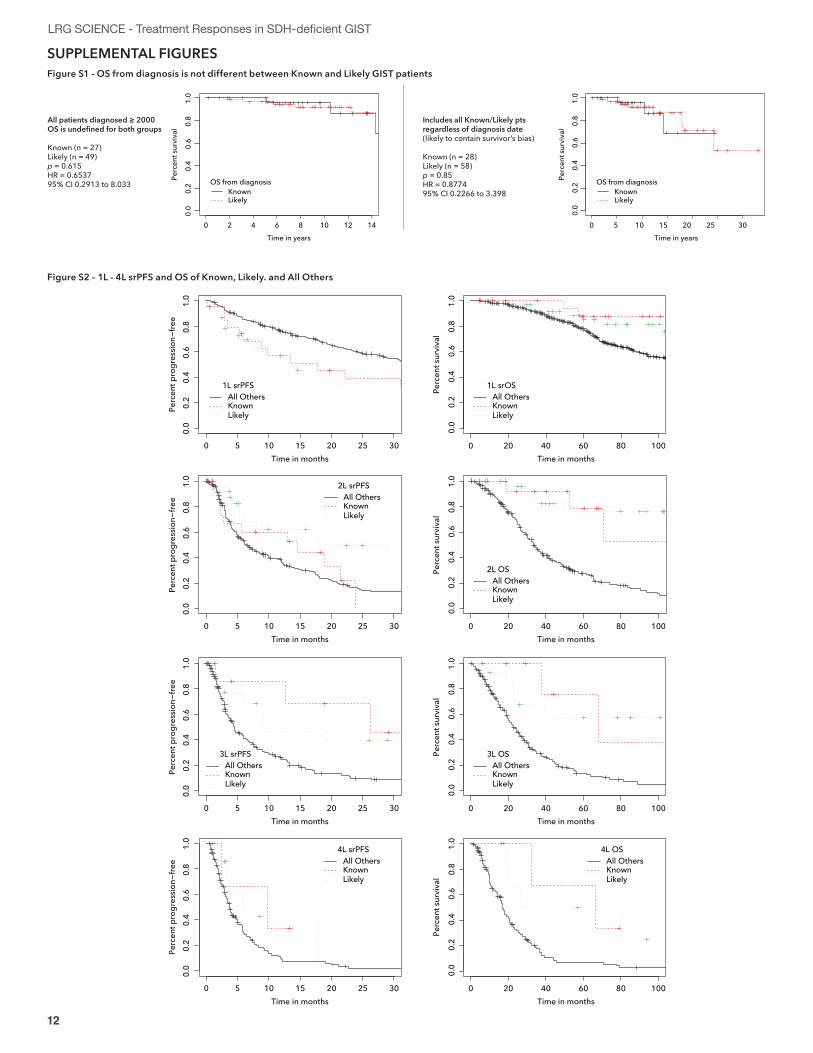
SUPPLEMENTAL FIGURES Figure S1 - OS from diagnosis is not different between Known and Likely GIST patients
0 5 10 15 20 25 30
0.0
0.2
0.4
0.6
0.8
1.0
Time in years
Perc
ent s
urvi
val
Includes all Known/Likely ptsregardless of diagnosis date(likely to contain survivor’s bias)
Known (n = 28)Likely (n = 58)p = 0.85HR = 0.877495% CI 0.2266 to 3.398
OS from diagnosisKnown Likely
0.0
0.2
0.4
0.6
0.8
1.0
Time in years
Perc
ent s
urvi
val
OS from diagnosisKnown Likely
0 2 4 6 8 10 12 14
All patients diagnosed ≥ 2000OS is undefined for both groups
Known (n = 27)Likely (n = 49)p = 0.615HR = 0.653795% CI 0.2913 to 8.033
Figure S2 – 1L - 4L srPFS and OS of Known, Likely. and All Others
10 15 20 25 30
0.0
0.2
0.4
0.6
0.8
1.0
Time in months
Perc
ent p
rogr
essio
n−fre
e
0 5 1000.
00.
20.
40.
60.
81.
0Time in months
Perc
ent s
urvi
val
0 20 40 60 80
10 15 20 25 30
0.0
0.2
0.4
0.6
0.8
1.0
Time in months
Perc
ent p
rogr
essio
n−fre
e
0 5 100
0.0
0.2
0.4
0.6
0.8
1.0
Time in months
Perc
ent s
urvi
val
0 20 40 60 80
10 15 20 25 30
0.0
0.2
0.4
0.6
0.8
1.0
Time in months
Perc
ent p
rogr
essio
n−fre
e
0 5 100
0.0
0.2
0.4
0.6
0.8
1.0
Time in months
Perc
ent s
urvi
val
0 20 40 60 80
10 15 20 25 30
0.0
0.2
0.4
0.6
0.8
1.0
Time in months
Perc
ent p
rogr
essio
n−fre
e
0 5 100
0.0
0.2
0.4
0.6
0.8
1.0
Time in months
Perc
ent s
urvi
val
0 20 40 60 80
1L srPFSAll OthersKnownLikely
1L srOSAll OthersKnownLikely
3L srPFSAll OthersKnownLikely
3L OSAll OthersKnownLikely
4L srPFSAll OthersKnownLikely
4L OSAll OthersKnownLikely
2L srPFSAll OthersKnownLikely
2L OSAll OthersKnownLikely
12 13
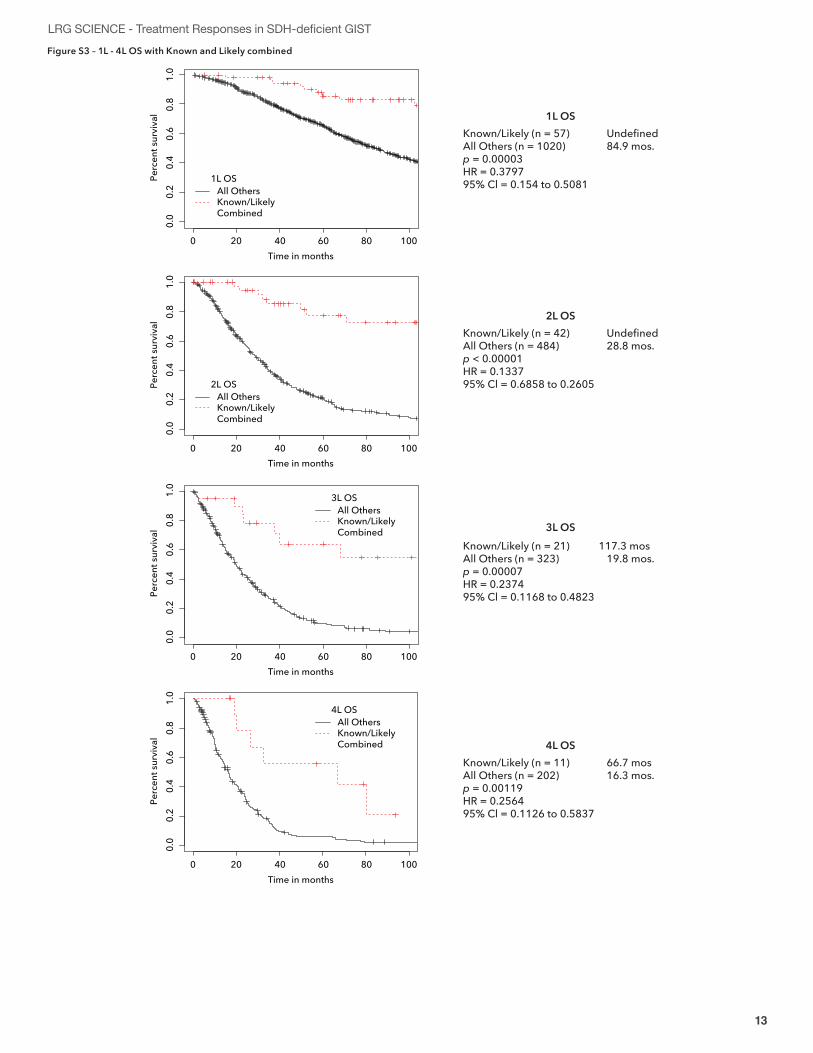
LRG SCIENCE - Treatment Responses in SDH-deficient GISTFigure S3 – 1L - 4L OS with Known and Likely combined
0.0
0.2
0.4
0.6
0.8
1.0
Time in months
Perc
ent s
urvi
val
40 60 80 1000 20
40 60 80 1000 20
0.0
0.2
0.4
0.6
0.8
1.0
Time in months
Perc
ent s
urvi
val
Time in months
Time in months
40 60 80 1000 20
0.0
0.2
0.4
0.6
0.8
1.0
Perc
ent s
urvi
val
40 60 80 1000 20
0.0
0.2
0.4
0.6
0.8
1.0
Perc
ent s
urvi
val
Known/Likely (n = 57) UndefinedAll Others (n = 1020) 84.9 mos.p = 0.00003HR = 0.379795% Cl = 0.154 to 0.5081
1L OS
Known/Likely (n = 42) UndefinedAll Others (n = 484) 28.8 mos.p < 0.00001HR = 0.133795% Cl = 0.6858 to 0.2605
2L OS
Known/Likely (n = 21) 117.3 mosAll Others (n = 323) 19.8 mos.p = 0.00007HR = 0.237495% Cl = 0.1168 to 0.4823
3L OS
Known/Likely (n = 11) 66.7 mosAll Others (n = 202) 16.3 mos.p = 0.00119HR = 0.256495% Cl = 0.1126 to 0.5837
4L OS
1L OSAll OthersKnown/Likely Combined
2L OSAll OthersKnown/Likely Combined
3L OSAll OthersKnown/Likely Combined
4L OSAll OthersKnown/Likely Combined
14 15
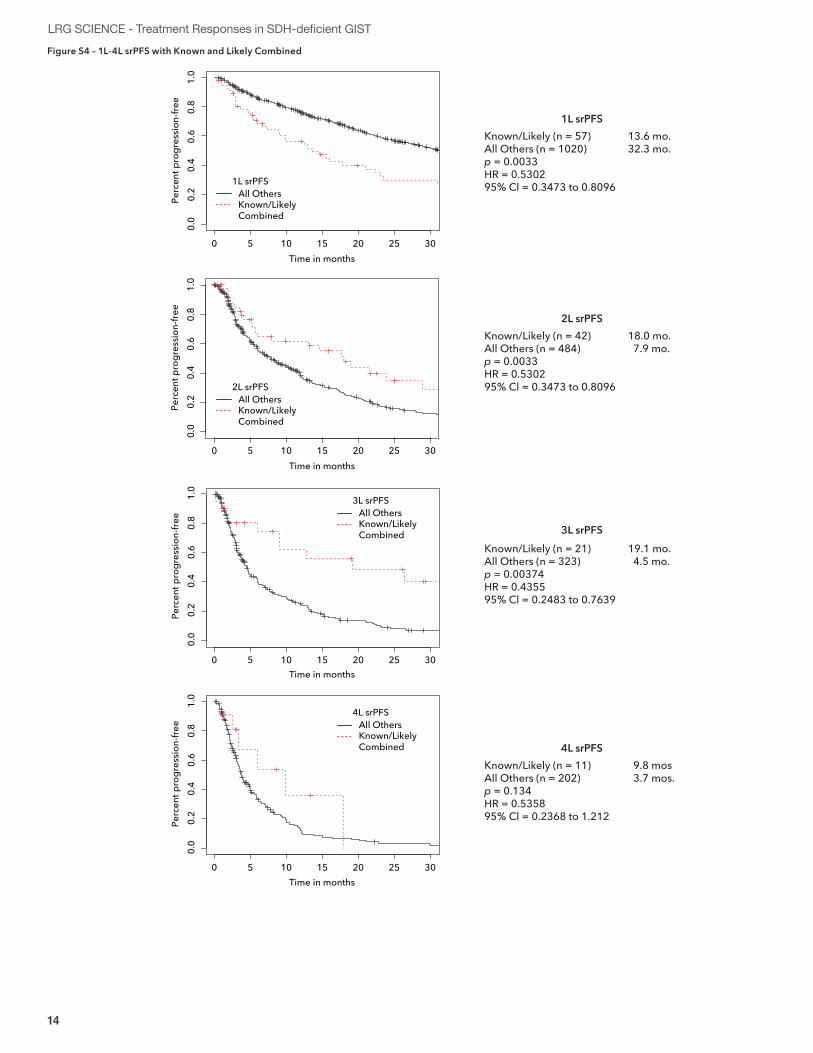
LRG SCIENCE - Treatment Responses in SDH-deficient GISTFigure S4 – 1L-4L srPFS with Known and Likely Combined
Time in months
0.0
0.2
0.4
0.6
0.8
1.0
Perc
ent p
rogr
essio
n-fre
e
Time in months
0.0
0.2
0.4
0.6
0.8
1.0
Perc
ent p
rogr
essio
n-fre
e
Time in months
Time in months
0.0
0.2
0.4
0.6
0.8
1.0
Perc
ent p
rogr
essio
n-fre
e0.
00.
20.
40.
60.
81.
0Pe
rcen
t pro
gres
sion-
free
Known/Likely (n = 57) 13.6 mo.All Others (n = 1020) 32.3 mo.p = 0.0033HR = 0.530295% Cl = 0.3473 to 0.8096
1L srPFS
Known/Likely (n = 42) 18.0 mo.All Others (n = 484) 7.9 mo.p = 0.0033HR = 0.530295% Cl = 0.3473 to 0.8096
2L srPFS
Known/Likely (n = 21) 19.1 mo.All Others (n = 323) 4.5 mo.p = 0.00374HR = 0.435595% Cl = 0.2483 to 0.7639
3L srPFS
Known/Likely (n = 11) 9.8 mosAll Others (n = 202) 3.7 mos.p = 0.134HR = 0.535895% Cl = 0.2368 to 1.212
4L srPFS
1L srPFSAll OthersKnown/Likely Combined
2L srPFSAll OthersKnown/Likely Combined
3L srPFSAll OthersKnown/Likely Combined
4L srPFSAll OthersKnown/Likely Combined
10 15 20 30250 5
10 15 20 30250 5
10 15 20 30250 5
10 15 20 30250 5
14 15
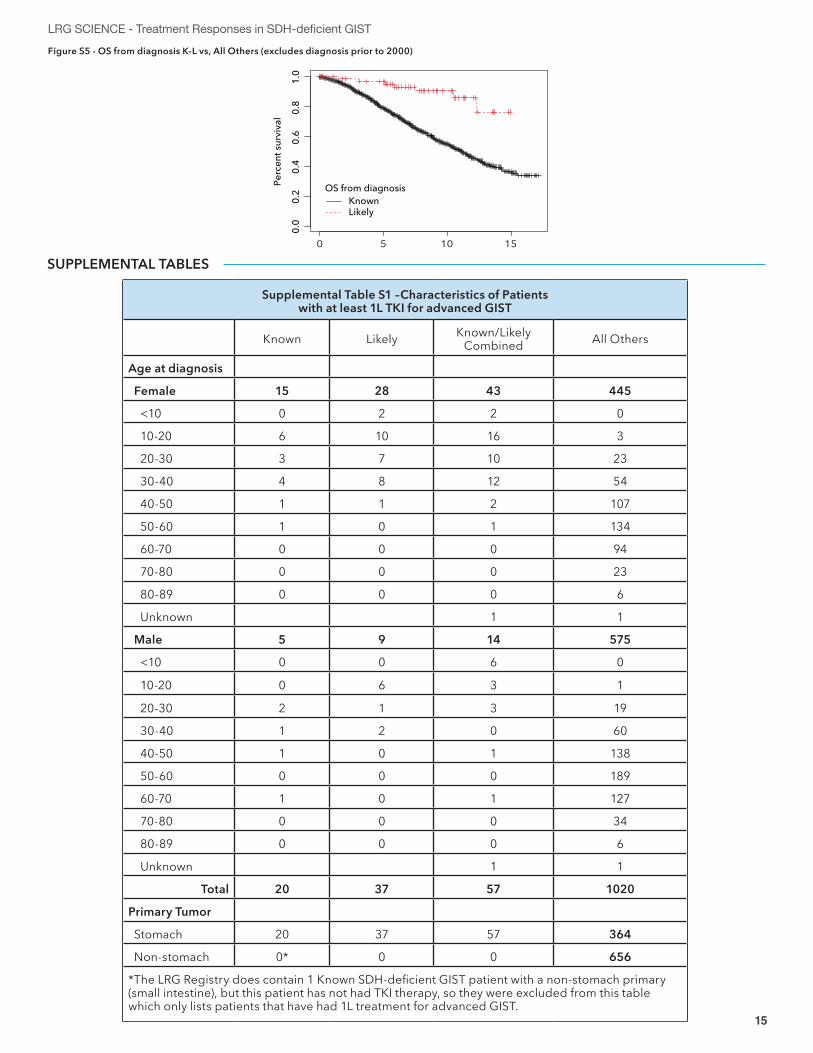
LRG SCIENCE - Treatment Responses in SDH-deficient GISTFigure S5 - OS from diagnosis K-L vs, All Others (excludes diagnosis prior to 2000)
0.0
0.2
0.4
0.6
0.8
1.0
Time in yearsPe
rcen
t sur
viva
l
OS from diagnosisKnown Likely
10 150 5
SUPPLEMENTAL TABLES
Supplemental Table S1 –Characteristics of Patients with at least 1L TKI for advanced GIST
Known Likely Known/Likely Combined All Others
Age at diagnosis
Female 15 28 43 445
<10 0 2 2 0
10-20 6 10 16 3
20-30 3 7 10 23
30-40 4 8 12 54
40-50 1 1 2 107
50-60 1 0 1 134
60-70 0 0 0 94
70-80 0 0 0 23
80-89 0 0 0 6
Unknown 1 1
Male 5 9 14 575
<10 0 0 6 0
10-20 0 6 3 1
20-30 2 1 3 19
30-40 1 2 0 60
40-50 1 0 1 138
50-60 0 0 0 189
60-70 1 0 1 127
70-80 0 0 0 34
80-89 0 0 0 6
Unknown 1 1
Total 20 37 57 1020
Primary Tumor
Stomach 20 37 57 364
Non-stomach 0* 0 0 656
*The LRG Registry does contain 1 Known SDH-deficient GIST patient with a non-stomach primary (small intestine), but this patient has not had TKI therapy, so they were excluded from this table which only lists patients that have had 1L treatment for advanced GIST.
16 17
LRG SCIENCE - Treatment Responses in SDH-deficient GIST
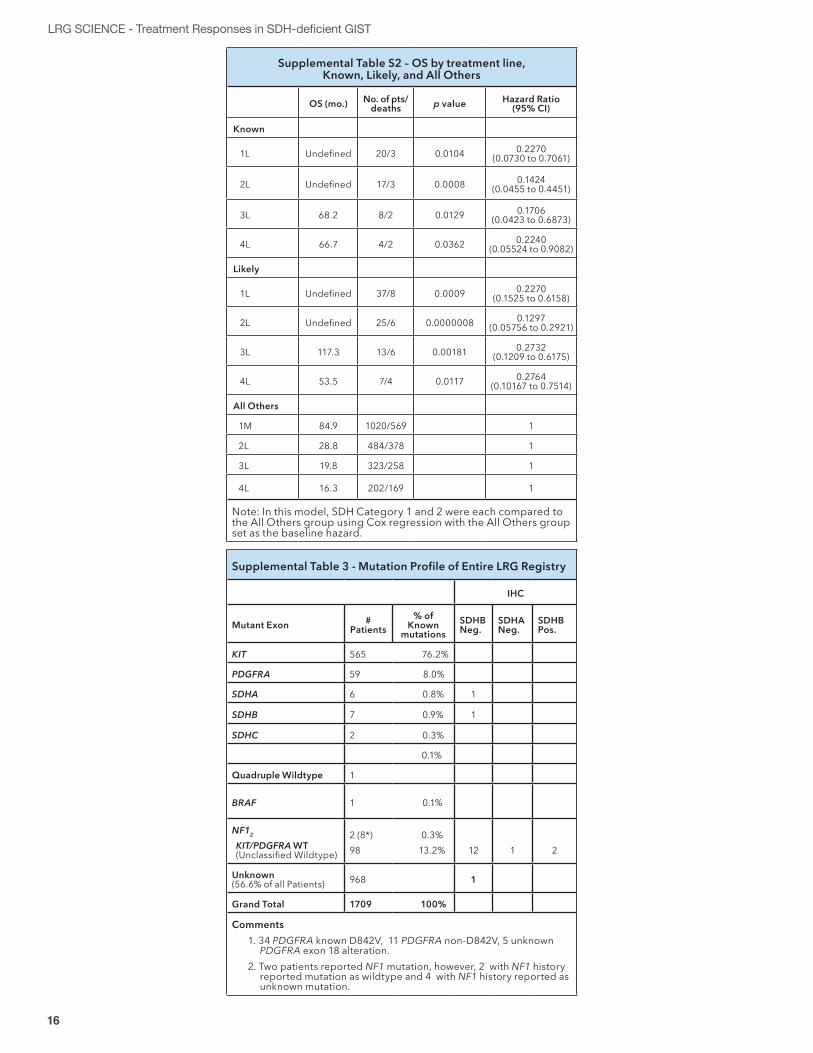
Supplemental Table S2 – OS by treatment line, Known, Likely, and All Others
OS (mo.) No. of pts/deaths p value Hazard Ratio
(95% CI)
Known
1L Undefined 20/3 0.0104 0.2270 (0.0730 to 0.7061)
2L Undefined 17/3 0.0008 0.1424 (0.0455 to 0.4451)
3L 68.2 8/2 0.0129 0.1706 (0.0423 to 0.6873)
4L 66.7 4/2 0.0362 0.2240 (0.05524 to 0.9082)
Likely
1L Undefined 37/8 0.0009 0.2270 (0.1525 to 0.6158)
2L Undefined 25/6 0.0000008 0.1297 (0.05756 to 0.2921)
3L 117.3 13/6 0.00181 0.2732 (0.1209 to 0.6175)
4L 53.5 7/4 0.0117 0.2764 (0.10167 to 0.7514)
All Others
1M 84.9 1020/569 1
2L 28.8 484/378 1
3L 19.8 323/258 1
4L 16.3 202/169 1
Note: In this model, SDH Category 1 and 2 were each compared to the All Others group using Cox regression with the All Others group set as the baseline hazard.
Supplemental Table 3 - Mutation Profile of Entire LRG Registry
IHC
Mutant Exon # Patients
% of Known
mutationsSDHB Neg.
SDHA Neg.
SDHB Pos.
KIT 565 76.2%
PDGFRA 59 8.0%
SDHA 6 0.8% 1
SDHB 7 0.9% 1
SDHC 2 0.3%
0.1%
Quadruple Wildtype 1
BRAF 1 0.1%
NF12
KIT/PDGFRA WT (Unclassified Wildtype)
2 (8*) 0.3%98 13.2% 12 1 2
Unknown (56.6% of all Patients) 968 1
Grand Total 1709 100%
Comments1. 34 PDGFRA known D842V, 11 PDGFRA non-D842V, 5 unknown
PDGFRA exon 18 alteration.2. Two patients reported NF1 mutation, however, 2 with NF1 history
reported mutation as wildtype and 4 with NF1 history reported as unknown mutation.
16 17
LRG SCIENCE - Treatment Responses in SDH-deficient GIST
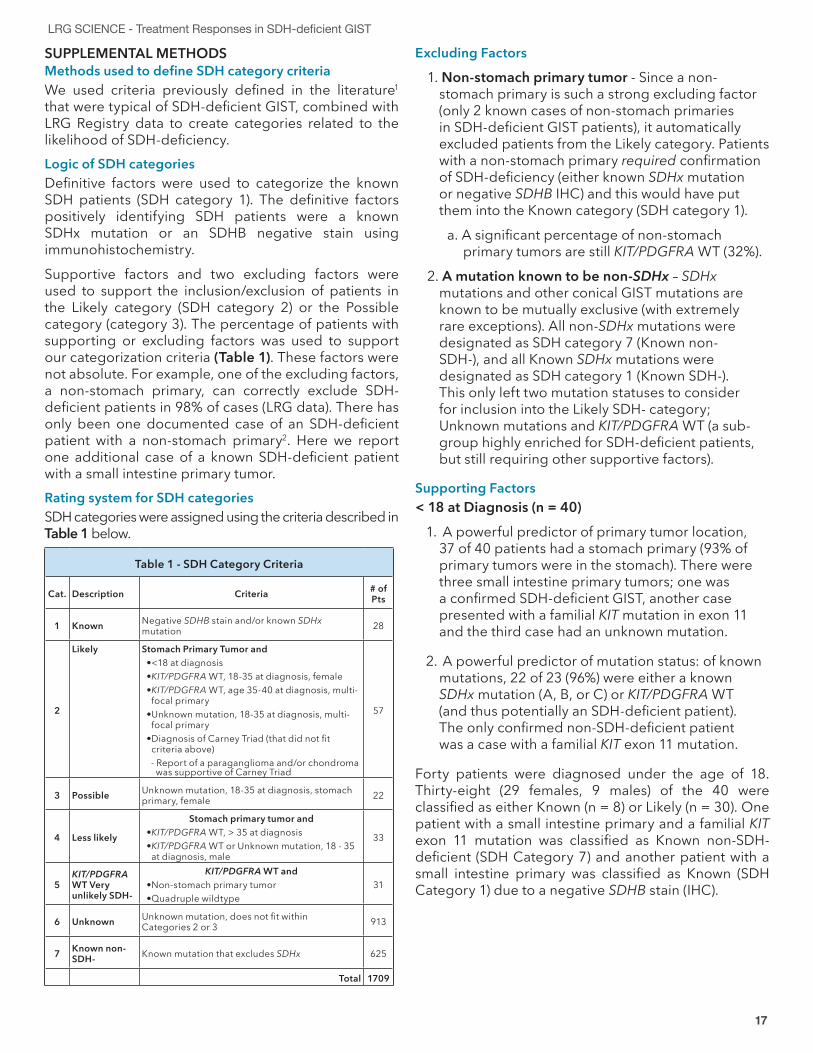
SUPPLEMENTAL METHODSMethods used to define SDH category criteriaWe used criteria previously defined in the literature1 that were typical of SDH-deficient GIST, combined with LRG Registry data to create categories related to the likelihood of SDH-deficiency.Logic of SDH categoriesDefinitive factors were used to categorize the known SDH patients (SDH category 1). The definitive factors positively identifying SDH patients were a known SDHx mutation or an SDHB negative stain using immunohistochemistry. Supportive factors and two excluding factors were used to support the inclusion/exclusion of patients in the Likely category (SDH category 2) or the Possible category (category 3). The percentage of patients with supporting or excluding factors was used to support our categorization criteria (Table 1). These factors were not absolute. For example, one of the excluding factors, a non-stomach primary, can correctly exclude SDH-deficient patients in 98% of cases (LRG data). There has only been one documented case of an SDH-deficient patient with a non-stomach primary2. Here we report one additional case of a known SDH-deficient patient with a small intestine primary tumor.Rating system for SDH categories SDH categories were assigned using the criteria described in Table 1 below.
Table 1 - SDH Category Criteria
Cat. Description Criteria # of Pts
1 Known Negative SDHB stain and/or known SDHx mutation 28
2
Likely Stomach Primary Tumor and• <18 at diagnosis• KIT/PDGFRA WT, 18-35 at diagnosis, female• KIT/PDGFRA WT, age 35-40 at diagnosis, multi-
focal primary• Unknown mutation, 18-35 at diagnosis, multi-
focal primary• Diagnosis of Carney Triad (that did not fit
criteria above) - Report of a paraganglioma and/or chondroma was supportive of Carney Triad
57
3 Possible Unknown mutation, 18-35 at diagnosis, stomach primary, female 22
4 Less likely
Stomach primary tumor and• KIT/PDGFRA WT, > 35 at diagnosis• KIT/PDGFRA WT or Unknown mutation, 18 - 35
at diagnosis, male
33
5KIT/PDGFRA WT Very unlikely SDH-
KIT/PDGFRA WT and• Non-stomach primary tumor• Quadruple wildtype
31
6 Unknown Unknown mutation, does not fit within Categories 2 or 3 913
7 Known non-SDH- Known mutation that excludes SDHx 625
Total 1709
Excluding Factors
1. Non-stomach primary tumor - Since a non-stomach primary is such a strong excluding factor (only 2 known cases of non-stomach primaries in SDH-deficient GIST patients), it automatically excluded patients from the Likely category. Patients with a non-stomach primary required confirmation of SDH-deficiency (either known SDHx mutation or negative SDHB IHC) and this would have put them into the Known category (SDH category 1).
a. A significant percentage of non-stomach primary tumors are still KIT/PDGFRA WT (32%).
2. A mutation known to be non-SDHx – SDHx mutations and other conical GIST mutations are known to be mutually exclusive (with extremely rare exceptions). All non-SDHx mutations were designated as SDH category 7 (Known non-SDH-), and all Known SDHx mutations were designated as SDH category 1 (Known SDH-). This only left two mutation statuses to consider for inclusion into the Likely SDH- category; Unknown mutations and KIT/PDGFRA WT (a sub-group highly enriched for SDH-deficient patients, but still requiring other supportive factors).
Supporting Factors< 18 at Diagnosis (n = 40)
1. A powerful predictor of primary tumor location, 37 of 40 patients had a stomach primary (93% of primary tumors were in the stomach). There were three small intestine primary tumors; one was a confirmed SDH-deficient GIST, another case presented with a familial KIT mutation in exon 11 and the third case had an unknown mutation.
2. A powerful predictor of mutation status: of known mutations, 22 of 23 (96%) were either a known SDHx mutation (A, B, or C) or KIT/PDGFRA WT (and thus potentially an SDH-deficient patient). The only confirmed non-SDH-deficient patient was a case with a familial KIT exon 11 mutation.
Forty patients were diagnosed under the age of 18. Thirty-eight (29 females, 9 males) of the 40 were classified as either Known (n = 8) or Likely (n = 30). One patient with a small intestine primary and a familial KIT exon 11 mutation was classified as Known non-SDH-deficient (SDH Category 7) and another patient with a small intestine primary was classified as Known (SDH Category 1) due to a negative SDHB stain (IHC).
18 19
LRG SCIENCE - Treatment Responses in SDH-deficient GIST
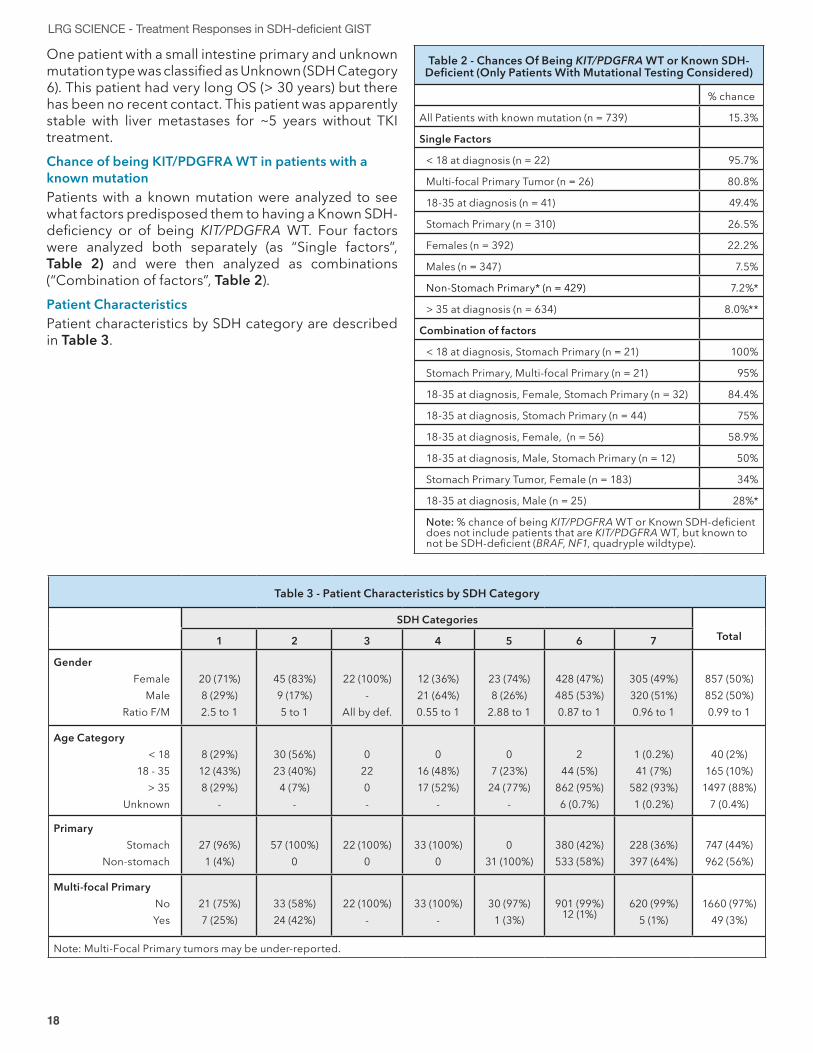
One patient with a small intestine primary and unknown mutation type was classified as Unknown (SDH Category 6). This patient had very long OS (> 30 years) but there has been no recent contact. This patient was apparently stable with liver metastases for ~5 years without TKI treatment. Chance of being KIT/PDGFRA WT in patients with a known mutationPatients with a known mutation were analyzed to see what factors predisposed them to having a Known SDH-deficiency or of being KIT/PDGFRA WT. Four factors were analyzed both separately (as “Single factors”, Table 2) and were then analyzed as combinations (“Combination of factors”, Table 2). Patient CharacteristicsPatient characteristics by SDH category are described in Table 3.
Table 2 - Chances Of Being KIT/PDGFRA WT or Known SDH-Deficient (Only Patients With Mutational Testing Considered)
% chance
All Patients with known mutation (n = 739) 15.3%
Single Factors
< 18 at diagnosis (n = 22) 95.7%
Multi-focal Primary Tumor (n = 26) 80.8%
18-35 at diagnosis (n = 41) 49.4%
Stomach Primary (n = 310) 26.5%
Females (n = 392) 22.2%
Males (n = 347) 7.5%
Non-Stomach Primary* (n = 429) 7.2%*
> 35 at diagnosis (n = 634) 8.0%**
Combination of factors
< 18 at diagnosis, Stomach Primary (n = 21) 100%
Stomach Primary, Multi-focal Primary (n = 21) 95%
18-35 at diagnosis, Female, Stomach Primary (n = 32) 84.4%
18-35 at diagnosis, Stomach Primary (n = 44) 75%
18-35 at diagnosis, Female, (n = 56) 58.9%
18-35 at diagnosis, Male, Stomach Primary (n = 12) 50%
Stomach Primary Tumor, Female (n = 183) 34%
18-35 at diagnosis, Male (n = 25) 28%*
Note: % chance of being KIT/PDGFRA WT or Known SDH-deficient does not include patients that are KIT/PDGFRA WT, but known to not be SDH-deficient (BRAF, NF1, quadryple wildtype).
Table 3 - Patient Characteristics by SDH Category
SDH CategoriesTotal1 2 3 4 5 6 7
GenderFemale
MaleRatio F/M
20 (71%)8 (29%)2.5 to 1
45 (83%)9 (17%)5 to 1
22 (100%)-
All by def.
12 (36%)21 (64%)0.55 to 1
23 (74%)8 (26%)
2.88 to 1
428 (47%)485 (53%)0.87 to 1
305 (49%)320 (51%)0.96 to 1
857 (50%)852 (50%)0.99 to 1
Age Category< 18
18 - 35> 35
Unknown
8 (29%)12 (43%)8 (29%)
-
30 (56%)23 (40%)
4 (7%)-
0220-
016 (48%)17 (52%)
-
07 (23%)
24 (77%)-
244 (5%)
862 (95%)6 (0.7%)
1 (0.2%)41 (7%)
582 (93%) 1 (0.2%)
40 (2%)165 (10%)
1497 (88%)7 (0.4%)
PrimaryStomach
Non-stomach27 (96%)
1 (4%)57 (100%)
022 (100%)
033 (100%)
00
31 (100%)380 (42%)533 (58%)
228 (36%)397 (64%)
747 (44%)962 (56%)
Multi-focal PrimaryNoYes
21 (75%)7 (25%)
33 (58%)24 (42%)
22 (100%)-
33 (100%)-
30 (97%)1 (3%)
901 (99%) 12 (1%)
620 (99%)5 (1%)
1660 (97%)49 (3%)
Note: Multi-Focal Primary tumors may be under-reported.
18 19
LRG SCIENCE - Treatment Responses in SDH-deficient GIST
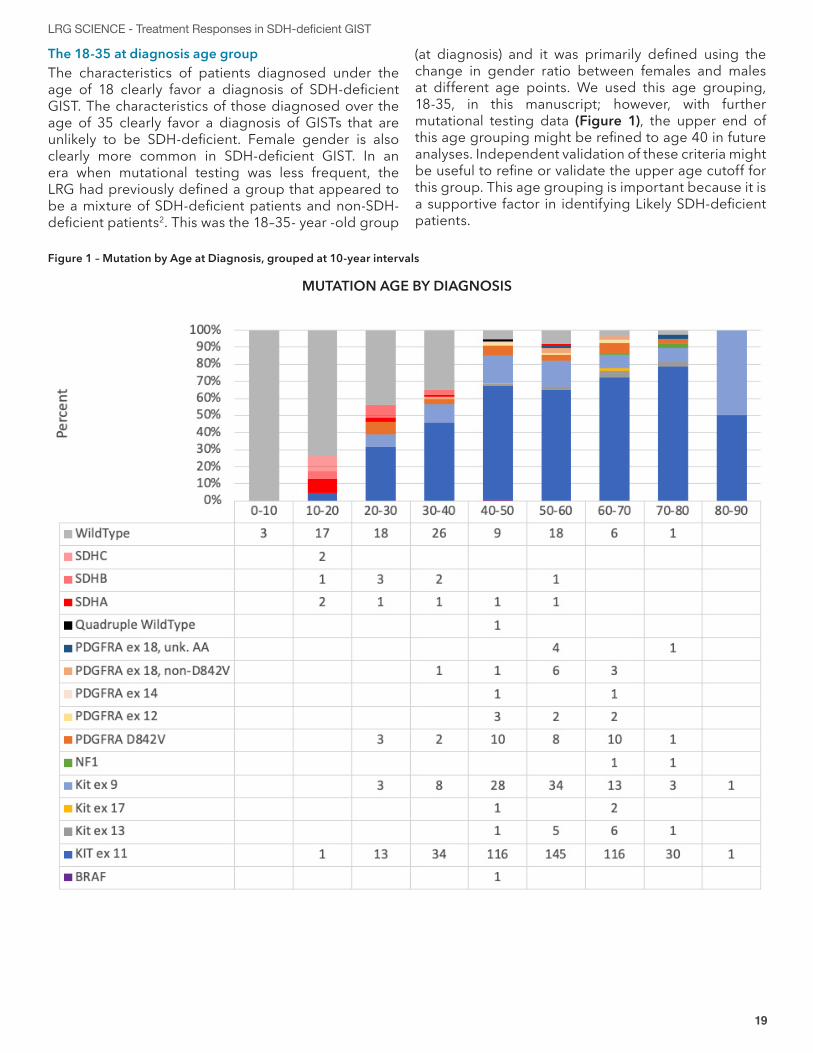
Figure 1 – Mutation by Age at Diagnosis, grouped at 10-year intervals
MUTATION AGE BY DIAGNOSIS
The 18-35 at diagnosis age groupThe characteristics of patients diagnosed under the age of 18 clearly favor a diagnosis of SDH-deficient GIST. The characteristics of those diagnosed over the age of 35 clearly favor a diagnosis of GISTs that are unlikely to be SDH-deficient. Female gender is also clearly more common in SDH-deficient GIST. In an era when mutational testing was less frequent, the LRG had previously defined a group that appeared to be a mixture of SDH-deficient patients and non-SDH-deficient patients2. This was the 18–35- year -old group
(at diagnosis) and it was primarily defined using the change in gender ratio between females and males at different age points. We used this age grouping, 18-35, in this manuscript; however, with further mutational testing data (Figure 1), the upper end of this age grouping might be refined to age 40 in future analyses. Independent validation of these criteria might be useful to refine or validate the upper age cutoff for this group. This age grouping is important because it is a supportive factor in identifying Likely SDH-deficient patients.
20 21
LRG SCIENCE - Treatment Responses in SDH-deficient GIST
REFERENCES1. Boikos, S. A. et al. Molecular Subtypes of KIT/PDGFRA Wild-Type Gastrointestinal Stromal Tumors: A Report From the
National Institutes of Health Gastrointestinal Stromal Tumor Clinic. JAMA Oncol 2, 922–928 (2016).2. Elston, M. S. et al. A Duodenal SDH-Deficient Gastrointestinal Stromal Tumor in a Patient With a Germline SDHB
Mutation. J Clin Endocrinol Metab 102, 1447–1450 (2017).
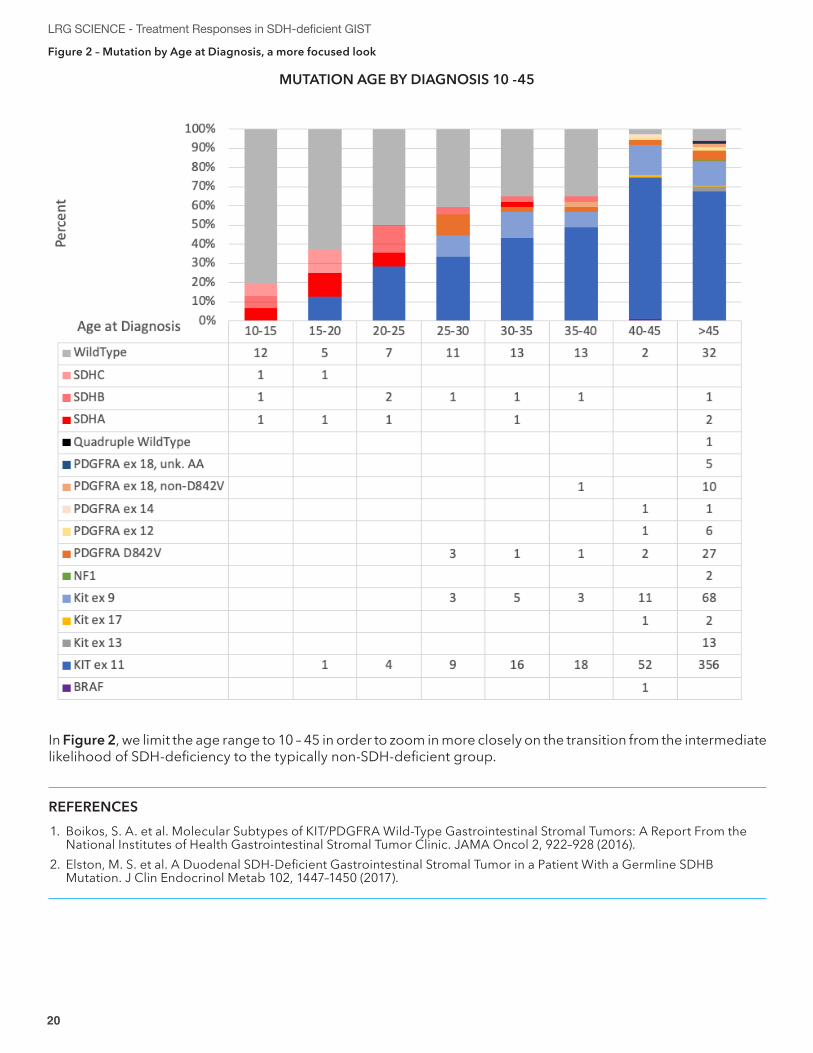
Figure 2 – Mutation by Age at Diagnosis, a more focused look
MUTATION AGE BY DIAGNOSIS 10 -45
In Figure 2, we limit the age range to 10 – 45 in order to zoom in more closely on the transition from the intermediate likelihood of SDH-deficiency to the typically non-SDH-deficient group.

20 21
LRG SCIENCE - Treatment Responses in SDH-deficient GIST
COMMENTARY SECTION
The manuscript by Call JW et al examines patient reported treatment responses from data collected by the Life Raft Group (LRG) Patient Registry in patients with succinate dehydrogenase gastrointestinal stromal tumor (SDH-deficient GIST). As reported SDH-deficient GIST is a rare sub-type of GIST representing no more than 8.7% of all the gastric GISTs reported in this series. In contrast to other forms of GIST, SDH-deficient GIST is seen in young people (more frequently in females) and in fact makes up all the cases of GIST diagnosed before the age of 20. In contrast to other retrospective series this registry is based on a robust data of patient reported treatment outcomes. A total of 1709 patients are included in the LRG data base and includes patients with all sub-types of GIST. The registry represents a unique opportunity to understand this rare form of cancer especially by using this source of patient reported assessments. A review of the literature demonstrates that patient-reported assessments are not routinely performed during treatment. When symptoms are measured, they are graded by clinicians with little patient input. The handful of studies that have specifically sought to compare patient and clinician symptom reporting have found significant differences in the rating of treatment side effects between patients and clinicians. As a result, patient-reported outcome (PRO) tools are gaining momentum for evaluation of effects during the treatment of cancers1. The LRG GIST Registry is in fact the largest patient reported treatment data base in this disease and offers an exceptional opportunity to better understand this disease in general and for the rare sub-types of this disease such as SDH-deficient GIST.In the case of SDH-deficient GIST, The LRG is able to expand the patient numbers by not only including those patients with documented SDHB loss by immune-histochemical stain or with an SDH mutation (classified as SDH-deficient “Known”) but also to include patients who meet a definition of SDH-deficient “Likely” which is defined as young patients that are KIT/PDGFRA WT or for whom mutational status is not known with multifocal stomach primaries. Patients who carry a diagnosis supportive of Carney Triad are also included in the “Likely” group. This expansion of the definition added an additional 57 “likely” patients to the SDH-deficient group and increased the patient numbers from 28 (Known) to 86 (Combined). A comparison of “known” to “likely” showed similar outcomes for patient reported progression free survival (prPFS) and for overall survival (OS). This allowed the authors to therefore examine the “combined” group for subsequent analysis, allowing for comparisons between the patients in the LRG Registry who are non-SDH-deficient GIST. This analysis shows that the SDH-deficient patients have a better OS when compared to non-SDH-deficient GIST patients but the response to imatinib as first line therapy is inferior. Because of the striking drop-off in survival for the non-SDH-deficient GIST patients following imatinib failure, survival for SDH-deficient GIST remains superior when treated with sunitinib (second line) or third line (regorafenib and beyond) therapies. However, as the authors remind us, even though the survival is superior for SDH-deficient GIST patients, it remains a formidable and fatal disease for a young patient population for whom we lack effective therapies. The LRG should most be applauded for providing evidence-based data that also includes descriptions of the symptoms and quality of life issues that patients with all types of GIST are likely to experience in the short and the long term while taking KIT-targeted therapy. In addition, the LRG has taken a leadership role in advocating for patients with SDH-deficient GIST. In particular, it helped to create the Pediatric & SDH-Deficient GIST Consortium. The aim of the consortium is to of find a cure through global collaboration. This new data set provides us further insight into this evolving field.
Gary K. Schwartz, MD, FASCOChief, Hematology and Oncology Columbia University Vagelos School of Medicine New York Presbyterian Hospital Deputy Director, Hebert Irving Comprehensive Cancer Center New York, NY 10032
1. Reeve BB, Mitchell SA, Dueck AC, et al. Recommended patient-reported core set of symptoms to measure in adult cancer treatment trials. J Natl Cancer Inst. 2014;106(7).
22 23
LRG SCIENCE - Treatment Responses in SDH-deficient GIST
The Life Raft Group has to be congratulated on this manuscript, presenting collected experience with GIST patients whose tumors have been shown to be SDH-deficient or are suspected so. I would like to take the opportunity to add some thoughts and comments on this rare issue.Interestingly, the clinical course may be indolent as well as very aggressive which underlines the fact that we have not yet fully understood what finally drives these tumors.With respect to treatment options, many physicians will likely follow the general recommendations for treatment of advanced GIST. However, given the fact that SDH-deficient GIST generally does not harbour activating mutations for KIT or PDGFR, we personally do not recommend the use of imatinib, since there is no molecular basis for efficacy and also no formal proof of activity. Prolonged disease stabilization, if seen in these patients, cannot be attributed to treatment unless the disease has been shown to progress prior to starting any therapy.Sunitinib and regorafenib are multi-targeted kinase inhibitors and have a much broader mechanisms of action. In one of our current patients with SDH-deficient GIST, a young lady in her early twenties, deep molecular sequencing has revealed a massive overexpression of FGF4 (fibroblast growth factor 4). This leads to an activation of the FGF/FGFR pathway and could therefore be targeted by an FGFR inhibitor. Regorafenib is known to also inhibit this receptor kinase which could be the explanation, that our patient derived substantial and prolonged benefit from regorafenib treatment. When she finally progressed, we switched to lenvatinib, which is an even more potent inhibitor of FGFR and could achieve another response in the patient´s GIST.Interestingly, the subgroup analysis of the GRID study (regorafenib vs. placebo in refractory GIST) has shown the best efficacy for regorafenib in patients with exon 11 mutated GIST and SDH-deficient GIST, respectively1.Recently, it has been shown that SDH-deficient GIST may harbour NTRK fusions. Under such circumstances, treatment with an NTRK inhibitor like larotrectinib or entrectinib is associated with a nearly 100% chance of success. We therefore strongly recommend deep molecular sequencing for all of these patients as a standard of care.Finally, the rarity of this disease and the complex treatment consideration make it absolutely mandatory that these patients are seen and treated by GIST experts.
Peter Reichardt, MD, PhDHelios Klinikum Berlin-Buch, Sarcoma Center Berlin-Brandenburg Berlin, Germany
1. Demetri G, Reichardt P, Kang, Y, Blay, J, Rutkowski, P, Gelderblom, H et al. Efficacy and safety of regorafenib for advanced gastrointestinal stromal tumours after failure of imatinib and sunitinib (GRID): an international, multicentre, randomised, placebo-controlled, phase 3 trial. Nov 2012, DOI:https://doi.org/10.1016/S0140-6736(12)61857-1.
In this issue of LRG Science, the article “Treatment Responses in SDH-deficient GIST” provides some new perspectives:
• For the first time the real-world effectiveness of approved therapies in these patients who make up 10% of all GIST is described
• Also addressed is the challenge of the rarity and the natural course this GIST mutation type presents management and research. This challenge that can be met by finding, studying, and treating more patients who today may not have a complete GIST diagnosis.
• A simple algorithm is presented that can help identify patients with this form of GIST to begin to further address these issues.
In comparing SDH-deficient GIST to the much more familiar and ten times more common KIT/PDGFRa mutant GIST this paper fills a drawer full of adjectives including: rare, undiagnosed, unpredictable, chronic, syndromic and unresponsive to approved therapy.
continued on next page
22 23
LRG SCIENCE - Treatment Responses in SDH-deficient GIST
We can add that SDH-deficient GIST is also:Incurable - Surgery can cure small KIT/PDGFRa GISTs. Surgical management of SDH-deficient GIST is different. Neoadjuvant therapy with Imatinib probably won’t work. A goal is to minimize comorbidity. Complete gastrectomy’s are not recommended if they can be avoided. Complete tumor removal may not confer a risk advantage. Unique - SDH is an entirely different oncogene. KIT/PDGFRa mutations cause a tyrosine kinase to constantly signal at the cell surface. SDH mutations result in a loss-of-function of an enzyme complex affecting cell metabolism resulting in the loss of tumor suppressors in the cell. SDH complex disruption is characterized by profoundly different gene expression in these GIST cells. Complex - SDH-deficient GIST management is further complicated by the historically distinct management specialties that may be required over the course of a patient’s disease. Younger patients may bridge the Pediatric/Adult surgery and oncology worlds. SDH-deficient GIST will likely require oncologists and surgeons who specialize in Sarcoma. Paragangliomas may require a Neuroendocrinologist. Germline mutations may require a Geneticist. Translational – SDH-deficient GIST has no approved targeted therapies. Outside surgery there are limited clinical trial options … currently two … one on each coast.To address these challenges The Life Raft Group has organized an SDH-deficient GIST consortium to move research forward.
Addressing the usage of the word ‘indolent’One adjective used here and in the literature for comparing SDH-deficient GIST… and before that Wild-Type GIST to GIST in general…is indolent. Is it really a useful adjective in this context? The adjective indolent is originally derived from the Latin ‘in dolens’ meaning ‘causing no pain’. Later indolent acquired the meaning lazy or idle. The NCI Dictionary of Cancer Terms describes indolent as “A type of cancer that grows slowly” borrowing from the later more pejorative meaning and not the Latin root. Somehow, this seems off-key especially when considering the SDH-deficient patients who have reached out to The Life Raft Group for support. In almost all cases these are not patients who are “without pain.” Many are managing either an aggressive disease or a massive tumor load. They are typically dealing with the after-effects of multiple surgeries and the side effects of drugs of questionable efficacy. And they have much higher rates of recurrence.The literature includes reports that would also seem to contrast with this characterization. One notes the high rate of metastatic disease and unpredictable course. Mason & Hornick in Am J Surg Pathol. 2016 Dec;40(12):1616-1621.Another notes the difficulty in comparing two forms of GIST with distinctly different natural histories. Weldon J Clin Oncol. 2017 Feb 10;35(5):523-528.For those patients who have died and for their caregivers this is not an indolent disease. Perhaps a better use context a better use for the adjective indolent would be for micro-GISTs.
Jim HughesFather of SDH-deficient GIST patient Nancy Hughes Welsh (1967-2005)Member of the Life Raft Group Board of Directors
155 US Highway 46, Suite 202 Wayne, NJ 07470 973-837-9092
fax 973-837-9095 www.liferaftgroup.org
LRG ScIence is intended to highlight articles created by data collected from: The LRG Patient Registry, SideEQ, Project Surveillance, and our collaborative efforts, such as the Pediatric & SDH-Deficient GIST Consortium. It will also include content and commentary from GIST experts, case studies, editorials on vital issues and breaking news. LRG Science is based on a foundation of Real World Evidence and Real World Data.
To inquire about authoring an LRG SCIENCE article, providing commentary on an article, or to subscribe to our LRG SCIENCE mailing list, please contact [email protected]
Patient Powered Real World Evidence