Pulmonary Hypertension - PeaceHealth Presentation PC11 Ameen.pdfDiagnosis of Pulmonary Hypertension...
37
Pulmonary Hypertension Khuram Ameen Oregon Lung Specialists
Transcript of Pulmonary Hypertension - PeaceHealth Presentation PC11 Ameen.pdfDiagnosis of Pulmonary Hypertension...

Pulmonary Hypertension
Khuram Ameen Oregon Lung Specialists

No Relevant Disclosures

Definition OF Pulmonary Arterial Hypertension
Mean Pulmonary artery pressure of 25 mm or greater at rest and 30 or greater with exercise
Pulmonary capillary wedge pressure (PCWP) <15 mmHg
Pulmonary vascular resistance (PVR) >120 dynes/sec/cm5

WHO Classification
Group 1. Pulmonary arterial hypertension (PAH)
Group 2. Pulmonary hypertension with left heart disease
Group 3. Pulmonary hypertension associated with lung diseases and/or hypoxemia
Group 4. Pulmonary hypertension due to chronic thrombotic and/or embolic disease
Group 5. Miscellaneous

PAH Is Difficult to Diagnose
Early symptoms of PAH are subtle and nonspecific Symptoms include dyspnea, fatigue, angina, syncope, among
others1,2
Idiopathic pulmonary arterial hypertension (IPAH) is a diagnosis of exclusion Diagnosis typically takes 2 to 3 years3
1. Peacock AJ et al, eds. Pulmonary Circulation: Diseases and Their Treatment. 2nd ed. Arnold; 2004. 2. National Institutes of Health. National Heart, Lung, and Blood Institute diseases and conditions index. What is pulmonary arterial hypertension? Available at:
http://www.nhlbi.nih.gov/health/dci/Diseases/pah/pah_what.html. Accessed October 18, 2005. 3. Rich S et al. Ann Intern Med. 1987;107:216-223.

Clinical Presentation
Common Initial Symptoms (N =187)
Patients (%)
Dyspnea 60
Fatigue 19
Syncope or near syncope 13
Chest pain 7
Palpitations 5
Leg edema 3

Diagnosis Of Pulmonary Hypertension
Patients suspected of having PH generally
undergo extensive diagnostic testing, which is aimed at confirming its presence and identifying its cause.
The goal of diagnostic testing is to confirm that PH exists and to identify its underlying cause.

Diagnosis of Pulmonary Hypertension
Pulmonary function tests It is usually severe interstitial lung disease (with lung volumes below 50 percent of predicted) or obstructive lung disease that produces PH. In most circumstances, PH should not be attributed to lung disease if the PFTs are only mildly abnormal since PH itself can cause PFT abnormalities
Chest radiograph enlargement of the central pulmonary arteries with attenuation of the peripheral vessels, Right ventricular enlargement
Electrocardiography signs of right ventricular hypertrophy or strain Most ECG signs are not sensitive

Diagnosis of Pulmonary Hypertension
Overnight oximetry Overnight oximetry can be used to screen patients for Obstructive Sleep Apnea-Hypopnea (OSAH)-related nocturnal oxyhemoglobin desaturation, although it is not an acceptable diagnostic test for OSAH. Polysomnography is the gold standard diagnostic test for OSAH and should be considered when the clinical suspicion for OSAH is high
V/Q scan Ventilation-perfusion (V/Q) scanning is used to evaluate patients for thromboembolic disease. A normal V/Q scan accurately excludes chronic thromboembolic disease with a sensitivity of 90 to 100 percent and a specificity of 94 to 100 percent

Diagnosis of Pulmonary Hypertension
Echocardiography Echocardiography is performed to estimate the pulmonary artery systolic pressure and to assess right ventricular size, thickness, and function. In addition, echocardiography can evaluate right atrial size, left ventricular systolic and diastolic function, and valve function, while detecting pericardial effusions and intracardiac shunts

Diagnosis of Pulmonary Hypertension
Right heart catheterization Right heart catheterization is necessary to confirm the
diagnosis of PH and accurately determine the severity of the hemodynamic derangements
The presence and/or severity of a congenital or acquired left-to-right shunt can be confirmed when noninvasive studies are not definitive
A vasoreactivity test is necessary for reasons other than the initiation of advanced therapy
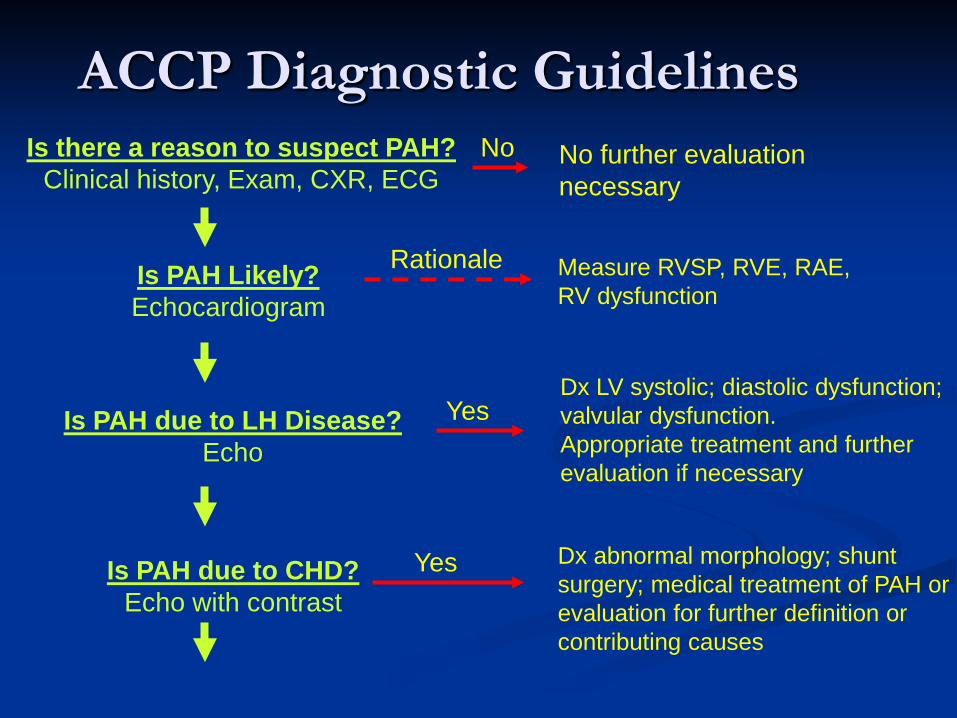
Is there a reason to suspect PAH? Clinical history, Exam, CXR, ECG
No further evaluation necessary
Is PAH Likely? Echocardiogram
No
Is PAH due to LH Disease? Echo
Measure RVSP, RVE, RAE, RV dysfunction
Dx LV systolic; diastolic dysfunction; valvular dysfunction. Appropriate treatment and further evaluation if necessary
Yes
Is PAH due to CHD? Echo with contrast
Rationale
Dx abnormal morphology; shunt surgery; medical treatment of PAH or evaluation for further definition or contributing causes
Yes
ACCP Diagnostic Guidelines
McGoon, et al. Chest 2004

ACCP Diagnostic Guidelines (cont.)
Is PAH due to CTD, HIV? Serologies
Is chronic PE suspected? V/Q scan
Dx scleroderma, SLE, other CTD, HIV. Medical treatment for PAH and further evaluation for contributing causes
Is chronic PE confirmed and operable? Pulmonary angiogram
Yes
Is PAH due to lung disease or hypoxemia? PFT’s, arterial saturation
Yes
Thromboendarterectomy if appropriate or medical treatment
No
Yes
Dx parenchymal lung disease, hypoxemia or sleep disorder. Medical treatment, oxygen, positive pressure breathing, and further evaluation for other contributing causes
Yes
McGoon, et al. Chest 2004

ACCP Diagnostic Guidelines (cont.)
McGoon, et al. Chest 2004
What limitations are caused by the PAH?
FC, 6 MWT
What are the precise hemodynamics?
RHC
Document PA and RA pressures, PCWP (LV or LA pressure if PCWP unobtainable or uncertain), transpulmonary gradient, CO,PVR,SvO2,response to vasodilators: Confirm PAH , or IPAH if no other cause identified. Discuss genetic testing and counseling of IPAH family
Document exercise capacity regardless of cause of PH: Establish baseline, prognosis and document progression/response to treatment with serial re-assessment

Classification of PAH Group One (ACCP 2004)
1.1 Idiopathic (iPAH)
1.2 Familial
1.3 Associated with Collagen vascular disease
Congenital systemic to pulmonary shunts
Portal hypertension
HIV infection
Drugs and Toxins
Other (hemoglobinopathy, glycogen storage diseases etc.)
1.4 Associated with significant venous or capillary involvement 1.5 Persistent pulmonary hypertension of the newborn
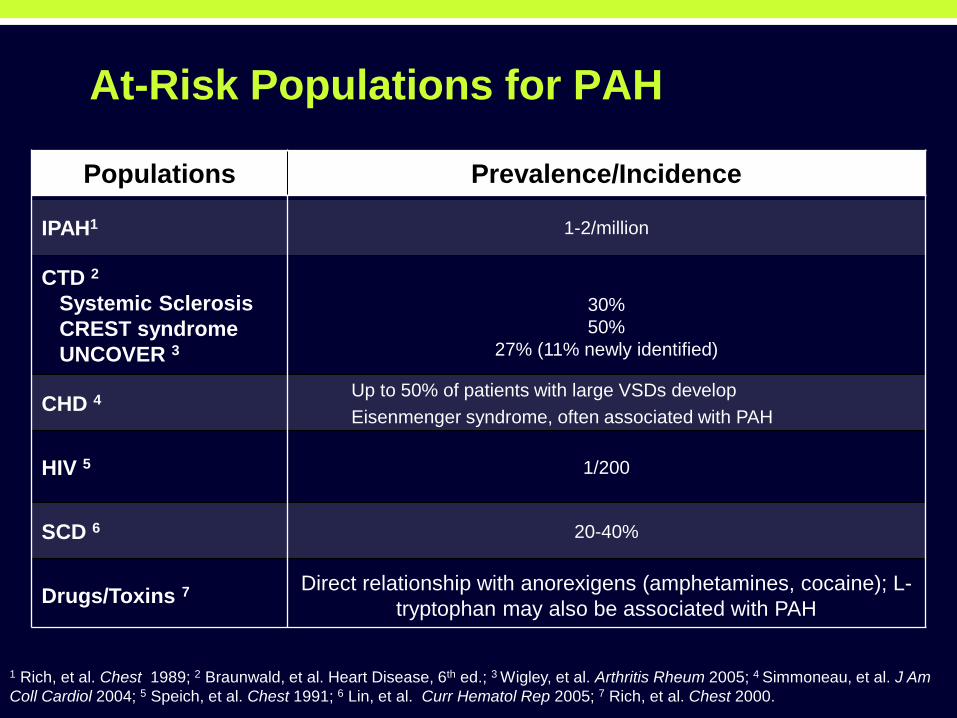
At-Risk Populations for PAH
Populations Prevalence/Incidence
IPAH1 1-2/million
CTD 2
Systemic Sclerosis CREST syndrome UNCOVER 3
30% 50%
27% (11% newly identified)
CHD 4 Up to 50% of patients with large VSDs develop Eisenmenger syndrome, often associated with PAH
HIV 5 1/200
SCD 6 20-40%
Drugs/Toxins 7 Direct relationship with anorexigens (amphetamines, cocaine); L-tryptophan may also be associated with PAH
1 Rich, et al. Chest 1989; 2 Braunwald, et al. Heart Disease, 6th ed.; 3 Wigley, et al. Arthritis Rheum 2005; 4 Simmoneau, et al. J Am Coll Cardiol 2004; 5 Speich, et al. Chest 1991; 6 Lin, et al. Curr Hematol Rep 2005; 7 Rich, et al. Chest 2000.

Increased Pulmonary Resistance and Pressure
Pre-Symptomatic Symptomatic Severely Symptomatic
High flow, low resistance vessel Low flow, high resistance vessel
Adapted from Gaine, et al. JAMA 2000.
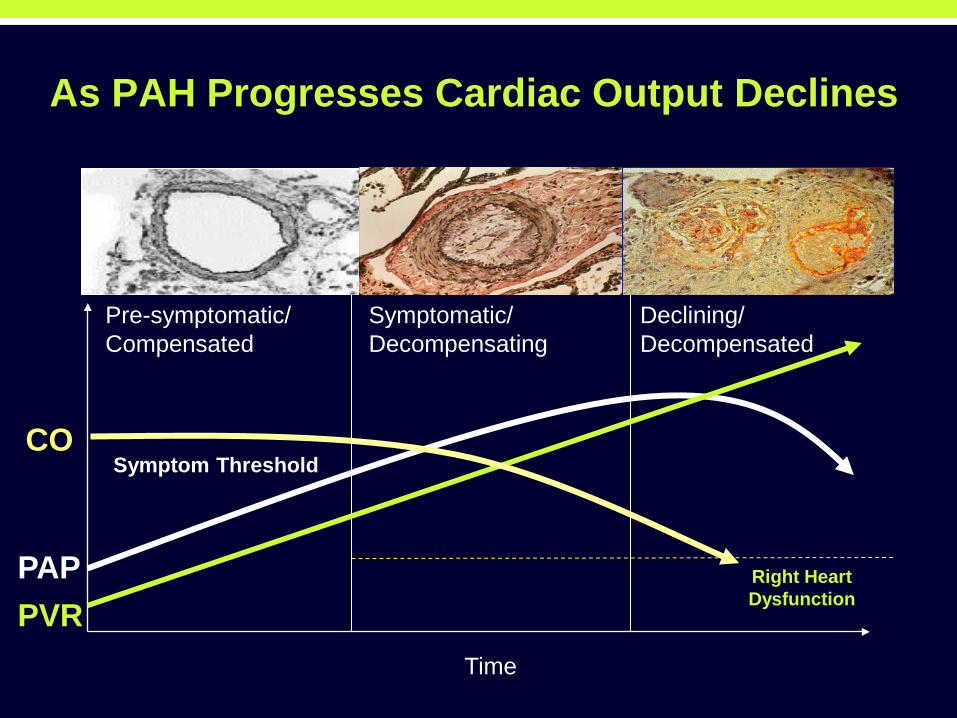
As PAH Progresses Cardiac Output Declines
Time
PAP PVR
CO
Pre-symptomatic/ Compensated
Symptomatic/ Decompensating
Symptom Threshold
Right Heart Dysfunction
Declining/ Decompensated

IPAH: Rapid Progression and Poor Survival
Adapted from: D’Alonzo, et al. Ann Intern Med 1991.
PAH Survival
0
20
40
60
80
100
0 0.5 1 1.5 2 2.5 3 3.5 4 4.5 5 Years of Followup
Surv
ival
(%)
68%
48% 34%
PAH Survival
0
20
40
60
80
100
0 0.5 1 1.5 2 2.5 3 3.5 4 4.5 5 Years of Followup
Surv
ival
(%)
68%
48% 34%

PAH: Survival Based on Etiology1
1. Adapted from McLaughlin VV et al. Chest. 2004;126:78-92.
1 2 3 4 5 Years
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0
0
Survival in PAH
CHD CVD HIV IPAH Portopulm

PAH/SSc Progresses Even More Rapidly
Koh, et al. Br J Rheumatol 1996
0
10
20
30
40
50
60
70
80
90
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13
Years from Diagnosis of Pulmonary Hypertension
Perc
ent S
urvi
val
PAH
Lung Involvement without PAH
No Lung involvement

PAH Treatment: Targeting Known Pathophysiological Pathways
1. Kaplan NM. Systemic hypertension: mechanisms and diagnosis. In: Zipes DP, Libby P, Bonow RO, Braunwald E, eds. Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine. 7th ed. Saunders; 2005:959-987. 2. Spieker LE et al. J Am Coll Cardiol. 2001;37:1493-1505. 3. Badesch DB. Chest. 2004;126:35-62.
Prostacyclins Epoprostenol
Treprostinil IV/SQ?Oral Iloprost, inhaled
PDE-5 inhibitors
Sildenafil Tadalafil
Endothelin receptor antagonists Bosentan
*Sitaxsentan *Ambosertan

Pathways Involved in PAH
ET-1 binds to ETA and ETB receptors on smooth muscle and endothelial cells1
NO stimulates the cGMP pathway2
PGI2 stimulates the cAMP pathway2
Stimuli such as decreased blood flow, hypoxia, or shear stress induce the overproduction of ET-1 and decrease NO production3-5
Chronic imbalance of ET-1, NO, and PGI2 levels lead to pathophysiological changes3-8:
Vasoconstriction Increased vascular tone Smooth muscle cell proliferation
Vascular remodeling Right-heart hypertrophy
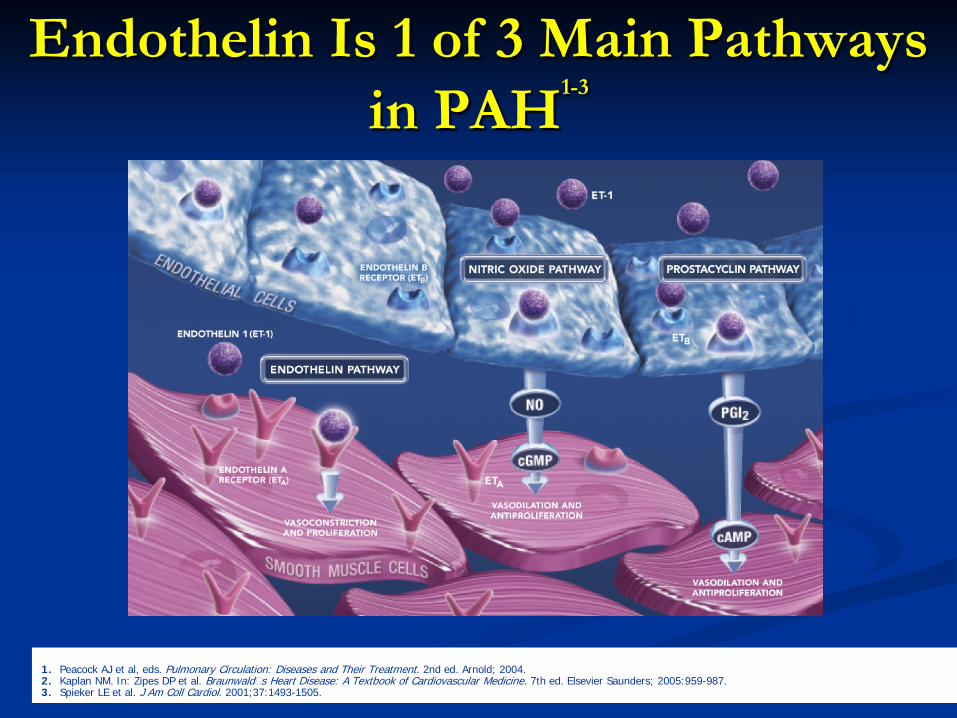
Endothelin Is 1 of 3 Main Pathways in PAH1-3
1. Peacock AJ et al, eds. Pulmonary Circulation: Diseases and Their Treatment. 2nd ed. Arnold; 2004. 2. Kaplan NM. In: Zipes DP et al. Braunwald�s Heart Disease: A Textbook of Cardiovascular Medicine. 7th ed. Elsevier Saunders; 2005:959-987. 3. Spieker LE et al. J Am Coll Cardiol. 2001;37:1493-1505.

Endothelial Dysfunction Primarily Drives PAH
Two hallmarks of PAH are vasoconstriction and vascular remodeling1 Vasoconstriction and cellular proliferation are driven by
ET-12 Vasodilation is driven by nitric oxide (NO) and
prostacyclin (PGI2), which are antiproliferative in nature3
Disease severity is associated with excess circulating ET-1 levels4
1. Jeffery TK et al. Pharmacol Ther. 2001;92:1-20. 2. Peacock AJ et al, eds. Pulmonary Circulation: Diseases and Their Treatment. 2nd ed. Arnold; 2004. 3. Hankins SR et al. Curr Cardiol Rep. 2000;2:244-251. 4. Rubens C et al. Chest. 2001;120:1562-1569.

Prostacyclins
Therapeutic Class 2001-2003
2004-2005 2006 1990s-2000
PDE-5 inhibitors
Endothelin receptor antagonists
PAH Treatment: Timeline of Recent Advances1-3
Epoprostenol
Treprostinil
Iloprost
Bosentan
Sitaxsentan*
Sildenafil
*Late stage clinical development 1. Humbert M et al. N Engl J Med. 2004;351:1425-1436. 2. CDER Priority Drug and Biologic Approvals in Calendar Year 2004. Available at http://www.fda.gov/cder/rdmt/NDAPriority04.htm. Accessed on April 10, 2006. 3. CDER Priority Drug and Biologic Approvals in Calendar Year 2005. Available at http://www.fda.gov/cder/rdmt/InternetPriority05.htm. Accessed on April 10, 2006.

WHO Functional Class of PAH Class I Patients with PH but without resulting limitation of physical activity.
Ordinary physical activity does not cause undue dyspnea, chest pain, or near syncope.
Class II Patients with PH resulting in slight limitation of physical activity. They are comfortable at rest. Ordinary physical activity causes undue dyspnea or fatigue, chest pain, or near syncope.
Class III Patients with PH resulting in marked limitation of physical activity. They are comfortable at rest. Less than ordinary activity causes undue dyspnea or fatigue, chest pain, or near syncope.
Class IV Patients with PH with inability to carry out any physical activity without symptoms. These patients manifest signs of right-heart failure. Dyspnea and/or fatigue may even be present at rest. Discomfort is increased by any physical activity.
Rubin. Chest 2004

PAH: Conventional Therapy
• Includes1
– Supplemental oxygen to treat chronic hypoxemia – Diuretics – Anticoagulants – Digoxin
• Some patients benefit from high-dose calcium channel blockers1
– Can alleviate pulmonary vasoconstriction and increase survival2
– Hypotension and edema can result in poor tolerance of required doses3
– Candidates identified by acute vasodilator challenge1,2
1. Humbert M et al. N Engl J Med. 2004;351:1425-1436. 2. Nauser TD, Stites SW. Am Fam Physician. 2001;63:1789-1798, 1800. 3. Mehta S. Chest. 2003;124:2045-2049.
PAH: Prostacyclin Therapy
• Epoprostenol (Flolan®)1
• Indicated for IPAH and for PAH patients associated with scleroderma – Class III-IV
• Given by continuous infusion – Requires in-dwelling central venous catheter
• Common dose-limiting adverse events: nausea, vomiting, headache, hypotension, and flushing
• Abrupt withdrawal can result in rebound PAH symptoms • Must keep reconstituted solution between 2° and 8°C
1. Flolan prescribing information. GlaxoSmithKline, 2002.

PAH: Prostacyclin Therapy (cont)
• Treprostinil (Remodulin®)1
• Indicated for PAH patients – Class II-IV
• Given via subcutaneous or intravenous infusion • Longer half-life than epoprostenol
– Reduces risk of rebound worsening • Common adverse events: pain (85%) or reaction (83%) at
infusion site • Stable at room temperature
1. Remodulin prescribing information. United Therapeutics Corporation, 2006.
PAH: Prostacyclin Therapy (cont)
• Inhaled iloprost (Ventavis®)1
• Indicated for PAH patients (WHO Group I) – Class III-IV
• Given via nebulizer – Short duration of action2
– 6 to 9 inhalations per day • Common adverse events: flushing, cough, headache
1. Ventavis prescribing information. CoTherix, Inc., 2005. 2. Humbert M et al. N Engl J Med. 2004;351:1425-1436.
PAH: Phosphodiesterase-5 Inhibitor Therapy
• Sildenafil (Revatio™)1
• Indicated for PAH patients (WHO Group I) • Oral
– Recommended dose 20 mg three times per day • Common adverse events: headache, dyspepsia, flushing
1. Revatio prescribing information. Pfizer, Inc., 2005.

PAH: Endothelin Receptor Antagonist Therapy
• Bosentan (Tracleer®)1
• Indicated for PAH patients (WHO Group I) – Class III-IV
• Oral – Initial dose: 62.5 mg bid x 4 weeks – Maintenance dose: 125 mg bid
• Liver enzymes measured prior to initiating treatment and then monthly
• Common adverse events: headache, flushing, abnormal hepatic function, leg edema, anemia
• Pregnancy must be excluded before start of treatment; monthly pregnancy tests required
1. Tracleer prescribing information. Actelion Pharmaceuticals US, Inc. 2005.

Significant Change in 6MWD BREATHE-1
Tracleer 125/250 mg bid (n=144)
Treatment Effect: 44 m (p<0.001)
Rubin, et al. N Engl J Med 2002
-10
20
40
0 4 8 16 12 Weeks
62.5 mg bid 125 or 250 mg bid
Placebo (n=69)
0
Cha
nge
in 6
MW
D (m
)
Data are mean ± SEM. Walk distance was somewhat greater with 250 mg BID, but the potential for increased liver injury causes this dose not to be recommended [125 mg BID (n=74) change in walk distance (m): 27 ± 75, 250 mg BID (n=70) change in walk distance (m): 46 ± 62].



PAH: Class II/III/IV Treatment Algorithm1
1. Adapted from Humbert M et al. N Engl J Med. 2004;351:1425-1436.
Continue calcium- channel blockers
Atrial septostomy or
Lung transplantation
Pulmonary arterial hypertension (WHO functional class II, III, or IV)
Conventional therapy (oral anticoagulant ± diuretics ± oxygen)
Yes No
Acute vasodilator response
Endothelin-receptor antagonist or
PDE5 Inhibitor or
Prostacyclin analogues or
Intravenous prostacyclin
Intravenous prostacyclin or
Endothelin-receptor antagonist or
Prostacyclin analogues or
PDE5 Inhibitor
Class II Oral calcium-channel blockers
Sustained Response PDE5 Inhibitor or
Prostacyclin analogue Endothelian-receptor
antagonists
Class IV Class III
No improvement or deterioration
Yes No