Public Partnerships, LLC (PPL) PPL’s FFissccaall IInntt er...
40
Dear Employee: Welcome aboard! You have received this packet because you intend to provide services as a Personal Attendant to an individual receiving support and funding through the Indiana Family and Social Services Administration (FSSA) Self-Directed Care Program. FSSA has contracted with Public Partnerships, LLC (PPL), a Fiscal Intermediary (FI), to make all payments on behalf of waiver program participants who utilize Personal Attendants. The FI will track all hours worked and pay for services on behalf of your Employer. The FI will also administer the required background checks on all Personal Attendants. PPL asks that you sign and return the enclosed forms as soon as possible. You must complete a separate packet for each Employer who employs you, even if you are hired by two people in the same household. PPL cannot pay any claims until a completed packet is received for your work with each Employer. PPL will issue your paychecks to you based on either telephonic or signed physical timesheets. These paychecks will reflect tax withholdings. If you have any questions, please call or email Public Partnerships at (866) 264- 2296 or INfssa-cs@pcgus.com. Thank you. How do I complete the forms? Is there an easy way to tell which ones apply to me? PPL has enclosed an instruction page for each form to help you complete the appropriate paperwork. We also have enclosed a checklist of all forms you need to return to PPL. Please use this to help you identify which forms to return to us. What should I expect as an Employee? Before you are eligible to provide services on your new job you must: Pass a statewide criminal history check Meet with your Employer to complete an employment contract and verify the information you have provided on your USCIS Form I-9 Complete the enclosed tax forms and submit to PPL for processing Report to your Employer about job performance and scheduling requests After you start your new job you will: Submit time each visit or submit signed timesheets to PPL every 2 weeks Receive a paycheck from PPL, based on time submitted to PPL, every 2 weeks Receive W-2 Wage Statement from PPL, on behalf of your Employer, every year PPL’s Fiscal Intermediary Service Employee Instructions to Create a Payroll Account Public Partnerships, LLC (PPL) IN FSSA Fiscal Intermediary 7776 S Pointe Pkwy W Ste. 150 Phoenix, AZ 85044 Phone: (866) 264-2296 Customer Service Email: INfssa-cs@pcgus.com TTY Phone: (800) 360-5899 Business Fax: (866) 799-9381 Time Sheet Fax: (866) 874-0478
Transcript of Public Partnerships, LLC (PPL) PPL’s FFissccaall IInntt er...

Dear Employee:
Welcome aboard! You have received this packet because you intend to provide services as a Personal Attendant to an individual receiving support and funding through the Indiana Family and Social Services Administration (FSSA) Self-Directed Care Program.
FSSA has contracted with Public Partnerships, LLC (PPL), a Fiscal Intermediary (FI), to make all payments on behalf of waiver program participants who utilize Personal Attendants. The FI will track all hours worked and pay for services on behalf of your Employer. The FI will also administer the required background checks on all Personal Attendants.
PPL asks that you sign and return the enclosed forms as soon as possible. You must complete a separate packet for each Employer who employs you, even if you are hired by two people in the same household. PPL cannot pay any claims until a completed packet is received for your work with each Employer. PPL will issue your paychecks to you based on either telephonic or signed physical timesheets. These paychecks will reflect tax withholdings. If you have any questions, please call or email Public Partnerships at (866) 264- 2296 or [email protected].
Thank you.
How do I complete the forms? Is there an easy way to tell which ones apply to me?
PPL has enclosed an instruction page for each form to help you complete the appropriate paperwork. We also have enclosed a checklist of all forms you need to return to PPL. Please use this to help you identify which forms to return to us.
What should I expect as an Employee?
Before you are eligible to provide services on your new job you must:
Pass a statewide criminal history check
Meet with your Employer to complete an employment contract and verify the information youhave provided on your USCIS Form I-9
Complete the enclosed tax forms and submit to PPL for processing Report to your Employer about job performance and scheduling requests
After you start your new job you will:
Submit time each visit or submit signed timesheets to PPL every 2 weeks Receive a paycheck from PPL, based on time submitted to PPL, every 2 weeks Receive W-2 Wage Statement from PPL, on behalf of your Employer, every year
PPPPLL’’ss FFiissccaall IInntteerrmmeeddiiaarryy SSeerrvviiccee Employee Instructions to Create a Payroll Account
Public Partnerships, LLC (PPL) IN FSSA Fiscal Intermediary 7776 S Pointe Pkwy W Ste. 150 Phoenix, AZ 85044 Phone: (866) 264-2296 Customer Service Email: [email protected] Phone: (800) 360-5899 Business Fax: (866) 799-9381 Time Sheet Fax: (866) 874-0478

Who is responsible for submitting timesheets to PPL?
It is the responsibility of the Employee to call the TIPS telephonic timesheet system to log in and out. If the Employee is submitting paper timesheets, it is the responsibility of the Employer to collect all timesheets from their Personal Attendants for a paycheck cycle and submit them to PPL together. If Personal Attendant timesheets for a single Employer are not submitted together, payments may be delayed or even denied.
What is the US Citizenship and Immigration Service (USCIS) Form I-9?
The USCIS Form I-9 is your employment eligibility verification. You must bring this form, and the documents listed on page 3 of the I-9, to your Employer. Your Employer will review the documents, confirm your identity and verify your identity under penalty of perjury by signing this form. Federal law requires that all Employers and Employees complete this form.
What taxes will be withheld and how will my paycheck stub change?
PPL will withhold Social Security, Medicare (FICA), and state and federal income taxes from your paycheck. A summary of all tax withholdings will appear on your paycheck stub throughout the calendar year. PPL also will mail you a W-2 form in January. You will need this W-2 form to file your individual tax return by April. Your Employer will receive regular reports from PPL about your total year to date wages and taxes paid.
When do I need to complete and return tax forms to Public Partnerships?
You must complete and return the required forms to PPL once you are hired by an Employer. Delays which go beyond the scheduled timeframe may result in payment delay, or inaccurate tax withholding for services you provide to your Employer.
Are there other forms I need to review?
Yes. PPL has enclosed the following forms for your review.
PPL Timesheet and Payment Calendar. A signed timesheet will authorize PPL to issue a paycheck. A timesheet can be completed online, faxed or mailed, but must to be legible, signed and for authorized service dates and hours. Paychecks are issued every other week. See the enclosed Payment Schedule for more information about processing days and deadlines. Please feel free to make copies of the Timesheet form to record Employee hours.
Thank you On behalf of your new Employer and FSSA, PPL would like to thank you for your commitment to individuals and families enrolled in the FI program. PPL encourages you to call or email us at 1-866-264-2296 or [email protected] if you have any questions regarding this new requirement or theprocess in general. PPL staff is available to help walk you through the forms over the phone. Thanks for your attention to this matter.
Sincerely,
PPL Fiscal Intermediary

STEP ONE – MEET WITH YOUR EMPLOYER TO FILL OUT FORMS
USCIS Form I-9 (Filled out by you, Section 2 signed by your employer)
Employment Terms and Conditions
Federal Tax Exemption Information Form
STEP TWO – MAIL FORMS TO PPL
USCIS Form I-9. US Citizenship and Immigration Services (USCIS)
IRS W-4 Form. Employee’s Withholding Allowance Certificate
Form WH-4. Employee’s Withholding Exemption and County Status Certificate
Employment Terms and Conditions
Employee Data Form
Employee Training Checklist
Federal Tax Exemption Information Form
All forms must be signed and returned to PPL prior to issuing paychecks to employees.
If you have any questions, please call PPL at (866) 264-2296 or email PPL at [email protected]
CCHHEECCKK LLIISSTT PPPPLL’’ss FFiissccaall IInntteerrmmeeddiiaarryy SSeerrvviiccee
Public Partnerships, LLC (PPL) IN FSSA Fiscal Intermediary 7776 S Pointe Pkwy W Ste. 150 Phoenix, AZ 85044 Phone: (866) 264-2296 Customer Service Email: [email protected] Phone: (800) 360-5899 Business Fax: (866) 799-9381 Time Sheet Fax: (866) 874-0478
WHERE TO SEND FORMS:Fax: 1-866-799-9381 Mail: Public Partnerships, LLC
ATTN: IN FSSA 776 S Pointe Pkwy W, Suite 150 Phoenix, AZ 85044
Email: [email protected]

EMPLOYER NAME:
EMPLOYEE DATA FORM
PERSONAL INFORMATION
NAME:
PHONE:
ADDRESS:
SS#
OPTIONAL - SEX:
MALE
FEMALE
EMPLOYER NAME:
CITY: STATE: ZIP:
D.O.B.
OPTIONAL - RACE:
BLACK
HISPANIC
ASIAN/ PAC. ISLAND
NAT. AMER. OR ALASKAN
WHITE
OTHER
OPTIONAL - VETERAN STATUS:
SPECIAL DISABLED VETERAN
* Please check one that describes your veteran status.
*Means (A) a veteran who is entitled to compensation (or who, but for the receipt of military retired pay, would beentitled to compensation) under laws administered by the Department of Veteran Affairs for a disability rateof 10-20% in the case of a veteran who has been determined to have a serious employment disability
or (B) a person who was discharged or released from active duty because of a service connected disability.
VIETNAM ERA VETERAN*Means a veteran, any part of whose active military, naval or air service, was during the period August 5, 1964 through
May 7, 1975 who (1) served on active military duty for a period of more than 180 days and was discharged or releasedthere from with other than a dishonorable discharge, or (2) was discharged or released from active dutybecause of a service-connected disability. No veteran can be considered to be a veteran of the
Vietnam era under this paragraph after December 31, 1994.
OPTIONAL - FAMILY INFORMATION
SPOUSE: CHILD: CHILD: CHILD:
* Additional children may be listed on the back of this form.
OPTIONAL - EMERGENCY CONTACTS
CONTACT RELATIONSHIP
D.O.B.M / F D.O.B. M / F D.O.B. M / F D.O.B.
DAYTIME PHONE
*Information provided on this form is confidential and is treated as such. Completion of this data is voluntary and willnot affect your employment status. Identification can be declared at any time prior to, or if applicable, after hire.
CONSUMER NAME:
Employment Terms and Conditions Agreement Page 1 of 3
EMPLOYMENT TERMS AND CONDITIONS AGREEMENT
LETTER OF ACCEPTANCE
The following terms stated in this agreement apply to the following individuals: (please print)
Name of Employer: ______________________________________________
Name of Employee: ______________________________________________
Name of Waiver Program Participant: ______________________________________________
Certain unemployment tax exemptions exist for employers who hire family members. Is there a
family relationship between the Employee and Employer? If so, what is this relationship?
_____________________________________________________________________________
WHEREAS, the State of Indiana, Family and Social Services Administration (FSSA) has designated Public
Partnerships, LLC (PPL) as a Fiscal Intermediary (FI) to provide agent of the employer services on behalf of the
employer stated above, which shall include processing paychecks, performing state and federal withholdings and
reporting, and procuring unemployment insurance, and
WHEREAS, the employer has selected the employee to provide certain services and supports consistent with the
above named Employer’s Service Authorization, and
WHEREAS, the employer will 1) direct the employee on how to deliver services, 2) utilize the individual’s FSSA
funding allocation to support all aspects of the employee’s service, and 3) ensure compliance with the State of Indiana
Program Rules
THEREFORE, the employer and employee hereby agree as follows:
Offer: The employer is pleased to offer the employee a position to provide personal
attendant services to the waiver program participant. The employer believes
there is a good fit between the employee’s skills and interests, and the
individual’s needs.
Expected Start Date:
________/ ________/ _______. This date is contingent on the employee
agreeing to an annual, statewide criminal background check and submitting the
required documents to PPL. Once this information is received, PPL will
conduct the background check and report results to FSSA and the Employer.
Employee must not begin work until informed by PPL that they have been
certified to start.
Wage: $9.80 per hour. The employee will be paid on a bi-weekly schedule per
submission (telephonic, mail or fax) of timesheets to Public Partnerships, LLC,
agent of the employer. A valid timesheet must be signed and dated by the
Employment Terms and Conditions Agreement Page 2 of 3
Benefits:
Supervision:
Registry:
Criminal History:
Transportation:
Termination:
Form I-9:
employee and employer. PPL will withhold appropriate taxes and issue tax
statements based on tax forms filed by the employee and employer, respectively.
The employee is not eligible to receive benefits under this agreement, or
participate in any state pension or retirement plan.
Continued employment will be determined by the FSSA, Division of Aging and
the employer. Employment eligibility is based on satisfactory employee
performance, the employee remaining in good standing with their criminal
background, the employer’s needs, and the availability of State Program funding
for the waiver program participant.
The employee will be listed in a web-based provider registry as an approved
provider available for hire by other waiver program participants. If you do not want to be include in the provider registry please check the opt-out box below:
By signing this agreement, the employee signals his or her understanding that he
or she will be subject to a statewide limited criminal history and the result of the
history may determine employment eligibility.
Also, by signing this agreement, you acknowledge the following federal
regulation that may affect employment: The United States Department of Health
and Human Services-Office of the Inspector General (HHS-OIG) maintains a
List of Excluded Individuals/Entities (LEIE), which includes persons with
convictions for program-related fraud, patient abuse, or licensing board actions.
Medicaid payments cannot be made for services furnished by an excluded person
who is on the LEIE. PPL, in coordination with EverCare Select, is screening
prospective and current attendants monthly to assure compliance with this
federal law.
If the employee is providing transportation to the employer, the employee must
provide a copy of his or her valid driver’s license and proof of insurance. If
there are any changes to an employee’s driving history, the employee is
obligated to update the employer and Fiscal Intermediary.
Either party may terminate this agreement by notifying the other party and PPL,
in writing by submitting the “Notice of Termination” form 5 days prior to formal
separation of employment.
Employer is responsible for proper execution of USCIS Form I-9, as defined in
Instructions for Employment Eligibility Verification, Department of Homeland
Security. Employer must retain original Form I-9. PPL will only provide Form
I-9 in employment packets and retain a forwarded copy in PPL maintained
employee files.
Opt-out
Employment Terms and Conditions Agreement Page 3 of 3
Confidentiality
Upon receipt of information relating to the waiver program participant, the employee will become
a holder of confidential data. The employee agrees to use confidential data solely for carrying out
his/her responsibilities under this agreement.
Indemnification The employee agrees to indemnify and hold PPL and PPL’s principals, agents, employees and
subcontractors harmless for all claims, losses, expenses, fees, including attorney fees, costs and
judgments that may be asserted against PPL based on any acts or omissions of the employee and/or
employer in carrying out their individual responsibilities under this agreement.
Accepted:
__________________________ _________________________________
Employer Signature/Date Employee Signature/Date
Send Signed Agreement to PPL to Finalize EmploymentPlease return one signed copy of this agreement to PPL and keep copies for the employer and employee
records. Upon receipt by PPL, this agreement will be executed. An executed agreement will authorize PPL
to issue paychecks to the employee on behalf of the employer using FSSA funds awarded to the participant.
Public Partnerships, LLC
Fiscal Intermediary
7776 Pointe Pkwy W Ste. 150
(866) 799-9381 Fax
(866) 264-2296 Phone [email protected] Email
Phoenix, AZ 85044

Attendant/Employee Training Checklist
As a participant in the Indiana Self-Directed Attendant Care Program, I, the undersigned, affirm that I have received training in how to fulfill my role in the program and am presently in good understanding of how the program will work and what my responsibilities will be:
• I will complete all necessary paperwork required to become and employee.• I will report my time accurately and appropriately in accordance with the program’s
outlined timekeeping procedures.• I understand that Worker’s Compensation will not be provided by my employer, the fiscal
intermediary (PPL), or the State of Indiana and that I am responsible for my own negligentacts. As such, I will not take on responsibility for services that are outside the range of thejob description, specifically medically-related services.
• I will be treated with dignity and respect, which includes respect of my privacy andconfidentiality, and I will extend this respect to my employer.
• I will report abuse or fraud promptly to the specified authorities.
My signature below affirms that I have read and understood these responsibilities and willdo my best to discharge them.
_____________________________ _________________________ Signature Date

NEED HELP? CALL TOLL FREE 1-866-264-2296
Consumer and Employee Relationship Form
What is the purpose of this form?
Our contract with IN FSSA has specific guidelines as to who is allowed to provide services to our consumers. Please complete this form with your employer.
I ____________________________________ provide services to the (Print Employee’s Name)
Participant/Consumer _____________________________. My relationship to the consumer is (Check One): (Print Participant’s Name)
I hereby certify that the information presented above is correct to the best of my knowledge.
Employer Signature: _______________________________
Employee Signature: _________________________________
I am his/her Spouse
I am his/her Parent
I am his/her Legal Guardian
I am his/her Power of Attorney (POA); or his/her Health Care Representative (HCR); or the person directing care for the consumer (EOR)
I am None of the Above
Public Partnerships, LLC IN FSSA Financial Administrator 7776 S Pointe Pkwy W Ste. 150 Phoenix, AZ 85044
Revised: 6/1/12 PCG Public Partnerships, LLC
Form TE 20 Financial Administrator 7776 Pointe Pkwy W Ste. 150 Phoenix, AZ 85044
Application for Tax Exemptions Based on Age, Student Status, and Family Relationship
State Worked: _____________________________________ Program: _____________________________________
Participant Name: _____________________________ Employer Name: _____________________________________
Employee Name: _____________________________ Employee Date of Birth: ______ /______ /____________
Employees providing domestic services, such as personal assistance, may be exempt from paying certain federal and state taxes based on the employee’s age, student status, or family relationship to the employer. In some cases, the employer may also be exempt based on the employee’s status. If you and your employer qualify for these exemptions you must take them. PCG Public Partnerships will determine the tax exemptions that apply to you and to your employer (see enclosed guidelines). Employee – Please answer all the following questions based on your age, student status, and relationship to the employer:
1. Are you a non-resident alien temporarily in the United States on an F-1, J-1, M-1, or Q-1 visa admitted to the USfor the purpose of providing domestic services?
Yes, that description fits my status. No, that description does not fit my status.
2. Are you the child of the employer (includes adopted children)? Yes, my employer is my parent (mother or father). No, my employer is not my parent.
3. Are you the spouse of the employer? Yes, my employer is my spouse (husband, wife). No, my employer is not my spouse.
4. Are you the parent of the employer (includes adopted children)? Yes, my employer is my child (son or daughter). No, my employer is not my child.
5. If you answered “Yes” to Question 4, check any of the following that apply. If you answered “No”, proceed toQuestion 6.
Yes, I also provide care for my grandchild or step-grandchild in my child’s home. Yes, my grandchild or step-grandchild is under age 18, or has a physical or mental condition that requires
personal care of an adult for at least four continuous weeks during the calendar quarter in which services are performed.
Yes, my child (son or daughter) is widowed or divorced and not remarried, or living with a spouse who has a mental or physical condition which prohibits the spouse from caring for my grandchild for at least four continuous weeks during the calendar quarter in which services are performed.
6. Are you under the age of 18 or do you turn 18 this calendar year? Yes, I am under 18 or am turning 18 this calendar year. No, I am over 18.
If you answered “Yes” to Question 6, answer the following question. If you answered “No”, skip this section. Is the job of performing household services (personal assistance) your principal occupation? Note: Do not answer “Yes” if you are a student.
Yes, performing household services is my principal occupation. No, performing household services is not my principle occupation, or I am a student.
IMPORTANT: You must notify PCG Public Partnerships if your status changes. Employee Signature: ______________________________________ Date: ______/______/__________
Submit to:

Revised: 6/1/12 PCG Public Partnerships, LLC
Form TE 20 Financial Administrator 7776 Pointe Pkwy W Ste. 150 Phoenix, AZ 85044
Guide to Tax Exemptions Based on Age, Student Status, and Family Relationship Employee Copy – Keep for your records
Employees providing domestic services such as personal assistance may be exempt from paying certain federal and state taxes based on the employee’s age, student status or family relationship to the employer. In some cases, the employer may also be exempt from paying certain taxes based on the employee’s status. IMPORTANT: Please see IRS Publication: #926 – Household Employer’s Tax Guide, and IRS website article: “Foreign Student Liability for Social Security and Medicare Taxes” for additional information.
IMPORTANT:
These exemptions are not optional. If the employee and employer qualify for these tax exemptions they mustbe taken.
If the employee’s earnings are exempt from these taxes, the employee may not qualify for the related benefits,such as retirement benefits and unemployment compensation.
The questions regarding family relationship refer to the relationship between the employee and the employer ofrecord (common law employer). In some cases, the program participant is the employer of record. In othercases, the employer of record may be someone other than the program participant. Check program rules.
Program rules may prohibit some types of employees. For example, most Medicaid-funded programs do notpermit a spouse to be paid as an employee for providing services to a spouse. Check program rules.
PCG Public Partnerships will determine the tax exemptions that apply to the employee and employer based onthe information provided by the employee. PCG Public Partnerships cannot provide tax advice.
Tax Exemptions for Non-Resident Students
For a non-resident student in the United States on an F-1, J-1, M-1, or Q-1 visa admitted to the US for the purpose of providing domestic services, the employer and employee are exempt from paying FICA (Social Security and Medicare taxes) and the employer is exempt from paying FUTA (Federal Unemployment Tax) on wages paid to this employee. The employer may also be exempt from paying State Unemployment Insurance, depending on the rules in the state.
Tax Exemptions for Children Employed by Parent
For a child under 21 employed by his or her parent, the employer and employee are exempt from paying FICA (Social Security and Medicare taxes) and the employer is exempt from paying FUTA (Federal Unemployment Tax) on wages paid to this employee until the child (employee) turns 21 years of age. The employer may also be exempt from paying State Unemployment Insurance, depending on the rules in the state.
Tax Exemptions for Spouses Employed Spouses
For a spouse (husband, wife, or domestic partner in some states) employed by his or her spouse, the employer and employee are exempt from paying FICA (Social Security and Medicare taxes) and the employer is exempt from paying FUTA (Federal Unemployment Tax) on wages paid to this employee. The employer may also be exempt from paying State Unemployment Insurance, depending on the rules in the state.
Revised: 6/1/12 PCG Public Partnerships, LLC
Form TE 20 Financial Administrator 7776 Pointe Pkwy W Ste. 150 Phoenix, AZ 85044
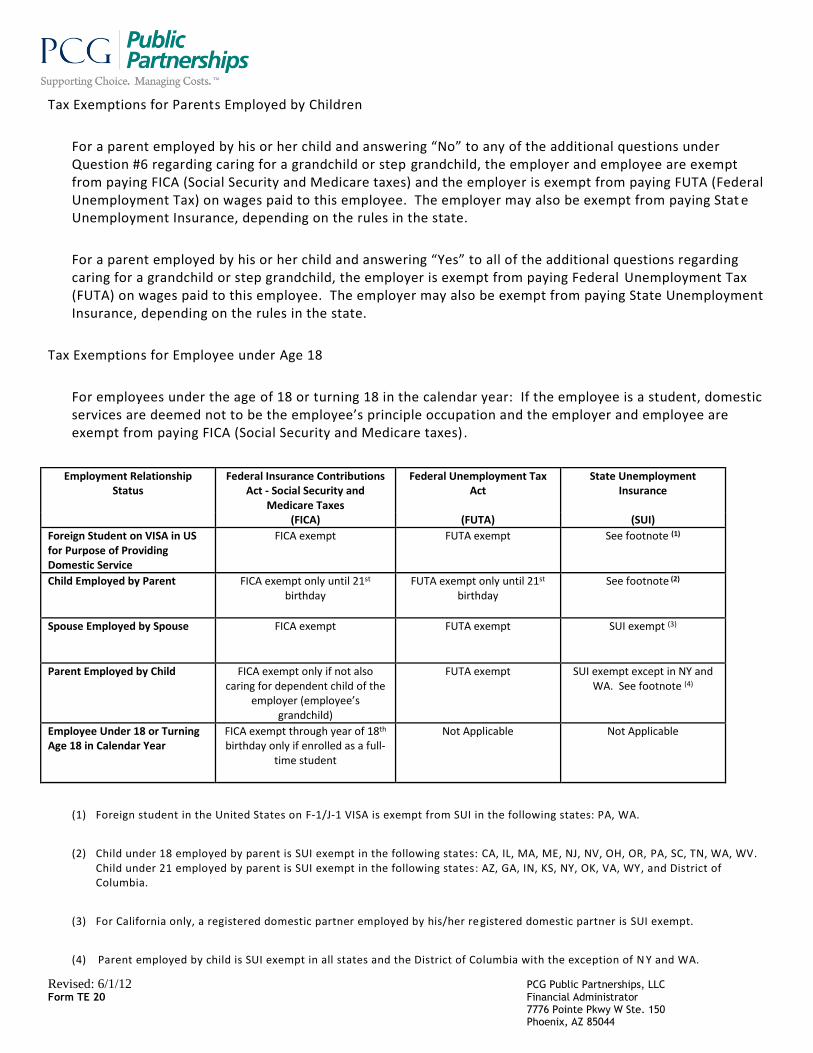
Tax Exemptions for Parents Employed by Children
For a parent employed by his or her child and answering “No” to any of the additional questions under Question #6 regarding caring for a grandchild or step grandchild, the employer and employee are exempt from paying FICA (Social Security and Medicare taxes) and the employer is exempt from paying FUTA (Federal Unemployment Tax) on wages paid to this employee. The employer may also be exempt from paying Stat e Unemployment Insurance, depending on the rules in the state.
For a parent employed by his or her child and answering “Yes” to all of the additional questions regarding caring for a grandchild or step grandchild, the employer is exempt from paying Federal Unemployment Tax (FUTA) on wages paid to this employee. The employer may also be exempt from paying State Unemployment Insurance, depending on the rules in the state.
Tax Exemptions for Employee under Age 18
For employees under the age of 18 or turning 18 in the calendar year: If the employee is a student, domestic services are deemed not to be the employee’s principle occupation and the employer and employee are exempt from paying FICA (Social Security and Medicare taxes) .
Employment Relationship Status
Federal Insurance Contributions Act - Social Security and
Medicare Taxes
Federal Unemployment Tax Act
State Unemployment Insurance
(FICA) (FUTA) (SUI)
Foreign Student on VISA in US for Purpose of Providing Domestic Service
FICA exempt FUTA exempt See footnote (1)
Child Employed by Parent FICA exempt only until 21st birthday
FUTA exempt only until 21st birthday
See footnote (2)
Spouse Employed by Spouse FICA exempt FUTA exempt SUI exempt (3)
Parent Employed by Child FICA exempt only if not also caring for dependent child of the
employer (employee’s grandchild)
FUTA exempt SUI exempt except in NY and WA. See footnote (4)
Employee Under 18 or Turning Age 18 in Calendar Year
FICA exempt through year of 18th birthday only if enrolled as a full-
time student
Not Applicable Not Applicable
(1) Foreign student in the United States on F-1/J-1 VISA is exempt from SUI in the following states: PA, WA.
(2) Child under 18 employed by parent is SUI exempt in the following states: CA, IL, MA, ME, NJ, NV, OH, OR, PA, SC, TN, WA, WV.Child under 21 employed by parent is SUI exempt in the following states: AZ, GA, IN, KS, NY, OK, VA, WY, and District ofColumbia.
(3) For California only, a registered domestic partner employed by his/her re gistered domestic partner is SUI exempt.
(4) Parent employed by child is SUI exempt in all states and the District of Columbia with the exception of N Y and WA.

Public Partnerships, LLC Attention: IN FSSA 7776 S Pointe Pkwy W Suite 150 Phoenix, AZ 85044
Paperwork Reminder: Form I-9
Please note that Federal rules require employees and employers to complete the relevant sections of the Form I-9. Employers must examine identity documents and record the employment eligibility of each employee they wish to hire.
As a reminder, third parties such as PPL are not permitted to complete this form on behalf of you or your employees. It is the responsibility of employers and employees to complete Form I-9 themselves.
PPL provides Employers with an enrollment package with a number of forms, including the Form I-9 and instructions for completing this form. Employers must:
Direct employees they wish to hire to properly and fully complete the I-9 Ensure that the employee completes and signs Section 1 of the I-9 Verify I-9 documentation and complete Section 2 of the I-9 Complete and sign as the employer in the Certification section of the I-9 Forward a copy of the completed I-9, along with all other completed enrollment forms, to PPL for record-keeping purposes
As the employer, you should retain the original Form I-9 for your own records.
PPL will maintain its copy, along with the other enrollment forms, per the records retention terms of the IN FSSA Program.
As always, we are here to assist you. If you have any questions or need further information, please contact PPL Customer Service at 866-264-2296.

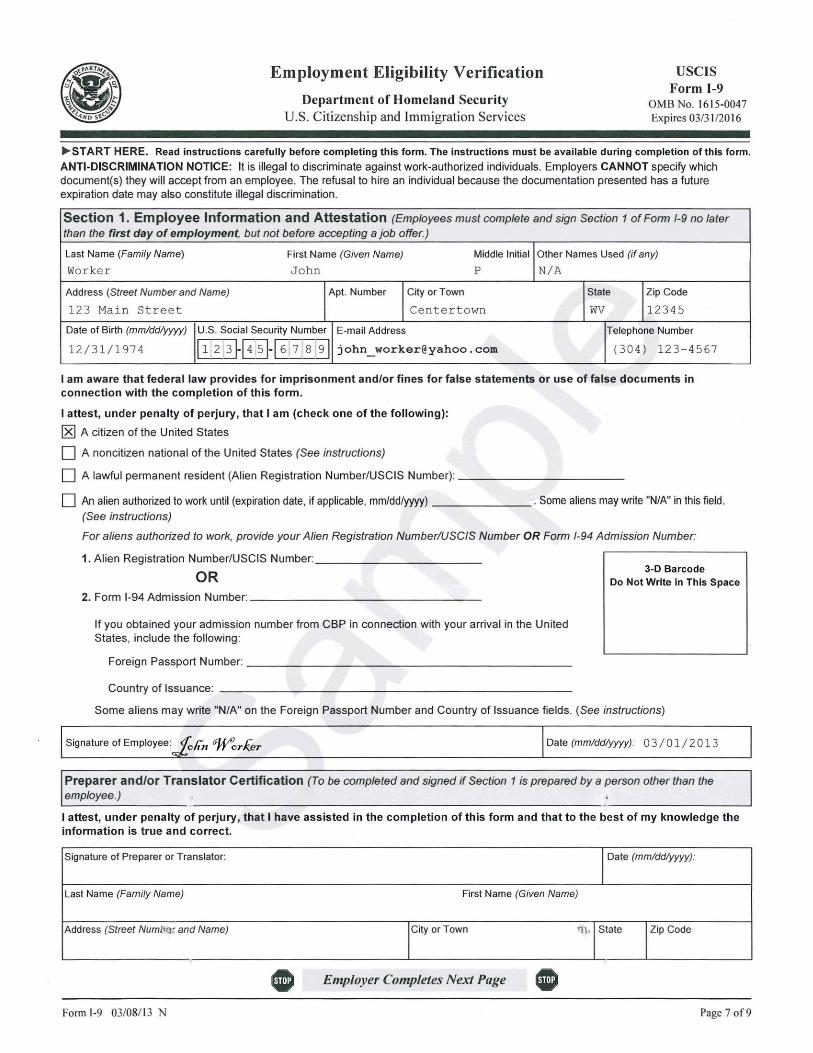
What is it for?
This form tells the USCIS that you – the employee - are eligible for employment in the United States.
Who needs to sign?
Two people need to sign it – 1) the employee and 2) the employer.
Why does the employer need to sign this?
The IRS holds both the employer and the employee responsible for an individual’s legal status and eligibility for employment.
I have a temporary work authorization that needs to be renewed at a later date. Can I still work?
Yes. If you are eligible to work now, you can complete this form. It is important that you keep your work authorizations up-to-date. Your employer will need to verify your status again once your temporary authorization has expired.
Do I need to do anything more than sign the I-9?
Yes. You need to show proof that you are legally eligible to work. There are 10 types of documents that verify work eligibility listed on page 2. Show these documents to your employer when he/she certifies the I-9.
USCIS FORM I-9 Employment Eligibility Verification

Instructions for Employment Eligibility Verification Department of Homeland Security
U.S. Citizenship and Immigration Services
Read all instructions carefully before completing this form.
US CIS Form 1-9
OMB No. 1615-0047 Expires 03/31 /20 16
Anti-Discrimination Notice. It is illegal to discriminate against any work-authorized individual in hiring, discharge, recruitment or referral for a fee, or in the employment eligibility verification (Form I-9 and E-Verify) process based on that individual's citizenship status, immigration status or national origin. Employers CANNOT specify which document(s) they will accept from an employee. The refusal to hire an individual because the documentation presented has a future expiration date may also constitute illegal discrimination. For more information, call the Office of Special Counsel for Immigration-Related Unfair Employment Practices (OSC) at 1-800-255-7688 (employees), 1-800-255-8155 (employers), or 1-800-237-2515 (TDD), or visit www.justice.gov/crt/about/osc.
I what Is the Purpose of This Form?
Employers must complete Form 1-9 to document verification of the identity and employment authorization of each new employee (both citizen and noncitizen) hired after November 6, 1986, to work in the United States. In the Commonwealth of the Northern Mariana Islands (CNMI), employers must complete Form 1-9 to document verification of the identity and employment authorization of each new employee (both citizen and noncitizen) hired after November 27, 2011. Employers should have used Form 1-9 CNMI between November 28, 2009 and November 27, 2011.
I General Instructions
Employers are responsible for completing and retaining Form I-9. For the purpose of completing this form, the term "employer" means all employers, including those recruiters and referrers for a fee who are agricultural associations, agricultural employers, or farm labor contractors. Complete, sign, and submit to PPL.d
Form l-9 is made up of three sections. Employers may be fined if the form is not complete. Employers are responsible for retaining completed forms. Do not mail completed forms to U.S. Citizenship and Immigration Services (USCIS) or Immigration and Customs Enforcement (ICE).
I Section 1. Employee Information and Attestation - Instructions for Employees
Newly hired employees must complete and sign Section 1 of Form Is Section 1 should never be completed before the employee has accepted a job offer. This must be completed before you can start work.Provide the following information to complete Section 1:
Name: Provide your full legal last name, first name, and middle initial. Your last name is your family name or surname. If you have two last names or a hyphenated last name, include both names in the last name field. Your first name is your given name. Your middle initial is the first letter of your second given name, or the first letter of your middle name, if any.
Other names used: Provide all other names used, if any (including maiden name). If you have had no other legal names, write "N/ A." Address: Provide the address where you currently live, including Street Number and Name, Apartment Number (if applicable), (l.ity, State, and Zip Code. Do not provide a post office box address (P.O. JJox). Only border commuters from Canada or Mexico may use an international address in this field.
Date of Birth: Provide your date of birth in the mm/dd/yyyy format. For example, January 23 , 1950, should be written as 01123/1950.
U.S. Social Security Number: Provide your 9-digit Social Security number. Providing your Social Security number is voluntary. However, if your employer participates in E-Verify, you must provide your Social Security number. E-mail Address and Telephone Number (Optional): You may provide your e-mflil address and telephone number. Department of Homeland Security (DHS) may contact you if DHS learns o'f a potential mismatch between the information provided and the information in DHS or Social Security Administration (SSA) records. You may write "N/A" if you choose not to provide this information.
Form I-9 Instructions 03/08/ 13 N EMPLOYERS MUST RETAIN COMPLETED FORM 1-9
DO NOT MAIL COMPLETED FORM 1-9 TO ICE OR USCIS Page l of9

All employees must attest in Section I, under penalty of perjury, to their citizenship or immigration status by checking one of the fo11owing four boxes provided on the form:
1. A citizen of the United States
2. A noncitizen national of the United States: Noncitizen nationals of the United States are persons born in American Samoa, certain former citizens of the former Trust Territory of the Pacific Islands, and certain children of noncitizen nationals born abroad.
3. A lawful permanent resident: A lawful permanent resident is any person who is not a U.S. citizen and who resides in the United States under legally recognized and lawfully recorded permanent residence as an immigrant. The term "lawful permanent resident" includes conditional residents. If you check this box, write either your Alien Registration Number (A-Number) or USCIS Number in the field next to your selection. At this time, the USCIS Number is the same as the A-Number without the "A" prefix.
4. An alien authorized to work: If you are not a citizen or national of the United States or a lawful permanent resident, but are authorized to work in the United States, check this box. If you check this box:
a. Record the date that your employment authorization expires, if any. Aliens whose employment authorization does not expire, such as refugees, asylees, and certain citizens of the Federated States of Micronesia, the Republic ofthe Marshall Islands, or Palau, may write "N/A" on this line.
b. Next, enter your Alien Registration Number (A-Number)/USCIS Number. At thjs time, the USCIS Number is the same as your A-Number without the "A" prefix. If you have not received an A-Number/USCIS Number, record your Admission Number. You can find your Admission Number on Form 1-94, "Arrival-Departure Record," or as directed by USCIS or U.S. Customs and Border Protection (CPB).
(1) If you obtained your admission number from CBP in connection with your arrival in the United States, then also record information about the foreign passport you used to enter the United States (number and country of issuance).
(2) If you obtained your admission number from USCIS within the United States, or you entered the Uruted States without a foreign passport, you must write "N/ A" in the Foreign Passport Number and Country of Issuance fields.
Sign your name in the "Signature of Employee" block and record the date you completed and signed Section 1. By signing and dating this form, you attest that the citizenship or immigration status you selected is correct and that you are aware that you may be imprisoned and/or fined for making false statements or using false documentation when completing this form. To fully complete this form, you must present to your employer documentation that establishes your identity and employment authorization. Choose which documents to present from the Lists of Acceptable Documents, found on the last page of this form. You must present this documentation no later than the third day after beginning employment, although you may present the required documentation before this date.
Preparer and/or Translator Certification - Complete ONLY if someone helped you fill out Section I.M.The Preparer and/or Translator Certification must be completed if the employee requires assistance to complete Section 1 (e.g., the employee needs the instructions or responses translated, someone other than the employee fills out the information blocks, or some~~e with disabilities needs additional assistance). The employee must still ~gn Section 1.
Minors and Certain Employees with Disabilities (Special Placement)
Parents or legal guardians assisting minors (individuals under 18) and certain employees with disabilities should review the guidelines in the Handbookfor Employers: Instructions for Completing Form 1-9 (M-274) on www.uscis.gov/ I-9Central before completing Section 1. these individuals have special procedures for establishing identity if they cannot present an identity document for Form 1-9. The special procedures include (1) the parent or legal guardian filling out Section 1 and writing "mi.r10r under age 18" or "special placement," whichever applies, in the employee signature block; and (2) the employer writi~g "minor under age 18" or "special placement" under List B in Section ·2:'
Form I-9 Instructions 03/08113 N Page 2 of9
Section 2. Employer or Authorized Representative Review and Verification
Before completing Section 2, employers must ensure that Section 1 is completed properly and on time. Employers may not ask an individual to complete Section 1 before he or she has accepted a job offer.
Employers or their authorized representative must complete Section 2 by examining evidence of identity and employment authorization within 3 business days of the employee1S first day of employment. For example, if an employee begins employment on Monday, the employer must complete Section 2 by Thursday of that week. However, if an employer hires an individual for less than 3 business days, Section 2 must be completed no later than the first day of employment. An employer may complete Form I-9 before the first day of employment if the employer has offered the individual a job and the individual has accepted. This must be completed prior to employment.
Employers cannot specify which document(s) employees may present from the Lists of Acceptable Documents, found on the last page of Form I-9, to establish identity and employment authorization. Employees must present one selection from List A OR a combination of one selection from List Band one selection from List C. List A contains documents that show both identity and employment authorization. Some List A documents are combination documents. The employee must present combination documents together to be considered a List A document. For example, a foreign passport and a Form I-94 containing an endorsement of the alien1s nonimmigrant status must be presented together to be considered a List A document. List B contains documents that show identity only, and List C contains documents that show employment authorization only. If an employee presents a List A document, he or she should not present a List Band List C document, and vice versa. If an employer participates in E-Verify, the List B document must include a photograph.
In the field below the Section 2 introduction, employers must enter the last name, first name and middle initial, if any, that the employee entered in Section 1. This will help to identify the pages of the form should they get separated.
Employers or their authorized representative must:
1. Physically examine each original document the employee presents to determine if it reasonably appears to be genuine and to relate to the person presenting it. The person who examines the documents must be the same person who signs Section 2. The examiner of the documents and the employee must both be physically present during the examination of the employee1s documents.
2. Record the document title shown on the Lists of Acceptable Documents, issuing authority, document number and expiration date (if any) from the original document(s) the employee presents. You may write 11N/A 11 in any unused fields. lfthe employee is a student or exchange visitor who presented a foreign passport with a Form I-94, the employer should also enter in Section 2:
a. The student1s Form I-20 or DS-2019 number (Student and Exchange Visitor Information System-SEVIS Number); and the program end date from Form 1-20 or DS-2019.
3. Under Certification, enter the employee1s first day of employment. Temporary staffing agencies may enter the first day the employee was placed in a job pool. Recruiters and recruiters for a fee do not enter the employee1s first day of employment.
4. Provide the name and title of the person completing Section 2 in the Signature of Employer or Authorized Representative field.
5. Sign and date the attestation on the date Section 2 is completed.
6. Record the employer1s business name and address.
7. Return the employee1S documentation.
Employers may, but are not required to, photocopy the document(s) presented. If photocopies are made, they should be made for ALL new hires or reverifications. Photocopies must be retained and presented with Form 1-9 in case of an inspection J:ty DHS or other federal government agency. Employers must always coll?'Blete Section 2 even if they photocopy an employee1s document(s). Making photocopies of an employee1s docume·nt(s) cannot take the place of completing Form I-9. Employers are still responsible for completing and retaining Form I-9.
Form 1-9 Instructions 03/08/13 N Page 3 of9
Unexpired Documents
Generally, only unexpired, original documentation is acceptable. The only exception is that an employee may present a certified copy of a birth certificate. Additionally, in some instances, a document that appears to be expired may be acceptable if the expiration date shown on the face of the document has been extended, such as for individuals with temporary protected status. Refer to the Handbook for Employers: 1nstructionsfor Completing Form 1-9 (M-274) or 1-9 Central (www.uscis.gov/I-9Central) for examples.
Receipts
If an employee is unable to present a required document (or documents), the employee can present an acceptable receipt in lieu of a document from the Lists of Acceptable Documents on the last page of this form. Receipts showing that a person has applied for an initial grant of employment authorization, or for renewal of employment authorization, are not acceptable. Employers cannot accept receipts if employment will last less than 3 days. Receipts are acceptable when completing Form I-9 for a new hire or when reverification is required.
Employees must present receipts within 3 business days of their first day of employment, or in the case of reverification, by the date that reverification is required, and must present valid replacement documents within the time frames described below.
There are three types of acceptable receipts:
1. A receipt showing that the employee has applied to replace a document that was lost, stolen or damaged. The employee must present the actual document within 90 days from the date of hire.
2. The arrival portion of Form I-94/I-94A with a temporary 1-551 stamp and a photograph of the individual. The employee must present the actual Permanent Resident Card (Form I-551) by the expiration date of the temporary 1-551 stamp, or, if there is no expiration date, within 1 year from the date of issue.
3. The departure portion of Form I-94/I-94A with a refugee admission stamp. The employee must present an unexpired Employment Authorization Document (Form 1-766) or a combination of a List B document and an unrestricted Social Security card within 90 days.
When the employee provides an acceptable receipt, the employer should:
1. Record the document title in Section 2 under the sections titled List A, List B, or List C, as applicable.
2. Write the word "receipt" and its document number in the "Document Number" field. Record the last day that the receipt is valid in the "Expiration Date" field.
By the end of the receipt validity period, the employer should:
1. Cross out the word "receipt" and any accompanying document number and expiration date.
2. Record the number and other required document information from the actual document presented.
3. Initial and date the change.
See the Handbook for Employers: 1nstructionsfor Completing Form 1-9 (M-274) at www.uscis.gov/I-9Central for more information on receipts.
I Section 3. Reverification and Rehires Complete this section ONLY if rehiring within 3 years.
Employers or their authorized representatives should complete Section 3 when reverifying that an employee is authorized to work. When rehiring an employee within 3 years of the date Form I-9 was originally completed, employers have the option to complete a new Form l-9 or complete Section 3. When completing Section 3 in either a reverification or rehire situation, ifthe employee's name has changed, record the name change in Block A.
~- ~i
For employees who provide an employment authorization expiration date in Section 1, employers must reverify employment authorization on of before the date provided. ;!·
Form 1-9 Instructions 03/08/13 N Page 4 of9
Some employees may write "N/A" in the space provided for the expiration date in Section 1 if they are aliens whose employment authorization does not expire (e.g., asylees, refugees, certain citizens of the Federated States ofM.icronesia, the Republic of the Marshall Islands, or Palau). Reverification does not apply for such employees unless they chose to present evidence of employment authorization in Section 2 that contains an expiration date and requires reverification, such as Form I-766, Employment Authorization Document.
Reverification applies if evidence of employment authorization (List A or List C document) presented in Section 2 expires. However, employers should not reverify: 1. U.S. citizens and noncitizen nationals; or
2. Lawful permanent residents who presented a Permanent Resident Card (Form I-SS 1) for Section 2.
Reverification does not apply to List B documents.
If both Section 1 and Section 2 indicate expiration dates triggering the reverification requirement, the employer should reverify by the earlier date. For reverification, an employee must present unexpired documentation from either List A or List C showing he or she is still authorized to work. Employers CANNOT require the employee to present a particular document from List A or List C. The employee may choose which document to present.
To complete Section 3, employers should follow these instructions:
1. Complete Block A if an employee's name has changed at the time you complete Section 3.
2. Complete Block B with the date of rehire if you rehire an employee within 3 years of the date this form was originally completed, and the employee is still authorized to be employed on the same basis as previously indicated on this form. Also complete the "Signature of Employer or Authorized Representative" block.
3. Complete Block "C if:
a. The employment authorization or employment authorization document of a current employee is about to expire and requires reverification; or
b. You rehire an employee within 3 years of the date this form was originally completed and his or her employment authorization or employment authorization document has expired. (Complete Block B for this employee as well.)
To complete Block C:
a. Examine either a List A or List C document the employee presents that shows that the employee is currently authorized to work in the United States; and
b. Record the document title, document number, and expiration date (if any).
4. After completing block A, B or C, complete the "Signature of Employer or Authorized Representative" block, including the date.
For reverification purposes, employers may either complete Section 3 of a new Form 1-9 or Section 3 of the previously completed Form I-9. Any new pages of Form I-9 completed during reverification must be attached to the employee's original Form I-9. If you choose to complete Section 3 of a new Form l-9, you may attach just the page containing Section 3, with the employee's name entered at the top of the page, to the employee's original Form 1-9. If there is a more current version ofForm l-9 at the time of reverification, you must complete Section 3 of that version ofthe form.
I What Is the Filing Fee? This will be retained by PPL.
There is no fee for completing Form I-9. This form is not filed with USCIS or any government agency. Form I-9 must be retained by the employer and made available for inspection by U.S. Government officials as specified in the "USCIS Privacy Act Statement" below.
I USCIS Forms and Information
For more detailed information about completing Form I-9, employers and employees should refer to the Handbook for Employers: Instructions for Completing Form 1-9 (M-2 74).
Form l-9lnstructions 03/08/13 N Page 5 of9
' ·

You can also obtain information about Form r-9 from the USCIS Web site at www.uscis.gov/I-9Central, bye-mailing USCIS at [email protected], or by calling 1-888-464-4218. For TDD (hearing impaired), call1-877-875-6028.
To obtain users forms or the Handbook for Employers , you can download them from the users Web site at www.uscis. gov/forms. You may order USCIS forms by calling our toll-free number at 1-800-870-3676. You may also obtain forms and information by contacting the users National Customer Service Center at 1-800-375-5283. For TDD (hearing impaired), cal11-800-767-1833.
Information about E-Verify, a free and voluntary program that allows participating employers to electronically verify the employment eligibility of their newly hired employees, can be obtained from the USCIS Web site at www.dhs.gov/E-Verify, bye-mailing USers at [email protected] or by calling 1-888-464-4218. For TDD (hearing impaired), call 1-877-87 5-6028. PPL will verify electronically.
Employees with questions about Form I-9 and/or E-Verify can reach the USCIS employee hotline by calling 1-888-897-7781. For TDD (hearing impaired), call 1-877-875-6028.
l Photocopying and Retaining Form 1-9
A blank Form I-9 may be reproduced, provided all sides are copied. The instructions and Lists of Acceptable Documents must be available to all employees completing this form. Employers must retain each employee's completed Form I-9 for as long as the individual works for the employer. Employers are required to retain the pages of the form on which the employee and employer enter data. If copies of documentation presented by the employee are made, those copies must also be kept with the form. Once the individual's employment ends, the employer must retain this form for either 3 years after the date of hire or 1 year after the date employment ended, whichever is later.
Form I-9 may be signed and retained electronica11y, in compliance with Department of Homeland Security regulations at 8 CFR 274a.2.
l US CIS Privacy Act Statement
AUTHORITIES: The authority for collecting this information is the Immigration Reform and Control Act of 1986, Public Law 99-603 (8 USC 1324a).
PURPOSE: This information is collected by employers to comply with the requirements of the Immigration Reform and Control Act of 1986. This law requires that employers verify the identity and employment authorization of individuals they hire for employment to preclude the unlawful hiring, or recruiting or referring for a fee, of aliens who are not authorized to work in the United States.
DISCLOSURE: Submission of the information required in this form is voluntary. However, failure of the employer to ensure proper completion of this form for each employee may result in the imposition of civil or criminal penalties. In addition, employing individuals knowing that they are unauthorized to work in the United States may subject the employer to civil and/or criminal penalties.
ROUTINE USES: This information will be used by employers as a record of their basis for determining eligibility of an employee to work in the United States. The employer will keep this form and make it available for inspection by authorized officials of the Depar~ment of Homeland Security, Department of Labor, and Office of Special Counsel for Immigration-Related Unfair Employment Practices.
jPaperwork Reduction Act
An agency may not conduct or sponsor an information collection and a person is not required to respond to a collection of information unless it displays a currently valid OMB control number. The public reporting burden for this collection of information is estimated at 35 minutes per response, including the time for reviewing instructions and completing and retaining the form. Send comments regarding this burden estimate or any other aspect of this collectio~ of information, including suggestions for reducing this burden, to: U.S. Citizenship and Immigration Services, Regulatory Coordination Division, Office of Policy and Strategy, 20 Massachusetts Avenue NW, Washington, DC 20529-2140; OMB No. 1615-0047. Do not mail your completed Form l-9 to this address.
Form l-9 Instructions 03/08/ L 3 N Page 6 of9
Employment Eligibility Verification Department of Homeland Security
U.S. Citizenship and Immigration Services
USC IS Form l-9
OMB No. 161 5-0047 Expires 03/31/20 16
.... START HERE. Read instructions carefully before completing this form. The instructions must be available during completion of this form. ANTI-DISCRIMINATION NOTICE: It is illegal to discriminate against work-authorized individuals. Employers CANNOT specify which document(s) they will accept from an employee. The refusal to hire an individual because the documentation presented has a future expiration date may also constitute illegal discrimination.
Section 1. Employee Information and Attestation (Employees must complete and sign Section 1 of Form 1-9 no later than the first day of employment, but not before accepting a job offer.)
Last Name (Family Name) First Name (Given Name) Middle Initial Other Names Used (if any)
Worker John p N/A
Address (Street Number and Name) Apt. Number City or Town State Zip Code
123 Main Street Cen t ertown wv 12345 Date of Birth (mmlddlyyyy) E-mail Address Telephone Number
12/31/ 1 974 I U.S. Social Security Number
~-[I~-[II 7 1 s ~ [email protected] (304 ) 123 - 456 7
I am aware that federal law provides for imprisonment and/or fines for false statements or use of false documents in connection with the completion of this form.
I attest, under penalty of perjury, that I am (check one of the following):
[8] A citizen of the United States
D A noncitizen national of the United States (See instructions)
D A lawful permanent resident (Alien Registration Number/USCIS Number): ------------
0 An alien authorized to work until (expiration date, if applicable, mm/dd/yyyy) _______ . Some aliens may write "N/A" in this field . (See instructions)
For aliens authorized to work, provide your Alien Registration Number/USCIS Number OR Form 1-94 Admission Number:
1. Alien Registration Number/USCIS Number: ___________ _
OR 3-D Barcode
Do Not Write in This Space
2. Form 1-94 Admission Number:-----------------
If you obtained your admission number from CBP in connection with your arrival in the United States, include the fo llowing :
Foreign Passport Number: -----------------------
Country of Issuance: -------------------------
Some aliens may write "N/A" on the Foreign Passport Number and Country of Issuance fields. (See instructions)
Signature of Employee: John Worker Date (mmldd/yyyy): 0 3/01 I 2 013
Pre parer and/or Translator Certificat ion (To be completed and signed if Section 1 is prepared by a person other than the employee.)
I attest, under penalty of perjury, that I have assisted in the completion of th is form and that to the best of my knowledge the information is true and correct.
Signature of Pre parer or Translator: I Date (mmlddlyyyy):
Last Name (Family Name) First Name (Given Name)
Address (Street Numi,~r. and Name) City or Town 'I I State Zip Code
I Employer Completes Next Page • Form l-9 03/08/13 N Page 7 of 9

Section 2. Employer or Authorized Representative Review and Verification (Employers or their authorized representative must complete and sign Section 2 within 3 business days of the employee's first day of employment. You must physically examine one document from List A OR examine a combination of one document from List Band one document from List Cas listed on the "Lists of Acceptable Documents" on the next page of this form. For each document you review, record the following information: document title, issuing authority, document number, and expiration date, if any.)
Employee Last Name, First Name and Middle Initial from Section 1:
List A Identity and Employment Authorization
Document Title:
Issuing Authority:
Document Number:
Expiration Date (if any)(mmlddlyyyy):
Document Title :
Issuing Authority:
Document Number:
Expiration Date (if any)(mmlddlyyyy):
Document Title :
Issuing Authority:
Document Number:
Expiration Date (if any)(mm/ddlyyyy) :
Certification
OR List B Identity
Document Title: Drive r s Li cense
Issuing Authority: wv DMV
Document Number: WV- 124 7 95
Expiration Date (if any)(mmlddlyyyy) : 1213112017
AND List C Employment Authorization
Document Title : Soc i al Security Card
Issuing Authority: Social Secur ity Adm i n Document Number: 1 2 3 - 4 5-67 89
Expiration Date (if any)(mmlddlyyyy): N/A
3-D Barcode Do Not Write in This Space
I attest, under penalty of perjury, that (1) I have examined the document(s) presented by the above-named employee, (2) the above-listed document(s) appear to be genuine and to relate to the employee named, and (3) to the best of my knowledge the employee is authorized to work in the United States.
The employee's first day of employment (mmlddlyyyy) : 0 3 I 01 I 2 013 (See instructions for exemptions.) Signature of Employer or Authorized Representati I Date (mmldd!YYW) I Title of Employer or Authorized Representative
0310112013 Emp l oyer o f Record Last Na
Jane Boss mily Name) First Name (Given Name) I Employer's Business or Organization Name
Bos s Jane J a ne Bos s Employer's Business or Organization Address (Street Number and Name) City or Town State Zip Code
234 Main Street Centerbu rg wv 12345
Section 3. Reverification and Rehires (To be completed and ~;· ;gned by employer or authorized representative.) A. New Name (if applicable) Last Name (Family Name) First Name (Given Name} Middle Initial I B. Date of Rehire (if applicable) (mmldd/yyyy).'
C. If employee's previous grant of employment authorization has expired, provide the information for the document from List A or List C the employee presented that establishes current employment authorization in the space provided below.
Document Title : Document Number: I Expiration Date (if any)(mmlddlyyyy):
I attest, under penalty of perjury, that to the best of my knowledgel)~~·is employee is authorized to work in the United States, and if the employee presented document(s}, the document(s) I have examined appear to be genuine and to relate to the individual.
Signature of Employer or Authorized Representative: Date (mm!ddlyyyy): : Print Name of Employer or Authorized Representative:
Form I -9 03/0811 3 N Page 8 of 9

USCIS Form I-9
OMB No. 1615-0047 Expires 08/31/2019
Employment Eligibility Verification Department of Homeland Security
U.S. Citizenship and Immigration Services
Form I-9 11/14/2016 N Page 1 of 3
►START HERE: Read instructions carefully before completing this form. The instructions must be available, either in paper or electronically,during completion of this form. Employers are liable for errors in the completion of this form.
ANTI-DISCRIMINATION NOTICE: It is illegal to discriminate against work-authorized individuals. Employers CANNOT specify which document(s) an employee may present to establish employment authorization and identity. The refusal to hire or continue to employ an individual because the documentation presented has a future expiration date may also constitute illegal discrimination.
Section 1. Employee Information and Attestation (Employees must complete and sign Section 1 of Form I-9 no laterthan the first day of employment, but not before accepting a job offer.)Last Name (Family Name) First Name (Given Name) Middle Initial Other Last Names Used (if any)
Address (Street Number and Name) Apt. Number City or Town State ZIP Code
Date of Birth (mm/dd/yyyy) U.S. Social Security Number
- -
Employee's E-mail Address Employee's Telephone Number
I am aware that federal law provides for imprisonment and/or fines for false statements or use of false documents in connection with the completion of this form.
I attest, under penalty of perjury, that I am (check one of the following boxes):
1. A citizen of the United States
2. A noncitizen national of the United States (See instructions)
3. A lawful permanent resident
4. An alien authorized to work until (See instructions)
(expiration date, if applicable, mm/dd/yyyy):
(Alien Registration Number/USCIS Number):
Some aliens may write "N/A" in the expiration date field.
Aliens authorized to work must provide only one of the following document numbers to complete Form I-9: An Alien Registration Number/USCIS Number OR Form I-94 Admission Number OR Foreign Passport Number.
1. Alien Registration Number/USCIS Number:
2. Form I-94 Admission Number:
3. Foreign Passport Number:
Country of Issuance:
OR
OR
QR Code - Section 1 Do Not Write In This Space
Signature of Employee Today's Date (mm/dd/yyyy)
Preparer and/or Translator Certification (check one): I did not use a preparer or translator. A preparer(s) and/or translator(s) assisted the employee in completing Section 1.(Fields below must be completed and signed when preparers and/or translators assist an employee in completing Section 1.)I attest, under penalty of perjury, that I have assisted in the completion of Section 1 of this form and that to the best of my knowledge the information is true and correct.Signature of Preparer or Translator Today's Date (mm/dd/yyyy)
Last Name (Family Name) First Name (Given Name)
Address (Street Number and Name) City or Town State ZIP Code
Employer Completes Next Page

Form I-9 11/14/2016 N Page 2 of 3
USCIS Form I-9
OMB No. 1615-0047 Expires 08/31/2019
Employment Eligibility Verification Department of Homeland Security
U.S. Citizenship and Immigration Services
Section 2. Employer or Authorized Representative Review and Verification (Employers or their authorized representative must complete and sign Section 2 within 3 business days of the employee's first day of employment. You must physically examine one document from List A OR a combination of one document from List B and one document from List C as listed on the "Lists of Acceptable Documents.")
Last Name (Family Name) M.I.First Name (Given Name)Employee Info from Section 1 Citizenship/Immigration Status
List AIdentity and Employment Authorization Identity Employment Authorization
OR List B AND List C
Additional Information QR Code - Sections 2 & 3 Do Not Write In This Space
Document Title
Issuing Authority
Document Number
Expiration Date (if any)(mm/dd/yyyy)
Document Title
Issuing Authority
Document Number
Expiration Date (if any)(mm/dd/yyyy)
Document Title
Issuing Authority
Document Number
Expiration Date (if any)(mm/dd/yyyy)
Document Title
Issuing Authority
Document Number
Expiration Date (if any)(mm/dd/yyyy)
Document Title
Issuing Authority
Document Number
Expiration Date (if any)(mm/dd/yyyy)
Certification: I attest, under penalty of perjury, that (1) I have examined the document(s) presented by the above-named employee, (2) the above-listed document(s) appear to be genuine and to relate to the employee named, and (3) to the best of my knowledge theemployee is authorized to work in the United States. The employee's first day of employment (mm/dd/yyyy): (See instructions for exemptions)
Signature of Employer or Authorized Representative Today's Date(mm/dd/yyyy) Title of Employer or Authorized Representative
Last Name of Employer or Authorized Representative First Name of Employer or Authorized Representative Employer's Business or Organization Name
Employer's Business or Organization Address (Street Number and Name) City or Town State ZIP Code
Section 3. Reverification and Rehires (To be completed and signed by employer or authorized representative.)A. New Name (if applicable)Last Name (Family Name) First Name (Given Name) Middle Initial
B. Date of Rehire (if applicable)Date (mm/dd/yyyy)
Document Title Document Number Expiration Date (if any) (mm/dd/yyyy)
C. If the employee's previous grant of employment authorization has expired, provide the information for the document or receipt that establishescontinuing employment authorization in the space provided below.
I attest, under penalty of perjury, that to the best of my knowledge, this employee is authorized to work in the United States, and if the employee presented document(s), the document(s) I have examined appear to be genuine and to relate to the individual. Signature of Employer or Authorized Representative Today's Date (mm/dd/yyyy) Name of Employer or Authorized Representative
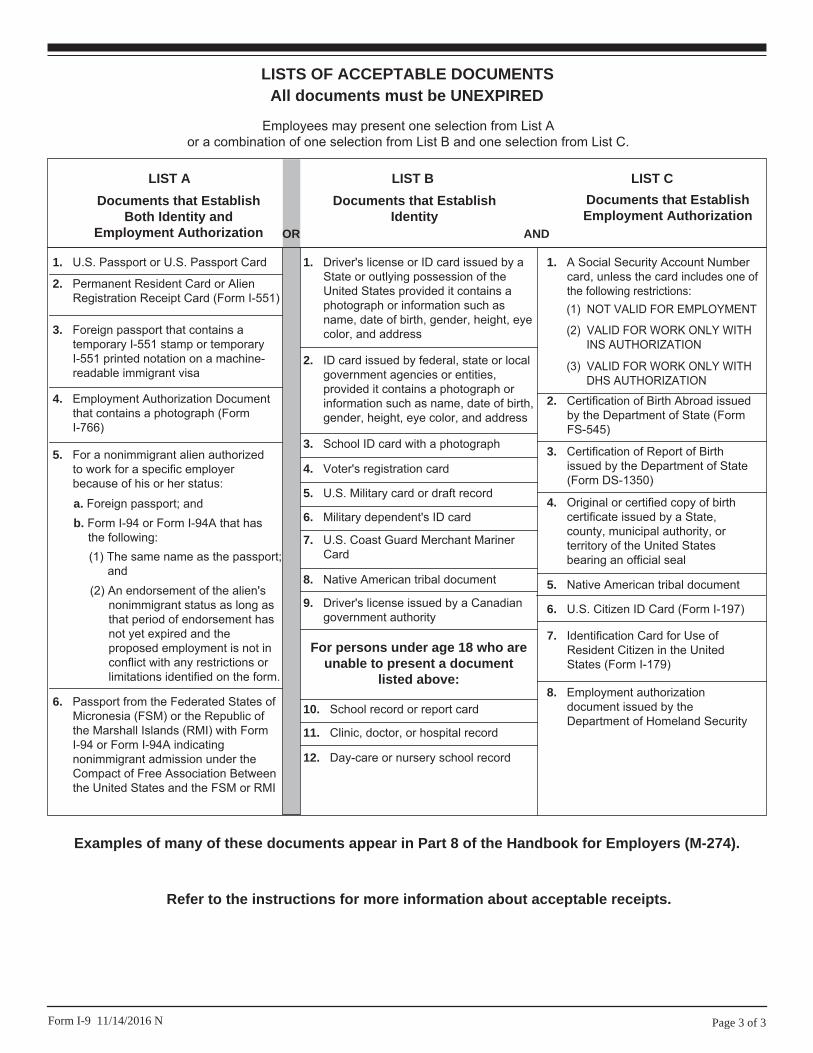
LISTS OF ACCEPTABLE DOCUMENTSAll documents must be UNEXPIRED
Employees may present one selection from List A or a combination of one selection from List B and one selection from List C.
LIST A
2. Permanent Resident Card or AlienRegistration Receipt Card (Form I-551)
1. U.S. Passport or U.S. Passport Card
3. Foreign passport that contains atemporary I-551 stamp or temporaryI-551 printed notation on a machine-readable immigrant visa
4. Employment Authorization Documentthat contains a photograph (FormI-766)
5. For a nonimmigrant alien authorizedto work for a specific employerbecause of his or her status:
Documents that Establish Both Identity and
Employment Authorization
6. Passport from the Federated States ofMicronesia (FSM) or the Republic ofthe Marshall Islands (RMI) with FormI-94 or Form I-94A indicatingnonimmigrant admission under theCompact of Free Association Betweenthe United States and the FSM or RMI
b. Form I-94 or Form I-94A that hasthe following:(1) The same name as the passport;
and(2) An endorsement of the alien's
nonimmigrant status as long asthat period of endorsement hasnot yet expired and theproposed employment is not inconflict with any restrictions orlimitations identified on the form.
a. Foreign passport; and
For persons under age 18 who are unable to present a document
listed above:
1. Driver's license or ID card issued by aState or outlying possession of theUnited States provided it contains aphotograph or information such asname, date of birth, gender, height, eyecolor, and address
9. Driver's license issued by a Canadiangovernment authority
3. School ID card with a photograph
6. Military dependent's ID card
7. U.S. Coast Guard Merchant MarinerCard
8. Native American tribal document
10. School record or report card
11. Clinic, doctor, or hospital record
12. Day-care or nursery school record
2. ID card issued by federal, state or localgovernment agencies or entities,provided it contains a photograph orinformation such as name, date of birth,gender, height, eye color, and address
4. Voter's registration card
5. U.S. Military card or draft record
Documents that Establish Identity
LIST B
OR AND
LIST C
8. Employment authorizationdocument issued by theDepartment of Homeland Security
1. A Social Security Account Numbercard, unless the card includes one ofthe following restrictions:
2. Certification of Birth Abroad issuedby the Department of State (FormFS-545)
3. Certification of Report of Birthissued by the Department of State(Form DS-1350)
4. Original or certified copy of birthcertificate issued by a State,county, municipal authority, orterritory of the United Statesbearing an official seal
5. Native American tribal document
7. Identification Card for Use ofResident Citizen in the UnitedStates (Form I-179)
Documents that Establish Employment Authorization
6. U.S. Citizen ID Card (Form I-197)
(2) VALID FOR WORK ONLY WITHINS AUTHORIZATION
(3) VALID FOR WORK ONLY WITHDHS AUTHORIZATION
(1) NOT VALID FOR EMPLOYMENT
Page 3 of 3Form I-9 11/14/2016 N
Examples of many of these documents appear in Part 8 of the Handbook for Employers (M-274).
Refer to the instructions for more information about acceptable receipts.

What is it for?
This form tells the IRS about the withholding allowances for which the employee is eligible.
Who needs to sign?
Every employee working with an employer who is using the FI.
What if an employee does not want to sign this tax form?
The FI needs this form completed and signed in order to withhold taxes with the employee’s desired allowances. In order to pay an employee, the FI must have a completed and signed form on file.
How should I complete the W-4 worksheet?
The FI cannot give advice about what allowances you should claim. If you have questions about what allowances you should claim, contact your tax professional.
IRS FORM W-4 Employee’s Withholding Allowing Certificate
Form W-4 (2019)Future developments. For the latest information about any future developments related to Form W-4, such as legislation enacted after it was published, go to www.irs.gov/FormW4.Purpose. Complete Form W-4 so that your employer can withhold the correct federal income tax from your pay. Consider completing a new Form W-4 each year and when your personal or financial situation changes.Exemption from withholding. You may claim exemption from withholding for 2019 if both of the following apply.• For 2018 you had a right to a refund of all federal income tax withheld because you had no tax liability, and
• For 2019 you expect a refund of all federal income tax withheld because you expect to have no tax liability.If you’re exempt, complete only lines 1, 2, 3, 4, and 7 and sign the form to validate it. Your exemption for 2019 expires February 17, 2020. See Pub. 505, Tax Withholding and Estimated Tax, to learn more about whether you qualify for exemption from withholding.
General Instructions
If you aren’t exempt, follow the rest of these instructions to determine the number of withholding allowances you should claim for withholding for 2019 and any additional amount of tax to have withheld. For regular wages, withholding must be based on allowances you claimed and may not be a flat amount or percentage of wages.
You can also use the calculator at www.irs.gov/W4App to determine your tax withholding more accurately. Consider
using this calculator if you have a more complicated tax situation, such as if you have a working spouse, more than one job, or a large amount of nonwage income not subject to withholding outside of your job. After your Form W-4 takes effect, you can also use this calculator to see how the amount of tax you’re having withheld compares to your projected total tax for 2019. If you use the calculator, you don’t need to complete any of the worksheets for Form W-4.
Note that if you have too much tax withheld, you will receive a refund when you file your tax return. If you have too little tax withheld, you will owe tax when you file your tax return, and you might owe a penalty.Filers with multiple jobs or working spouses. If you have more than one job at a time, or if you’re married filing jointly and your spouse is also working, read all of the instructions including the instructions for the Two-Earners/Multiple Jobs Worksheet before beginning. Nonwage income. If you have a large amount of nonwage income not subject to withholding, such as interest or dividends, consider making estimated tax payments using Form 1040-ES, Estimated Tax for Individuals. Otherwise, you might owe additional tax. Or, you can use the Deductions, Adjustments, and Additional Income Worksheet on page 3 or the calculator at www.irs.gov/W4App to make sure you have enough tax withheld from your paycheck. If you have pension or annuity income, see Pub. 505 or use the calculator at www.irs.gov/W4App to find out if you should adjust your withholding on Form W-4 or W-4P. Nonresident alien. If you’re a nonresident alien, see Notice 1392, Supplemental Form W-4 Instructions for Nonresident Aliens, before completing this form.
Specific Instructions
Personal Allowances Worksheet
Complete this worksheet on page 3 first to determine the number of withholding allowances to claim.Line C. Head of household please note: Generally, you may claim head of household filing status on your tax return only if you’re unmarried and pay more than 50% of the costs of keeping up a home for yourself and a qualifying individual. See Pub. 501 for more information about filing status.
Line E. Child tax credit. When you file your tax return, you may be eligible to claim a child tax credit for each of your eligible children. To qualify, the child must be under age 17 as of December 31, must be your dependent who lives with you for more than half the year, and must have a valid social security number. To learn more about this credit, see Pub. 972, Child Tax Credit. To reduce the tax withheld from your pay by taking this credit into account, follow the instructions on line E of the worksheet. On the worksheet you will be asked about your total income. For this purpose, total income includes all of your wages and other income, including income earned by a spouse if you are filing a joint return.Line F. Credit for other dependents. When you file your tax return, you may be eligible to claim a credit for other dependents for whom a child tax credit can’t be claimed, such as a qualifying child who doesn’t meet the age or social security number requirement for the child tax credit, or a qualifying relative. To learn more about this credit, see Pub. 972. To reduce the tax withheld from your pay by taking this credit into account, follow the instructions on line F of the worksheet. On the worksheet, you will be asked about your total income. For this purpose, total
Separate here and give Form W-4 to your employer. Keep the worksheet(s) for your records.
Form W-4Department of the Treasury Internal Revenue Service
Employee’s Withholding Allowance Certificate Whether you’re entitled to claim a certain number of allowances or exemption from withholding is
subject to review by the IRS. Your employer may be required to send a copy of this form to the IRS.
OMB No. 1545-0074
20191 Your first name and middle initial Last name
Home address (number and street or rural route)
City or town, state, and ZIP code
2 Your social security number
3 Single Married Married, but withhold at higher Single rate.
Note: If married filing separately, check “Married, but withhold at higher Single rate.”
4 If your last name differs from that shown on your social security card,
check here. You must call 800-772-1213 for a replacement card.
5 Total number of allowances you’re claiming (from the applicable worksheet on the following pages) . . . . 5
6 Additional amount, if any, you want withheld from each paycheck . . . . . . . . . . . . . . 6 $7 I claim exemption from withholding for 2019, and I certify that I meet both of the following conditions for exemption.
• Last year I had a right to a refund of all federal income tax withheld because I had no tax liability, and
• This year I expect a refund of all federal income tax withheld because I expect to have no tax liability.If you meet both conditions, write “Exempt” here . . . . . . . . . . . . . . . 7
Under penalties of perjury, I declare that I have examined this certificate and, to the best of my knowledge and belief, it is true, correct, and complete.
Employee’s signature
(This form is not valid unless you sign it.) Date
8 Employer’s name and address (Employer: Complete boxes 8 and 10 if sending to IRS and complete boxes 8, 9, and 10 if sending to State Directory of New Hires.)
9 First date of employment
10 Employer identification number (EIN)
For Privacy Act and Paperwork Reduction Act Notice, see page 4. Cat. No. 10220Q Form W-4 (2019)

Form W-4 (2019) Page 2
income includes all of your wages and other income, including income earned by a spouse if you are filing a joint return.Line G. Other credits. You may be able to reduce the tax withheld from your paycheck if you expect to claim other tax credits, such as tax credits for education (see Pub. 970). If you do so, your paycheck will be larger, but the amount of any refund that you receive when you file your tax return will be smaller. Follow the instructions for Worksheet 1-6 in Pub. 505 if you want to reduce your withholding to take these credits into account. Enter “-0-” on lines E and F if you use Worksheet 1-6.
Deductions, Adjustments, and Additional Income Worksheet
Complete this worksheet to determine if you’re able to reduce the tax withheld from your paycheck to account for your itemized deductions and other adjustments to income, such as IRA contributions. If you do so, your refund at the end of the year will be smaller, but your paycheck will be larger. You’re not required to complete this worksheet or reduce your withholding if you don’t wish to do so.
You can also use this worksheet to figure out how much to increase the tax withheld from your paycheck if you have a large amount of nonwage income not subject to withholding, such as interest or dividends.
Another option is to take these items into account and make your withholding more accurate by using the calculator at www.irs.gov/W4App. If you use the calculator, you don’t need to complete any of the worksheets for Form W-4.
Two-Earners/Multiple Jobs Worksheet
Complete this worksheet if you have more than one job at a time or are married filing jointly and have a working spouse. If you
don’t complete this worksheet, you might have too little tax withheld. If so, you will owe tax when you file your tax return and might be subject to a penalty.
Figure the total number of allowances you’re entitled to claim and any additional amount of tax to withhold on all jobs using worksheets from only one Form W-4. Claim all allowances on the W-4 that you or your spouse file for the highest paying job in your family and claim zero allowances on Forms W-4 filed for all other jobs. For example, if you earn $60,000 per year and your spouse earns $20,000, you should complete the worksheets to determine what to enter on lines 5 and 6 of your Form W-4, and your spouse should enter zero (“-0-”) on lines 5 and 6 of his or her Form W-4. See Pub. 505 for details.
Another option is to use the calculator at www.irs.gov/W4App to make your withholding more accurate.Tip: If you have a working spouse and your incomes are similar, you can check the “Married, but withhold at higher Single rate” box instead of using this worksheet. If you choose this option, then each spouse should fill out the Personal Allowances Worksheet and check the “Married, but withhold at higher Single rate” box on Form W-4, but only one spouse should claim any allowances for credits or fill out the Deductions, Adjustments, and Additional Income Worksheet.
Instructions for Employer
Employees, do not complete box 8, 9, or 10. Your employer will complete these boxes if necessary.
New hire reporting. Employers are required by law to report new employees to a designated State Directory of New Hires. Employers may use Form W-4, boxes 8, 9,
and 10 to comply with the new hire reporting requirement for a newly hired employee. A newly hired employee is an employee who hasn’t previously been employed by the employer, or who was previously employed by the employer but has been separated from such prior employment for at least 60 consecutive days. Employers should contact the appropriate State Directory of New Hires to find out how to submit a copy of the completed Form W-4. For information and links to each designated State Directory of New Hires (including for U.S. territories), go to www.acf.hhs.gov/css/employers.
If an employer is sending a copy of Form W-4 to a designated State Directory of New Hires to comply with the new hire reporting requirement for a newly hired employee, complete boxes 8, 9, and 10 as follows. Box 8. Enter the employer’s name and address. If the employer is sending a copy of this form to a State Directory of New Hires, enter the address where child support agencies should send income withholding orders. Box 9. If the employer is sending a copy of this form to a State Directory of New Hires, enter the employee’s first date of employment, which is the date services for payment were first performed by the employee. If the employer rehired the employee after the employee had been separated from the employer’s service for at least 60 days, enter the rehire date.Box 10. Enter the employer’s employer identification number (EIN).

Form W-4 (2019) Page 3
Personal Allowances Worksheet (Keep for your records.)A Enter “1” for yourself . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . A
B Enter “1” if you will file as married filing jointly . . . . . . . . . . . . . . . . . . . . . . . B
C Enter “1” if you will file as head of household . . . . . . . . . . . . . . . . . . . . . . . C
D Enter “1” if: { • You’re single, or married filing separately, and have only one job; or• You’re married filing jointly, have only one job, and your spouse doesn’t work; or• Your wages from a second job or your spouse’s wages (or the total of both) are $1,500 or less.
} D
E Child tax credit. See Pub. 972, Child Tax Credit, for more information.• If your total income will be less than $71,201 ($103,351 if married filing jointly), enter “4” for each eligible child. • If your total income will be from $71,201 to $179,050 ($103,351 to $345,850 if married filing jointly), enter “2” for each eligible child.
• If your total income will be from $179,051 to $200,000 ($345,851 to $400,000 if married filing jointly), enter “1” for each eligible child.
• If your total income will be higher than $200,000 ($400,000 if married filing jointly), enter “-0-” . . . . . . . E
F Credit for other dependents. See Pub. 972, Child Tax Credit, for more information.• If your total income will be less than $71,201 ($103,351 if married filing jointly), enter “1” for each eligible dependent.
• If your total income will be from $71,201 to $179,050 ($103,351 to $345,850 if married filing jointly), enter “1” for every two dependents (for example, “-0-” for one dependent, “1” if you have two or three dependents, and “2” if you have four dependents).
• If your total income will be higher than $179,050 ($345,850 if married filing jointly), enter “-0-” . . . . . . . F
G Other credits. If you have other credits, see Worksheet 1-6 of Pub. 505 and enter the amount from that worksheet here. If you use Worksheet 1-6, enter “-0-” on lines E and F . . . . . . . . . . . . . . . . . . G
H Add lines A through G and enter the total here . . . . . . . . . . . . . . . . . . . . . . H
For accuracy, complete all worksheets that apply. {
• If you plan to itemize or claim adjustments to income and want to reduce your withholding, or if you have a large amount of nonwage income not subject to withholding and want to increase your withholding, see the Deductions, Adjustments, and Additional Income Worksheet below.
• If you have more than one job at a time or are married filing jointly and you and your spouse both work, and the combined earnings from all jobs exceed $53,000 ($24,450 if married filing jointly), see the Two-Earners/Multiple Jobs Worksheet on page 4 to avoid having too little tax withheld.
• If neither of the above situations applies, stop here and enter the number from line H on line 5 of Form W-4 above.
Deductions, Adjustments, and Additional Income Worksheet
Note: Use this worksheet only if you plan to itemize deductions, claim certain adjustments to income, or have a large amount of nonwage income not subject to withholding.
1
Enter an estimate of your 2019 itemized deductions. These include qualifying home mortgage interest, charitable contributions, state and local taxes (up to $10,000), and medical expenses in excess of 10% of your income. See Pub. 505 for details . . . . . . . . . . . . . . . . . . . . . . 1 $
2 Enter: { $24,400 if you’re married filing jointly or qualifying widow(er)$18,350 if you’re head of household$12,200 if you’re single or married filing separately
} . . . . . . . . . . . 2 $
3 Subtract line 2 from line 1. If zero or less, enter “-0-” . . . . . . . . . . . . . . . . . 3 $4 Enter an estimate of your 2019 adjustments to income, qualified business income deduction, and any
additional standard deduction for age or blindness (see Pub. 505 for information about these items) . . 4 $5 Add lines 3 and 4 and enter the total . . . . . . . . . . . . . . . . . . . . . . 5 $6 Enter an estimate of your 2019 nonwage income not subject to withholding (such as dividends or interest) . 6 $7 Subtract line 6 from line 5. If zero, enter “-0-”. If less than zero, enter the amount in parentheses . . . 7 $8 Divide the amount on line 7 by $4,200 and enter the result here. If a negative amount, enter in parentheses.
Drop any fraction . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
9 Enter the number from the Personal Allowances Worksheet, line H, above . . . . . . . . . . 9
10
Add lines 8 and 9 and enter the total here. If zero or less, enter “-0-”. If you plan to use the Two-Earners/
Multiple Jobs Worksheet, also enter this total on line 1 of that worksheet on page 4. Otherwise, stop here
and enter this total on Form W-4, line 5, page 1 . . . . . . . . . . . . . . . . . . . 10

Form W-4 (2019) Page 4
Two-Earners/Multiple Jobs Worksheet
Note: Use this worksheet only if the instructions under line H from the Personal Allowances Worksheet direct you here.
1
Enter the number from the Personal Allowances Worksheet, line H, page 3 (or, if you used the Deductions, Adjustments, and Additional Income Worksheet on page 3, the number from line 10 of that worksheet) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
2
Find the number in Table 1 below that applies to the LOWEST paying job and enter it here. However, if you’re married filing jointly and wages from the highest paying job are $75,000 or less and the combined wages for you and your spouse are $107,000 or less, don’t enter more than “3” . . . . . . . . . . . . . 2
3 If line 1 is more than or equal to line 2, subtract line 2 from line 1. Enter the result here (if zero, enter “-0-”) and on Form W-4, line 5, page 1. Do not use the rest of this worksheet . . . . . . . . . . . . 3
Note: If line 1 is less than line 2, enter “-0-” on Form W-4, line 5, page 1. Complete lines 4 through 9 below to figure the additional withholding amount necessary to avoid a year-end tax bill.
4 Enter the number from line 2 of this worksheet . . . . . . . . . . . 4
5 Enter the number from line 1 of this worksheet . . . . . . . . . . . 5
6 Subtract line 5 from line 4 . . . . . . . . . . . . . . . . . . . . . . . . . . 6
7 Find the amount in Table 2 below that applies to the HIGHEST paying job and enter it here . . . . . 7 $8 Multiply line 7 by line 6 and enter the result here. This is the additional annual withholding needed . . . 8 $
9
Divide line 8 by the number of pay periods remaining in 2019. For example, divide by 18 if you’re paid every 2 weeks and you complete this form on a date in late April when there are 18 pay periods remaining in 2019. Enter the result here and on Form W-4, line 6, page 1. This is the additional amount to be withheld from each paycheck . . . . . . . . . . . . . . . . . . . . . . . . . . . 9 $
Table 1
Married Filing Jointly
If wages from LOWEST paying job are—
Enter on line 2 above
$0 - $5,000 05,001 - 9,500 19,501 - 19,500 2
19,501 - 35,000 335,001 - 40,000 440,001 - 46,000 546,001 - 55,000 655,001 - 60,000 760,001 - 70,000 870,001 - 75,000 975,001 - 85,000 1085,001 - 95,000 1195,001 - 125,000 12
125,001 - 155,000 13155,001 - 165,000 14165,001 - 175,000 15175,001 - 180,000 16180,001 - 195,000 17195,001 - 205,000 18205,001 and over 19
All Others
If wages from LOWEST paying job are—
Enter on line 2 above
$0 - $7,000 07,001 - 13,000 1
13,001 - 27,500 227,501 - 32,000 332,001 - 40,000 440,001 - 60,000 560,001 - 75,000 675,001 - 85,000 785,001 - 95,000 895,001 - 100,000 9
100,001 - 110,000 10110,001 - 115,000 11115,001 - 125,000 12125,001 - 135,000 13135,001 - 145,000 14145,001 - 160,000 15160,001 - 180,000 16180,001 and over 17
Table 2
Married Filing Jointly
If wages from HIGHEST paying job are—
Enter on line 7 above
$0 - $24,900 $42024,901 - 84,450 50084,451 - 173,900 910
173,901 - 326,950 1,000326,951 - 413,700 1,330413,701 - 617,850 1,450617,851 and over 1,540
All Others
If wages from HIGHEST paying job are—
Enter on line 7 above
$0 - $7,200 $4207,201 - 36,975 500
36,976 - 81,700 91081,701 - 158,225 1,000
158,226 - 201,600 1,330201,601 - 507,800 1,450507,801 and over 1,540
Privacy Act and Paperwork Reduction Act Notice. We ask for the information on this form to carry out the Internal Revenue laws of the United States. Internal Revenue Code sections 3402(f)(2) and 6109 and their regulations require you to provide this information; your employer uses it to determine your federal income tax withholding. Failure to provide a properly completed form will result in your being treated as a single person who claims no withholding allowances; providing fraudulent information may subject you to penalties. Routine uses of this information include giving it to the Department of Justice for civil and criminal litigation; to
cities, states, the District of Columbia, and U.S. commonwealths and possessions for use in administering their tax laws; and to the Department of Health and Human Services for use in the National Directory of New Hires. We may also disclose this information to other countries under a tax treaty, to federal and state agencies to enforce federal nontax criminal laws, or to federal law enforcement and intelligence agencies to combat terrorism.
You aren’t required to provide the information requested on a form that’s subject to the Paperwork Reduction Act unless the form displays a valid OMB control number. Books or records relating
to a form or its instructions must be retained as long as their contents may become material in the administration of any Internal Revenue law. Generally, tax returns and return information are confidential, as required by Code section 6103.
The average time and expenses required to complete and file this form will vary depending on individual circumstances. For estimated averages, see the instructions for your income tax return.
If you have suggestions for making this form simpler, we would be happy to hear from you. See the instructions for your income tax return.

FORM WH-4 Employee’s Withholding Exemption and County Status Certificate
What is it for?
This form tells your employer about the withholding allowances for which you are eligible.
Who needs to sign?
Every employee working with an employer who is using the FI.
What if an employee does not want to sign this tax form?
The FI needs this form completed and signed in order to withhold taxes with the employee’s desired allowances. If you do not submit this form to the FI, you will have the same federal and state tax exemptions..
How should I complete the WH-4 worksheet?
The FI cannot give advice about what allowances you should claim. If you have questions about what allowances you should claim, contact your tax professional.

State of IndianaEmployee’s Withholding Exemption and County Status Certificate
This form is for the employer’s records. Do not send this form to the Department of Revenue.The completed form should be returned to your employer.
Full Name _______________________________________________________ Social Security Number or ITIN __________________________
Home Address ________________________________ City _______________________ State ______ Zip Code ______________________
Indiana County of Residence as of January 1: ________________________________________ (See instructions)
Indiana County of Principal Employment as of January 1: _______________________________ (See instructions)
___________________________________________________________________________How to Claim Your Withholding Exemptions
1. You are entitled to one exemption. If you wish to claim the exemption, enter “1” .............................................................................. ___________ Nonresident aliens must skip lines 2 through 6. See instructions
2. If you are married and your spouse does not claim his/her exemption, you may claim it, enter “1” ................................................... ___________3. You are allowed one (1) exemption for each dependent. Enter number claimed ............................................................................... ___________4. Additional exemptions are allowed if: (a) you and/or your spouse are over the age of 65 and/or
(b) if you and/or your spouse are legally blind. Check box(es) for additional exemptions: You are 65 or older □ or blind □ Spouse is 65 or older □ or blind □ Enter the total number of boxes checked ........................................................................................................................................... ___________
5. Add lines 1, 2, 3, and 4. Enter the total here ..................................................................................................................................... ►6. You are entitled to claim an additional exemption for each qualifying dependent (see instructions) .................................................. ►
7. Enter the amount of additional state withholding (if any) you want withheld each pay period ........................................................... $ __________8. Enter the amount of additional county withholding (if any) you want withheld each pay period ......................................................... $ __________
I hereby declare that to the best of my knowledge the above statements are true. Signature: ______________________________________________________________________ Date: __________________________
Form WH-4State Form 48845 (R5 / 12-18)

Instructions for Completing Form WH-4This form should be completed by all resident and nonresident employees having income subject to Indiana state and/or county income tax.
Print or type your full name, Social Security number or ITIN and home address. Enter your Indiana county of residence and county of principal employment as of January 1 of the current year. If you neither lived nor worked in Indiana on January 1 of the current year, enter ‘not applicable’ on the line(s). If you move to (or work in) another county after January 1, your county status will not change until the next calendar tax year.
Nonresident alien limitation. A nonresident alien is allowed to claim only one exemption for withholding tax purposes. If you are a nonresident alien, enter “1” on line 1, then skip to line 7. You are considered to be a nonresident alien if you are not a citizen of the United States and do not meet the green card test and the substantial presence test (get Publication 519 from www.irs.gov for information about these tests).
All other employees should complete lines 1 through 7.
Lines 1 & 2 - You are allowed to claim one exemption for yourself and one for your spouse (if he/she does not claim the exemption for him/herself). If a parent or legal guardian claims you on their federal tax return, you may still claim an exemption for yourself for Indiana purposes. You cannot claim more than the correct number of exemptions; however, you are permitted to claim a lesser number of exemptions if you wish additional withholding to be deducted.
Line 3 - Dependent Exemptions: You are allowed one exemption for each of your dependents based on state guidelines. To qualify as your dependent, a person must receive more than one-half of his/her support from you for the tax year and must have less than $4,150 gross income during the tax year (unless the person is your child and is under age 19 or under age 24 and a full-time student at least during 5 months of the tax year at a qualified educational institution).
Line 4 - Additional Exemptions. You are also allowed one exemption each for you and/or your spouse if either is 65 or older and/or blind.
Line 5 - Add the total of exemptions claimed on lines 1, 2, 3, and 4. Enter the total in the box provided.
Line 6 - Additional Dependent Exemptions. An additional exemption is allowed for certain dependent children that are included on line 3. The dependent child must be a son, stepson, daughter, stepdaughter, foster child, and/or child for whom you are a legal guardian.
Lines 7 & 8 - If you would like an additional amount to be withheld from your wages each pay period, enter the amount on the line provided. NOTE: An entry on this line does not obligate your employer to withhold the amount. You are still liable for any additional taxes due at the end of the tax year. If the employer does withhold the ad-ditional amount, it should be submitted along with the regular state and county tax withholding.
You may file a new Form WH-4 at any time if the number of exemptions increases. You must file a new Form WH-4 within 10 days if the number of exemptions previously claimed by you decreases for any of the following reasons:(a) you divorce (or are legally separated from) your spouse for whom you have been claiming an exemption or your spouse claims him/herself on a separate Form WH-4; or(b) someone else takes over the support of a dependent you claim or you no longer provide more than one-half of the person’s support for the tax year.
Penalties are imposed for willingly supplying false information or information which would reduce the withholding exemption.

DDIIRREECCTT DDEEPPOOSSIITTIINNFFOORRMMAATTIIOONN GGUUIIDDEE
20
Phone: Administrative Fax: (866) 799‐9381 TTY: Timesheet Fax: (866) 874‐0478 Email:
(866)264‐2296(800)360‐5899 [email protected] Web: www.publicpartnerships.com
Direct Deposit, also known as Electronic Funds Transmission (EFT), is the fastest and safest way to receive your paycheck from PPL on behalf of your employer. Your payment can be deposited directly into your checking account, savings account, or to a pay card of your choice. To sign up, review the steps below and complete the Direct Deposit application.
1. Meet Direct Deposit RequirementsComplete the Direct Deposit Application.Agree to immediately notify PPL in writing if you change your bank, account number, accounttype, ABA routing number, or contact information. You may need to submit a new Direct DepositApplication form. Failure to comply with this may result in delay of payment.
2. Submit Direct Deposit Application to PPLOnce you have completed the Direct Deposit application, you must gather and submit account verification documents to PPL. This differs depending on where you want your funds to go: • Checking account: Submit a voided check or a letter from your bank that states the checking
account number where your funds should be deposited.
• Savings account: Submit a letter from your bank that states your savings account number whereyour funds should be deposited.
• Pay card/debit card: Submit documentation from the pay card’s enrollment process or the paycard’s financial entity that verifies the account and the routing numbers.
NOTE: If you choose this option, please note that PPL does not support any particular pay card/debit card financial institution and is not responsible for any fees established by the financial institution. PPL recommends you review all pertaining to your pay card prior to enrolling and activating it.
3. Await confirmation from PPLYour Direct Deposit account will become active after PPL verifies your account number with your bank or pay card. The whole process will take 1 to 2 pay cycles from the time we receive your completed and signed application.
If there is a change in bank account information, your PPL payment account will be taken off Direct Deposit status until the new bank account information is verified. Verification may take a few weeks. You will receive paper checks in the interim period.
The Direct Deposit payment is sent on the check date (see Payroll Schedule) and should be in your bank account 24‐48 hours afterwards. Please note that bank holidays may delay posting. After considering bank holidays, contact PPL if you don’t receive your payment on time.
That’s it! Once your Direct Deposit becomes active, you will receive a summary of your gross wages, tax withholding, etc. on a document called a “Remittance Advice” that is mailed to you. Thank you for signing up – we hope you enjoy having faster access to your payments!

Public Partnerships, LLC - Indiana FSSA Program FORM -EFT1
CREATE OR CHANGE PPL EFT ACCOUNT CLOSE EXISTING PPL EFT ACCOUNT
PAYEE INFORMATION
OR
3 Payee Name 4 Telephone Number
5 Payee Address
6 City 7 State 8 Zip
AUTHORIZATION FOR SET-UP, CHANGE OR CANCELLATIONI authorize PPL to stop making electronic transfers to my account without advance notice. I certify that I'm authorized to contract for entity receiving deposits per this agreement, & that all information provided is accurate.
9 Signature (Required) 10 Title 11 Date
ACCOUNT DETAIL INFORMATION
12 Financial Institution Name (My Bank's Name)
13 Bank Address
14 Bank Routing Number Checking Savings Debit
16 My Account Number
17 Bank City 18 Bank State 19 Bank Zip
CANCELLATION
Cancellation Reason
I do not have access to the PPL Web Portal, please send Remittance Advice
Staff Entry:Date:
PPL Use ONLY
15 Account Type
Sect
ion
5
EIN
SSN
DIRECT DEPOSIT APPLICATION
Sect
ion
4
MAIL WITH VOIDED CHECK TO: Indiana FSSA Program, Public Partnerships, LLC, 7776 S Pointe Pkwy W Ste. 150 Phoenix, AZ 85044
New Debit Card Set-up
Change Account Number
Change Account Type
Cancellation Request
Change Financial Institution
New Direct Deposit Set-up
Check the appropriate box below based on your request.
Sect
ion
1Se
ctio
n 2
Sect
ion
3
Disclosure of your Social Security Number (SSN) is voluntary pursuant to 42 USC 405c2C. PPL will use to file required information returns to IRS.
I authorize PPL to process payments owed to me for services authorized by a IN FSSA Program in the state of Indiana. Per my request, PPL will deposit
my payment directly to my bank account indicated below using Automated Clearing House (ACH) transaction. I recognize that if I fail to provide
complete and accurate information on this form, processing may be delayed or made impossible, or my electronic payments may be erroneously
made. I certify I have read and agree to comply with PPL rules governing payments and electronic transfers. I authorize PPL to withdraw from the
designated account all amounts deposited electronically in error. If the designated account is closed or has an insufficient balance to allow withdrawal,
then I authorize PPL to withhold any payment owed to me by PPL until the erroneous deposited amounts are repaid. If I decide to change or revoke
this authorization, I recognize that I must forward such notice to PPL.
1 Federal Employer Identification No. (EIN)
2 Social Security Number (SSN)

FFRREEQQUUEENNTTLLYY AASSKKEEDD QQUUEESSTTIIOONNSS AABBOOUUTT PPAAYY CCAARRDDSS
22
Phone: Administrative Fax: (877) 818‐9787 TTY: Timesheet Fax: (866) 661‐0309 Email:
(866)896‐0040(800)360‐5899 [email protected] Web: www.publicpartnerships.com
1. Do I need a bank account to obtain a pay card?No, you do not need a bank account to obtain a pay card.
2. What is a pay card?A pay card is an easy way to have your money deposited each payday without having a bankaccount. You are able to use this pay card at any ATM or it can be used just like a debit card tomake purchases directly.
3. Where can I obtain a pay card?A pay card can be obtained at a local merchant store (Wal‐Mart, CVS, Walgreens, etc) for anominal fee or via the pay card company’s website.
4. Is a new pay card needed for each pay cycle?No, the same pay card is used every pay cycle and the pay amount is directly transferred ontothe card.
5. What if all the money on the pay card is not used before the next pay cycle?The remaining balance on your pay card will carry over with your next deposit.
6. How do I know the balance on my pay card?For many pay cards, there will be a customer service number for the financial institution on theback of your pay card that you can call to obtain your card balance. Simply follow the directionsprovided to obtain your balance. If there is not a phone number for balances indicated on yourcard, refer back to your pay card enrollment paperwork for more information.
7. Are there any fees with the pay card?Your particular pay card may have transaction fees. PPL is not responsible for any feesestablished by the pay card’s financial institution.
8. Can I use my pay card at an ATM and will there be surcharges?Pay cards are usually accepted at any ATM. If the ATM charges a surcharge, you will be notifiedbefore the transaction is completed. You can accept the charge or you will have the option ofcanceling the transaction if you do not want to pay the fee.
9. Can I use my pay card to make online purchases?Usually, your pay card can be used to make online purchases. Refer to your pay card enrollmentpaperwork for additional information.
There are many websites where you can get free general information and/or information regarding pay cards such as, www.consumer‐action.org or www.usapaycard.com.

What You Need to Know About Incident Reporting
It is a requirement for anyone with direct care responsibilities of a participant including employers of records, providers and case managers with knowledge of an incident that affects, or potentially affects, this participant’s health, safety, or welfare to submit an initial Incident Report. An incident involving:
A) abuse, neglect, or exploitation of a participant or the death of a participantmust be submitted within 24 hours of the incident
OR
B) an “unusual occurrence” affecting the participant’s health, safety and welfareare must be submitted within 48 hours of the time of the incident
• An unusual occurrence includes, but is not limited to:o Significant injury to the participanto A residential fire resulting in relocation, and/or property loss in the
participant’s homeo Threat to public safety caused by the participanto Participant becomes a missing persono Medication erroro Criminal activity
Please submit reports on the Incident Reporting Website: https://ddrsprovider.fssa.in.gov/IFUR/
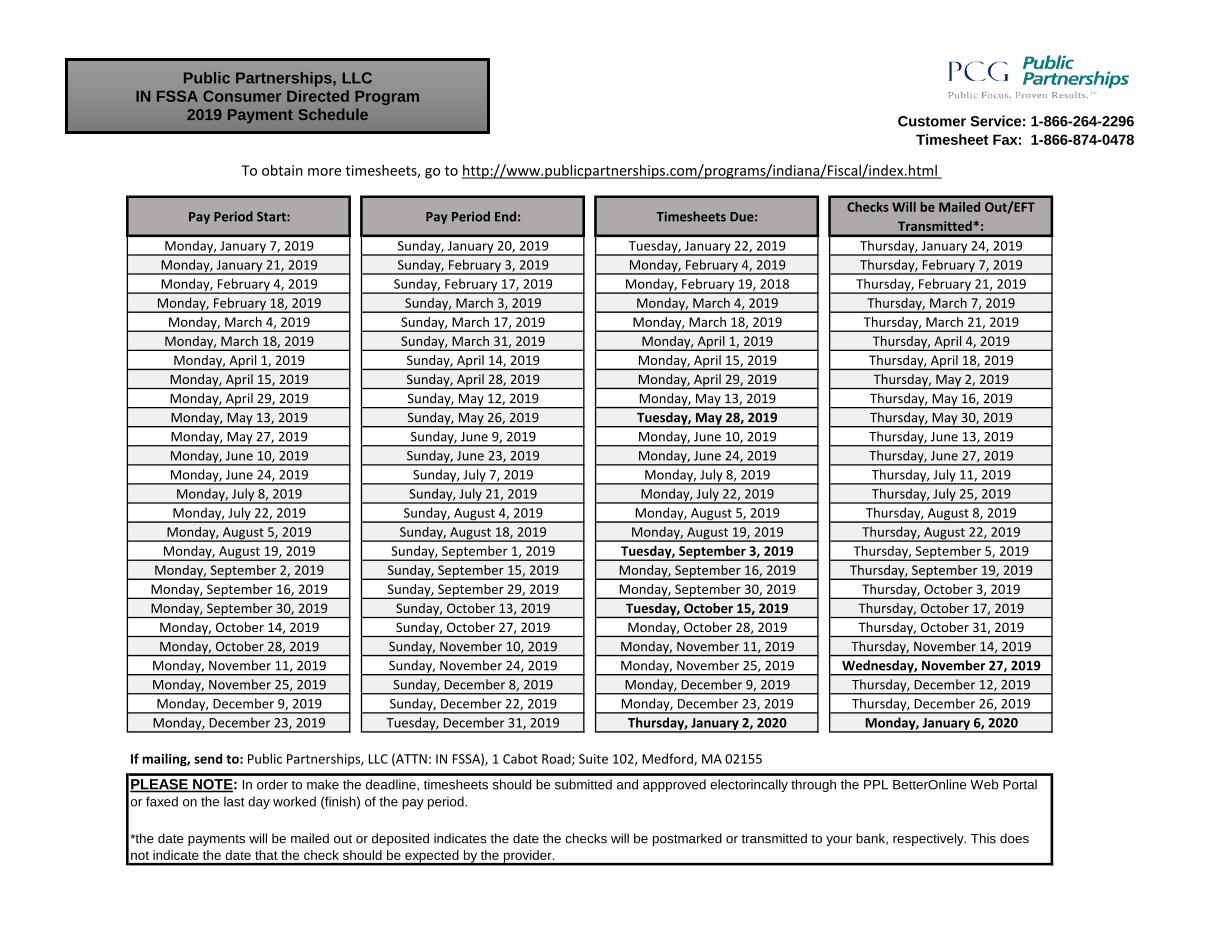
Customer Service: 1-866-264-2296Timesheet Fax: 1-866-874-0478
Pay Period Start: Pay Period End: Timesheets Due:Checks Will be Mailed Out/EFT
Transmitted*:Monday, January 7, 2019 Sunday, January 20, 2019 Tuesday, January 22, 2019 Thursday, January 24, 2019
Monday, January 21, 2019 Sunday, February 3, 2019 Monday, February 4, 2019 Thursday, February 7, 2019Monday, February 4, 2019 Sunday, February 17, 2019 Monday, February 19, 2018 Thursday, February 21, 2019
Monday, February 18, 2019 Sunday, March 3, 2019 Monday, March 4, 2019 Thursday, March 7, 2019Monday, March 4, 2019 Sunday, March 17, 2019 Monday, March 18, 2019 Thursday, March 21, 2019
Monday, March 18, 2019 Sunday, March 31, 2019 Monday, April 1, 2019 Thursday, April 4, 2019Monday, April 1, 2019 Sunday, April 14, 2019 Monday, April 15, 2019 Thursday, April 18, 2019
Monday, April 15, 2019 Sunday, April 28, 2019 Monday, April 29, 2019 Thursday, May 2, 2019Monday, April 29, 2019 Sunday, May 12, 2019 Monday, May 13, 2019 Thursday, May 16, 2019Monday, May 13, 2019 Sunday, May 26, 2019 Tuesday, May 28, 2019 Thursday, May 30, 2019Monday, May 27, 2019 Sunday, June 9, 2019 Monday, June 10, 2019 Thursday, June 13, 2019Monday, June 10, 2019 Sunday, June 23, 2019 Monday, June 24, 2019 Thursday, June 27, 2019Monday, June 24, 2019 Sunday, July 7, 2019 Monday, July 8, 2019 Thursday, July 11, 2019Monday, July 8, 2019 Sunday, July 21, 2019 Monday, July 22, 2019 Thursday, July 25, 2019
Monday, July 22, 2019 Sunday, August 4, 2019 Monday, August 5, 2019 Thursday, August 8, 2019Monday, August 5, 2019 Sunday, August 18, 2019 Monday, August 19, 2019 Thursday, August 22, 2019
Monday, August 19, 2019 Sunday, September 1, 2019 Tuesday, September 3, 2019 Thursday, September 5, 2019Monday, September 2, 2019 Sunday, September 15, 2019 Monday, September 16, 2019 Thursday, September 19, 2019
Monday, September 16, 2019 Sunday, September 29, 2019 Monday, September 30, 2019 Thursday, October 3, 2019Monday, September 30, 2019 Sunday, October 13, 2019 Tuesday, October 15, 2019 Thursday, October 17, 2019
Monday, October 14, 2019 Sunday, October 27, 2019 Monday, October 28, 2019 Thursday, October 31, 2019Monday, October 28, 2019 Sunday, November 10, 2019 Monday, November 11, 2019 Thursday, November 14, 2019
Monday, November 11, 2019 Sunday, November 24, 2019 Monday, November 25, 2019 Wednesday, November 27, 2019Monday, November 25, 2019 Sunday, December 8, 2019 Monday, December 9, 2019 Thursday, December 12, 2019Monday, December 9, 2019 Sunday, December 22, 2019 Monday, December 23, 2019 Thursday, December 26, 2019
Monday, December 23, 2019 Tuesday, December 31, 2019 Thursday, January 2, 2020 Monday, January 6, 2020
If mailing, send to: Public Partnerships, LLC (ATTN: IN FSSA), 1 Cabot Road; Suite 102, Medford, MA 02155
To obtain more timesheets, go to http://www.publicpartnerships.com/programs/indiana/Fiscal/index.html
PLEASE NOTE: In order to make the deadline, timesheets should be submitted and appproved electorincally through the PPL BetterOnline Web Portal or faxed on the last day worked (finish) of the pay period.
*the date payments will be mailed out or deposited indicates the date the checks will be postmarked or transmitted to your bank, respectively. This does not indicate the date that the check should be expected by the provider.
Public Partnerships, LLCIN FSSA Consumer Directed Program
2019 Payment Schedule

Self-Directed Attendant Care Program
Spend-Down Policy
EFFECTIVE DATE: MAY 5, 2010
Individuals receiving services through the Aged and Disabled Waiver’s Self-Directed Attendant Care program may have a spend-down. Having a spend-down means that an individual must pay his or her provider(s) directly for a portion of the services he or she receives each month.
If the individual you provide services to has a spend-down, and that amount has not already been met through other incurred medical charges for a particular month, that amount will be deducted from your wages.
If PPL deducts money from your wages for spend-down, PPL will send you a statement with your paycheck listing the amount deducted for the spend-down. You will then need to collect the amount of the spend-down directly from your employer, who is responsible for paying you the amount of the spend-down.
Toll-Free Numbers Phone: 1-866-264-2296
E mail: [email protected] Timesheet Fax: 1-866-874-0478
Administrative Fax: 1-866-799-9381 TTY: 1-800-360-5899

Attention Provider
Legislation signed by the President on August 10, 2010 repeals the Advanced Earned Income
Tax Credit. Recipients will not be able to claim Advance EITC after December 31, 2010.
Due to this legislation, we are unable to process any requests for advanced EIC. Please note
that the Earned Income Credit still exists. It is just that you can no longer request this credit
in advance in your paycheck. It can be claimed on Form 1040 when you file your 2011
income tax paperwork.
IRS Publication 596 explains the Earned Income Credit in great detail. Please refer to this
document for additional guidance. If further clarification on this legislation is needed, please
contact a tax professional.
Thank you,
PPL
Public Partnerships, LLC 7776 Pointe Pkwy E Ste. 150 Phoenix, AZ 85044
617.426.2026 Phone 866-421-3309 Fax