Public injecting, harm reduction services
82
Public injecting drug use and the local harm reduction services József Rácz
-
Upload
jozsef-racz -
Category
Health & Medicine
-
view
981 -
download
2
description
This ERASMUS lecture is about a Hungarian public injection scene, about the local harm reduction services (run by Blue Point Drug Counselling and Outpatient Centre) and about connections of public injecting to other risks, including "police risks".
Transcript of Public injecting, harm reduction services

Public injecting drug use and the local harm reduction services
József Rácz

Public injecting
Blue Point Drug Counselling and Outpatient Centre: Contact Cafe
8th district of Budapest
Injecting and sexual risk behaviours
Local harm reduction services
Risks of injecting: HIV, HCV
Data on needle exchange
Characteristics of the clientele
Harm reduction methods
Summary of a large scale study on needle exchange (Australia, 2009)

Public injecting scenes and shooting galleries

„Hurry up”, „rushed” injecting: sharing, neglecting safer injecting, discarded needles, more difficult access to needle exchange services
Searching clothes (jack-ups): needles’ legal status
Greater use of ‘discretion’ on the part of police has alsobeen recommended as a measure that may ensure that enforcement operations do not interfere with public health efforts – agreement between needle exchange services and police: this is not legal, but the police follows the recommendations (Hungary)
Drug market enforcement approaches interact with and transform various practices and social dynamics in the broaderrisk environment of IDU, and thereby constitute a potentsource of harm within drug markets
Street-level drug problems will appear elsewhere when the police crack down the public drug scene
Role of the police
Kerr et al., 2005;Small et al., 2006
•More illegal drug use
•More illegal drug using populations
•More difficult access to services
•New strategy maintaining public order and public health goals

Blue Point Drug Counselling and Outpatient Centre

8th district of Budapest with the placement of needle exchange program of Blue Point: the Contact Cafe

General background of 8th district

The VIII. district of Budapest faces a number of difficulties. This is an area where there are multiple social, health, livelihood, community, etc.. problems.
The drug and social problems are much higher compared to other districts.
The legal and illegal drugs and the presence of a large number of consumers in a very open drugscene requires various and several care providers at different levels to be present.
In particular, there are many addicts living in the district who are suspicious of institutional care, which is a high-threshold care service.
The legal and illegal drug use associated with poor living conditions and low social status seriously increases the risk of spreading diseases. The clients with health problems often do not turn to a doctor or do not ask for care and treatment.
Cultrual diversity – including Roma culture - is one of the characteristics of the disctrict. There are large differences of inhabitants concerning ethnicity, nationality, education and housing, and social status and health.
(The „Integrated Rehabilitation Strategy for Urban Development” of the capital places an emphasis on refurbishing the district, but this is impossible without dealing with social problems.)
The well-defined part of the disctict’s inhabitants are living in poor conditions, bad housing, has poor health culture, poor mental status and is low skilled and unemployed.
The socio-cultural background

Dezső Tamás’s photos
Feeling of the 8th district

(Semi)Public injecting sites

social workerwith visibility coat
Druglitter


Shooting galleryType 1





Shooting galleryType 2
Csoki 36 ys old, heroin dependent. His wife, Zita 35 ys old, heroin dependent. Their son, Csabika 17 ys old, heroin dependent.
„At the deepnest of drug world”Baptis Charity „Street Front”, Marcell Miletics, Miklós Barcs, Péter Borbély

Discarded needles, drug litter


Routes of transmitting infections
Defining the points of harm reduction interventions:•See -s!
Most difficult interventions

Common needle use
Sharing:Needles/SyringesFilterCookingWaterNeedles for preparation of drug solution
Direct sharingIndirect sharing
•Same syringes
•Backloading
•Frontloading

Activities at needle exchange programHarm reduction goals
Reaching out „hidden” injecting drug users: oureach and street work
Prevention of infections, especially:oHIVoHCV - injecting equipments/paraphernalia!oOther communicable diseases
• Only contact with helping services: low threshold service – only contact with majority society: ponts of treatment contacts/admissions
Needle exchange, outreach and street work + collecting syringesProviding information, education, counselling
Testing or referral to testingSexual risk behaviours – prevention (condoms)
First aid, referral to medical treatmentReferrals to other cares (health or social care)
Clients involvement – empowermentRehabilitation and reintegration
Activities: 4-8 p.m., 6x a week

Collecting dirty needles Most important for the local community & for the local self-government

Special programs at needle exchange (Contact Cafe)
Ladys’ Night: clients as well as helpers are women: once a week•Traumatization•PTSD•Sex workers•Sexual problems
Cooperation with „Sober Babies” Association•For pregnant injecting drug using women•For mothers with babies
Decreasing the digital edge•Computer literacy + social network site use

„User friendly milieu”



Roma culture on YouTube (videos watched by our clients)

Legal open sceneSwiss „needle parks: 1980s-1990s: failure – re-designing of the Swiss drug policy
Incidence of regular heroin users(Nordt és Stohler, 2006)
Results:New heroin users referred to treatment in two ys.4% yearly decrease in the number of problem heroin users.
Needle Park in Zürich, 1992

Risks of (public) injecting

The ranges around the estimates in this table define the boundaries within which the actual numbers lie, based on the best available information.
Regional HIV and AIDS statistics and features 2009
TOTAL 33.3 million[31.4 million – 35.3 million]
2.6 million[2.3 million – 2.8 million]
Adults and children newly infected with HIV
Adults and children living with HIV
Sub-Saharan Africa
Middle East and North Africa
South and South-East Asia
East Asia
Central and South America
Caribbean
Eastern Europe and Central Asia
Western and Central Europe
North America
Oceania
22.5 million[20.9 million – 24.2 million]
4.1 million[3.7 million – 4.6 million]
1.4 million[1.2 million – 1.6 million]
1.4 million[1.3 million – 1.6 million]
1.5 million[1.2 million – 2.0 million]
1.8 million[1.6 million – 2.0 million]
270 000[240 000 – 320 000]
92 000[70 000 – 120 000]
130 000[110 000 – 160 000]
70 000[44 000 – 130 000]
460 000[400 000 – 530 000]
770 000[560 000 – 1.0 million]
240 000[220 000 – 270 000]
820 000[720 000 – 910 000]
57 000[50 000 – 64 000]
75 000[61 000 – 92 000]
82 000[48 000 – 140 000]
17 000[13 000 – 21 000]
31 000[23 000 – 40 000]
4500[3400 – 6000]
1.8 million[1.6 million – 2.1 million]
Adult & child deaths due to AIDS
1.3 million[1.1 million – 1.5 million]
260 000[230 000 – 300 000]
58 000[43 000 – 70 000]
76 000[60 000 – 95 000]
26 000[22 000 – 44 000]
24 000[20 000 – 27 000]
36 000[25 000 – 50 000]
12 000[8500 – 15 000]
8500[6800 – 19 000]
1400[<1000 – 2400]
0.8%[0.7% - 0.8%]
Adult prevalence (15‒49) [%]
5.0%[4.7% – 5.2%]
0.3%[0.3% – 0.3%]
0.5%[0.4% – 0.6%]
0.8%[0.7% – 0.9%]
0.5%[0.4% – 0.7%]
0.2%[0.2% – 0.3%]
0.1%[0.1% – 0.1%]
1.0%[0.9% – 1.1%]
0.2%[0.2% – 0.2%]
0.3%[0.2% – 0.3%]

12/06 e
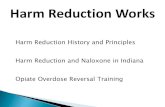
Proportions of HIV infections in different population groups by region, 2005
IDU: Injecting Drug UsersMSM: Men having sex with menCSW: Commercial Sex Workers
Latin America
MSM 26%
IDU 19%
CSW 4%
All others 38%
South and South-East Asia*
CSW clients 13%
Eastern Europe and Central Asia
MSM 4%
IDU 67%
CSW 5%
All others 17%
CSW clients 7%
* India was omitted from this analysis because the scale of its HIV epidemic (which is largely heterosexual) masks the extent to which other at-risk populations feature in the region’s epidemics.
MSM 5%
IDU 22%
CSW 8%
All others 24%
CSW clients 41%
Figure 2

Estimated occurance of injecting drug use per 1000 inhabitants, in the 15-64 ys groups (EMCDDA, 2009)
Contact Cafe32

Risks: The silent epidemic
Sitting on a bomb…

Hepatitis C infections in the European Union, 1995-2005
(Rantala és van de Laar, 2008)

HCV prevalences among injecting drug users(regional and national data),
2006-2007 (EMCDDA, 2009)
*: data from Contact Cafe

Source: OEK, 2007, 2008, 2009
HIV, HCV testing – HIV: 0%
Centre 2006 2007 2008
person HCV +% person HCV+% person HCV+%
Drug Prevention Foundation
55 34,5 100 34,7 100 34
Blue Point 20 75 70 75 70 63,2
Nyírő Hospital,
Drug Outpatient Centre
50 34 80 18 65 23
Soroksar Methadone Centre
15 20 40 21,6 40 25
Baptist Charity
„Street Front”
20 25 30 21,4 30 21,4

MedlinePlusThe is no spontaneousrecovery, just onlybecause of treatment.
At-risk group Acute infection (100%)
Recovered (15-30%) Chronic,
carrying the virus
55-85%
70 persons: chronic hepatic illness5-20 persons: cirrhosis - 20-30 ys – no symptoms1-5 persons: death (cirrhosis, hepatocellular carcinoma)
The Hepatitis C epidemic(EMCDDA, 2007)
Why it is „silent”!

Treated HCV infected patients after HCV testing (Gazdag és Szabó, 2007)
2 IFNtreated
9 clients visitedthe outpatient
centre
60 HCV+ drug users
175 tested drug users
Cost of treatment of HCV infection:
Treatment (1 year): 3,5 - 4m HUF
Total life span: 3,5 - 7m HUF

Finger stick (qiuck) HCV testing

Data on needle exchange program

Data
•Clients•Visits (one client may have more visits)•Needle: delivered & taken back

January 09 January Febr March April May June July August Sept. Oct. Nov. Dec
Registered clients in 2010 (from January to December

2010.II.
félév
2010.I.
félév
2009.II.
félév
2009.I.
félév
2008.II.
félév
2008.I.
félév
2007.II.
félév
2007.I.
félév
2006.II.
félév
300
250
200
150
100
50
0
201221216221
233227205
276265
New clienst (per half a year)
2006 2nd halfyear
2010 2nd halfyear
N %
Active clients*
1047 50.7
Inactive clients
1019 49.3
sum 2066 100.0
Active and inactive clients
(total clients: 100%)
*visited the NEP at least once in 2010

Gender distribution in a certain year (%)
2010.
2009.
2008.
2007.
2006.
100%80%60%40%20%0%
28.0%
24.0%
27.6%
22.9%
18.6%
72.0%
76.0%
72.4%
77.1%
81.4%
Nõ
Férfi
N=2066
MaleFemale
Age of registered clients
<19 20-24 25-29 30-34 35-39 40+ys
malefemale
Total

Inactive clients
(%)
Active clients
(%)7th district 3.2% 4.7%
8th district 54.0% 55.5% 9th district 9.9% 10.5% 10th district 4.5% 6.2% „distant clients” 28.4% 23.1% Sum 100.0% 100.0%
2010.
2009.
2008.
2007.
2006.
100%80%60%40%20%0%
3%
2%
7%
4%
5%25%
42%
29%
30%
68%
62%
54%
66%
68%
30%
egyéb szer
absztinens,másnak visz
mefedron
heroin(ópiátok)
amfetamin
abstinentother
Drug use among registered clients
Place of residency

Place of residency
District N %
1. 2 ,2
2. 1 ,1
3. 15 1,4
4. 5 ,5
5. 7 ,7
6. 18 1,7
7. 41 3,9
8. 604 57,9
9. 113 10,8
10. 47 4,5
11. 22 2,1
12. 6 ,6
13. 53 5,1
14. 23 2,2
15. 9 ,9
16. 6 ,6
17. 3 ,3
18. 3 ,3
19. 14 1,3
20. 14 1,3
21. 5 ,5
22. 2 ,2
23. 4 ,4
Non Bp. 27 2,6
Sum 1044 100,0
} 7+ 8+ 9 district = 72,6%
Important for the local self-government

Clients’ visits per monthJanuary 2009 – July 2010
Febr. March

Delivered injectors in 2010
Injectors taken back in 2010
Clients’ visits per day
Febr. March
older clients return syringes in 45% of cases, while the proportion of returning the used syringes in case of new clients is only 22%

Typical client:
From the 8th district
Late 20s
Male
Amphetamine user
Socially excluded
Wrong employment position, criminality
Defined themselves as Roma

Main characteristics of the 8th district scene1.Many IDUs in a small territory: close community
2. Public injecting + shooting galleries (Type 1+2) + „drug litter”
3. High HCV infection prevalence, high risk behaviours prevalences1. injecting: common or shared injection equipment use2. sexual: without condoms, IDU sex partners, IDU sex workers
4. Difficult access to treatment visible!1. addiction treatment2. HCV treatment3. other (primary care, gyneacologist)

Local community affected
Fear from injecting drug users
Public nuisances
Discarded needles at playgrounds as well
Street drug dealing
Crime for drugs
Children as witness of injecting„Solutions”
Abstinence-oriented treatment
Methadone maintenance
Police presence
Needle exchangeLocal survey N=150

What does the needle exchange program do: some examples?

Safer injecting practices

Safer injecting practices

Safer injecting practices

More use – syringe deformities
Gyarmathy et al., 2009
Mean volume of fluid retained in two types of syringes

Needle exchange

Needle + paraphernalia exchange

Condoms and sexual counselling

Country Region Number syringes 2005
Number syringes 2006
Belgium Flemish community 390 522 538 783
Belgium French community 261 182 246 519
Bulgaria National (1) (6) 600 000 210 464
Czech Republic National (2) 3 274 000 3 868 880
Denmark National (3) 910 000
Germany National
Estonia National 867 600 1 615 270
Ireland National
Greece National 29 782 34 809
Spain National 3 184 845
France National
Italy National
Cyprus National 0 0
Latvia National 123 895
Lithuania National 258 650 196 952
Luxembourg National 406 451 332 347
Hungary National 85 127 142 433
Malta National 220 211 225 716
Netherlands Regional (9) 440 000 380 000
Austria Regional (7) 1 811 962 2 082 840
Poland National (10) 372 000 318 155
Portugal National (8) 2 845 031 2 591 150
Romania (4) 1 038 000 300 000
Slovakia Regional (13) 362 055 384 293
Finland National (11) 1 891 903 2 400 000
Sweden National 117 894
United Kingdom England and Wales 27.000.000 (2002)
United Kingdom Northern Ireland (12) 85 801 97 684
Croatia 135 981
Turkey 0 0
Norway National (5) 3 300 000
Needle exchange in the EU

Adequate syringe coverage: as many syringes from the SEP as their self reported injections in the last 30 days. SEPs were classified based on their syringe dispensation policy:
•unlimited needs-based distribution; •unlimited one-for-one exchange plus a few additional syringes; •per visit limited one-for-one plus a few additional syringes; Blue Point +5•unlimited one-for-one exchange; •per visit limited one-for-one exchange.
Findings:•unlimited needs-based distribution = 61%; •unlimited one-for-one plus = 50%; •limited one-for-one plus = 41%; •unlimited one-for-one = 42%; •limited one-for-one = 26%.
In multivariate analysis, adequate syringe coverage was significantly higher for all dispensation policies compared to per visit limited one-for-one exchange. Conclusion: Providing less restrictive syringe dispensation is associated with increased prevalence of adequate syringe coverage among clients.
Syringe dispensation policyBluthental et al., 2006

Drug use among needle exchange clients and their
friends (≠ clients)
Márványkövi, Melles, Légmán and Rácz, 2008
Drug use – last 30 days (%)
57,161,4
17,1
51,4
12,9
40,040,0
82,9
5,7
54,3
21,424,3
48,6
72,1
11,4
52,9
17,1
32,1
0
10
20
30
40
50
60
70
80
90
heroin amphetamine
non-presc. methadone
marijuana ecstasy sedatives
non roma drug user
roma drug user
total

Márványkövi, Melles, Légmán és Rácz, 2008
Injecting risk behaviours(≠ clients)
paraphernalialast 30 days
paraphernalialifetime
needleslast 30 days
needleslifetime
total 52% 75% 9% 56%
roma idu 60%* 80% 11,4%* 51,4%
non-roma idu 44%* 70% 7,1%* 60%
* p < 0,05

Mean N Sd
Outpatient 1,98 49 1,31Methadone maintenance 4,28 50 1,33
Daily clinic 1,50 28 1,04
Inpatient 2,39 49 1,50
Residential (TC) 3,03 39 1,50
1: easy access………………………5: very difficult access
Márványkövi, Melles, Légmán és Rácz, 2008Márványkövi, Melles és Rácz, 2006
Perceived access to different treatments

Public health measures(Gyarmathy and Rácz, 2010)
HCV as a HIV marker: at 30-35% HCV infection rate (Vickerman)1. Substitution (methadone, buprenorphine,
buprenorphine/naloxone=Suboxone)2. Access to sterile needles (needle exchange,
pharmacists)3. HIV, HCV testing + counselling4. Medically supervised injecting
Blue Point services
1. Substitutions: no funding2. Needle exchange: problem of long-term funding3. HIV, HCV testing + counselling: cooperation with the National
Centre for Epidemiology4. Supervised injection: against the law
From the literature:

Sydney Medically supervised
injecting facilities

München

Sydney

Sydney

Entrance: Vancouver
Exit
Köln
Hannover
Frankfurt

Medically supervised injecting facilitiesHedrich, 2004 (EMCDDA)
Road to survival
• It needs local, city and national level consents• More advantages than disadvantages
• It is placed in a complex caring – treatment structure• It does not fulfil irreal expectations:
– Erases public injecting– Persuades injecting drug users to stop their drug use– In itself is not enough for decreasing morbidity and mortality rates– Solves problems with drug dealing and trafficking

Some experiences from a large scale Australian study on needle exchanges – 2000 - 2009

Estimated number of Australian IDUs
No. of syringes distributed in Australia)
≈150 injector/IDU

Injecting acts per injecting drug users (Australia Government Report, 2009)
Figure shows that injecting drug users are not able to decrease their drug use!
Injecting drug using visitors of the 8th district are about: 2.000 persons (1.500-2.500).
It means 800.000 injecting occasions per year, but here amphetamine users are the majority (who inject more frequently than heroin users), this number
maybe more than 1 million occasions per yearDistributed needles by the Contact Cafe are about 100.000/year, coverege of
injecting occasions are about 12,5% (10%).Similar coverege to Austratalia (150 injectors/person) – means about 300.000
injectors in a year.

Cost-effectiveness of Australian NSPs
Summary of investmentThe number of needles and syringes distributed in Australia increased during the past decade (from ~27 million to ~31 million).
Measures for NSPs to increase referrals to drug treatment and other services.• Over the last decade there has beeno Increases in funding for primary sites.o Increases in the number of secondary sites.o Increases (by 15%) in the numbers of units of equipment provided.o Stable spending on sterile injection equipment.O There were 85 primary sites, 737 secondary sites, 20 enhanced secondary sites, and 118 vending machines in 2010.

Effectiveness of NSPs
It was estimated that over the last decade (2000-2009) NSPs have directly averted:
• 32,050 new HIV infections;• 96,667 new HCV infections.
When secondary transmissions (sexual or mother-to-child transmission from infected IDUs) are considered, the epidemiological benefits are even greater.

Economic analysis of NSPs during 2000-2009
During 2000-2009, gross funding for NSP services was $243m. This investment yielded:• Healthcare costs saved of $1.28 billion.• Approximately 140,000 DALYs gained.• Net financial cost-saving of $1.03 billion.
It was estimated that:• For every one dollar invested in NSPs, more than four dollars were returnedin healthcare cost-savings in the short-term (ten years) if only direct costs are included; greater returns are expected over longer time horizons.• The majority of the cost savings were found to be associated with HCV-relatedoutcomes. However, when only HIV-related outcomes were considered in theanalysis, it cost $4,500 per DALY gained associated with HIV infection.• If patient/client costs and productivity gains and losses are included in the analysis,then the net present value of NSPs is $5.85bn; that is, for every one dollar invested inNSPs (2000-2009), $27 is returned in cost savings. This return increases considerably over a longer time horizon.• NSPs are very cost-effective compared to other common public health interventions.
DALY: disability-adjusted life year

The simulated number of annual (a) HIV and (b) HCV transmissionsamong IDUs in Australia versus the percentage of injections that are
shared and theaverage number of times each syringe is used before disposal.
The dashed lines refer to current levels of sharing and syringe use.
HIV HCV

Scatter plots of the simulated number of annual (a) HIV and (b) HCVtransmissions among IDUs in Australia versus the number of sterile
syringesdistributed in Australia are shown, assuming that syringe distribution
changes theaverage number of times each syringe is used before disposal.
The blue dots are results from 1000 simulations, the red curves represent the median parameter values, and the black dashed lines refer to current levels of syringe distribution.