
Pump Work: The “ C ” in CPR: Evidence on Epinephrine and Chest Compressions Myra H. Wyckoff, MD...
58
Pump Work: The “C” in CPR: Evidence on Epinephrine and Chest Compressions Myra H. Wyckoff, MD Associate Professor of Pediatrics UT Southwestern Medical Center at Dallas
-
Upload
brittany-robertson -
Category
Documents
-
view
218 -
download
2
Transcript of Pump Work: The “ C ” in CPR: Evidence on Epinephrine and Chest Compressions Myra H. Wyckoff, MD...
Pump Work: The “C” in CPR: Evidence on Epinephrine and Chest
CompressionsMyra H. Wyckoff, MD
Associate Professor of Pediatrics
UT Southwestern Medical Center at Dallas
Disclosures
I am not on any speakers bureaus
I do not intend to discuss unapproved uses of a commercial product
I received a manikin from Laerdal for cardiac compression research
I have a translational research grant funded by Ikaria
Audience Response Question
In the past year, have you been in the delivery room when chest compressions were administered to a newborn?
1=Yes
2=No
Goal of Compressions
Generate sufficient O2 delivery to the coronary and cerebral circulation while waiting for a definitive restoration of a cardiac rhythm by pharmacologic intervention (such as Epi)
Coronary perfusion is a determinant of return of spontaneous circulation (ROSC) and cerebral perfusion is a determinant of neurologic outcome
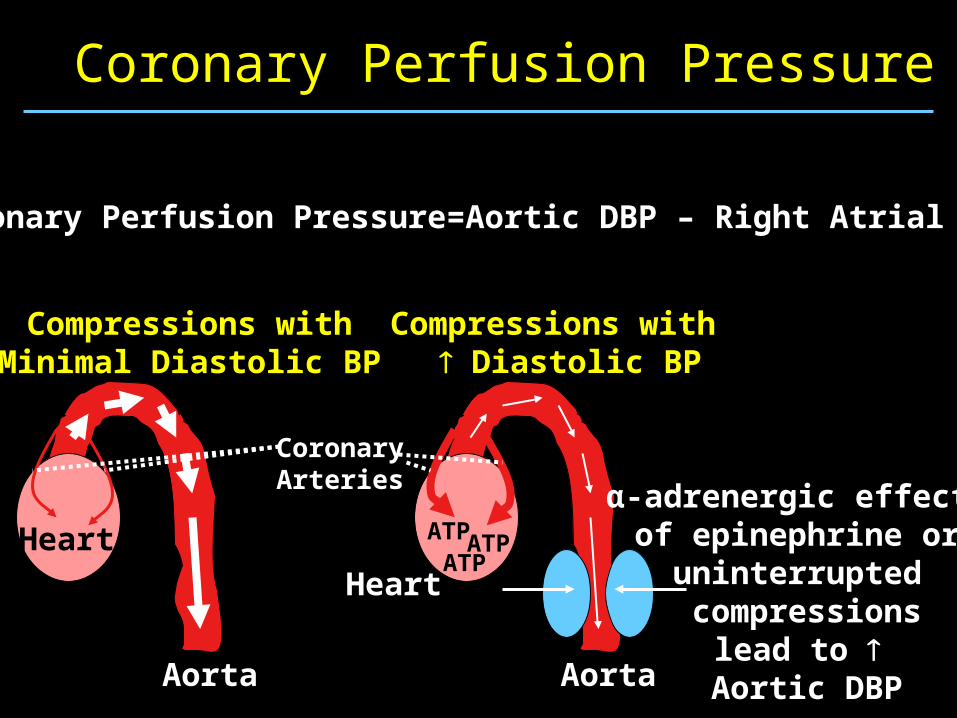
Compressions withMinimal Diastolic BP
Aorta
Heart
Compressions with Diastolic BP
Aorta
Heart
Coronary Perfusion Pressure
ATPATP
ATPα-adrenergic effects
of epinephrine or uninterrupted compressions
lead to Aortic DBP
CoronaryArteries
Coronary Perfusion Pressure=Aortic DBP – Right Atrial DBP
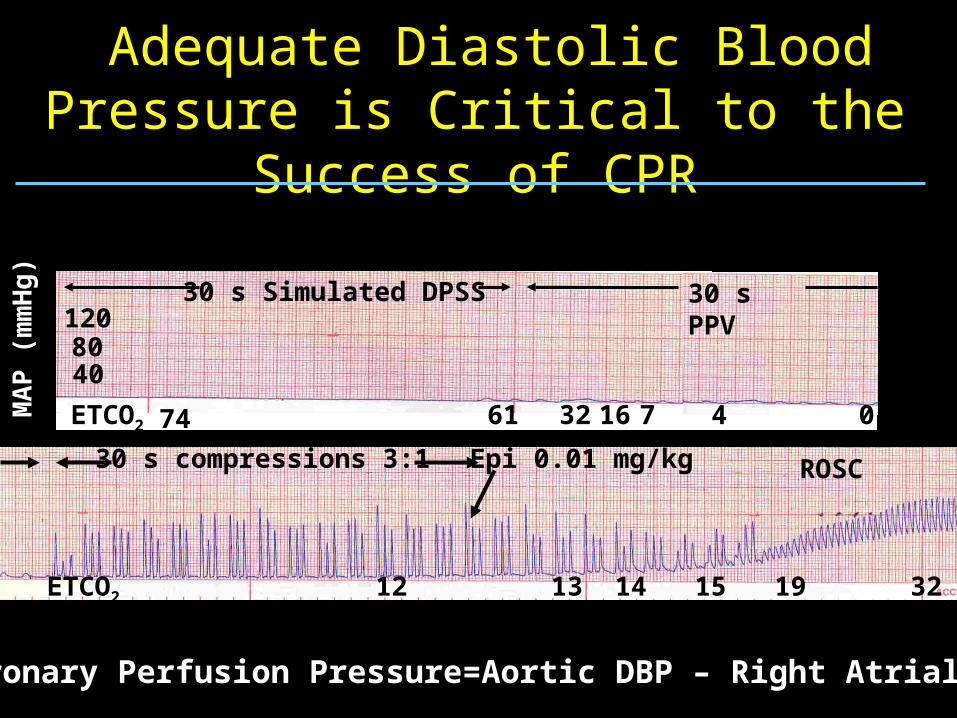
Adequate Diastolic Blood Pressure is Critical to the Success of CPR
ETCO2 74 61 1632 47 0MA
P (
mm
Hg
)
4080120
30 s Simulated DPSS 30 s PPV
12
Epi 0.01 mg/kg
13 14 15 19 32
30 s compressions 3:1 ROSC
ETCO2
Coronary Perfusion Pressure=Aortic DBP – Right Atrial DBP
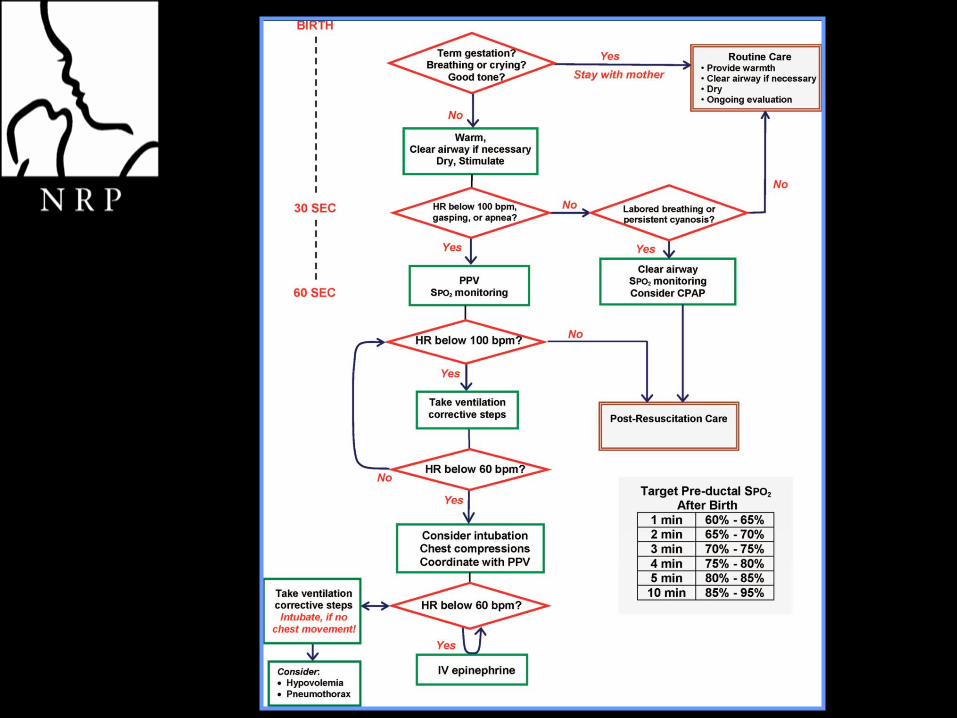
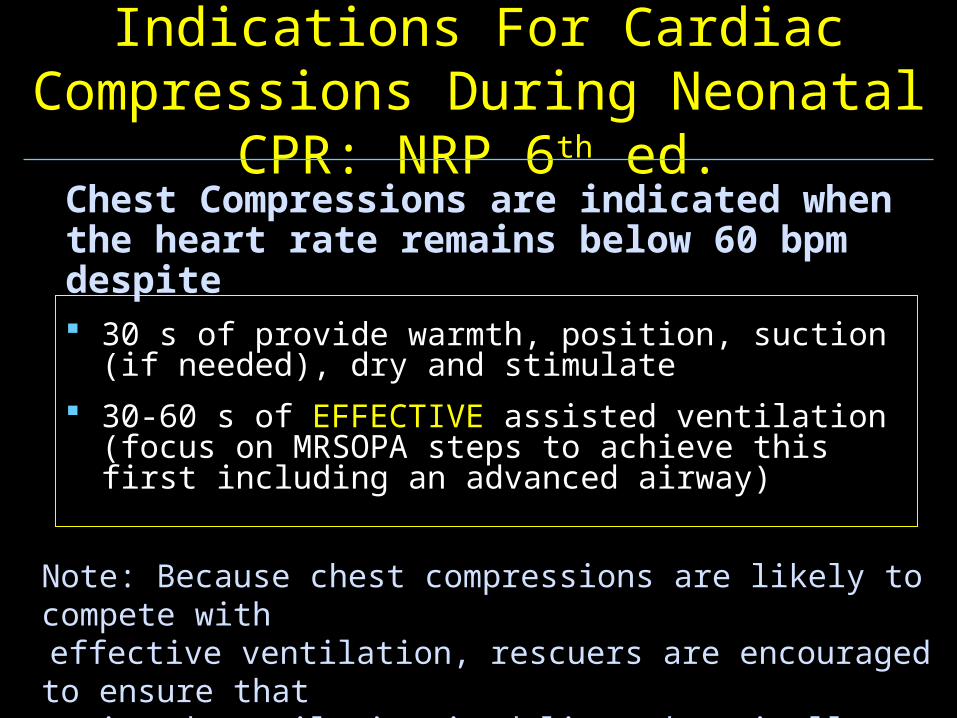
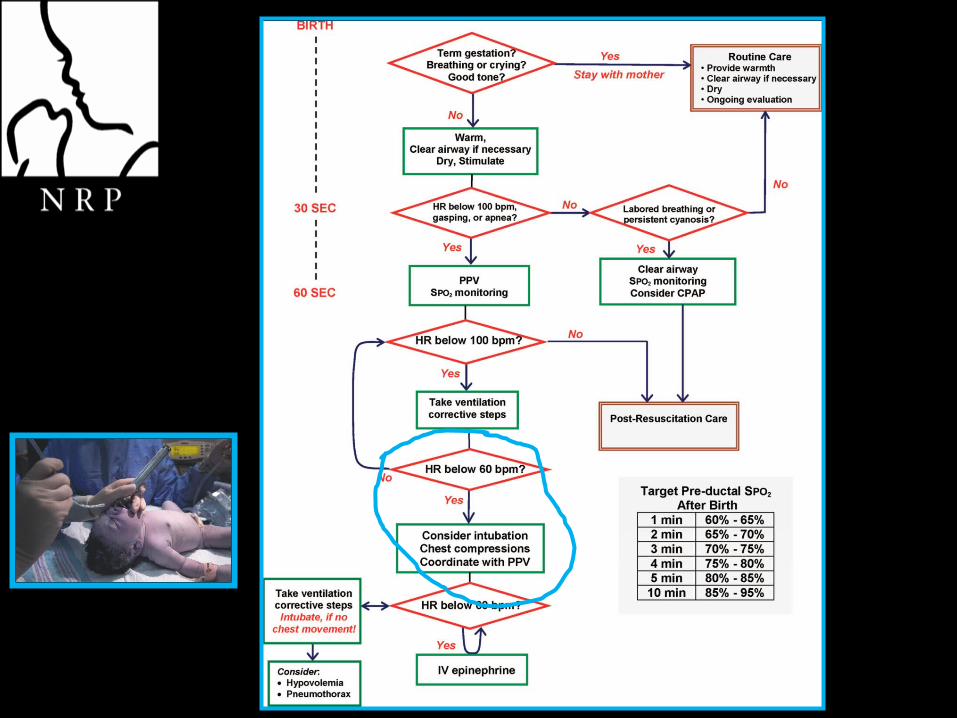
Indications For Cardiac Compressions During Neonatal CPR: NRP 6th ed.
30 s of provide warmth, position, suction (if needed), dry and stimulate
30-60 s of EFFECTIVE assisted ventilation (focus on MRSOPA steps to achieve this first including an advanced airway)
Chest Compressions are indicated when the heart rate remains below 60 bpm despite
Note: Because chest compressions are likely to compete with effective ventilation, rescuers are encouraged to ensure that assisted ventilation is delivered optimally BEFORE initiation of chest compressions
Copyright ©2010 American Academy of Pediatrics
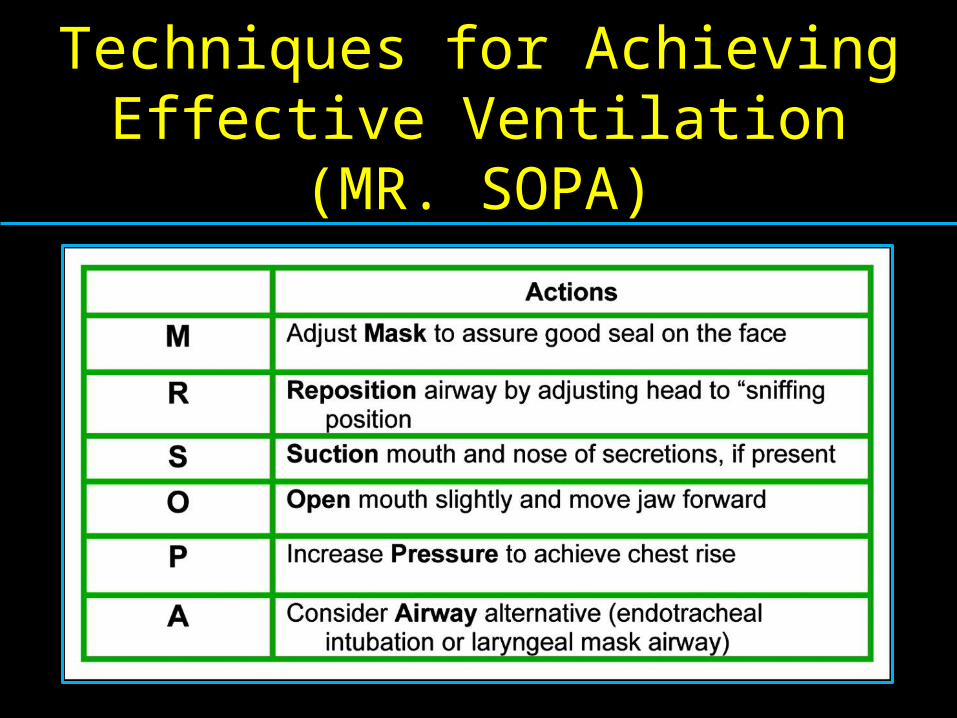
Mnemonic for remembering the six steps for improving efficacy of positive-pressure
ventilation
Techniques for Achieving Effective Ventilation
(MR. SOPA)
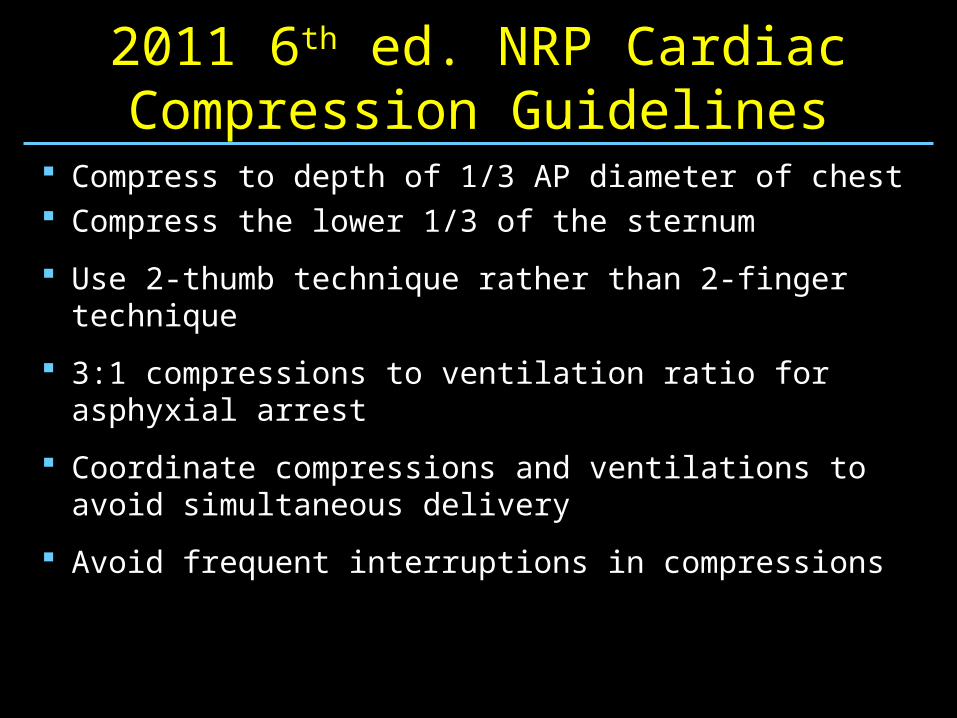
2011 6th ed. NRP Cardiac Compression Guidelines
Compress to depth of 1/3 AP diameter of chest Compress the lower 1/3 of the sternum
Use 2-thumb technique rather than 2-finger technique
3:1 compressions to ventilation ratio for asphyxial arrest
Coordinate compressions and ventilations to avoid simultaneous delivery
Avoid frequent interruptions in compressions
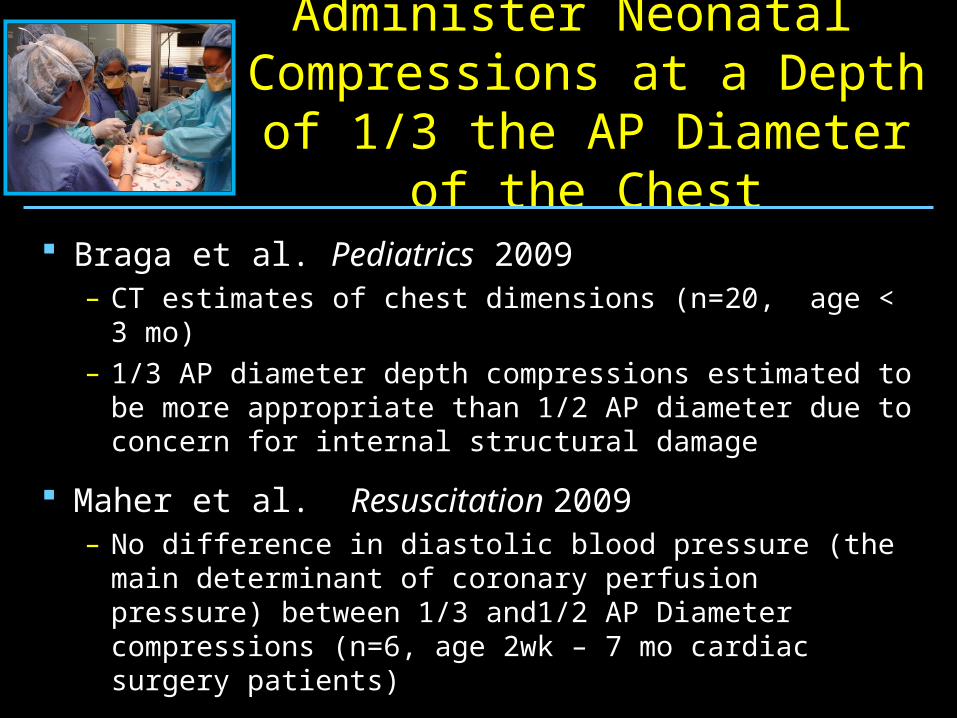
Administer Neonatal Compressions at a Depth of 1/3 the AP Diameter of the Chest
Braga et al. Pediatrics 2009– CT estimates of chest dimensions (n=20, age < 3 mo)– 1/3 AP diameter depth compressions estimated to be
more appropriate than 1/2 AP diameter due to concern for internal structural damage
Maher et al. Resuscitation 2009– No difference in diastolic blood pressure (the main
determinant of coronary perfusion pressure) between 1/3 and1/2 AP Diameter compressions (n=6, age 2wk – 7 mo cardiac surgery patients)
Administer Compressions at a Depth of 1/3 the AP Diameter
of the Chest
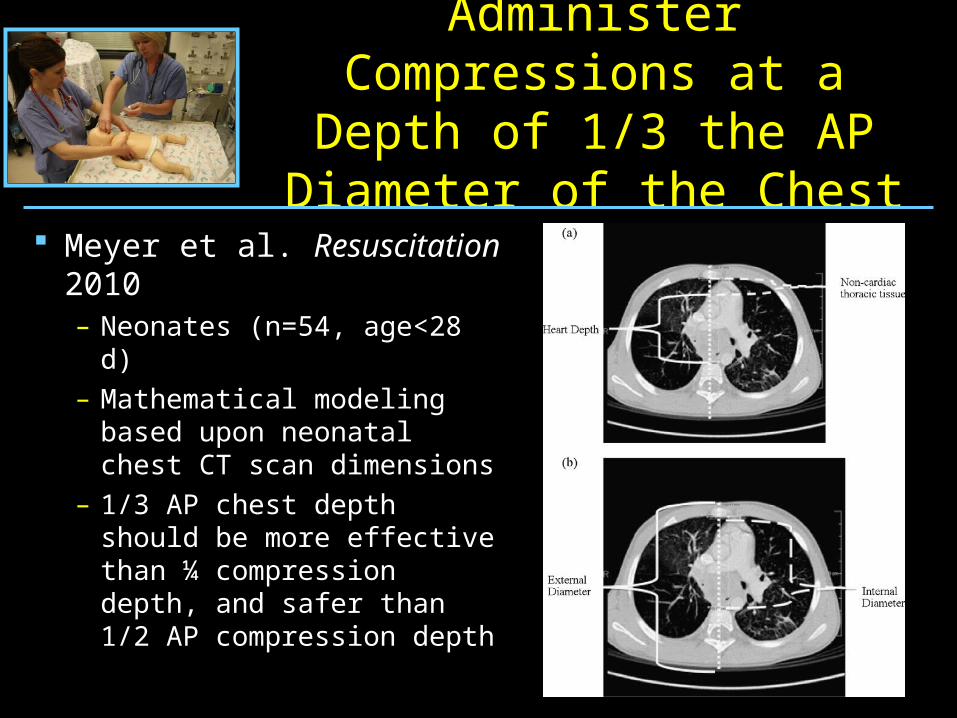
Meyer et al. Resuscitation 2010– Neonates (n=54, age<28 d)– Mathematical modeling
based upon neonatal chest CT scan dimensions
– 1/3 AP chest depth should be more effective than ¼ compression depth, and safer than 1/2 AP compression depth
Administer Neonatal Compressions Over Lower
1/3 of Sternum
Orlowski et al. Ann Emerg Med 1986– Heart lies under lower 1/3 of sternum in > 67% of
children (n=187, age < 17yrs ) as noted on CXR– Significantly better MAP achieved with compressions
administered over lower 1/3 compared to mid sternum (n=10, age 1 mo – 3 yrs).
Philips et al. Lancet 1986– Heart under lower 1/3 of sternum in 87% of infants
(n=55, age 27 wks EGA - 13 mo post-term)
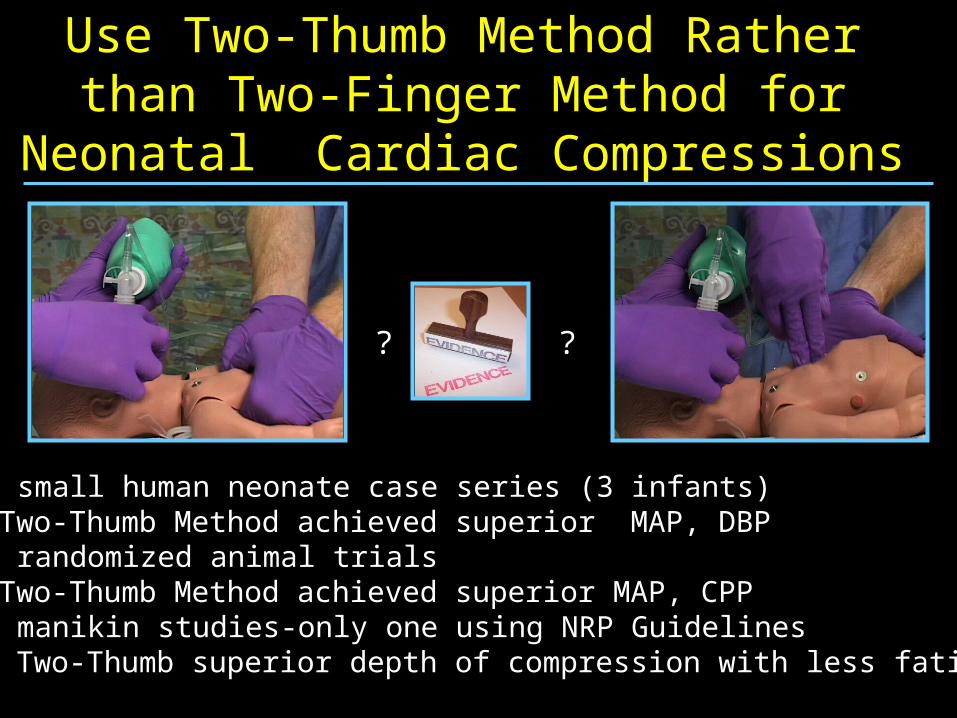
Use Two-Thumb Method Rather than Two-Finger Method for Neonatal Cardiac
Compressions
2 small human neonate case series (3 infants)—Two-Thumb Method achieved superior MAP, DBP
2 randomized animal trials—Two-Thumb Method achieved superior MAP, CPP
3 manikin studies-only one using NRP Guidelines— Two-Thumb superior depth of compression with less fatigue
? ?
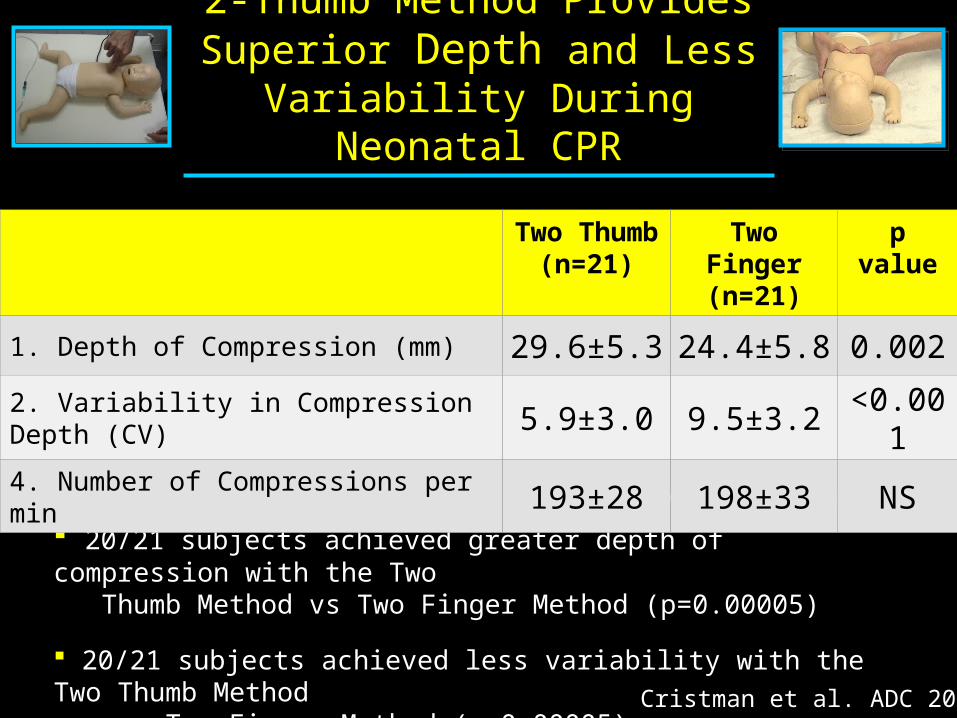
2-Thumb Method Provides Superior Depth and Less
Variability During Neonatal CPR
Coefficient of Variation (CV) = standard deviation/mean *100
20/21 subjects achieved greater depth of compression with the Two Thumb Method vs Two Finger Method (p=0.00005)
20/21 subjects achieved less variability with the Two Thumb Method vs Two Finger Method (p=0.00005)
Cristman et al. ADC 2011
Two Thumb(n=21)
Two Finger(n=21)
p value
1. Depth of Compression (mm) 29.6±5.3 24.4±5.8 0.0022. Variability in Compression Depth (CV) 5.9±3.0 9.5±3.2 <0.0014. Number of Compressions per min 193±28 198±33 NS
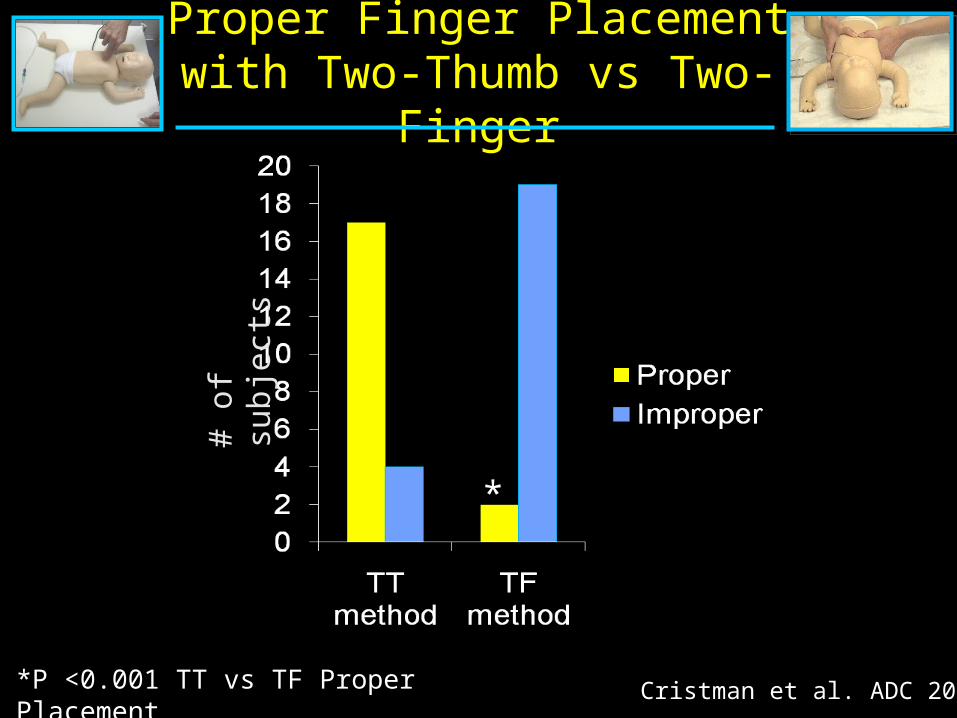
Proper Finger Placement with Two-Thumb vs Two-Finger
*P <0.001 TT vs TF Proper Placement
# of
sub
ject
s
*
Cristman et al. ADC 2011
Sounds good but….. Won’t the two-finger technique be needed
at least briefly so that the compressors hands are not blocking access to the umbilical cord for emergent umbilical venous line placement?
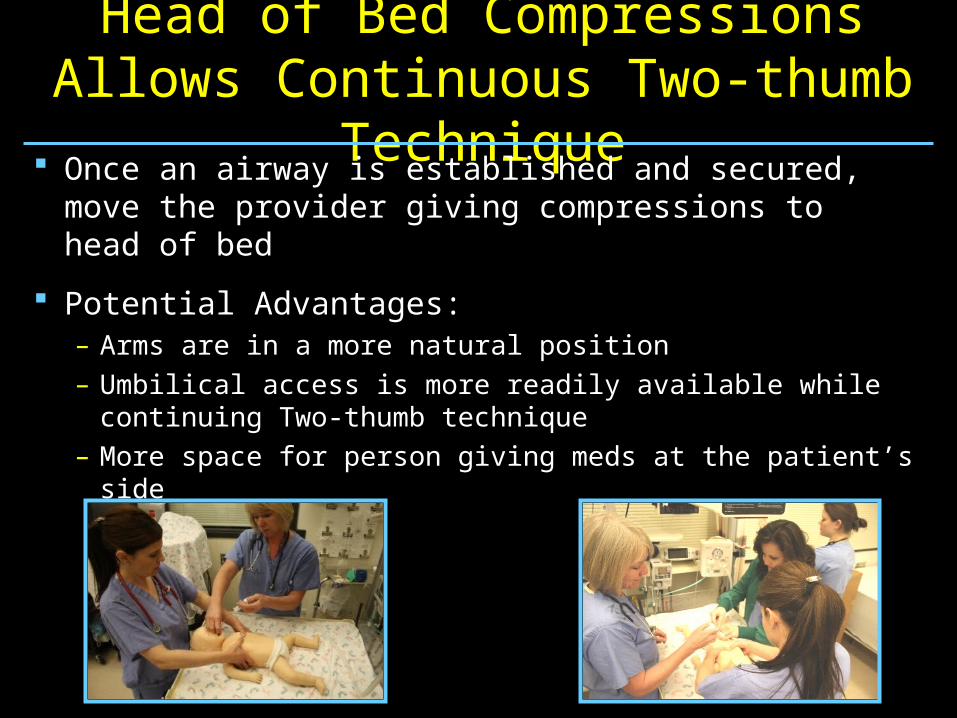
Head of Bed Compressions Allows Continuous Two-thumb Technique
Once an airway is established and secured, move the provider giving compressions to head of bed
Potential Advantages:– Arms are in a more natural position– Umbilical access is more readily available while
continuing Two-thumb technique– More space for person giving meds at the patient’s side
Audience Response Question
In the past year, have you been practicing delivering compressions from the head of the bed?
1=Yes
2=No
Audience Response Question
For those that have been practicing or actually performing giving compressions from the head of the bed…have you found this technique helpful?
1=Yes
2=No
3=Undecided
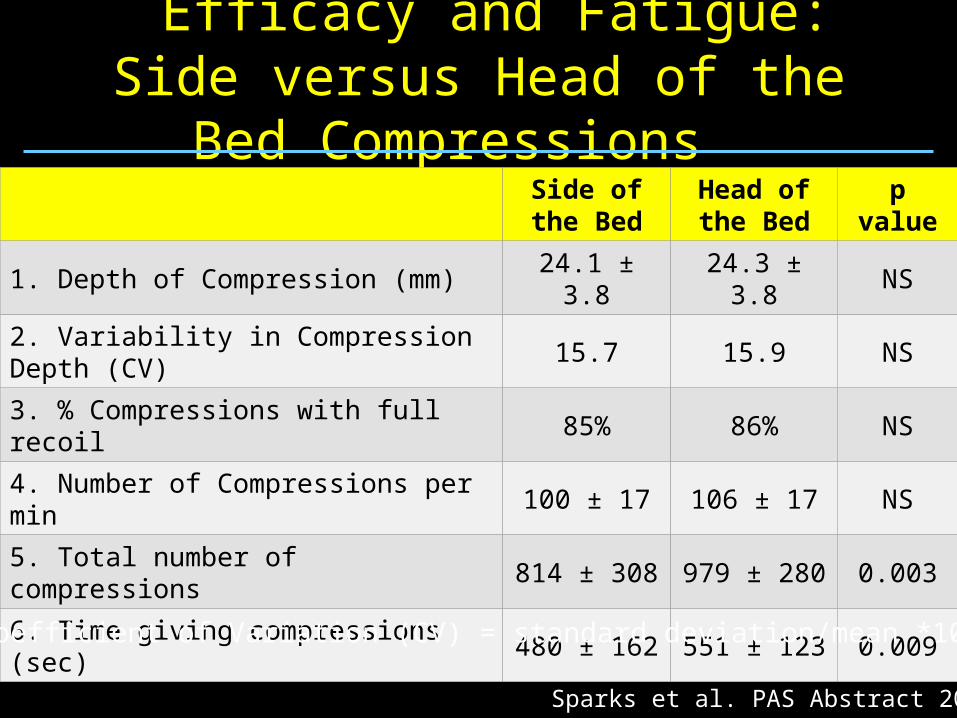
Efficacy and Fatigue: Side versus Head of the Bed Compressions
Side of the Bed
Head of the Bed
p value
1. Depth of Compression (mm) 24.1 ± 3.8 24.3 ± 3.8 NS
2. Variability in Compression Depth (CV) 15.7 15.9 NS
3. % Compressions with full recoil 85% 86% NS
4. Number of Compressions per min 100 ± 17 106 ± 17 NS
5. Total number of compressions 814 ± 308 979 ± 280 0.003
6. Time giving compressions (sec) 480 ± 162 551 ± 123 0.009
Coefficient of Variation (CV) = standard deviation/mean *100
Sparks et al. PAS Abstract 2011
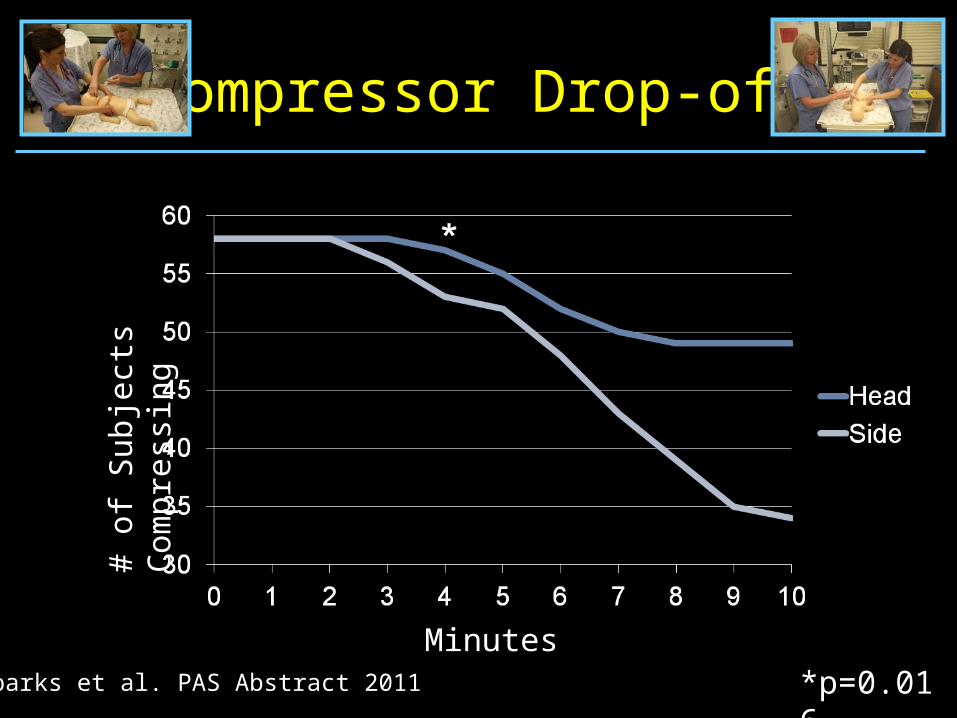
Compressor Drop-off
*p=0.016
# of
Sub
ject
s C
ompr
essi
ng
MinutesSparks et al. PAS Abstract 2011
What is the Optimal Compression to Ventilation Ratio For Neonatal
CPR?
In Adult V-fib Cardiac Arrest…
Immediately after the cardiac arrest:– Aortic oxygen and carbon dioxide concentrations are
close to pre-arrest state– When compressions are initiated, this is the blood that
will be flowing to the coronaries – The problem is the lack of flow and not so much the
content of the blood
Ventilation from chest compressions and gasping seems to provide adequate ventilation and oxygenation for resuscitation in the short term
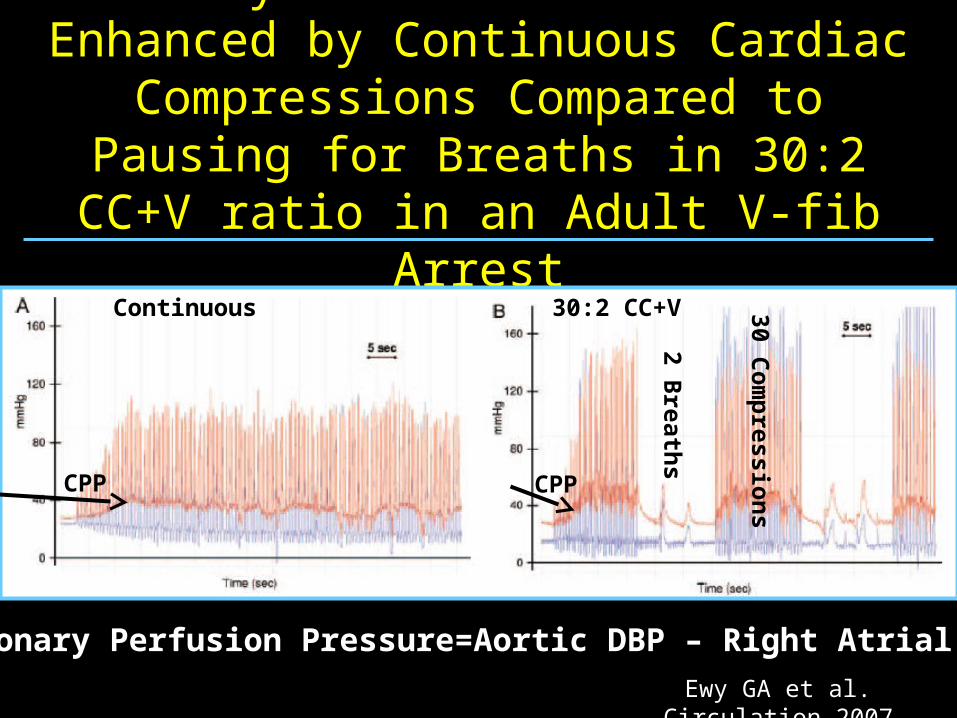
Coronary Perfusion Pressure is Enhanced by Continuous Cardiac Compressions
Compared to Pausing for Breaths in 30:2 CC+V ratio in an Adult V-fib Arrest
Ewy GA et al. Circulation 2007
Continuous 30:2 CC+V
Coronary Perfusion Pressure=Aortic DBP – Right Atrial DBP
2 Breath
s
CPP CPP
30 Co
mp
ression
s
Asphyxia-induced Cardiac Arrest is Different…..
At arrest, there is significant hypoxemia, hypercarbia, and acidemia
This promotes maximal systemic vasodilation and very low diastolic blood pressure
Piglet studies of CPR for asphyxial arrests show that in addition to compressions rescue breathing is critical to achieve return of spontaneous circulation
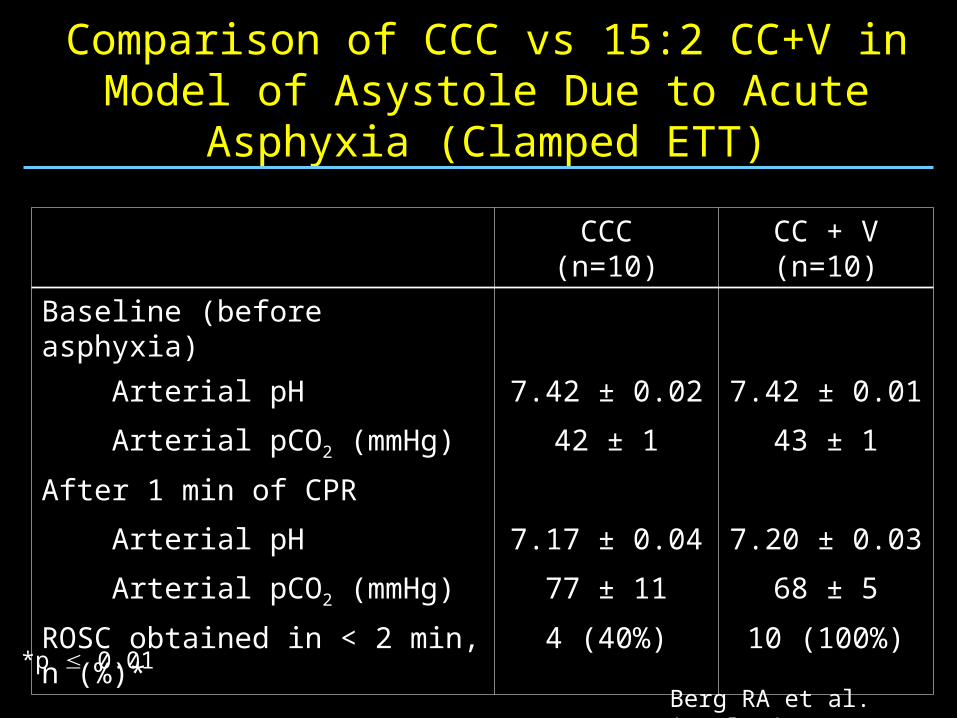
Comparison of CCC vs 15:2 CC+V in Model of Asystole Due to Acute Asphyxia (Clamped ETT)
CCC(n=10)
CC + V(n=10)
Baseline (before asphyxia)
Arterial pH 7.42 ± 0.02 7.42 ± 0.01
Arterial pCO2 (mmHg) 42 ± 1 43 ± 1
After 1 min of CPR
Arterial pH 7.17 ± 0.04 7.20 ± 0.03
Arterial pCO2 (mmHg) 77 ± 11 68 ± 5
ROSC obtained in < 2 min, n (%)* 4 (40%) 10 (100%)
Berg RA et al. Circulation 2000
*p 0.01
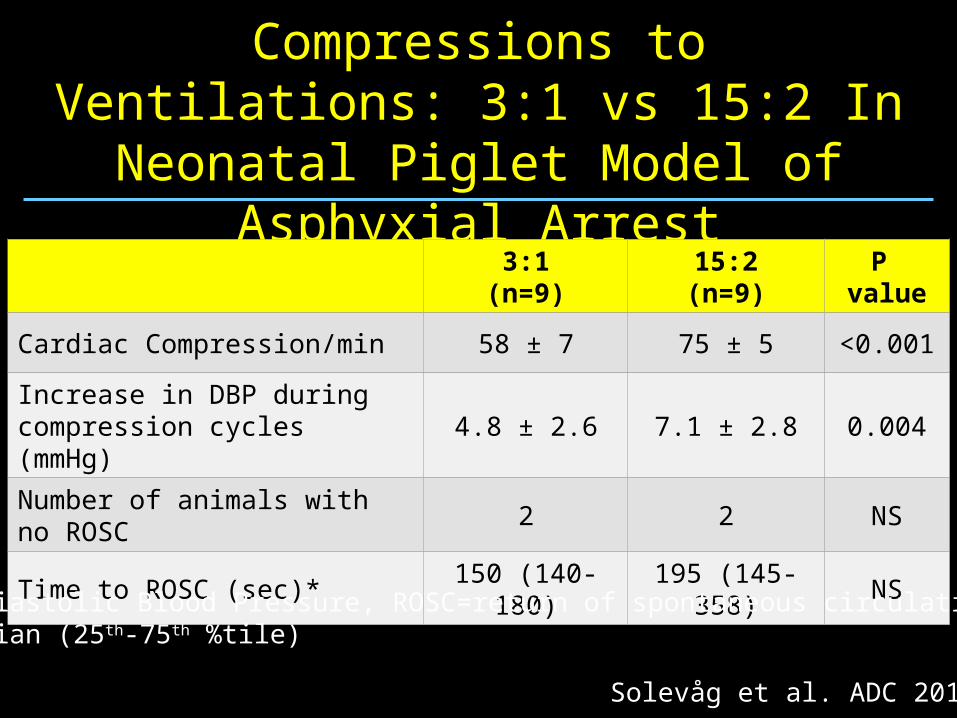
Extended Series of Compressions to Ventilations: 3:1 vs 15:2 In Neonatal
Piglet Model of Asphyxial Arrest
3:1(n=9)
15:2(n=9)
P value
Cardiac Compression/min 58 ± 7 75 ± 5 <0.001
Increase in DBP during compression cycles (mmHg)
4.8 ± 2.6 7.1 ± 2.8 0.004
Number of animals with no ROSC
2 2 NS
Time to ROSC (sec)* 150 (140-180) 195 (145-358) NS
Solevåg et al. ADC 2011
DBP=Diastolic Blood Pressure, ROSC=return of spontaneous circulation* Median (25th-75th %tile)
Should we continue to coordinate the compressions
and ventilations?
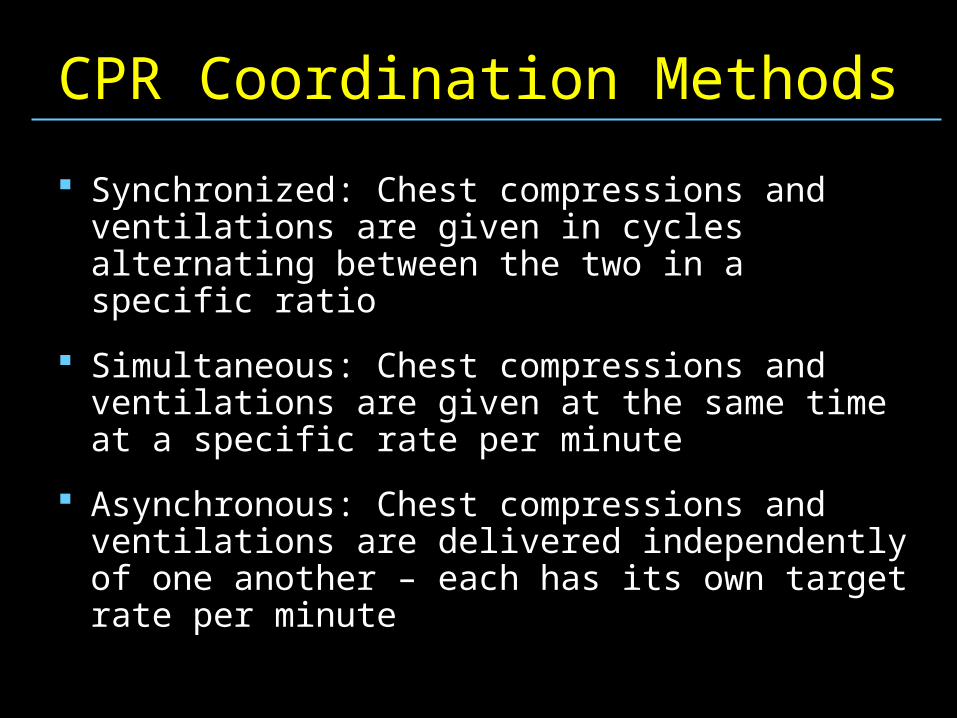
CPR Coordination Methods
Synchronized: Chest compressions and ventilations are given in cycles alternating between the two in a specific ratio
Simultaneous: Chest compressions and ventilations are given at the same time at a specific rate per minute
Asynchronous: Chest compressions and ventilations are delivered independently of one another – each has its own target rate per minute
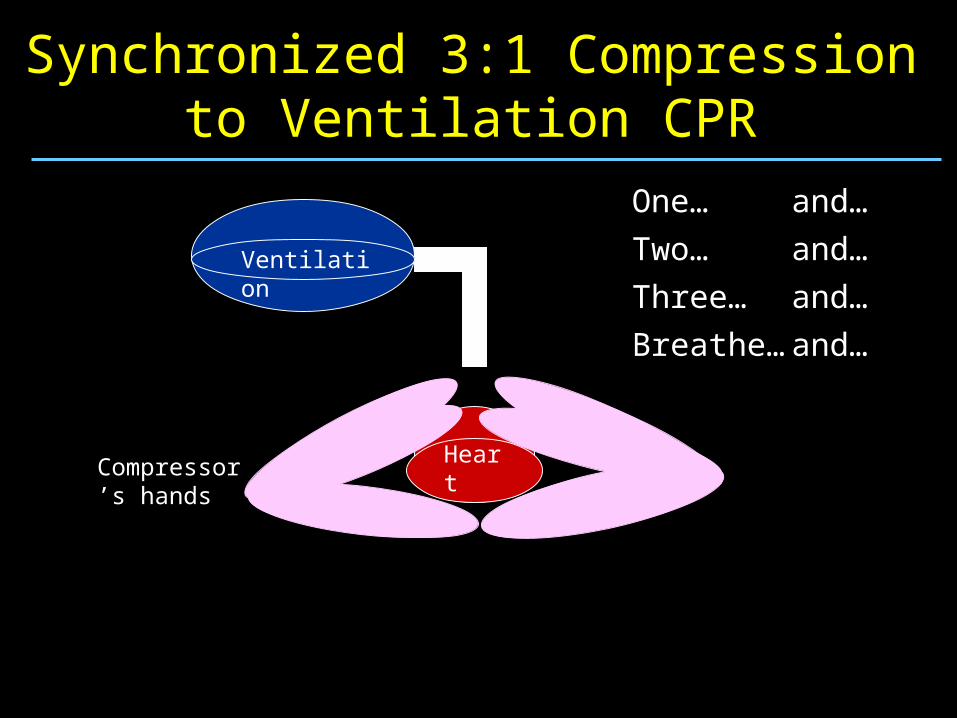
Synchronized 3:1 Compression to Ventilation CPR
One… and…
Two… and…
and…
and…Three…
Breathe…
Ventilation
HeartCompressor’s hands
Synchronized 3:1 Compression to Ventilation CPR
One… and…
Two… and…
and…
and…Three…
Breathe…
Ventilation
HeartCompressor’s hands
Simultaneous Compression and Ventilation CPR
Ventilation
HeartCompressor’s hands
Simultaneous Compression and Ventilation CPR
Ventilation
HeartCompressor’s hands
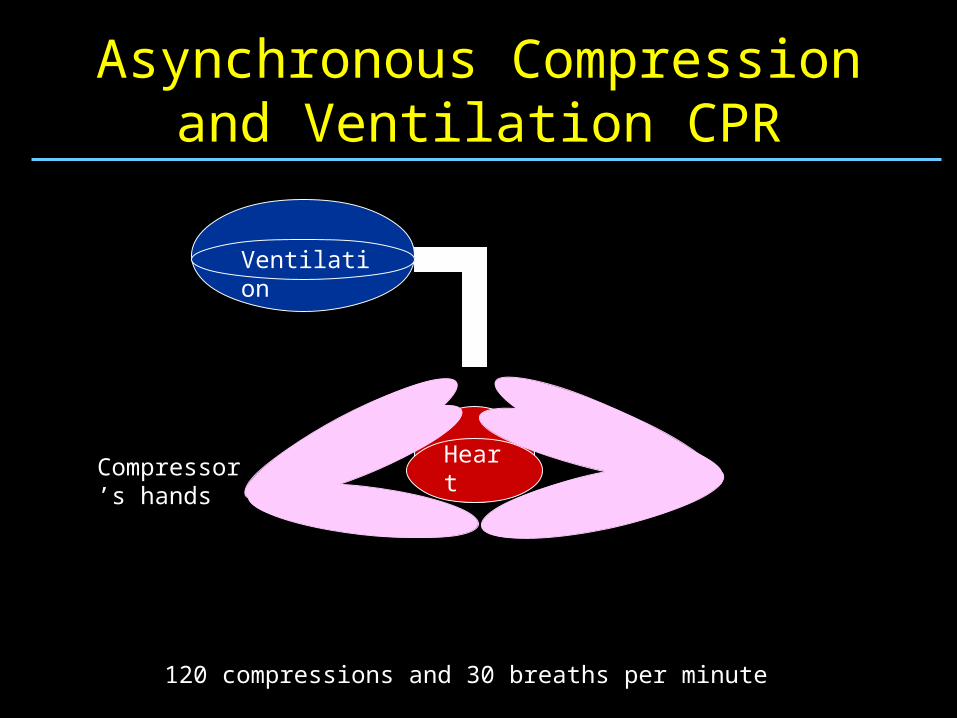
Asynchronous Compression and Ventilation CPR
Ventilation
HeartCompressor’s hands
120 compressions and 30 breaths per minute
Asynchronous Compression and Ventilation CPR
Ventilation
HeartCompressor’s hands
120 compressions and 30 breaths per minute
What Does NRP Currently Say About Asynchronization?
“Avoid giving a compression and a ventilation simultaneously, because one will decrease the efficacy of the other.”
2 activities must be coordinated, with one ventilation interposed after every third compression
Should provide a total of 30 breaths and 90 compressions per minute
What evidence is used to substantiate the current
recommendations?
Simultaneous Method – 2 Studies
Designed to look at the possibility of better cardiac output by increasing the intrathoracic pressure using simultaneous compressions and ventilations– Both use a cardiac arrest model
When compared to 5:1 synchronized compressions, simultaneous CPR:– Did not enhance cerebral and myocardial perfusion
– Resulted in higher PCO2 values raising the concern that this technique might limit ventilation
Berkowitz et al. Ped Res 1989Hou SH et al. Japan Circ J 1994
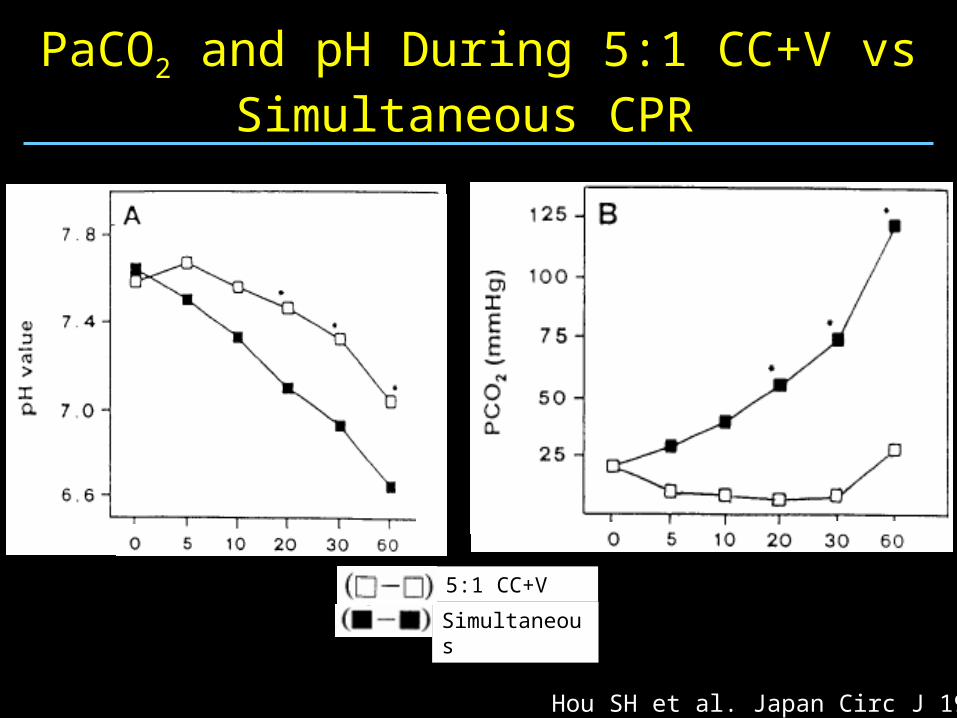
PaCO2 and pH During 5:1 CC+V vs Simultaneous CPR
5:1 CC+V
Simultaneous
Hou SH et al. Japan Circ J 1994
Limited Applicability
The simultaneous compression groups do not represent what we want to do in the DR– High PIP (60 cm H2O) for ventilations
– Compression rate of 60 bpm– Would not attempt the simultaneous events since we
are not trying to utilize higher intrathoracic pressure to enhance cardiac output
There are no published studies of asynchronous compressions in neonates or neonatal models of profound asphyxia
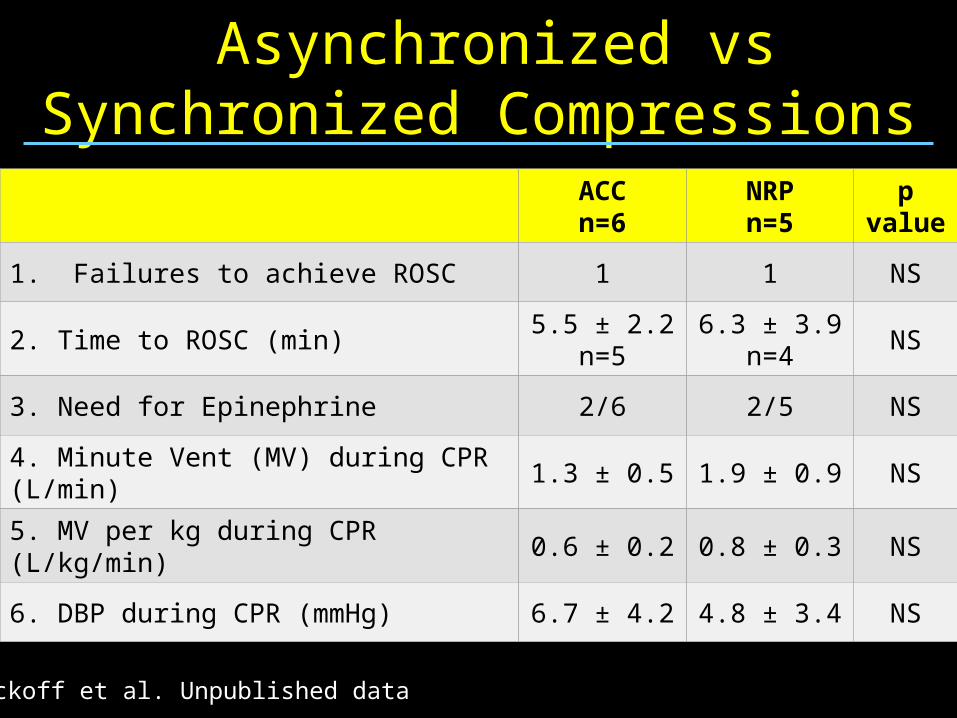
Asynchronized vs Synchronized Compressions
ACCn=6
NRPn=5
p value
1. Failures to achieve ROSC 1 1 NS
2. Time to ROSC (min)5.5 ± 2.2
n=56.3 ± 3.9
n=4NS
3. Need for Epinephrine 2/6 2/5 NS
4. Minute Vent (MV) during CPR (L/min) 1.3 ± 0.5 1.9 ± 0.9 NS
5. MV per kg during CPR (L/kg/min) 0.6 ± 0.2 0.8 ± 0.3 NS
6. DBP during CPR (mmHg) 6.7 ± 4.2 4.8 ± 3.4 NS
Wyckoff et al. Unpublished data
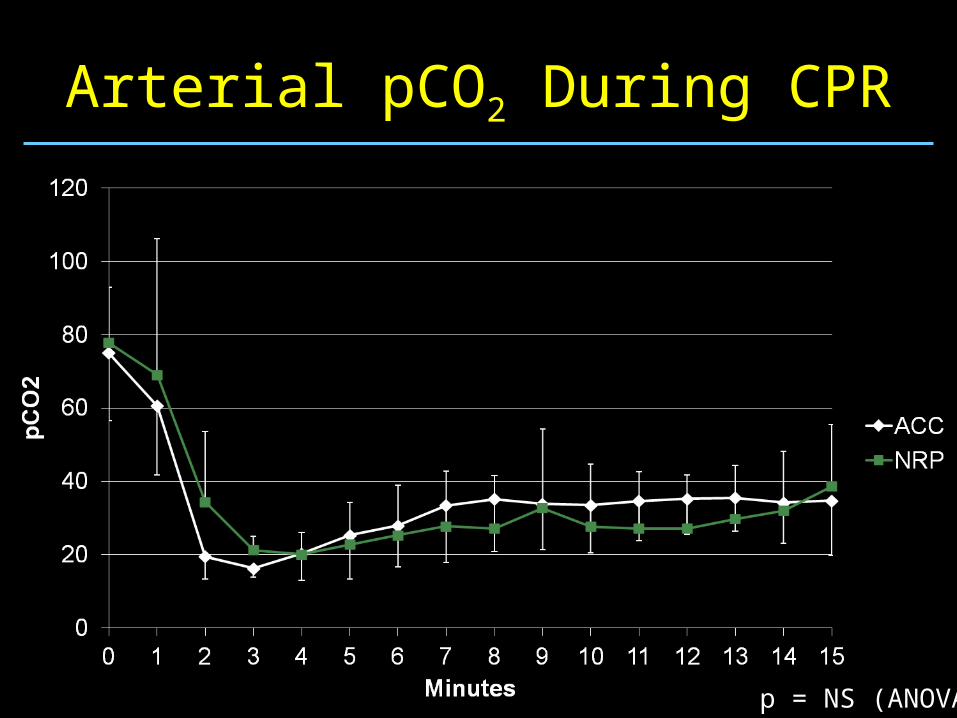
Arterial pCO2 During CPR
p = NS (ANOVA)
What can we do to interrupt compressions less?
For Starters…. Be aware of the many pauses in circulation that can inadvertently
come up during CPR and help your team stay focused on optimizing perfusion
Continue compressions for at least 45-60s before interrupting to auscultate for heart rate
If at all possible, assign the role of auscultation for heart rate to a team member that is not responsible for compressions or ventilations– Takes longer than 6 seconds to put on stethoscope to determine the
heart rate and get hands back into position
Be aware that pulse oximetry will likely not pick up during this time or the heart rate may reflect the compression rate
End-tidal CO2 (ETCO2) Monitoring During CPR
Quantitative ETCO2 monitoring is a non-invasive tool that has been shown to predict and demonstrate ROSC during experimental and human cardiac arrest
Used to monitor cardiac output and efficacy of CPR in adults where low ETCO2 levels indicate —poor cardiac output (r=0.82 Idris et al, 1994)—poor cardiac perfusion pressure (r=.91 Sanders et al, 1985)—predict low rates of ROSC (Kern et al, 1989)
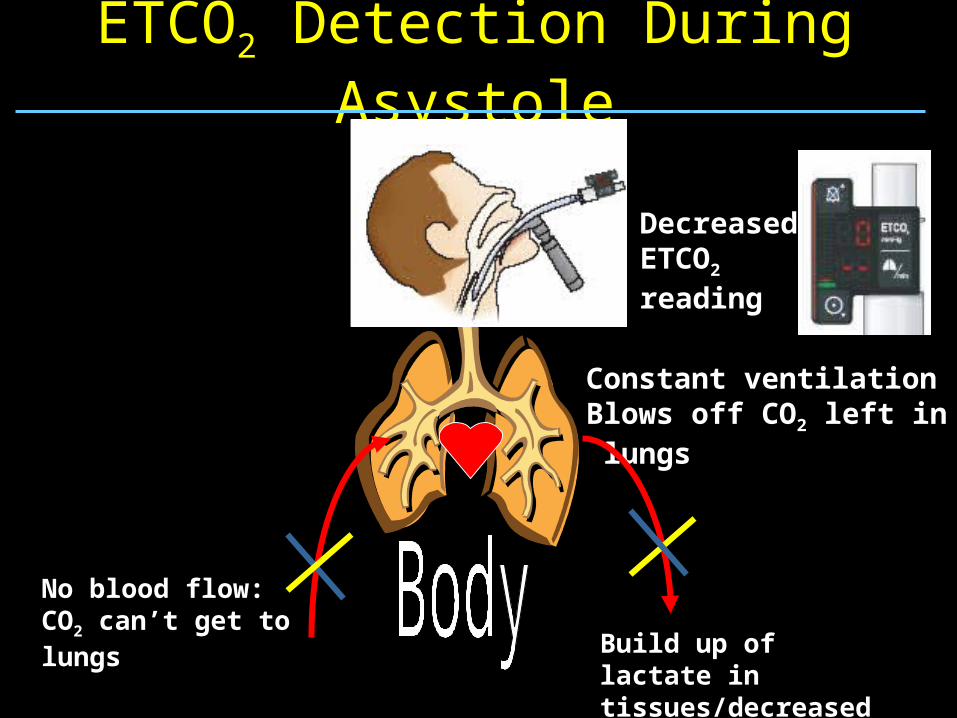
ETCO2 Detection During Asystole
No blood flow: CO2 can’t get to lungs
Constant ventilationBlows off CO2 left in lungs
Build up of lactate in tissues/decreased CO2 production
Decreased ETCO2 reading
ETCO2 Detection with Return of Spontaneous Circulation
Increased blood flow: CO2 can now get to lungs
Constant ventilationblows off CO2
Increased CO2 production in tissues
Markedly increased ETCO2 reading
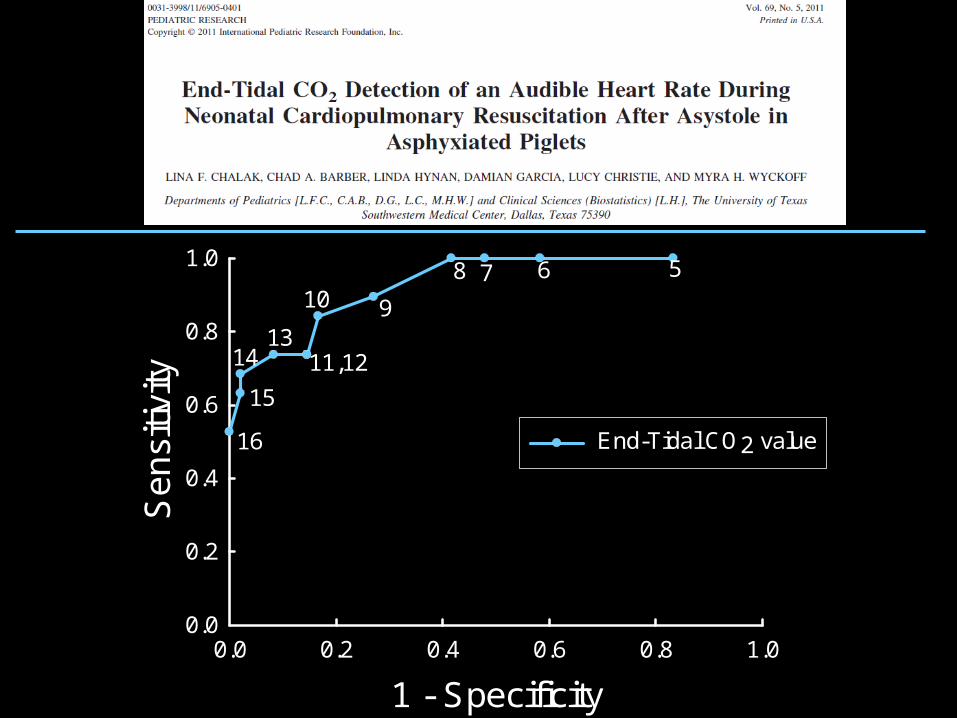
ROC Curve for ETCO2 Detection of Audible Heart Rate
1 - Specificity
0.0 0.2 0.4 0.6 0.8 1.0
Se
nsi
tivity
0.0
0.2
0.4
0.6
0.8
1.0
End-Tidal CO2 value
5678
910
11,1213
14
15
16
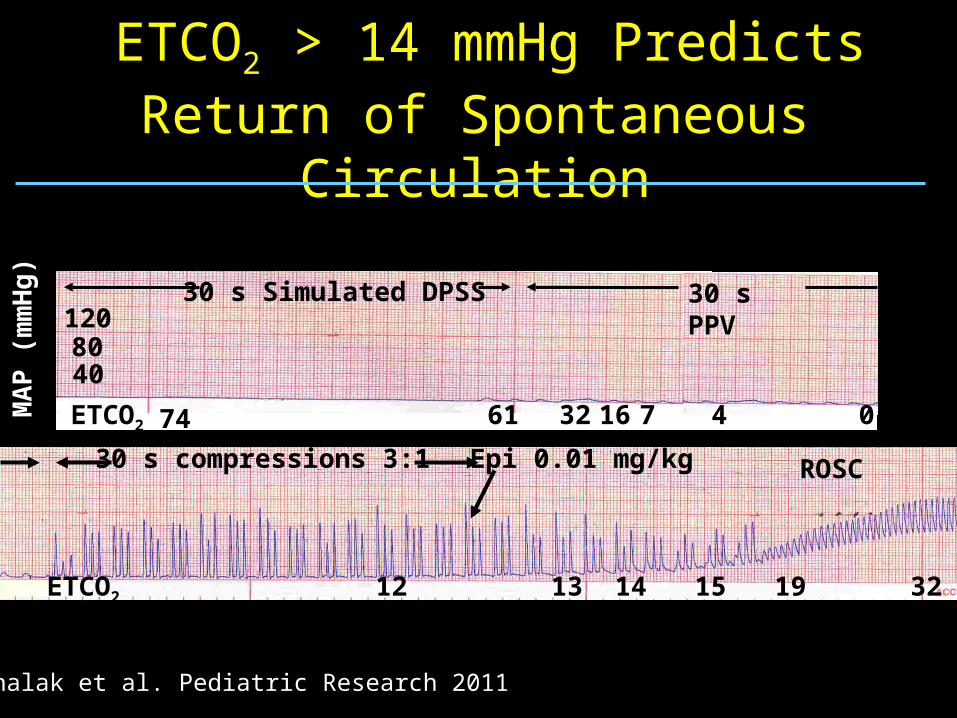
ETCO2 > 14 mmHg Predicts Return of Spontaneous Circulation
ETCO2 74 61 1632 47 0MA
P (
mm
Hg
)
4080120
30 s Simulated DPSS 30 s PPV
12
Epi 0.01 mg/kg
13 14 15 19 32
30 s compressions 3:1 ROSC
ETCO2
Chalak et al. Pediatric Research 2011
Audience Response Question
In the past year, have you been in the delivery room when epinephrine was given to a newborn?
1=Yes
2=No
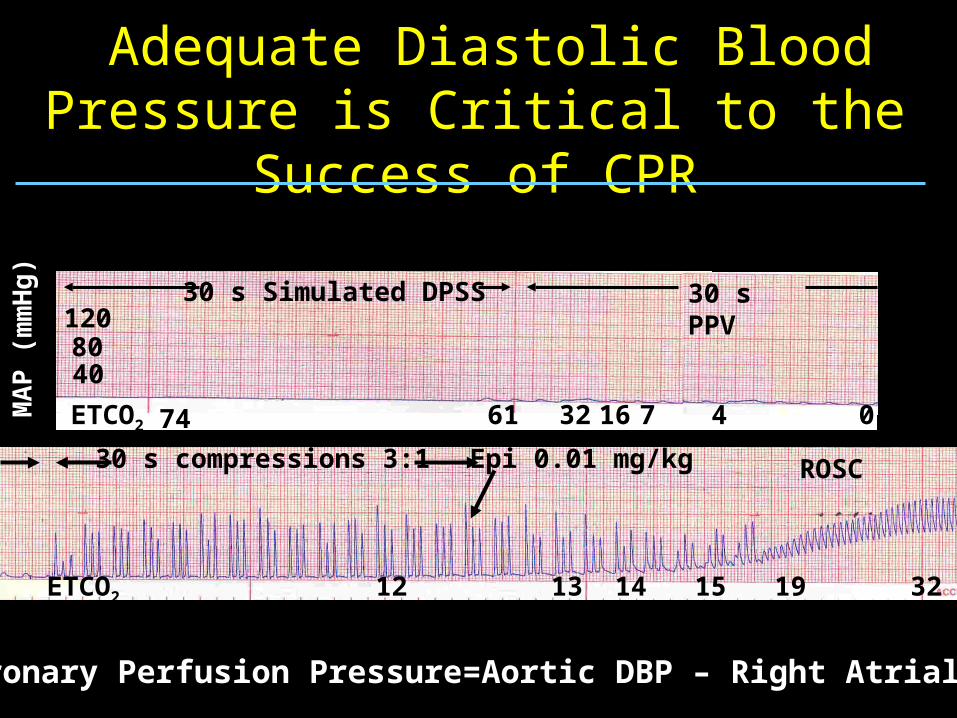
Adequate Diastolic Blood Pressure is Critical to the Success of CPR
ETCO2 74 61 1632 47 0MA
P (
mm
Hg
)
4080120
30 s Simulated DPSS 30 s PPV
12
Epi 0.01 mg/kg
13 14 15 19 32
30 s compressions 3:1 ROSC
ETCO2
Coronary Perfusion Pressure=Aortic DBP – Right Atrial DBP
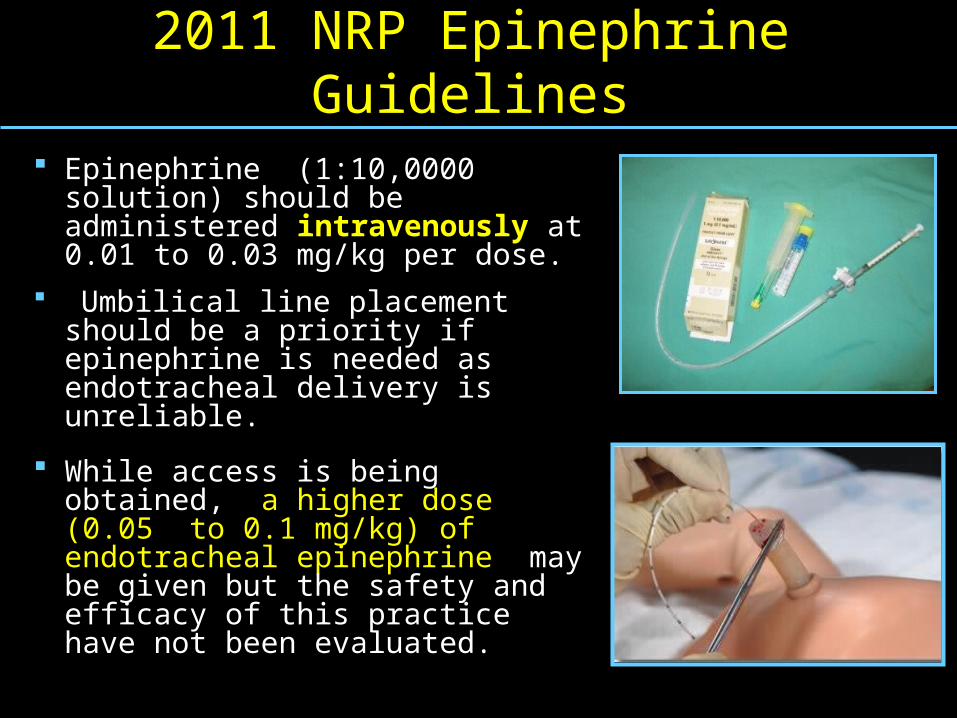
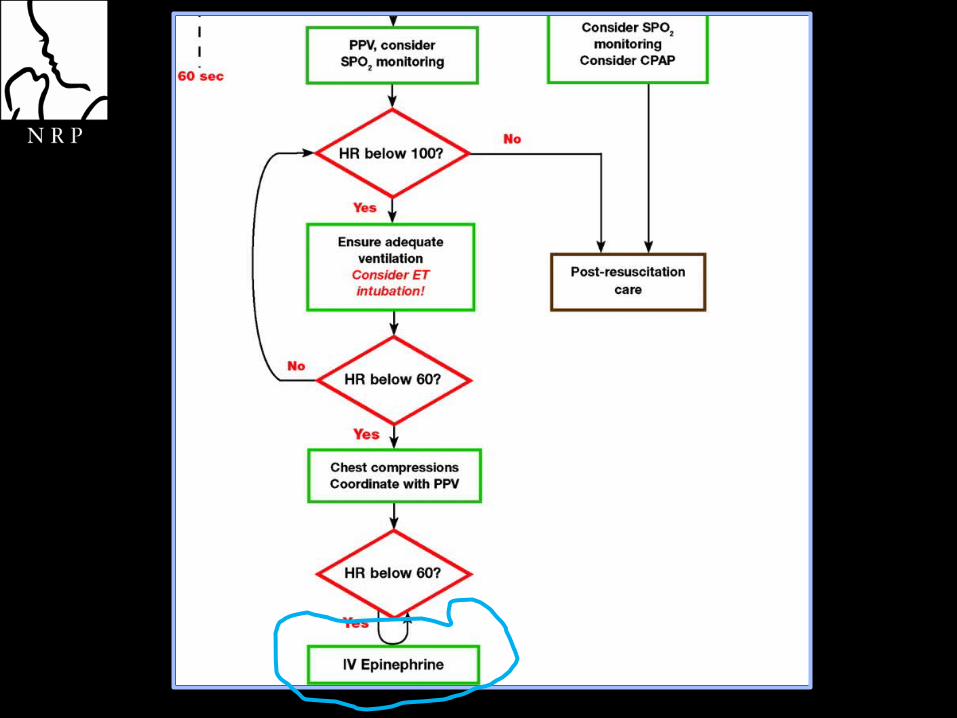
2011 NRP Epinephrine Guidelines
Epinephrine (1:10,0000 solution) should be administered intravenously at 0.01 to 0.03 mg/kg per dose.
Umbilical line placement should be a priority if epinephrine is needed as endotracheal delivery is unreliable.
While access is being obtained, a higher dose (0.05 to 0.1 mg/kg) of endotracheal epinephrine may be given but the safety and efficacy of this practice have not been evaluated.
Can We Do It Better? Is 1/3 the AP diameter really the optimal depth of
compression clinically?
Are there other ergonomic changes that could be made to optimize compressions?
Is coordination of compressions and ventilations really necessary ?
Would use of ETCO2 to predict return of adequate heart rate during cardiac compressions lead to less interruptions and better outcomes?
Is a heart rate less than 60 bpm the optimal time to initiate compressions?
Two Changes You MayWish to Make in Your Practice
Intubate to optimize ventilation prior to initiation of compressions
Once the airway is secure, perform compressions from the head of the bed
This will allow you to use the more effective two-thumb technique for cardiac compressions at all times, even while umbilical access is being obtained
Ackowledgments
Thanks to the AAP for several of the drawings and photos used for illustration


















