Public Holiday - Shire of Broome Holiday BRAC Movie Day! Bring your bean bag or cushion! We will...
12
Monday 16th January Tuesday 17th January Wednesday 18th January Thursday 19th January Friday 20th January Atomic Apple Crumble TABLOID WATER SPORTS Lets make our own Grass Heads! Design and make your own grass head, then watch its grow hair! Inflatable Slip and Slide fun on Father Mac oval! Bring your water guns! BRAC Movie Day! Bring your bean bag or cushion! We will supply the popcorn! Monday 23rd January Tuesday 24th January Wednesday 25th January Thursday 26th January Friday 27th January Cooking fun with BOAB health services! WATER FIGHT!!! Lets play some team Skirmish Games! RED VS BLUE Who Will Win? Bring your own Water gun! Kitchen Science! Let have some fun and try some scientific experiments with food! Public Holiday BRAC Movie Day! Bring your bean bag or cushion! We will supply the popcorn!
Transcript of Public Holiday - Shire of Broome Holiday BRAC Movie Day! Bring your bean bag or cushion! We will...

Monday
16th January
Tuesday
17th January
Wednesday
18th January
Thursday
19th January
Friday
20th January
Atomic Apple
Crumble TABLOID
WATER
SPORTS
Lets make our
own Grass Heads!
Design and make
your own grass
head, then watch
its grow hair!
Inflatable Slip
and Slide fun on
Father Mac
oval!
Bring your
water guns!
BRAC Movie Day!
Bring your bean
bag or cushion!
We will supply
the popcorn!
Monday
23rd January
Tuesday
24th January
Wednesday
25th January
Thursday
26th January
Friday
27th January
Cooking fun with
BOAB health
services!
WATER FIGHT!!!
Lets play some
team Skirmish
Games!
RED VS BLUE
Who Will Win?
Bring your own
Water gun!
Kitchen Science!
Let have some
fun and try
some scientific
experiments
with food!
Public
Holiday
BRAC Movie Day!
Bring your bean
bag or cushion!
We will supply
the popcorn!

Dear Parent/Guardian
Please find attached the program information for the January 2017 BRAC School Holiday Program.
It is BRAC’s policy that a New Enrolment form must be complete each calendar year. Please find a New Enrolment form
attached below.
Program details:
Cost: Enrolments can only be made with full payment. There are limited spaces so it is strongly recommended you book
early to avoid disappointment. Enrolments are non-refundable unless a medical certificate is provided with the request.
Half day - 8.00am – 2.30pm: $40
Full Day – 8.00am – 4.30pm: $55
Dates:
Week 1 Week 2 Monday 16 January 2017 Monday 23 January 2017 Tuesday 17 January 2017 Tuesday 24 January 2017 Wednesday 18 January 2017 Wednesday 25 January 2017 Thursday 19 January 2017 Thursday Public Holiday Friday 20 January 2017 Friday 27 January 2017 Please see attached program for details on each day’s activities. **The Program will be held in the Stadium and Multipurpose Room at the Main Centre. Please drop and pick up your children from there. Age Limit: 6 years – 12 years Enrolments Open: 12 December 2016
Broome Recreation and Aquatic Centre Cable Beach Road, Broome
Phone: 9191 8720 Fax: 9193 6714
Email: [email protected] Web: www.broome.wa.gov.au

What to bring:
Hat and sunscreen is a must. NO HAT NO PLAY.
Footwear is a must; thongs are acceptable but some consideration should be given to the day’s programmed activities.
Water bottle
Swimmers and towel. Bring everyday just in case. Please clearly label all items (clothes, bags, water bottles etc) brought to the BRAC School Holiday Program.
Not permitted:
Games consoles, MP3 players, Trading cards and valuables are not allowed on the school holiday program as we
encourage children to participate in all of the activities. BRAC staff will take no responsibility for these items if
lost, stolen or damaged.
Food:
Morning tea, afternoon tea and lunch are not provided unless specified on the program.
Children are welcome to bring their own morning tea, lunch and afternoon tea. Ensure you provide your child
enough food for the whole day. The children are participating in physical activity so they do get hungry.
BRAC has a menu available for the BRAC School Holiday Program which includes options for morning tea, lunch
and afternoon. Please place your order at the kiosk in the morning when you arrive.
BRAC School Holiday Program participants are not allowed casual access to the kiosk during program hours.
Some programs (cinema) are conducted during meal times. Please check with reception before ordering.
Arrival/Departure:
Parents and Guardians must sign their children in and out each day. The child will only be able to leave if signed
out by a person nominated on their enrolment form.
Written notice is required if your child wishes to cycle to and from the centre.
Program:
Every effort will be made to deliver the advertised program but from time to time the program may need to
change due to unforeseen circumstances.
Center Rules:
Centre rules are established for the safety and well being of all the children. Failure to comply with the rules
may result in the exclusion from the program following consultation with staff, parents and Guardians.

January 2017 BRAC School Holiday Program Days of Enrolment (please tick those required):
Childs First Name
Monday 16 January
Tuesday 17 January
Wednesday 18 January
Thursday 19 January
Friday 20 January
Half Day
Full Day
Half Day
Full Day
Half Day
Full Day
Half Day
Full Day
Half Day
Full Day
Childs First Name
Monday 23 January
Tuesday 24 January
Wednesday 25 January
Thursday 26 January
Friday 27 January
Half Day
Full Day
Half Day
Full Day
Half Day
Full Day
Public Holiday
Half Day
Full Day
OFFICE USE ONLY
Amount paid:____________________________ Date:___________________________________
Staff Name:_____________________________ Receipt Number:_________________________
Broome Recreation & Aquatic Centre Cable Beach Road East
PO Box 44 BROOME WA 6725 Ph: (08) 9191 8720
Fax: (08) 9193 6714 Email: [email protected]
Web: www.broome.wa.gov.au

2017 School Holiday Enrolment Form
It is essential that prior to commencement of care the following information is complete and up to date. A new enrolment form must be completed for each calendar year. This form must be completed by a parent or guardian who has lawful authority in relation to the child. Please ensure that you notify BRAC of changes such as address, phone numbers or care arrangements. A brief explanation of ‘lawful authority’ can be found at the end of this form. CHILD DETAILS DATE: ___________________
Child Name Date of Birth Age M/F Swimming Ability
(Non/Weak / Med /Strong) 1.
2.
3.
Home address: _________________________________________________________________________________
PO Box:_______________________________________________________________________________________
Language(s) spoken at home: ______________________________________________________________________
Does the child/ren live with: both parents one parent guardian
PARENT/GUARDIAN 1 DETAILS
Full name:____________________________________ R/ship to the child:__________________________________
Telephone (M): _________________________________Telephone(W):____________________________________
Telephone (H):_____________________________________PO Box:_______________________________________
Email: _________________________________________________________________________________________
Authorised to collect the child YES NO
PARENT/GUARDIAN 2 DETAILS
Full name:____________________________________ R/ship to the child:__________________________________
Telephone (M): _________________________________Telephone(W):____________________________________
Telephone (H):_____________________________________PO Box:_______________________________________
Email: _________________________________________________________________________________________
Authorised to collect the child YES NO
Broome Recreation & Aquatic Centre Cable Beach Road East
PO Box 44 BROOME WA 6725 Ph: (08) 9191 8720
Fax: (08) 9193 6714 Email: [email protected]
Web: www.broome.wa.gov.au

EMERGENCY CONTACT (in addition to parent/guardian as listed above)
Please provided names of 2 people authorised to collect your child from the program in case of an emergency and to
provide consent to the medical treatment of your child in the event that NEITHER parent/guardian is available.
Identification must be provided upon request.
1. Full name:__________________________________ R/ship to the child:_________________________________
Telephone (M): ______________________________ Telephone(W):___________________________________
2. Full name:__________________________________ R/ship to the child:_________________________________
Telephone (M): ______________________________ Telephone(W):___________________________________
AUTHORISATION TO COLLECT CHILD/REN
Please complete the following information to notify staff of persons authorised to collect your child/ren from the
School Holiday Program. Staff will not under any circumstances allow any person to collect your child/ren other
than those listed below. Alternate arrangements will only apply where proper notification from you in writing is
received on that particular day. Identification must be produced upon request.
1. Full name: _______________________________ R/ship to the child:__________________________________
Telephone (M):___________________________ Telephone (W):_____________________________________
2. Full name: _______________________________ R/ship to the child:__________________________________
Telephone (M):___________________________ Telephone (W):_____________________________________
3. Full name: _______________________________ R/ship to the child:__________________________________
Telephone (M):___________________________ Telephone (W):_____________________________________
4. Full name: _______________________________ R/ship to the child:__________________________________
Telephone (M):___________________________ Telephone (W):_____________________________________
COURT ORDERS RELATING TO THE CHILD
Are there any court orders relating to the powers and responsibilities of the parents in relation to the child or
access to the child/ren? Please tick
NO – proceed to the next page YES – please read and complete the following
1. A copy of the original court order is to be provided along with this enrolment form.
2. Please give details if these court orders give powers to other persons which may affect the powers, duties,
responsibilities and/or authorities of a parent or guardian of the child to in regards to:
• Consent to the medical treatment of the child/ren and the authorisation of the service to seek medical
treatment by an appropriate medical or ambulance service
• Request or permit the administration of medication to the child/ren
• Authorise the taking of the child/ren outside the premises by a staff member of the service in the case
of emergency when reasonably required
• Collect the child/ren
Details: ______________________________________________________________________________________

FAMILY DOCTOR/MEDICAL SERVICE
Name: _______________________________________________________________________________________
Address: _____________________________________________________________________________________
Telephone: ____________________________________ Medicare No: ___________________________________
MEDICAL INFORMATION
Please provide details and attach a copy of relevant management procedures or plans for any ‘yes’ responses.
In the case of anaphylaxis you will be provided with a copy of the programs Medical Conditions Policy. You are required to
provide the program with an individual medical management plan (Action Plan) for your child signed by the medical
practitioner treating your child.
CHILD 1 __________________________________________
Has your child been diagnosed at risk of anaphylaxis? YES NO
Does your child have an auto injection device (e.g. EpiPen)? YES NO
Has the anaphylaxis medical plan been attached to this form? YES NO
Does your child have any special needs e.g. medical/physical? YES NO
Does your child suffer from any allergies or sensitivities? YES NO
Does your child have any dietary restrictions? YES NO
CHILD 2__________________________________________
Has your child been diagnosed at risk of anaphylaxis? YES NO
Does your child have an auto injection device (e.g. EpiPen)? YES NO
Has the anaphylaxis medical plan been attached to this form? YES NO
Does your child have any special needs e.g. medical/physical? YES NO
Does your child suffer from any allergies or sensitivities? YES NO
Does your child have any dietary restrictions? YES NO

CHILD 3__________________________________________
Has your child been diagnosed at risk of anaphylaxis? YES NO
Does your child have an auto injection device (e.g. EpiPen)? YES NO
Has the anaphylaxis medical plan been attached to this form? YES NO
Does your child have any special needs e.g. medical/physical? YES NO
Does your child suffer from any allergies or sensitivities? YES NO
Does your child have any dietary restrictions? YES NO
We regret that our School Holiday Program is unable to care for sick children or children with contagious illness.
PLEASE NOTE: If your child/ren requires the administration of medication please complete an ‘Authority to Give
Medication Form’.
OTHER INFORMATION
Please include any other information you feel the School Holiday Program needs to be aware of in relation to your
child and/or family , (e.g. excessive fears, toileting, behavioural styles, interests and abilities, cultural values and
religious beliefs, etc)?
CONDITIONS OF ENROLMENT
By enrolling my child/ren in the BRAC School Holiday Program, I agree to the following conditions:
1. Children are only accepted into the School Holiday program from 6 years of age through to 12 years of age.
2. Although all care will be taken, program staff will not be held responsible for accidents or loss of property in
connection with any child’s participation in the program.
3. I am willing for my child/ren to participate in all activities offered in the School Holiday Program. I agree it is my
responsibility to familiarise myself with the program and to advise BRAC in writing if I do not wish my child/ren
to participate in a particular activity.
4. In the event of accident, injury, trauma or illness suffered by my child/ren, I agree that program staff are
authorised, on behalf of myself, to seek or where appropriate administer such medical treatment as is
reasonably required. In regards to cases where an ambulance is called, I shall then reimburse BRAC for any
expense incurred.
5. In the case of an emergency and for training purposes I authorise the taking of my child/ren outside of the
premises of the program by a staff member.

6. All children enrolled are expected to follow the instruction of all BRAC staff members and behave appropriately.
If your child/ren does not behave appropriately BRAC reserves the right to call you to come and collect your
child. If this behaviour continues throughout the program BRAC reserves the right to “expel” your child from the
program.
7. I agree that my child/ren may be photographed while participating in the program for the internal use only. To
agree for photographic consent for advertising purposes I will complete the attached ‘Photographic Consent
Form’.
8. I give permission to the program to allow my child/ren to travel by Charted Bus, Public Transport and/or Private
Transport on a scheduled excursion outing, and to walk with staff members to a particular outing (if the need
arises).
PRIVACY DISCLAIMER
I agree that you may use my personal information for marketing purposes. You may use my personal information
to develop marketing list and other programs. You may include my name and contact details on marketing lists
and offer me goods and services via email or mail. If you do not agree to this Privacy Disclaimer, please tick this
box.
DECLARATION I declare that the information above is complete and accurate, and I have read, understood and agree to the conditions outlined above. I understand and agree that I will not hold The Shire of Broome, Broome Recreation and Aquatic Centre, or its staff, liable for any personal injury which may occur to my child/ren or loss of property, except for any liability by the Shire of Broome if it fails to render its services with due care and skill, or supplies any material in connection with those services which is not reasonably fit for the purpose for which they are supplied. Print Full Name:_________________________________________________ Date:__________________________ Parent/Guardian Signature:______________________________________________________________________ LAWFUL AUTHORITY: PARENTS All parents have power and responsibilities in relation to their children, which can only be challenged by a court order. Lawful authority is not affected by the relationship between parents, such as whether or not they have lived together or are married. A court order, such as under the Family Law Act, may take away the authority of a parent to act or may assign the responsibility to another person. GUARDIANS A guardian of a child also has lawful authority. A legal guardian is given lawful authority by a court order. The definition of ‘guardian’ under the Children’s Services Act 1996 also covers situations where a child does not live with his or hers parents and there are no court orders. In these cases the guardian is the person the child lives with who has day to day care and control of the child.
OFFICE USE ONLY Has the following been given to the parent/guardian: Applicable Medical Management Plan YES Date:_____________________

PHOTOGRAPHIC CONSENT FORM
Company Name: Shire of Broome
Centre Name: Broome Recreation and Aquatic Centre
1. Purpose:
A series of photographs are being taken to be used by the Centre and the Company in a variety of publications,
brochures, posters and on internet sites for promotional purposes. You will have the right of access to view
these photographs.
By signing this form you understand you are granting the Company the right to use these photographs for the
purposes indicated in this form of approval.
Please read this form carefully before signing and if you have any questions please contact the Program
Development Officer prior to signing.
2. Details of person being photographed
Name: ______________________________________________________________________________________
Address:____________________________________________________________________________________
Date of Birth:_________________________________________________________________________________
3. Granting of a non exclusive licence and conditions
(a) I agree to grant a non exclusive license to the Company and the Centre, at its discretion to copy or
reproduce such material (whether by photo, film or other electronic or printed media) as the Centre
determine, without acknowledgement of myself and without the entitlement to any remuneration of
compensation now or in the future. I agree that I will have no further rights in the photographs including
moral and copyright.
(b) The Company and the Centre agree not to use any photographs in a manner that may be deemed adverse,
or defamatory to the person signing this form.
4. Authorisation
I hereby agree to the terms and understand the conditions set out above (if under 18 a parent or guardian’s
signature is required).
__________________________________________ _____________________________________________
(signature) (Parent/Guardian Name)
_____________________________________________
(Parent/Guardian Name)
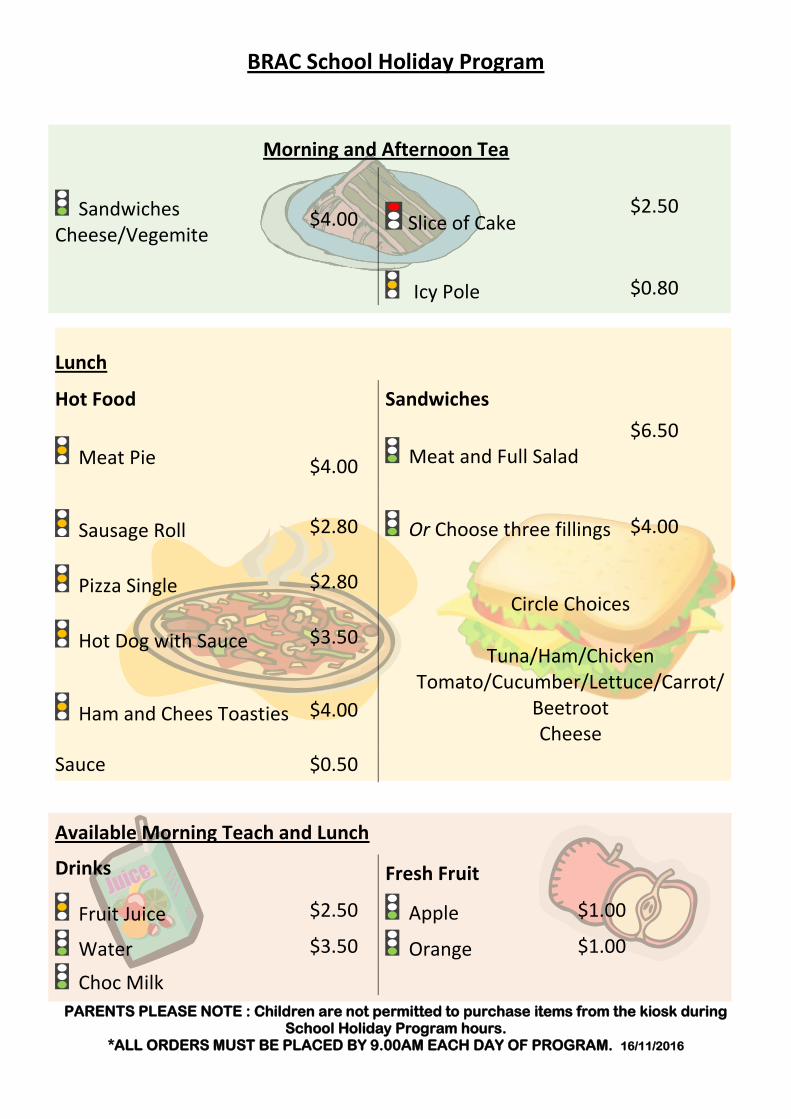
PARENTS PLEASE NOTE : Children are not permitted to purchase items from the kiosk during School Holiday Program hours.
*ALL ORDERS MUST BE PLACED BY 9.00AM EACH DAY OF PROGRAM. 16/11/2016
BRAC School Holiday Program
Morning and Afternoon Tea
Sandwiches Cheese/Vegemite
$4.00 Slice of Cake $2.50
Icy Pole $0.80
Lunch
Hot Food Sandwiches
Meat Pie $4.00 Meat and Full Salad
$6.50
Sausage Roll $2.80 Or Choose three fillings $4.00
Pizza Single $2.80 Circle Choices
Tuna/Ham/Chicken
Tomato/Cucumber/Lettuce/Carrot/ Beetroot Cheese
Hot Dog with Sauce $3.50
Ham and Chees Toasties $4.00
Sauce $0.50
Available Morning Teach and Lunch
Drinks Fresh Fruit
Fruit Juice $2.50 Apple $1.00
Water $3.50 Orange $1.00
Choc Milk

BROOME RECREATION AND AQUATIC CENTRE CREDIT CARD PAYMENT FORM
PERSON COMPLETING FORM: ________________________________________________________________________
IMPORTANT – PLEASE NOTE: Please complete ALL sections.
The Broome Recreation and Aquatic Centre does not accept Diners Club card, Bankcard or American Express.
NO notification confirming approval of payment will be given unless requested (ie. Receipt). Your bank statement for the credit card payment will state ‘Shire of Broome’. Payment will be processed the week following closure of enrolments to secure your child’s
enrolment
TOTAL AMOUNT TO BE PAID FROM CREDIT CARD
$ :
ACCOUNT TYPE Visa Master Card
CARD HOLDERS NAME (As shown on card): ___________________________________________________
CARD NO:
EXPIRY DATE / RECEIPT REQUIRED?
POSTAL ADDRESS ADDRESS______________________________________________________________________________________________________________ TOWN SUBURB______________________________________________________________STATE__________________POSTCODE___________
DAYTIME PHONE NO._____________________________________________________________________________ Email:__________________________________________________________________________________________
__________________________________________________________ _______/_______/_______ SIGNATURE OF CARD HOLDER DATE
OFFICE USE ONLY
STAFF NAME. ____________________________________________
RECEIPT NO. __________________ RECEIPT DATE ____/____/____