
Pulpal Pathology / orthodontic courses by Indian dental academy
Upload
ravi-acharyaCategory
view
288download
13
PULPAL PATHOLOGY AND ITS
SEQUELAE
Presenter
Dr. Ravi Acharya
PG Resident
Dept. Of Conservative Dentistry and Endodontics
B.P.Koirala Institute of Health Sciences
Dharan, Nepal

"The pulp lives for the dentin and the
dentin lives by the grace of the pulp.
Few marriages in nature are marked by
a greater affinity."
Alfred L. Ogilvie

CONTENTS
• Response of the pulp to dental caries
• Immune response in the dental pulp
• Hard tissue response to irritation
• Histologic changes in acute inflammation
• Histologic changes in the chronic inflammation
• Haemodynamic changes in the pulp during
caries

• Neural changes during pulpal inflammation
• Antiinflammatory and antinociceptive
mechanisms in the dental pulp
• Less common pulpal responses
• Factors limiting the pulps response
• Iatrogenic effects on the dental pulp
• Systemic factors
• Pulpal sequelae to impact trauma

The causes of pulp inflammation, necrosis, and dystrophy are:
I. Bacterial
A. Coronal ingress
1. Caries
2. Fracture
a. Complete
b. Incomplete (cracks, infraction)
3. Nonfracture trauma
4. Anomalous tract
a. Dens invaginatus (dens in dente)
b. Dens evaginatus
c. Radicular lingual groove (palatogingival
groove)

B. Radicular ingress
1. Caries
2. Retrogenic infection
a. Periodontal pocket
b. Periodontal abscess
3. Hematogenic

II. Traumatic
A. Acute
1. Coronal fracture
2. Radicular fracture
3. Vascular stasis
4. Luxation
5. Avulsion
B. Chronic
1. Adolescent female bruxism
2. Traumatism
3. Attrition or abrasion
4. Erosion

III. Iatral
A. Cavity preparation
1. Heat of preparation
2. Depth of preparation
3. Dehydration
4. Pulp horn extensions
5. Pulp hemorrhage
6. Pulp exposure
7. Pin insertion
8. Impression taking

B. Restoration
1. Insertion
2. Fracture
a. Complete
b. Incomplete
3. Force of cementing
4. Heat of polishing
C. Intentional extirpation and root canal filling
D. Orthodontic movement
E. Periodontal curettage
F. Electrosurgery

G. Laser burn
H. Periradicular curettage
I. Rhinoplasty
J. Osteotomy
K. Intubation for general anesthesia
IV. Chemical
A. Restorative materials
1. Cements
2. Plastics
3. Etching agents

4. Cavity liners
5. Dentin bonding agents
6. Tubule blockage agents
B. Disinfectants
1. Silver nitrate
2. Phenol
3. Sodium fluoride
C. Desiccants
1. Alcohol
2. Ether
3. Others

V. Idiopathic
A. Aging
B. Internal resorption
C. External resorption
D.Hereditary hypophosphatemia
E. Sickle cell anemia
F. Herpes zoster infection
G.Human immunodeficiency virus (HIV) and
acquired immune deficiency syndrome (AIDS)

RESPONSE OF THE PULP TO DENTAL
CARIES
• Bacteria are responsible for most pulpal disease.
• Kakehashi et al. proved that exposed pulps in
gnotobiotic (germ free) rats did not become
inflamed while similarly exposed pulps in rats with
a full oral flora did.

• The response of the pulp may vary depending on
whether the caries process progresses rapidly
(acute caries) or slowly (chronic caries), or is
completely inactive (arrested caries).
• Conditions for growth and availability of
nutrients are quite different in enamel caries than
in dentinal caries

• Products of bacterial metabolism, notably
organic acids and proteolytic enzymes, destroy
enamel and dentin.
• Relatively large bacterial product, bacterial
endotoxin, is able to diffuse through dentinal
tubules to the pulp chamber .

• Bacterial antigens diffusing from the lesion to the
pulp through the dentinal tubules are captured
and processed by APCs, which leads to the
activation of the immune system.
• Deep penetration of dentin by bacteria results in
acute inflammation and eventually infection and
necrosis of the pulp.

• The first reaction of odontoblasts to superficial
caries lesions in enamel is a marked reduction in
the cytoplasm: nucleus ratio, suggesting an altered
metabolism.
• In active lesions, primary odontoblasts are
involved in the formation of reactionary dentin.

• However, even before the appearance of
inflammatory changes, the size and number of
odontoblasts decrease, at which time their
metabolic activity is reduced while cellular
proliferative activity in the cell-free zone of the
pulp increases.

• Although normally tall columnar cells,
odontoblasts adversely affected by caries become
flat to cuboidal in shape.

• The boundary zone between primary and
reparative dentin is atubular and lacks continuity
of tubules.
• Electron microscopic examination of the
odontoblasts beneath a superficial caries lesion
revealed cellular injury in the form of ballooning
degeneration of mitochondria and a reduction in
the number and size of other cytoplasmic
organelles.

• Eventually, the primary odontoblasts die, usually
followed by proliferation of replacement
odontoblasts and reparative dentin formation.
•Bacteria infect some tubules
long before others are infected.

• The distribution of infected tubules is not
uniform, as neighboring uninfected tubules are
frequently found interspersed among infected
tubules.
•At the completion of cavity or
crown preparation, some infected
tubules may not have been
eliminated.

• Basic reactions that tend to protect the pulp
against caries includes:
1. Decrease in the permeability of the dentin due to
dentinal sclerosis,
2. Formation of new dentin (tertiary dentin),
3. Effectiveness of inflammatory and immunologic
reactions.

Dentinal Sclerosis:
• It develops at the periphery of almost all caries
lesions.
• Most common response to caries.
• In dentinal sclerosis, the dentinal tubules
become partly or completely filled with mineral
deposits consisting of both hydroxyapatite and
whitlockite crystals.

• Dentinal sclerosis reduces the permeability of
dentin, thus shielding the pulp from irritation.
• In order for sclerosis to occur, vital odontoblast
processes must be present within the tubules.

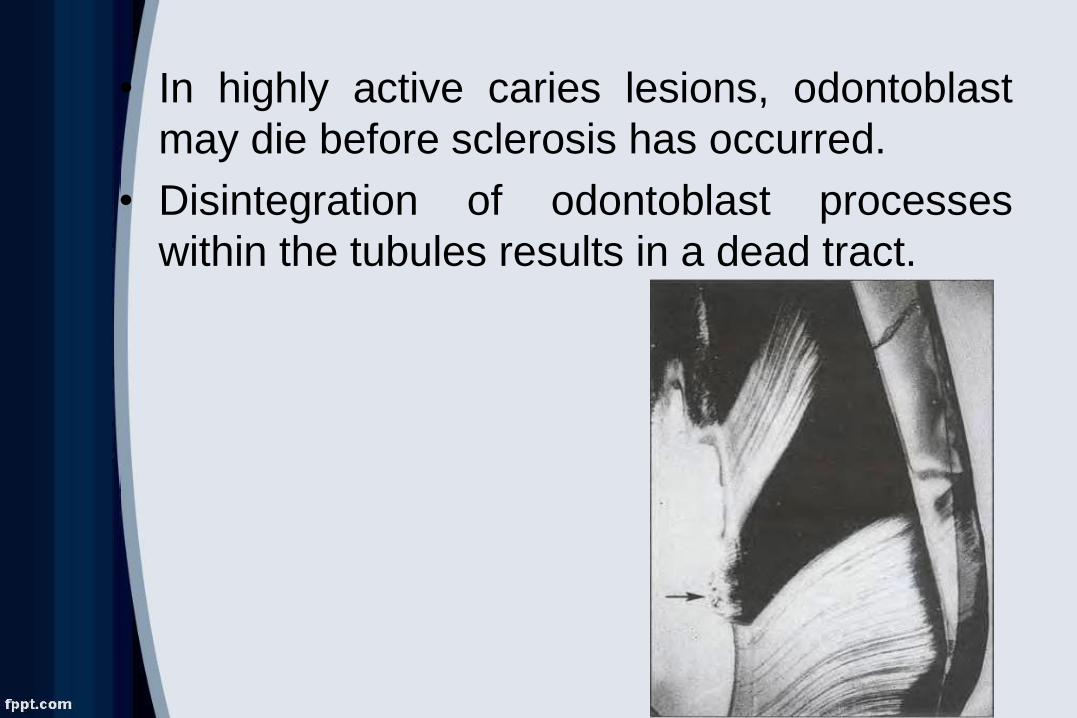
• In highly active caries lesions, odontoblast
may die before sclerosis has occurred.
• Disintegration of odontoblast processes
within the tubules results in a dead tract.

Tertiary dentin:
• There are two types of tertiary dentin based upon
the cell type responsible for dentin production:
1. Reactionary Dentin
2. Reparative Dentin

• Compared with primary dentin, reparative dentin
is less tubular and less well calcified.
• At times no tubules are formed; this type of
tertiary dentin has been characterized as a form of
fibrodentin.

• If the pulp is inflamed or has undergone
degenerative changes, the quality of the dentin is
more variable.
•An example of a poor
quality dentin is “Swiss
cheese” appearance of
dentin.
•The holes represent soft
tissue that was trapped in
the matrix and
subsequently underwent
necrosis.

Hard tissue response to irritation
Irritational dentin
• An odontoblast that is mildly stimulated
may form dentin that closely resembles
normal physiologic dentin.

• Since odontoblasts are incapable of
mitosis, they must be replaced by
underlying cells that mature from dividing
undifferentiated precursors or by
redifferentiation of fibroblasts.

• These new cells are atypical, frequently
without a process, and thus form an
atypical irregular structure called irritation
or reparative dentin.

• Its formation occurs independently of the
presence of inflammation and may form on
the walls of an irreversibly damaged pulp.
• Continued irritation dentin formation may
depend on persistent injurious stimuli; such
a condition is neither desirable nor
reparative.

• Anything that exposes or contacts dentin
has the potential to stimulate formation
of underlying irritation dentin.
• The morphology of irritation dentin has
been studied, but little is known of its
functions.

• Some attribute protective properties to this
tissue and therefore recommend methods
or materials to stimulate its formation.
• Others doubt its ability to protect the
underlying pulp.

• They have demonstrated its permeability,
permitting passage of chemicals and
bacteria and other substances.

• The presence of irritation dentin delays, but
does not prevent, the eventual penetration
of caries into the pulp.

BACTERIA AND THEIR BY-PRODUCT
CAN REACH THE PULP FROM OTHER
SOURCES
1. Anomalous Crown Morphology, Fractures,
and Cracks

Fig: Palatogingival GrooveClassification of invaginated teeth

2. Periodontal Disease
Saglie R et al: Scanning electron
microscopic depiction of the inside of
an ulcerated and infected pocket. Area
1 (right border) is the surface view of
lining epithelium. C, epithelial cell.
Dotted line demarcates the cut
surface of the epithelium (Area 2).
The basement lamina (BL) separates
the epithelium from connective tissue
(Area 3), which contains collagen
fibers (CF) and connective tissue cells
(CC). Bacteria (top arrow) enter a
hole (H) in the epithelium (left by a
desquamated cell) and travel through a
“tunnel” to emerge into connective
tissue through the hole. Abundant
cocci, rods, and filaments are seen
alongside the hole on the basement
lamina. Filaments and cocci are then
seen perforating the basement
membrane (double arrow) to
penetrate connective tissue and
reach blood and/or lymph vessels.

3.Blood Stream (Anachoresis)

ANTIGEN RECOGNITION IN THE
DENTAL PULP
• All three antigen-presenting cell types
expressing the type II major histocompatibility
complex (MHC) surface proteins,
macrophages, dendritic cells, and B
lymphocytes, are present and active in the
pulp's response to bacteria and toxins.

• In a normal healthy pulp, macrophages are
present in a resting form, as monocytcs.
• Macrophages require stimulation by bacteria or
cytokines before they express type II MHC
molecules.
• At rest they are found predominantly around
blood vessels though a few are distributed
throughout the tissue.

• Dendritic cells form a network throughout the
pulp concentrating around blood vessels and the
odontoblast layer.
• Some of the dendritic cells in the odontoblast
layer extend their processes into the dentinal
tubules.
• They constantly express the MHC molecules on
their surface without provocation.

• The number of dendritic cells increases in the
pulp when it becomes inflamed and they
accumulate beneath the carious lesion.


• B cells have been reported in the normal pulp but
are rather rare.
• Their role in the initial stages of antigen
recognition and presentation in the pulp is
unclear.
• Occasional T cells are found in normal pulp and
may be activated by antigen presenting cells
locally.

• In the pulp, there is a close anatomic relationship
between nerve fibers and dendritic cells, and
both increase in parallel when the pulp is
inflamed.

• The sympathetic nervous system has recently
been shown to have a modulating influence on
pulpal inflammation.
• The sympathetic system inhibits the production
of proinflammatory cytokines, although
stimulating the production of antiinflammatory
cytokines.

• In addition, T
lymphocytes and other
leukocytes produce anti
nociceptive molecules
such as β-endorphin and
somatostatin during
inflammation which
reduce the excitability of
pain fibers.

• Odontoblasts are the first cells to encounter an
antigen diffusing along the dentinal tubules.
• Odontoblasts respond differentially to the toxins
produced by gram-positive and gram negative
bacteria.

• Odontoblasts express microbial pattern
recognition receptors in situ, allowing
differential responses to gram-positive and
gram-negative bacteria.
• Pro-inflammatory cytokines and innate immune
responses in decayed teeth may result from TLR
signaling.
Veerayutthwilai O, Byers MR, Pharn TTT, et al. Differential regulation of immune
responses by odontoblasts. OralMicrobiol lmmunol 2007;22:5--1 3.

The Process of Antigen Recognition
• Dendritic cells and macrophages bind to and
phagocytize antigen that is then processed
intracellularly, bound to MHC molecules, and
moved to the cell membrane for recognition by T
cells.

• B cells bind antigen to specific cell surface
receptors.
• All the antigen-presenting cell types enter the
blood stream and carry the surface molecules
to the lymph nodes where T cell activation
takes place, though some may occur locally.

• The T cells respond not to the antigen itself but
to the modified complex in the cell membrane
of the antigen- presenting cells.
• Being stationary, the odontoblast does not
participate directly in the activation of T cells
but, presumably, activates dendritic cells.

HISTOLOGIC CHANGES IN ACUTE
INFLAMMATION
• Cariogenic bacteria in the dental plaque produce
a mixture of acids and enzymes that dissolve the
mineral elements of enamel and dentin and then
digest the organic matrix.
• The initial removal of mineral makes the enamel
more permeable and the bacterial toxins will
diffuse well ahead of cavitation.

• Once the dentin is reached, the toxins and, much
later, the bacteria themselves will travel along the
dentinal tubules.
• Clearly, variations in the composition and
thickness of enamel and dentin, and particularly
the patency of the dentinal tubules, will determine
the rate at which these toxins reach the pulp.

• In vital teeth, this
movement will be
opposed by the outward
flow of dentinal fluid.
• Toxins, however, reach
the pulp at a very early
stage relative to surface
changes.

HISTOLOGIC CHANGES IN CHRONIC
INFLAMMATION
• The immediate
"inflammatory" phase
of the immune
response begins very
shortly after the
antigen arrives in the
tissue.

• If the body has been exposed to the antigen on a
previous occasion, the production of specific
antibodies begins very quickly (within a few
hours).
• If antigen not encountered before, it takes
several days for the production of antibodies.

• At this stage, the pulpal response is
characterized by the presence of the
lymphocytes.

• If the carious lesion is not treated, however, the
increasing quantity of irritants will eventually
cause irreversible changes.
•These are at first limited
in size and may even form
a "pulpal abscess.“

• This local necrosis, unless checked, will
progress gradually throughout the tissue and
into the periradicular tissues.
• The progress of tissue damage in the pulp is
determined by the presence and spread of
bacterial toxins and is not due to the
"strangulation" of blood vessels.

Suppuration and Necrosis
• Exposure of the pulp to caries often results in
suppurative inflammation, depending upon the
nature of the invasive bacteria.
• The generation of chemotaxins by pyogenic
bacteria produces a massive accumulation of
neutrophils.

• HOCL produced from neutrophil destroys
bacteria by halogenation and lipid peroxidation.
• The ability to avoid phagocytosis is of key
importance in the virulence of pyogenic bacteria.

• Because of certain antiphagocytic virulence factors,
it is difficult for neutrophils to kill pyogenic
bacteria, and as a result more and more neutrophils
are mobilized in an attempt to overwhelm the
invading organisms.
• As bacteria invade deep into the dentin, neutrophils
begin to accumulate adjacent to the dentinal tubules.

• Because bacteria in the tubules are virtually
unassailable by host defenses, there is a constant
supply of chemotaxins to mobilize neutrophils.
• If the number of neutrophils reaches a critical
mass, an abscess, a walled-off area of suppuration,
will develop.

• The death of neutrophils in situ gives rise to
purulence, formed chiefly by autolysis of
neutrophils by their own lysosomal enzymes.
• As this process continues, an abscess cavity is
formed.

• Tissue necrosis develops when neutrophils release
activated oxygen metabolites and proteases.
• It results in liquefaction necrosis.
• As the caries exposure enlarges and an ever-
increasing number of bacteria enter the pulp, the
defending forces are eventually overwhelmed

• Therefore, when blood flow can no longer meet the
demand for inflammatory elements, the
inflammatory response can no longer be sustained
and bacteria may grow unopposed within the pulp
chamber.
• This ultimately leads to total pulp necrosis.
• Exposure of the pulp to caries does not invariably
result in suppuration.
• In the absence of a sufficient number of pyogenic
bacteria, a localized area of necrosis may develop.

• The body responds to this necrotic debris by
attempting to produce reparative dentin.

• Exposure of the pulp may also trigger extensive
fibrosis of the pulp.

Chronic ulcerative pulpitis
• The histologic term ulcerative is actually a
misnomer in these cases because no surface
epithelium is involved.
• This condition is the result of local excavation of
the surface of the pulp resulting from liquefaction
necrosis of pulp tissue.

• Excavation is likely to occur when drainage of
inflammatory exudate is established through a
pathway of decomposed dentin.
•The inflammation remains
localized and asymptomatic
because drainage prevents a
buildup of pressure.

Chronic hyperplastic pulpitis
• Occurs most often in primary and immature
permanent teeth with incompletely formed roots.
• At this stage of development, numerous blood
vessels enter the pulp through the wide apical
foramen.

• Histologically characterized by proliferation of
small vessels and fibroblasts and a chronic
inflammatory cell infiltrate.
• The lesion acquires a stratified squamous covering,
presumably because of grafting of vital
desquamated epithelial cells from the oral mucosa.

• Chronic hyperplastic pulpitis develops when carious
pulp exposure creates a large open cavity.
• This opening establishes a pathway for drainage of
the inflammatory exudate.

• When drainage is established, acute inflammation
subsides and chronic inflammatory tissue
proliferates through the opening created by the
exposure to form a polyp.

HEMODYNAMIC CHANGES IN THE PULP
DURING CARIES
Blood Flow
• Using plaque extract to initiate inflammation in a
rat incisor model, a 40% increase in blood flow
in a "moderately inflamed" pulp but a 35%
reduction in a "partially necrotic" pulp was
reported.
Kim S, Liu M, Simchon 5, Dorscher-Kim JE. Effects of selected inflammatory mediators on blood
flow and vascular permeability in the dental pulp. Proc Finn Dent Soc t 992;88 (Suppl 1):387-92.

• The application of Lippolysaccharide to the pulp
resulted, after 10 minutes, in a reduction in blood
flow that continued for the 3-hour duration of the
experiments. This was interpreted as a limited
ability of the pulp to respond.
Blelsa A, Berggreen E, Fristad I, et al. Cytokine signalling in rat pulp interstitial fluid and transcapillary fluid
exchange during lipopolysaccharide-induced acute inflammation. J PhysioI 2006;573:225-36.

Interstitial Fluid Pressure
• The healthy dental pulp has an interstitial
pressure of 5 to 10 mm Hg.
• One of the key changes during inflammation is
the movement of fluid from within the
capillaries into the interstitial space.

• Increasing the amount of fluid in a rigid chamber
leads to an increase in pressure. It was assumed,
for a long time, that such a pressure rise in the
pulp would cause compression of the blood
vessels leading to vascular stasis and necrosis.
• It was even suggested that this pressure change
could lead to strangulation of the vessels at the
apex causing necrosis in areas of the pulp not
directly affected by the bacterial toxins.

• Necrosis occurs beneath persisting carious
lesions only when bacterial toxins, spreading
throughout the pulp, poison cells directly.

NEURAL CHANGES DURING PULPAL
INFLAMMATION
• Sympathetic nerves control blood flow by constricting
precapillary sphincters and by interaction with other
elements of inflammation.
• It inhibits the production of proinflammatory cytokines,
stimulating the production of anti-inflammatory
cytokines and is involved in the recruitment of
inflammatory cells to the area.
• Has an inhibitory effect on odontocasts and stimulate
reparative dentin production.

• Afferent sensory fibers from the trigeminal
system plays an important role in response to
toxins and injury.
• They release substance P and Calcitonin Growth
Related Protein (CGRP).
• They both causes vasodilatation and increase
capillary permeability.

• In injured pulps, there is an increased expression
of nerve growth factor (NGF) and its receptors.
• A concomitant sprouting of the afferent terminals
and increased presence of substance P and CGRP
also takes place.

• Pulpal injury and inflammation are also
associated with neural changes outside the pulp
itself.
• In the trigeminal ganglion after pulpal injury the
expression of various neuropeptides increases.
• There are also detectable changes in the
supporting cells of the ganglion.

• Most significant from a clinical point of view are
changes in the nucleus related to central
sensitization.
• This may help explain the variable presentation of
pulpitis in terms of pain.

ANTI-INFLAMMATORY AND
ANTINOCICEPTIVE MECHANISMS IN THE
DENTAL PULP
• Neuroimmune interactions control pain
through the activation of opioid receptors on
sensory nerves by immune derived opioid
peptides.
• Opoid receptors are present on pulpal nerves.

• On exposure to stress, opioid peptides are
released, bind to opoid receptors on peripheral
sensory neurons, and induce endogenous
antinociception.

LESS COMMON PULPAL RESPONSES:
CALCIFICATION AND RESORPTION
• Calcification of the pulp
takes a variety of forms.
Discrete pulp stones occur
in a large proportion of the
population.
• The vast majority of pulp
stones are found in molars.

• Pulp stones are more common in patients with
atheromatous cardiovascular disease.
• A higher incidence of pulpal mineralization is
associated with some genetic disorders such as
Ehlers-Danlos syndrome and amelogenesis
imperfecta.

• A generalized, more diffuse mineralization of
the pulp may occur after trauma and is one of
several good reasons for follow-up radiographs.
• Internal resorption has
been considered an
alternative sequelae to
trauma.

WHEN THE PULPAL RESPONSE
SUCCEEDS: REPAIR AND REGENERATION
• The immune response, including inflammation,
is only one part of the pulp's total response to
toxins or injury.
• When effective, it neutralizes and removes any
foreign material and allows and probably
initiates the second part, recovery, repair, and
regeneration.

• When no cells are killed,
the original odontoblasts
can form reactionary
(tertiary) dentin.

• When the odontoblasts are
killed, new dentin-forming
cells develop from stem
cells (undifferentiated
mesenchymal cells) and
form reparative (tertiary)
dentin.

• The repair of larger areas of damage is more
variable and depends on the nature of any
clinical intervention.

ENCOURAGING A SUCCESSFUL
RESPONSE
• Most of our strategies for encouraging pulpal
repair involve removal of the irritant and
diseased tissue and the prevention of further
injury.

FACTORS LIMITING THE PULP'S
RESPONSE
• The only significant factor that limits the pulp's
ability respond to injury is age.
• The older pulp has a reduced number of cells,
innervation, and vascularity, but the immune
response remains active.

IATROGENIC EFFECTS ON THE DENTAL
PULP-Local Anesthetics
• Local anesthetics reduce pulpal blood flow by
approximately half when they contain
vasoconstrictors.
• It is important to remember that when preparing
a cavity in an anesthetized tooth the pulp is in a
suboptimal condition to respond.

Cavity/Crown Preparation
Heat: Cutting Dentin
The amount of heat produced is determined by:
1. Sharpness of the bur
2. Amount of pressure exerted on the bur
3. Length of time the cutting instruments
contacts tooth structure.

The two cooling methods most frequently
applied are:
1. Air cooling
2. Water cooling
Damage has been observed in pulps of teeth cut
with air-cooling only.

• Dentin is a good insulator of heat unless the
thickness of dentin between preparation and
pulp is less than 1.0 mm.
• The “blushing” of dentin is due to frictional heat
resulting in vascular injury in the pulp.

The safest way to prepare tooth structure is to
use:
1. Ultrahigh speeds of rotation (100,000-
250,000 rpm),
2. Efficient water-cooling system,
3. Light pressure,
4. Intermittent cutting


• The close proximity of
the pulp to the external
surface of the tooth,
particularly at the furcal
plane area, where tooth
preparation for full
coverage of
periodontally involved
teeth is so critical, has
been emphasized by
Sproles.

Heat: Laser Beams
• Laser irradiation can generate a large increase in
temperature within dentin and pulp tissue.
• Proper power setting, time of application, and
use of water spray will mitigate the temperature
increase to levels below the heat threshold of
pulp damage.

Pins
• Pulp damage may result from pinhole preparation
or pin placement.
• Coolants do not reach the depth of the pin
preparation.
• During preparation, there is always the risk of pulp
exposure.

• Furthermore, friction locked pins often
produce micro-fractures that may extend to the
pulp, subjecting the pulp to irritation and the
effects of microleakage.


Cavity Cleansing
• A prolonged blast of compressed air aimed
onto freshly exposed vital dentin will cause a
rapid outward movement of fluid in patent
dentinal tubules.
Activates strong capillary forces
Causes rapid outward flow of dentinal
fluid
Stimulates nociceptors also causes
odontoblast displacement
Removal of fluid from the tubules by blast of air

Etching Dentin/Smear Layer
• Microleakage is increased if the smear layer
remains, whereas dentin permeability is
increased if the smear layer is removed.

Impressions And Temporary Crowns
• Modeling compound may be damaging because
of the combination of heat and pressure.
• Rubber base and hydrocolloid materials do not
injure the pulp.

• The heat generated during the exothermic
polymerization of autopolymerizing resins may
also injure the pulp.
• Cooling is strongly recommended when
provisional crowns are fabricated directly.

• The temporary crown/cement should be in
place for a short period of time.
• Microleakage around temporary crowns is a
common cause of postoperative sensitivity.

Crown Cementation
• During the cementation of crowns, inlays, and
bridges, strong hydraulic forces may be exerted
on the pulp as cement compresses the fluid in the
dentinal tubules.
• In deep preparations, this can result in a
separation of the odontoblast layer from the
predentin.
• Vents in the casting will allow cement to escape
and facilitate seating.

Dental Materials
Microleakage
• The most important characteristic of any
restorative material, in determining its effect on
the pulp, is its ability to form a seal that prevents
the leakage of bacteria and their products onto
dentin and then into the pulp.

Cytotoxicity
• Certain restorative materials are composed of
chemicals having the potential to irritate the
pulp.
• When placed in a cavity, the intervening dentin
usually neutralizes or prevents leachable
ingredients from reaching the pulp in a high
concentration to cause injury.

• The thickness and permeability of dentin
between a material and the pulp affect the
response to the material.
• In addition, the penetration of some materials
through dentin may be limited by the outward
flow of fluid through the tubules that will be
increased if the pulp is inflamed.

Heat upon Setting
• Temperature increases during setting procedures
may be over l0°C but can be limited to 2 to 3°C
with care.
• Cooling techniques include the use of air/water
cooling and removing the temporary upon initial
polymerization.

• The most exothermic luting material is ZnOP
cement.
• However, during setting, an intrapulpal
temperature increase of only 2°C was recorded.
Heat of this magnitude is not sufficient to injure
the pulp.

Desiccation by Hygroscopy
• Some hygroscopic materials may potentially
cause injury by withdrawing fluid from dentin.
• Moisture absorbed by materials is probably much
less than that removed from dentin during cavity
drying, a procedure that produces an insignificant
amount of pulpal inflammation.

SPECIFIC MATERIALS –
Zinc Oxide- Eugenol
• Eugenol, is toxic when placed in direct contact
with tissue.
• When included in cements to temporize crown
preparation, some eugenol does reach the pulp,
but the amounts are small and unrelated to
RDT.

Zinc Phosphate Cement
• The phosphoric acid liquid phase was formerly
thought to injure the pulp.
• However, recent studies have shown that this is
not the case.

• Researchers reported that ZnOP is more likely
to produce pulpal sensitivity at the time of
cementation and 2 weeks after cementation
than glass ionomer. However, 3 months after
cementation, there is no difference in
sensitivity.

Polycarboxylate Cement
• When placed in cavities or used as a luting
cement, zinc polycarboxylate does not irritate the
pulp.
• In cementing well-fitting crowns and inlays,
neither polycarboxylate nor ZnOP cements
contract enough to permit the ingress of bacteria.

Restorative Resins
• The first adhesive bonding and resin composite
systems contracted during polymerization
resulting in gross microleakage and bacterial
contamination of the cavity.
• With recently developed hydrophilic adhesive
bonding composite systems, the problem of
marginal leakage appears to have been
diminished.


Glass Ionomer Cements
• A photo-activated RMGI showed minimal to no
cytotoxicity in vitro tests.
• In vivo tests demonstrated only minimal pulp
reactions when RMGI was evaluated in non
human usage models.

•Recent studies have
demonstrated that
pulpotomy is successful
when restored with an
RMGI Adhesive Resin
Systems or adhesive.
•RMGI has been used as a
definitive restorative agent
to decrease microleakage.

Amalgam
• There is shrinkage during setting, which results in
microleakage.
• This decreases as corrosion products accumulate
between restoration and cavity walls and can be
reduced by the use of liners.
• Amalgam is the only restorative material in which
the marginal seal improves with time.

MTA
• The most promising material is mineral trioxide
aggregate (MTA) because of its superior
characteristics as a direct pulp-capping agent
compared with Ca(OH)2 controls in several
animal models.
• Results show reparative dentin bridge formation
in the majority of samples with minimal
inflammatory cell response.

Histologic section from a
nonhuman primate pulp that
was direct capped with Dycal
for 24 months. The dentin
bridge contains a tunnel defect
running from the restoration
interface to the dental pulp,
Histologic section of a nonhuman primate
pulp that was direct capped with MTA for
5 months. A new dentin bridge is seen
midfield directly below the MTA particles
with new odontoblastoid cells along the
pulp interface. The deeper pulp is free of
operative debris chips and inflammation

POLISHING RESTORATIONS
• Polishing glass ionomer and composite
restorations does not cause an increased
temperature at the pulp-dentin interface.
• Polishing amalgam restoration produce
temperatures that may be damaging.

• When polishing an amalgam restoration with
continuous pressure and no water coolant, it is
recommended to not exceed 4,000 rpm.
• With use of coolant, light pressure, and
intermittent contact during polishing, there is a
low likelihood of heat-generated pulp damage.

POST-RESTORATIVE HYPERSENSITIVITY
• If pain is prolonged, a preexisting pulpitis may
have been exacerbated.
• If delayed, the cause may be microleakage of
bacterial toxins under a poorly sealed
temporary restoration.

• If pain evoked is by biting on a recently restored
tooth, an intracoronal restoration may be
exerting a strong shearing force on the dentin
walls of the preparation.
• Hyperocclusion from an extra-coronal
restoration is not injurious to the pulp but may
cause a transient hypersensitivity.

VITAL TOOTH BLEACHING
• Can cause mild pulpitis which is
reversed within 2 weeks.

VITALITY TESTING
• Heat and cold testing within normal
clinical parameters does not damage the
dental pulp.

ORTHODONTICS
• Orthodontic tooth movement of a routine nature
does not cause clinically significant changes in
the dental pulp.
• The heavy forces used to reposition impacted
canines frequently lead to pulp necrosis or
calcific metamorphosis.

A, Radiograph of canine intruded by trauma. B, Effect of hypoxia on
pulp owing to intrusion.Myelinated nerve showing vacuolization
of axon (closed arrow), disruption and smudging of myelin sheath
(open arrow), and loss of cellular detail. C, Loss of cellular
detail in the nucleus (N) and cytoplasm (C). Cell clumping in nucleus and
loss of organelles with rupture of lysosome (arrow) in cytoplasm.

• Bracket removal by use of an electrothermal
device (ETD) does not cause gross damage or
necrosis of dental pulp.
• There may be limited peripheral disruption of
odontoblasts with slight inflammation.

ULTRASONIC SCALING
• Ultrasonic scaling of roots requires
prolonged contact of the ultrasonic
device, and the potential for pulp damage
exists.
• Proper water cooling of both ultrasonic
and sonic scalers will prevent excessive
heat production in the pulp.

SYSTEMIC FACTOR
Hereditary Hypophosphatemia
• It is characterized dentally by the abnormally
large pulps and incomplete calcification of the
dentin.
• The pulps in these teeth appear to be fragile and
succumb to minor irritating stimuli.

SYSTEMIC FACTOR
• Sickle cell anemia
• Herpes zooster infection
• HIV and AIDS
PULPAL SEQUELAE TO IMPACT
TRAUMA
It can be categorized as
1. Repair
2. Calcification
3. Resorption
4. Necrosis

• The response depends on type, duration,
severity and suceptibility of the pulp to injury.
The result maybe:
1. Adaptation
2. Reversible injury
3. Death

Radiograph of max central
incisor. The pulp chamber and
canal are obliterated with
irritational dentin.
A, Radiograph of a maxillary left central
incisor. The canal is large because the trauma
stopped root development when the pulp
became necrotic. There is inflammatory
resorption of the apex. B, After endodontic
therapy.

CONCLUSION
• Exposure of dentin through attrition, trauma, or
caries produces profound pulpal reactions that
tend to reduce dentin permeability and stimulate
formation of additional dentin.
• These reactions are brought about by changes in
fibroblasts, nerves, blood vessels, odontoblasts,
leukocytes, and the immune system.

• Recent discoveries of the effects of nerves on
pulpal blood vessels and vice versa have
produced a new appreciation for the interaction
of these two systems in response to stimuli
applied to dentin.
• The special features of the dental pulp, including
restricted vascularity, enclosure in dentin, and
susceptability to bacterial infection or trauma,
play an important role in defining the
inflammatory and healing potential of this tissue

References
• Ingle’s Endodontics,5th and 6th edition
• Dental Pulp, Seltzer and Benders
• Cohen’s Pathways Of the Pulp,9th edition
• Essentials of Endodontics, Vimal K Sikri
• Textbook of Endodontics, Nisha Garg, 2nd
Edition



















