
Pulmonale Hypertonie: Warum gerade ich? Risikofaktoren und ... · Pulmonale Hypertonie: Warum...
39
Pulmonale Hypertonie: Warum gerade ich? Risikofaktoren und Krankheitsmechanismen Ralph Schermuly Department of Pulmonary Pharmacotherapy University of Giessen and Marburg Lung Center
Transcript of Pulmonale Hypertonie: Warum gerade ich? Risikofaktoren und ... · Pulmonale Hypertonie: Warum...
Pulmonale Hypertonie:
Warum gerade ich?
Risikofaktoren und Krankheitsmechanismen
Ralph Schermuly
Department of Pulmonary Pharmacotherapy
University of Giessen and Marburg Lung Center
0
10
20
30
40
50
60
70
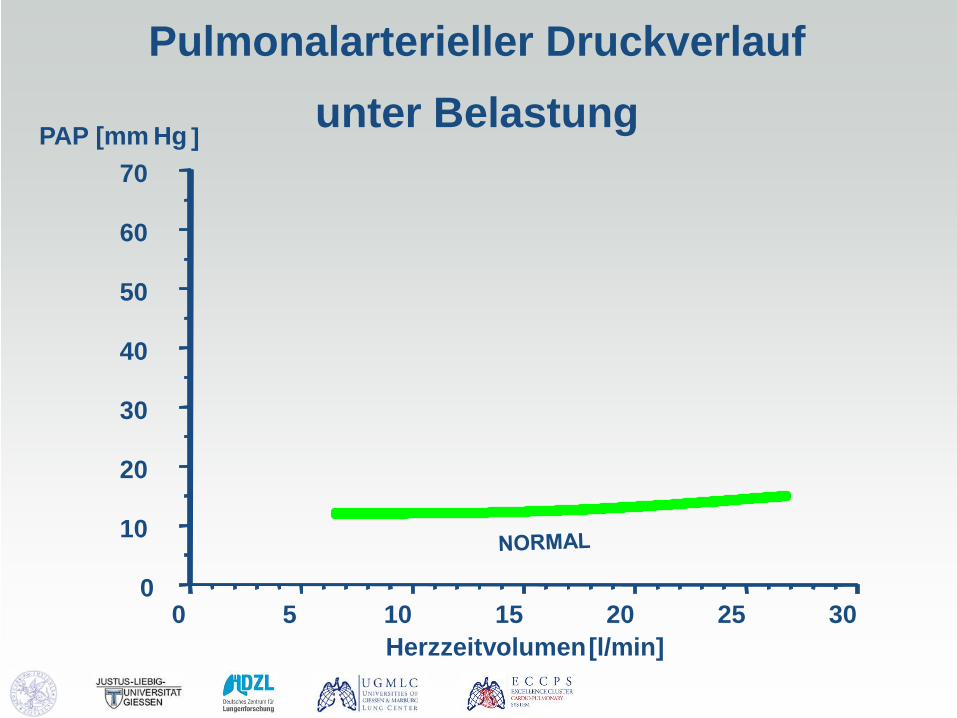
0 5 10 15 20 25 30 Herzzeitvolumen [l/min]
PAP [mm Hg ]
Pulmonalarterieller Druckverlauf unter Belastung
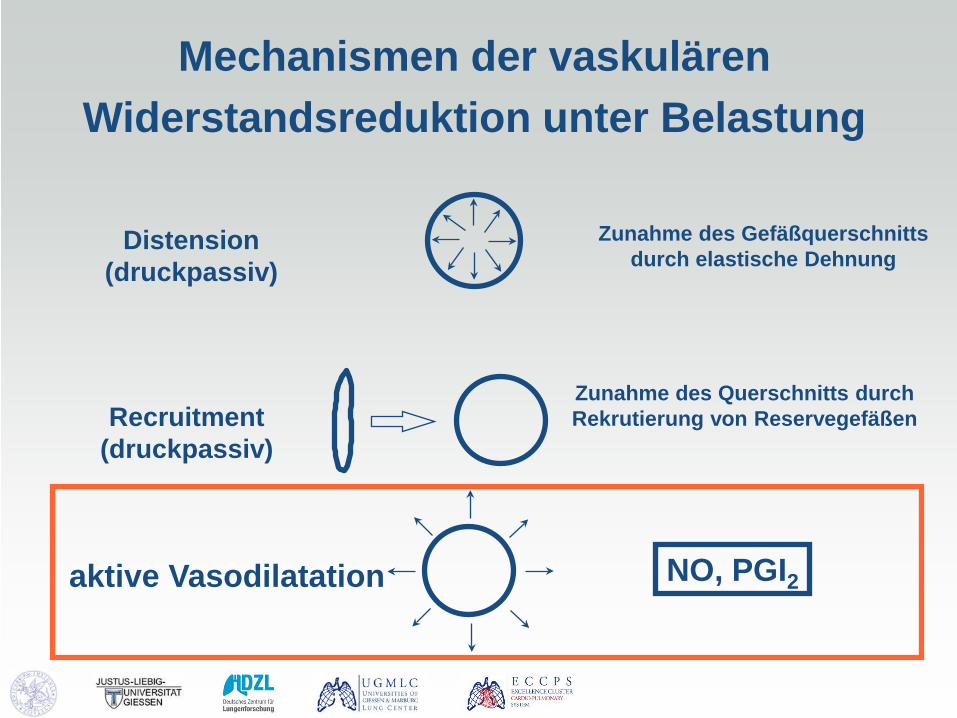
Mechanismen der vaskulären Widerstandsreduktion unter Belastung
Distension (druckpassiv)
Recruitment (druckpassiv)
aktive Vasodilatation
Zunahme des Gefäßquerschnitts durch elastische Dehnung
Zunahme des Querschnitts durch Rekrutierung von Reservegefäßen
NO, PGI2

Pulmonalvaskuläre Erkrankungen
0
10
20
30
40
50
60
70
0 5 10 15 20 25 30 Herzzeitvolumen [l/min]
PAP [ mm Hg ]
0
10
20
30
40
50
60
70
0 5 10 15 20 25 30 Herzzeitvolumen [l/min]
PAP [ mm Hg ]
Latente PH: COPD Fibrose Linksherzinsuff. Aging
Manifeste PH Kollagenosen
PAH

80 µm
15 µm
normal
De novo Muscularization / distal Migration
pulmonary vascular disease
Remodeling: Definition
Strukturelle Veränderungen der Gefäßwand,
charakterisiert durch endotheliale, mediale und
adventitielle Proliferation als Antwort auf Hypoxie,
Druckveränderungen oder Gefäßerkrankungen
Pulmonalarterielles Remodeling umfaßt alle
Schichten der Gefäßwand
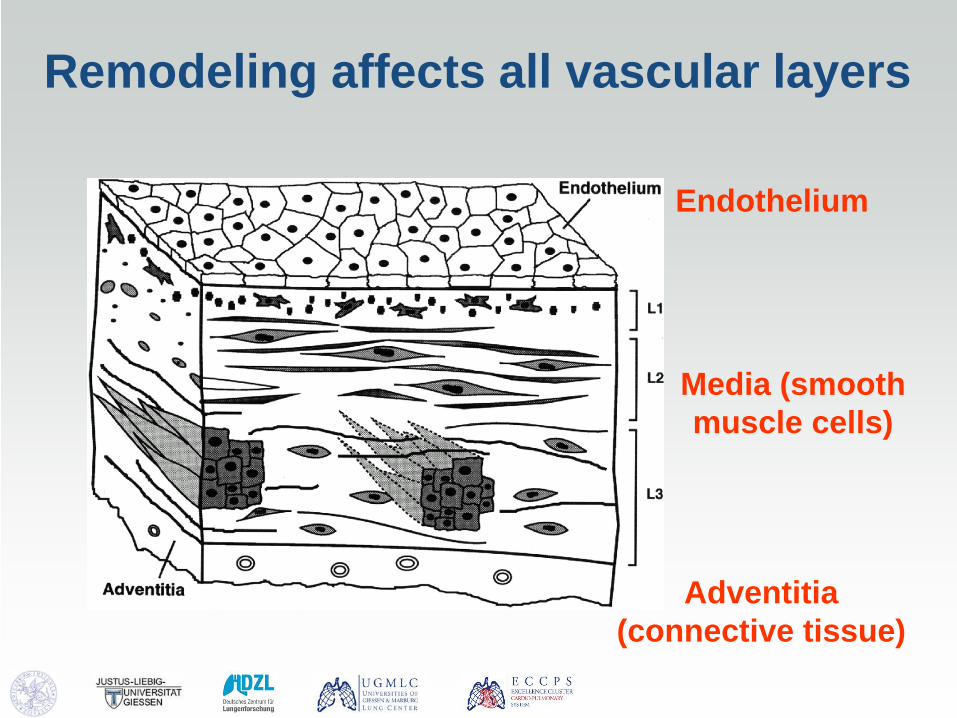
Remodeling affects all vascular layers
Endothelium
Media (smooth muscle cells)
Adventitia (connective tissue)

Mediahypertrophie
Neointimabildung
Lumenverengung
Rarefizierung
(‚Pruning‘)
Plexiforme Läsionen
(PAH)
Was sind die Charakteristika von ‚Remodeling‘?
De novo Muskularisierung

Ursachen des Lungenhochdrucks
Entzündung Linksherz- versagen
Sauerstoff- mangel

Idiopathic = rare disease
Different variants up to 100 million people worldwide
Mean survival rate - without therapy 2 - 4 years - < 3 months in right heart decompensation
chest-X-ray small pulmonary artery
Pulmonary Hypertension

I Preclinical/
No symptoms
II Symptomatic /
Stable
III Progression /
declining
Pulm pressure
Cardiac output
Leve
l
Time
PAH : a rapidly evolving disease
Years Months
Therapeutic window
RV function
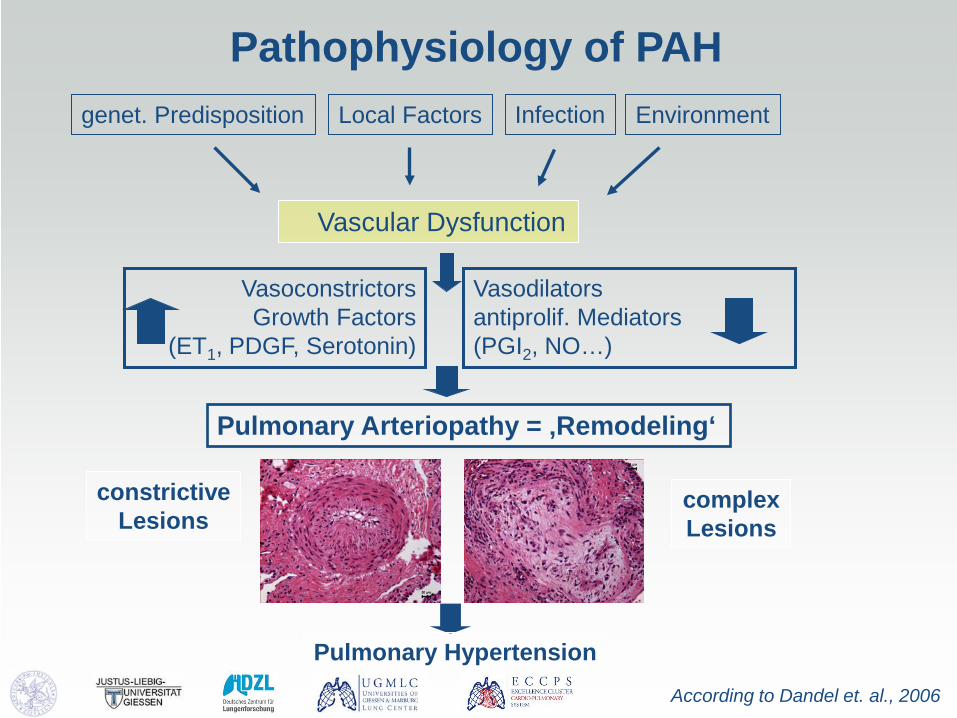
Pathophysiology of PAH genet. Predisposition Environment Local Factors
Vascular Dysfunction
Vasoconstrictors Growth Factors
(ET1, PDGF, Serotonin)
Vasodilators antiprolif. Mediators (PGI2, NO…)
Pulmonary Arteriopathy = ‚Remodeling‘
constrictive Lesions
complex Lesions
According to Dandel et. al., 2006
Pulmonary Hypertension
Infection

Molecular Pathology: Imbalance of vasoactive mediators
Humbert et. al., NEJM 2004
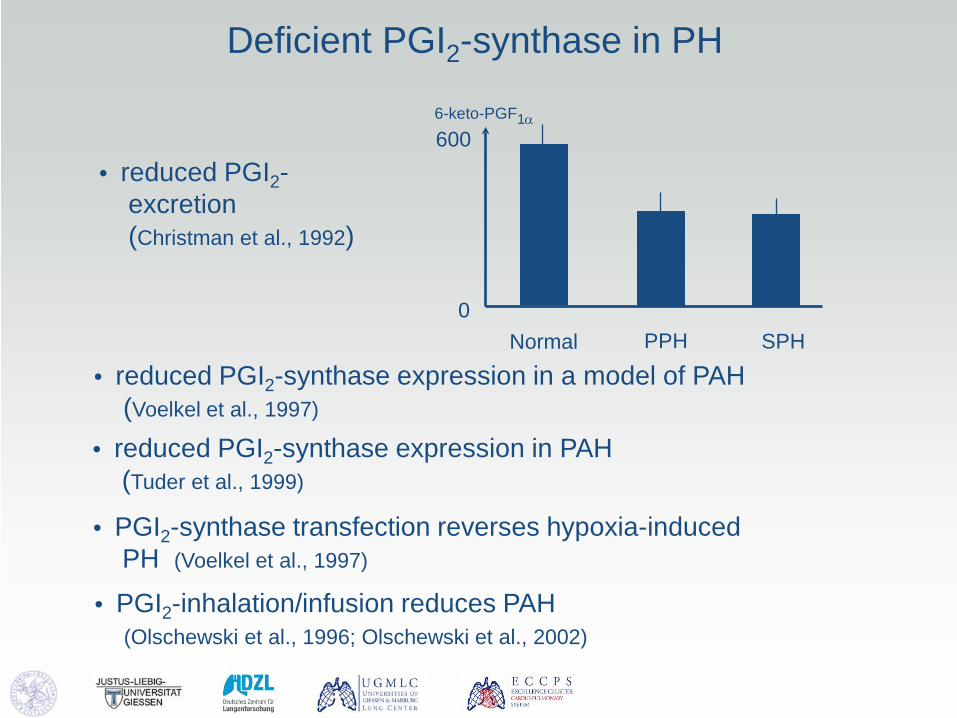
Deficient PGI2-synthase in PH
• reduced PGI2- excretion (Christman et al., 1992)
Normal PPH SPH
600
0
6-keto-PGF1α
• reduced PGI2-synthase expression in a model of PAH (Voelkel et al., 1997)
• PGI2-synthase transfection reverses hypoxia-induced PH (Voelkel et al., 1997)
• PGI2-inhalation/infusion reduces PAH (Olschewski et al., 1996; Olschewski et al., 2002)
• reduced PGI2-synthase expression in PAH (Tuder et al., 1999)
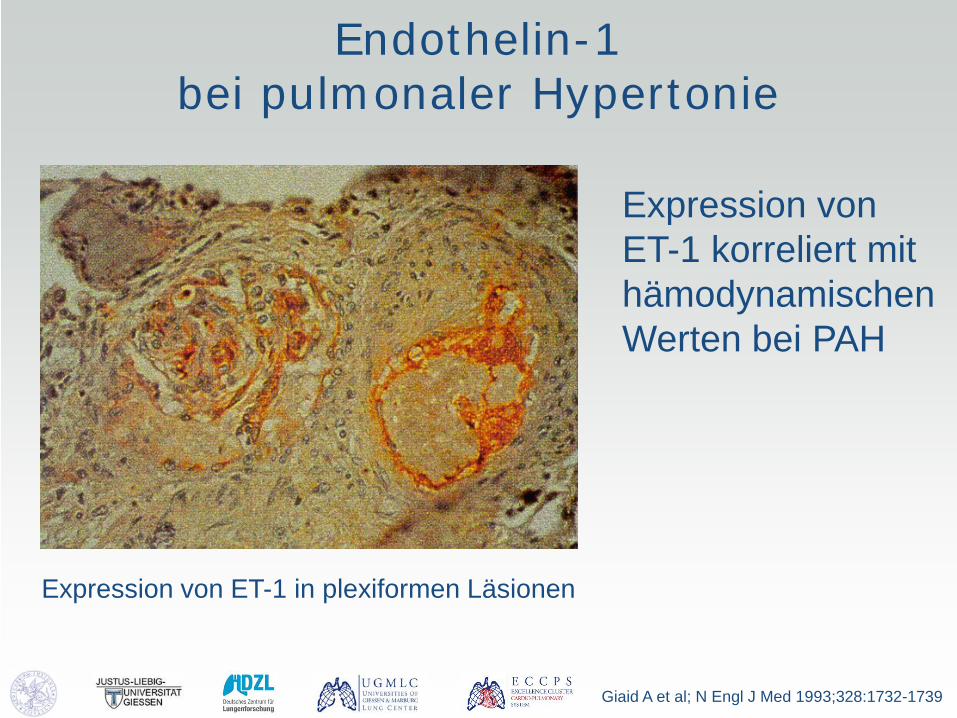
Endothelin-1 bei pulmonaler Hypertonie
Expression von ET-1 in plexiformen Läsionen
Giaid A et al; N Engl J Med 1993;328:1732-1739
Expression von ET-1 korreliert mit hämodynamischenWerten bei PAH

Endothelin Rezeptoren in Pulmonalarterien
Migneault A et al. Am J Respir Crit Care Med 2005
Sowohl ETA als auch ETB sind in der Media hoch exprimiert
Endothelin-Rezeptor A Endothelin-Rezeptor B
In Rot: Immunfluoreszenz-Markierung der Verteilung der ET-R in den kleinen Lungenarterien
Grün: Markierung Grenze von Endothel (E) und Media (M)
IEL interne elastische Lamina EEL externe elastische Lamina

1.Clozel M, et al. J Pharmacol Exp Ther 1989; 2.Yang Z, et al. Circulation 1999; 3.Kuhlmann, et al. Acta Physiol Scand 2005; 4.Girgis RE, et al. Am J Respir Crit Care Med 2005; 5.Amiri, et al. Circulation 2004; 6.Cambrey AD, et al. Am J Respir Cell Mol Biol 1994; 7.Shi-Wen X, et al. J Invest Dermatol 2001; 8.Yang, et al. Circulation 2004.
Endothelin induziert Dysfunktion von Endothelzellen, glatten Muskelzellen und
Fibroblasten und Zytokin-Freisetzung
glatte Muskelzellen Vasokonstriktion,
Hypertrophie, Proliferation1-2
Fibroblasten Fibrose6-7
Endothelin
Endotheliale Zellen Proliferation,
Dysfunktion3-5
Inflammation NF-kB und cytokine
Freisetzung, Erhöhte
Gefäßpermeabilität8

Ghofrani et al. Nat Rev Drug Discovery 2006
NO-sGC-PDE Pathway
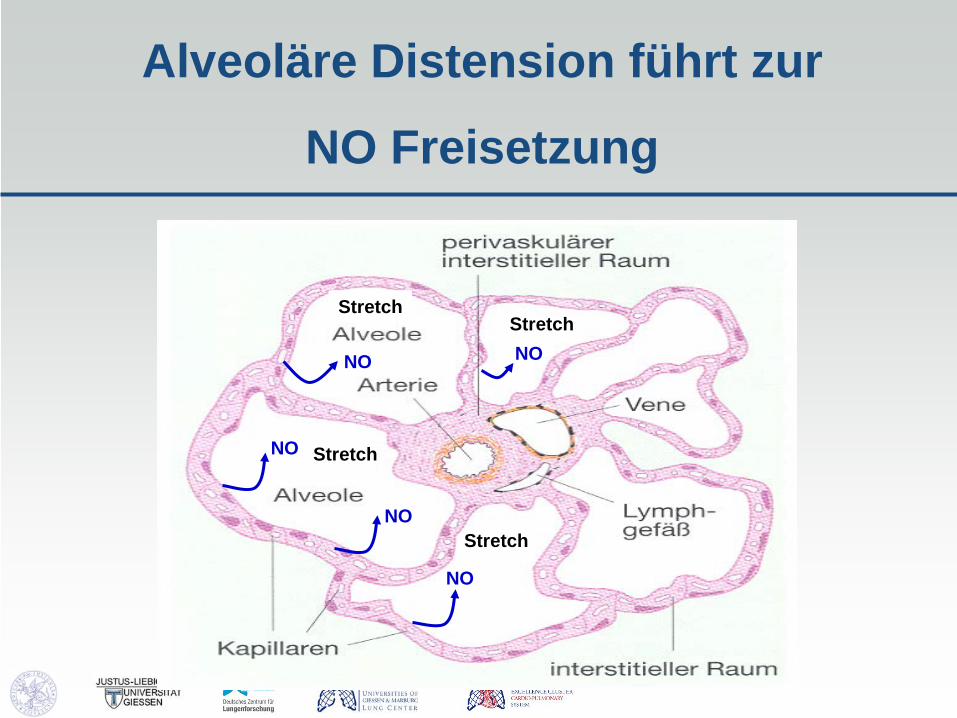
Alveoläre Distension führt zur
NO Freisetzung
Stretch
Stretch
Stretch Stretch
NO
NO
NO
NO
NO

Expression of Phosphodiesterase 5 in pulmonary vascular diseases
Wharton et al. AJRCCM 2005
α - Actin
PDE 5A
Schermuly et al., Circulation 2007
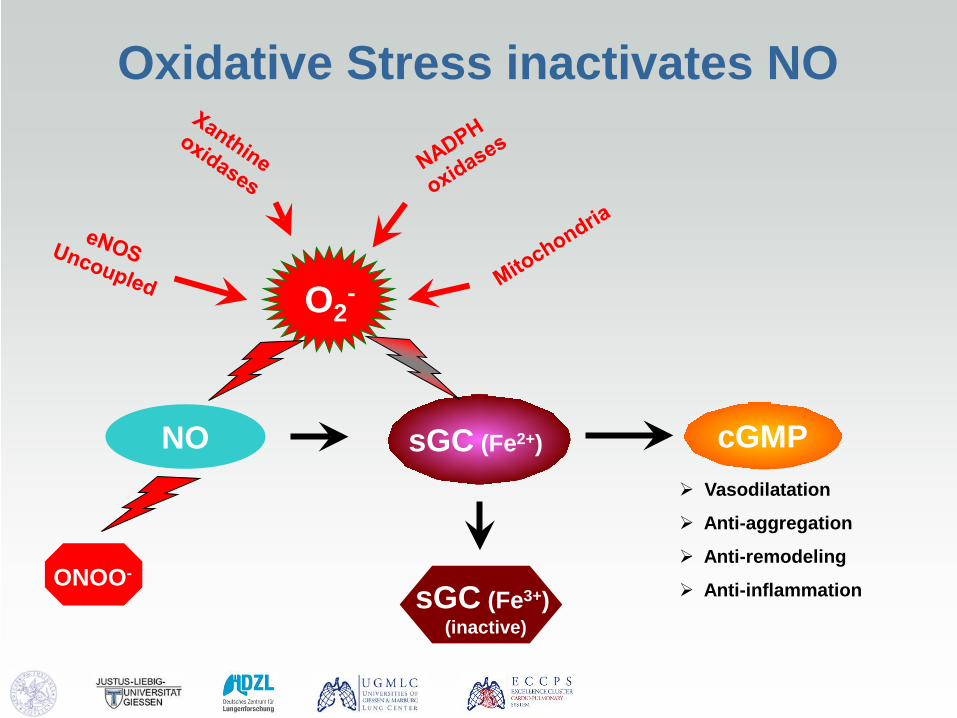
cGMP sGC (Fe2+) NO Vasodilatation
Anti-aggregation
Anti-remodeling
Anti-inflammation
O2-
sGC (Fe3+) (inactive)
ONOO-
Oxidative Stress inactivates NO
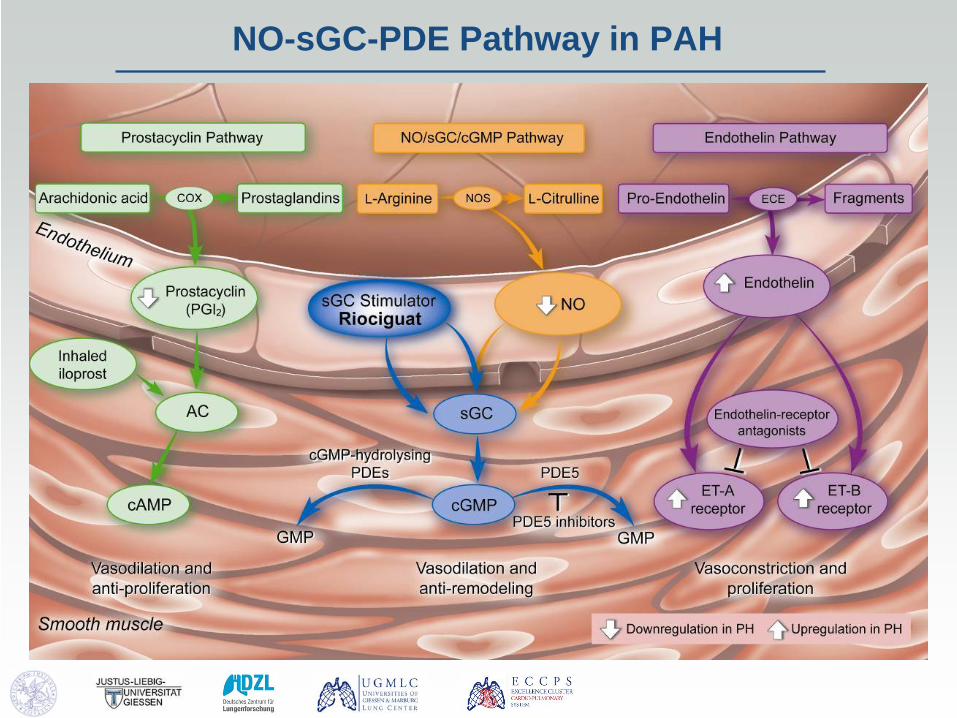
NO-sGC-PDE Pathway in PAH

RISK FACTOR (autoimmunity, HIV,
drugs,toxins…)
GENETIC PREDISPOSITION
(BMPR2, ALK-1, 5-HTT..)
PULMONARY VASCULAR DYSFUNCTION
Endothelial cell dysfunction
(NO, PgI2, ET-1…)
Smooth muscle cell dysfunction
(Kv1.5…)
INFLAMMATION/REMODELING (IL-1, IL-6, PDGF,
Chemokines…)
PULMONARY VASCULAR REMODELING DISEASE PROGRESSION
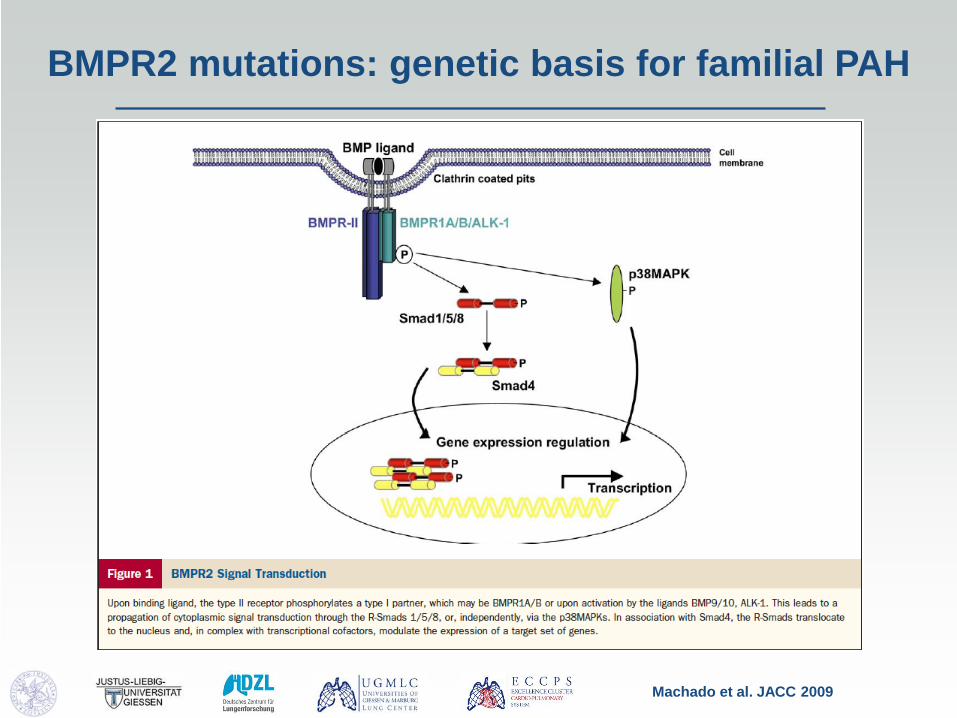
BMPR2 mutations: genetic basis for familial PAH
Machado et al. JACC 2009

Genetics
Mutation in gene encoding for bone morphogenetic protein receptor 2 (BMPR2) in 16 of 27 IPAH families
Deng et al, Am J Human Genet 2000;67:737-44, and Internat PPH Consortium Nat Genet 2000;26:81-4
BMP’s are members of the TGFβ superfamily BMPR2-smad signalling inhibits proliferation
BMPR2 mutations as a cause of PAH
Estimated < 10 – 20 % incidence of PAH in carriers of BMPR2 mutations
Not all familial PAH have detectable BMPR2 mutations
Incidence of BMPR2 mutations 5 % in sporadic IPAH BMPR2 mutations uncommon in other PAH
categories (anorexigens, CHD) BMPR2 mutations neither necessary nor sufficient

Genetics in PAH
Machado et al. JACC 2009
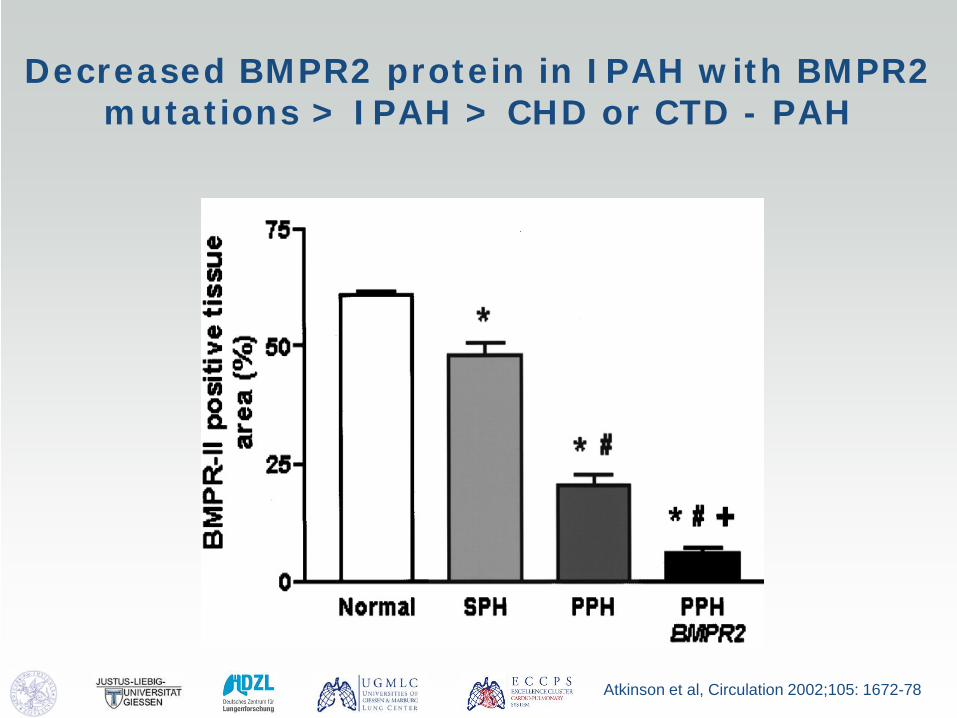
Decreased BMPR2 protein in IPAH with BMPR2 mutations > IPAH > CHD or CTD - PAH
Atkinson et al, Circulation 2002;105: 1672-78
Risk factor: HIV
• HIV infection is an established risk factor for PH • The use of highly active antiretroviral therapy (HAART) has
increased the life expectancy of HIV-infected patients. • With prolonged survival and improved control of infectious
susceptibility, vascular complications have emerged as a significant source of morbidity and mortality in HIV-infected patients
• These vascular complications, affecting >10% of those with HIV infections, include myocardial and pericardial tumours, cardiomyopathy, peripheral vasculitides, ischaemic heart disease and pulmonary arterial hypertension
• HIV-infected patients have a 2500-fold increased risk of developing PAH
• Mechanismsm unknown (evidence that the HIV proteins Env, Tat and Nef are implicated in cardiopulmomary complications)
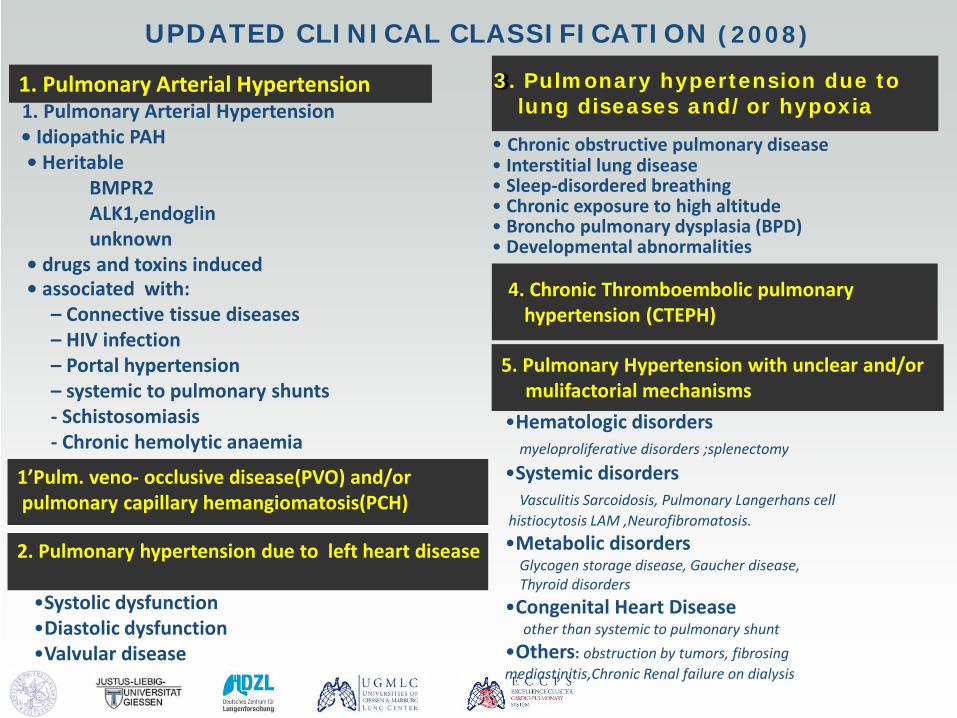
UPDATED CLINICAL CLASSIFICATION (2008)
1. Pulmonary Arterial Hypertension 1. Pulmonary Arterial Hypertension • Idiopathic PAH • Heritable BMPR2 ALK1,endoglin unknown • drugs and toxins induced • associated with: – Connective tissue diseases – HIV infection – Portal hypertension – systemic to pulmonary shunts - Schistosomiasis - Chronic hemolytic anaemia
3. Pulmonary hypertension due to lung diseases and/or hypoxia
2. Pulmonary hypertension due to left heart disease
4. Chronic Thromboembolic pulmonary hypertension (CTEPH)
• Chronic obstructive pulmonary disease • Interstitial lung disease • Sleep-disordered breathing • Chronic exposure to high altitude • Broncho pulmonary dysplasia (BPD) • Developmental abnormalities
•Systolic dysfunction •Diastolic dysfunction •Valvular disease
5. Pulmonary Hypertension with unclear and/or mulifactorial mechanisms
•Hematologic disorders myeloproliferative disorders ;splenectomy
•Systemic disorders Vasculitis Sarcoidosis, Pulmonary Langerhans cell histiocytosis LAM ,Neurofibromatosis. •Metabolic disorders Glycogen storage disease, Gaucher disease, Thyroid disorders •Congenital Heart Disease other than systemic to pulmonary shunt •Others: obstruction by tumors, fibrosing mediastinitis,Chronic Renal failure on dialysis
1’Pulm. veno- occlusive disease(PVO) and/or pulmonary capillary hemangiomatosis(PCH)

Vascular obstruction Chronic vasoconstriction Proliferation/Apoptosis
Migration/ECM synthesis Disturbed metabolism
Endothelial Dysfunction In-situ thrombosis
Inflammation
disease
Respiratory unit with pre-capillary resistance vessel
alveolus
endothelium
alveolus
Type II AEC
Type I AEC
Vascular lumen
smooth muscle fibroblasts
health
Cellular and molecular mechanisms of disease induction
Dysregulation of vascular tone PGI2 NO-sGC-cGMP axis PDE Endothelin Serotonin K- and Ca-channels
Abnormal proliferation TGF-beta, BMP Growth factors (PDGF, FGF) Transcription factors (Notch3) Metabolic changes Elastases / MMPs Cytokines and chemokines Hypoxia-induced vasomotion and remodeling HIF ROS Channles (e.g. Kv, TRPC) Mitochondria NADPH Oxidase
Clinical trials Tki, sGC, PDE, Rho-Ki, EPC,…
Schermuly et al. Nat Rev Cardiol 2011

Serotonin (5-HT) abnormalities in PAH
MacLean et al. British Journal of Pharmacology (2000) 131, 161 - 168

Serotonin (5-HT) receptor inhibition with Terguride inhibits MCT-PH
Dumitrascu et al. Eur Respir J 2011; 37: 1104–1118

Ion channels in PAH
Kuhr F K et al. Am J Physiol Heart Circ Physiol 2012;302:H1546-H1562

Vascular obstruction Chronic vasoconstriction Proliferation/Apoptosis
Migration/ECM synthesis Disturbed metabolism
Endothelial Dysfunction In-situ thrombosis
Inflammation
disease
Respiratory unit with pre-capillary resistance vessel
alveolus
endothelium
alveolus
Type II AEC
Type I AEC
Vascular lumen
smooth muscle fibroblasts
health
Cellular and molecular mechanisms of disease induction
Dysregulation of vascular tone PGI2 NO-sGC-cGMP axis PDE Endothelin Serotonin K- and Ca-channels
Abnormal proliferation TGF-beta, BMP Growth factors (PDGF, FGF) Transcription factors (Notch3) Metabolic changes Elastases / MMPs Cytokines and chemokines Hypoxia-induced vasomotion and remodeling HIF ROS Channles (e.g. Kv, TRPC) Mitochondria NADPH Oxidase
Clinical trials Tki, sGC, PDE, Rho-Ki, EPC,…
Schermuly et al. Nat Rev Cardiol 2011

Disordered elastin metabolism and deposition in PAH
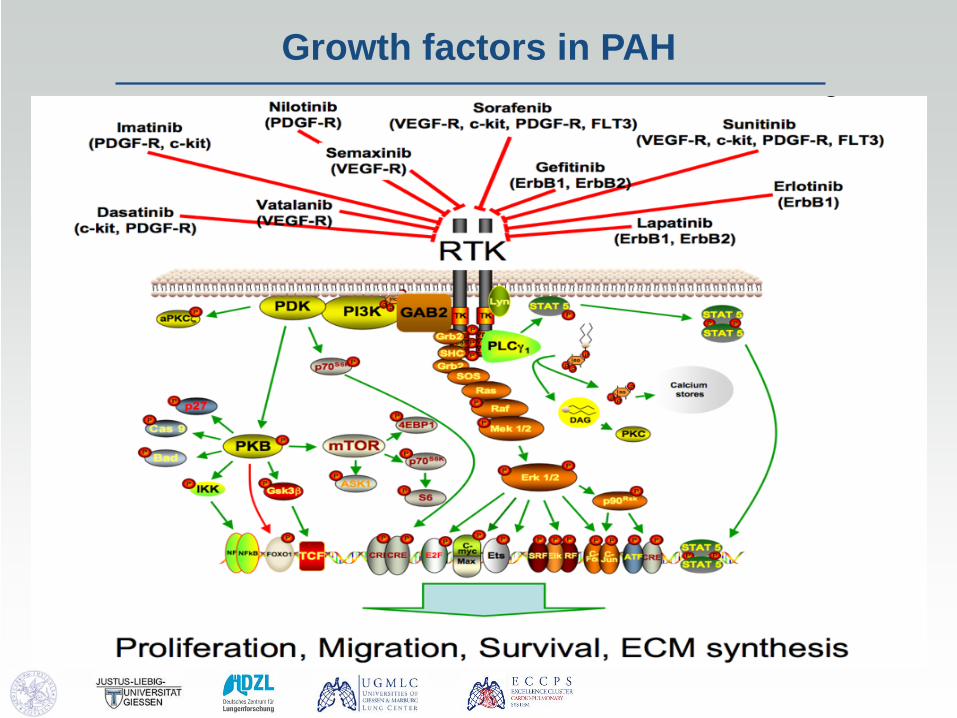
Growth factors in PAH
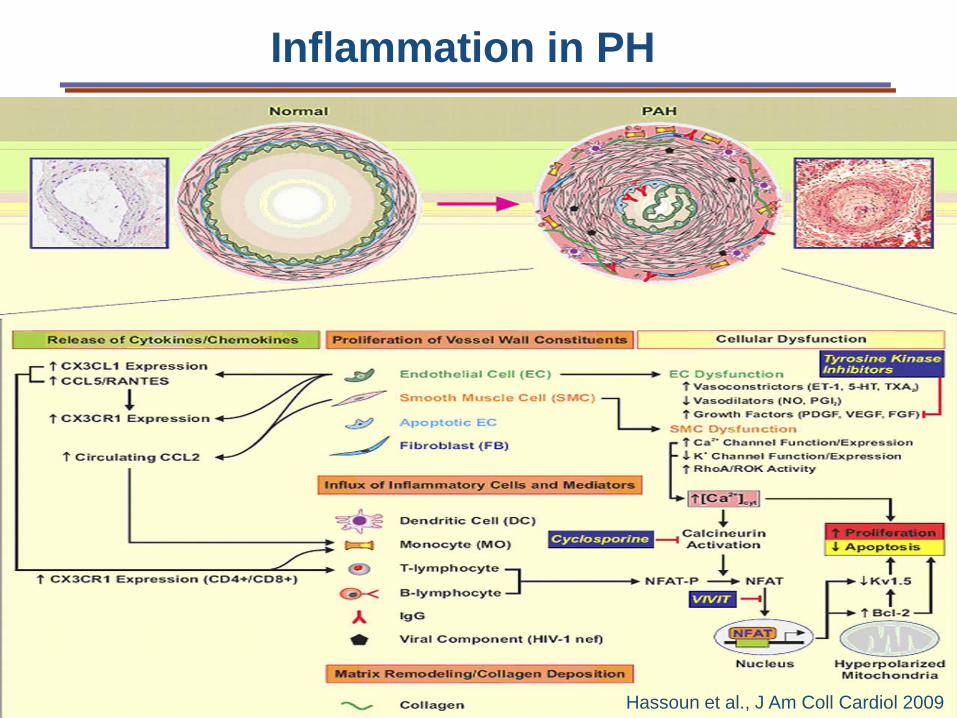
Hassoun et al., J Am Coll Cardiol 2009
Inflammation in PH
Summary
• Vasodilator – vasoconstrictor dysbalance – Endothelin – Prostacyclin – Nitric oxide – Serotonin
• Risk factors: Genetic predisposition (BMPR2, others), HIV infection, drugs, toxins, infections, autoimmune diseases, hypoxia
• Excessive vascular cell growth and inflammation • Proproliferative signaling pathways: growth factors,
cytokines, ion channels, elastases • New treatments: Prostanoids, ET antagonists, sGC
stimulators, RTKi, Metabolic modulators


















